
Severity of COVID-19 in Patients with Diarrhoea: A Systematic Review and Meta-Analysis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
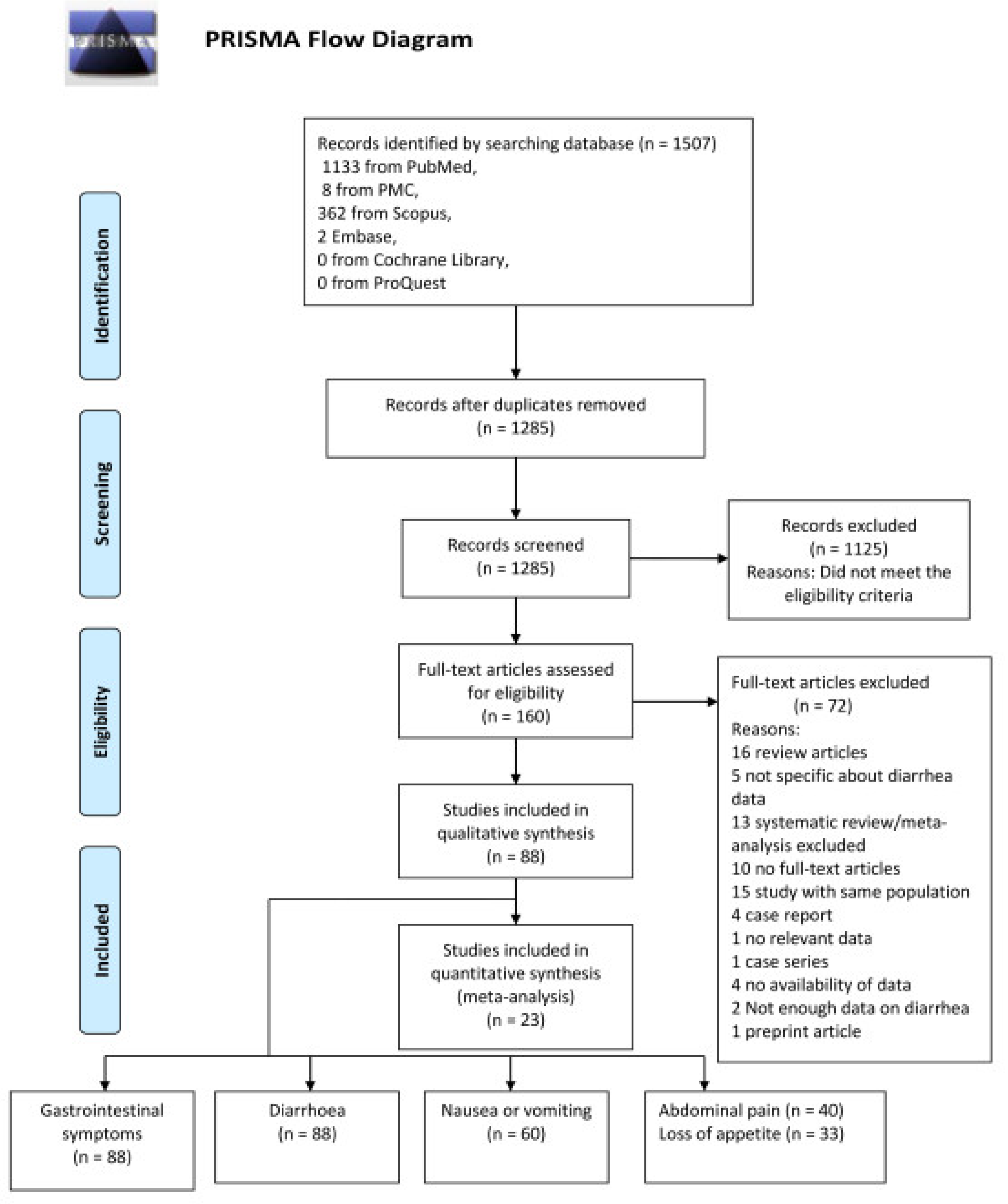
2.1. Methodology of Search and Selection Criteria
2.2. Extraction of Data and Definitions
2.3. Assessment of the Risk of Bias
2.4. Outcome
2.5. Statistical Analysis
3. Results
Study Characteristics and Statistical Findings
4. Discussion
4.1. The Implications of the Study
4.2. Limitation of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Elkhatib, W.F.; Abdelkareem, S.S.; Khalaf, W.S. Narrative review on century of respiratory pandemics from Spanish flu to COVID-19 and impact of nanotechnology on COVID-19 diagnosis and immune system boosting. Virol. J. 2022, 19, 167. [Google Scholar] [CrossRef]
- Grant, M.C.; Geoghegan, L.; Arbyn, M. The prevalence of symptoms in 24,410 adults infected by the novel coronavirus (SARS-CoV-2; COVID-19): A systematic review and meta-analysis of 148 studies from 9 countries. PLoS ONE 2020, 15, e0234765. [Google Scholar] [CrossRef]
- Klopfenstein, T.; Kadiane-Oussou, N.D.J.; Royer, P.-Y. Diarrhea: An underestimated symptom in Coronavirus disease 2019. Clin. Res. Hepatol. Gastroenterol. 2020, 44, 282–283. [Google Scholar] [CrossRef]
- Ozkurt, Z.; Çınar Tanrıverdi, E. COVID-19: Gastrointestinal manifestations, liver injury and recommendations. World J. Clin. Cases 2022, 10, 1140–1163. [Google Scholar] [CrossRef]
- Wang, M.-K.; Yue, H.-Y.; Cai, J. COVID-19 and the digestive system: A comprehensive review. World J. Clin. Cases 2021, 9, 3796–3813. [Google Scholar] [CrossRef]
- Aumpan, N.; Nunanan, P.; Vilaichone, R.K. Gastrointestinal manifestation as clinical predictor of severe COVID-19: A retrospective experience and literature review of COVID -19 in Association of Southeast Asian Nations (ASEAN). JGH Open 2020, 4, 1096–1101. [Google Scholar] [CrossRef]
- Ghimire, S.; Sharma, S.; Patel, A. Diarrhea Is Associated with Increased Severity of Disease in COVID-19: Systemic Review and Metaanalysis. SN Compr. Clin. Med. 2021, 3, 28–35. [Google Scholar] [CrossRef]
- Berlin, D.A.; Gulick, R.M.; Martinez, F.J. Severe COVID-19. N. Engl. J. Med. 2020, 383, 2451–2460. [Google Scholar] [CrossRef]
- The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 23 September 2021).
- Study Quality Assessment Tools|NHLBI, NIH. Available online: https://www.ncbi.nlm.nih.gov/pubmed/ (accessed on 25 September 2021).
- Lin, L.; Xu, C. Arcsine-based transformations for meta-analysis of proportions: Pros, cons, and alternatives. Health Sci. Rep. 2020, 3, e178. [Google Scholar] [CrossRef]
- Aghemo, A.; Piovani, D.; Parigi, T.L. COVID-19 Digestive System Involvement and Clinical Outcomes in a Large Academic Hospital in Milan, Italy. Clin. Gastroenterol. Hepatol. 2020, 18, 2366–2368. [Google Scholar] [CrossRef]
- An, P.; Chen, H.; Jiang, X. Clinical Features of 2019 Novel Coronavirus Pneumonia Presented Gastrointestinal Symptoms But Without Fever Onset. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Banno, A.; Hifumi, T.; Okamoto, H. Clinical characteristics and outcomes of critically ill COVID-19 patients in Tokyo: A single-center observational study from the first wave. BMC Infect. Dis. 2021, 21, 163. [Google Scholar] [CrossRef] [PubMed]
- Cai, Q.; Huang, D.; Ou, P. COVID-19 in a designated infectious diseases hospital outside Hubei Province, China. Allergy 2020, 75, 1742–1752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Utku, A.C.; Budak, G.; Karabay, O. Main symptoms in patients presenting in the COVID-19 period. Scott. Med. J. 2020, 65, 127–132. [Google Scholar] [CrossRef]
- Chang, D.; Lin, M.; Wei, L. Epidemiologic and Clinical Characteristics of Novel Coronavirus Infections Involving 13 Patients Outside Wuhan, China. JAMA 2020, 323, 1092. [Google Scholar] [CrossRef]
- Chen, A.; Agarwal, A.; Ravindran, N. Are Gastrointestinal Symptoms Specific for Coronavirus 2019 Infection? A Prospective Case-Control Study From the United States. Gastroenterology 2020, 159, 1161–1163. [Google Scholar] [CrossRef]
- Chen, Q.; Zheng, Z.; Zhang, C. Clinical characteristics of 145 patients with corona virus disease 2019 (COVID-19) in Taizhou, Zhejiang, China. Infection 2020, 48, 543–551. [Google Scholar] [CrossRef]
- Cheung, K.S.; Hung, I.F.N.; Chan, P.P.Y. Gastrointestinal Manifestations of SARS-CoV-2 Infection and Virus Load in Fecal Samples From a Hong Kong Cohort: Systematic Review and Meta-analysis. Gastroenterology 2020, 159, 81–95. [Google Scholar] [CrossRef]
- Cholankeril, G.; Podboy, A.; Aivaliotis, V.I. Association of Digestive Symptoms and Hospitalization in Patients With SARS-CoV-2 Infection. Am. J. Gastroenterol. 2020, 115, 1129–1132. [Google Scholar] [CrossRef]
- De Carvalho, H.; Richard, M.C.; Chouihed, T. Electrolyte imbalance in COVID-19 patients admitted to the Emergency Department: A case–control study. Intern. Emerg. Med. 2021, 16, 1945–1950. [Google Scholar] [CrossRef]
- Du, R.H.; Liu, L.M.; Yin, W. Hospitalization and Critical Care of 109 Decedents with COVID-19 Pneumonia in Wuhan, China. Ann. Am. Thorac. Soc. 2020, 17, 839–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duarte-Neto, A.N.; Monteiro, R.A.A.; Silva, L.F.F. Pulmonary and systemic involvement in COVID-19 patients assessed with ultrasound-guided minimally invasive autopsy. Histopathology 2020, 77, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Elmunzer, B.J.; Spitzer, R.L.; Foster, L.D. Digestive Manifestations in Patients Hospitalized With Coronavirus Disease 2019. Clin. Gastroenterol. Hepatol. 2020, 19, 1355–1365. [Google Scholar] [CrossRef] [PubMed]
- Ferm, S.; Fisher, C.; Pakala, T. Analysis of Gastrointestinal and Hepatic Manifestations of SARS-CoV-2 Infection in 892 Patients in Queens, NY. Clin. Gastroenterol. Hepatol. 2020, 18, 2378–2379. [Google Scholar] [CrossRef]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Hajifathalian, K.; Krisko, T.; Mehta, A. Gastrointestinal and Hepatic Manifestations of 2019 Novel Coronavirus Disease in a Large Cohort of Infected Patients From New York: Clinical Implications. Gastroenterology 2020, 159, 1137–1140. [Google Scholar] [CrossRef]
- Han, C.; Duan, C.; Zhang, S. Digestive Symptoms in COVID-19 Patients With Mild Disease Severity: Clinical Presentation, Stool Viral RNA Testing, and Outcomes. Am. J. Gastroenterol. 2020, 115, 916–923. [Google Scholar] [CrossRef]
- Han, J.; Gong, H.; Fu, L. Clinical and CT imaging features of SARS-CoV-2 patients presented with diarrhea. J. Infect. 2020, 81, e33–e35. [Google Scholar] [CrossRef]
- He, S.; Zhou, K.; Hu, M. Clinical characteristics of “re-positive” discharged COVID-19 pneumonia patients in Wuhan, China. Sci. Rep. 2020, 10, 17365. [Google Scholar] [CrossRef]
- Hu, C.; Li, J.; Xing, X. The effect of age on the clinical and immune characteristics of critically ill patients with COVID-19: A preliminary report. PLoS ONE 2021, 16, e0248675. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, J.G.; Hur, J.; Choi, E.Y. Prognostic Factors for Severe Coronavirus Disease 2019 in Daegu, Korea. J. Korean Med. Sci. 2020, 35, e209. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Han, C.; Bai, T. Gastroenterologists Reveal More Digestive Symptoms in COVID-19 Patients than Nongastroenterologists in Fever Clinic. Gastroenterol. Res. Pract. 2020, 2020, 8853922. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Lian, J.-S.; Hu, J.-H. Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut 2020, 69, 1002–1009. [Google Scholar] [CrossRef] [Green Version]
- Kang, M.K.; Kim, K.O.; Kim, M.C. Clinical characteristics of coronavirus disease 2019 patients with diarrhea in Daegu. Korean J. Intern. Med. 2020, 35, 1261–1269. [Google Scholar] [CrossRef]
- Kashefizadeh, A.; Ohadi, L.; Golmohammadi, M. Clinical features and short-term outcomes of COVID-19 in Tehran, Iran: An analysis of mortality and hospital stay. Acta Biomed. 2020, 91, e2020147. [Google Scholar]
- Kim, C.; Kim, W.; Jeon, J.H. COVID-19 infection with asymptomatic or mild disease severity in young patients: Clinical course and association between prevalence of pneumonia and viral load. PLoS ONE 2021, 16, e0250358. [Google Scholar] [CrossRef]
- Li, K.; Wu, J.; Wu, F. The Clinical and Chest CT Features Associated With Severe and Critical COVID-19 Pneumonia. Invest. Radiol. 2020, 55, 327–331. [Google Scholar] [CrossRef]
- Lin, L.; Jiang, X.; Zhang, Z. Gastrointestinal symptoms of 95 cases with SARS-CoV-2 infection. Gut 2020, 69, 997–1001. [Google Scholar] [CrossRef]
- Liu, K.; Fang, Y.Y.; Deng, Y. Clinical characteristics of novel coronavirus cases in tertiary hospitals in Hubei Province. Chin. Med. J. 2020, 133, 1025–1031. [Google Scholar] [CrossRef]
- Liu, Y.; Xiang, L.; Deng, K. Focusing on Gastrointestinal Symptoms in COVID-19 Is Far From Enough. Gastroenterology 2021, 160, 1429–1430. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Yang, Y.; Zhang, C. Clinical and biochemical indexes from 2019-nCoV infected patients linked to viral loads and lung injury. Sci. Chin. Life Sci. 2020, 63, 364–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo, I.L.; Lio, C.F.; Cheong, H.H. Evaluation of SARS-CoV-2 RNA shedding in clinical specimens and clinical characteristics of 10 patients with COVID-19 in Macau. Int. J. Biol. Sci. 2020, 16, 1698–1707. [Google Scholar] [CrossRef] [Green Version]
- Luan, Y.-Y.; Liu, Y.; Liu, X.-Y. Coronavirus disease 2019 (COVID-19) associated coagulopathy and its impact on outcomes in Shenzhen, China: A retrospective cohort study. Thromb. Res. 2020, 195, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Luo, S.; Deng, Z.; Zhang, X. Clinical characteristics and outcomes of 2019 novel coronavirus disease patients presenting with initial gastrointestinal symptoms in Wuhan, China: A retrospective cohort study. J. Gastroenterol. Hepatol. 2021, 36, 694–699. [Google Scholar] [CrossRef]
- Luo, S.; Zhang, X.; Xu, H. Don’t Overlook Digestive Symptoms in Patients With 2019 Novel Coronavirus Disease (COVID-19). Clin. Gastroenterol. Hepatol. 2020, 18, 1636–1637. [Google Scholar] [CrossRef]
- Ñamendys-Silva, S.A.; Alvarado-Ávila, P.E.; Domínguez-Cherit, G. Outcomes of patients with COVID-19 in the intensive care unit in Mexico: A multicenter observational study. Heart Lung 2021, 50, 28–32. [Google Scholar] [CrossRef]
- Ng, M.-Y.; Lee, E.Y.P.; Yang, J. Imaging Profile of the COVID-19 Infection: Radiologic Findings and Literature Review. Radiol. Cardiothorac. Imaging 2020, 2, e200034. [Google Scholar] [CrossRef] [Green Version]
- Nobel, Y.R.; Phipps, M.; Zucker, J. Gastrointestinal Symptoms and Coronavirus Disease 2019: A Case-Control Study From the United States. Gastroenterology 2020, 159, 373–375. [Google Scholar] [CrossRef]
- Pan, L.; Mu, M.; Yang, P. Clinical Characteristics of COVID-19 Patients With Digestive Symptoms in Hubei, China: A Descriptive, Cross-Sectional, Multicenter Study. Am. J. Gastroenterol. 2020, 115, 766–773. [Google Scholar] [CrossRef]
- Park, S.-K.; Lee, C.-W.; Park, D.-I. Detection of SARS-CoV-2 in Fecal Samples From Patients With Asymptomatic and Mild COVID-19 in Korea. Clin. Gastroenterol. Hepatol. 2020, 19, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Puah, S.H.; Young, B.E.; Chia, P.Y. Clinical features and predictors of severity in COVID-19 patients with critical illness in Singapore. Sci. Rep. 2021, 11, 7477. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, P.; Onukogu, I.; Ghanta, S. Gastrointestinal Symptoms and Outcomes in Hospitalized Coronavirus Disease 2019 Patients. Dig. Dis. 2020, 38, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Redd, W.D.; Zhou, J.C.; Hathorn, K.E. Prevalence and Characteristics of Gastrointestinal Symptoms in Patients With Severe Acute Respiratory Syndrome Coronavirus 2 Infection in the United States: A Multicenter Cohort Study. Gastroenterology 2020, 159, 765–767. [Google Scholar] [CrossRef]
- Remes-Troche, J.M.; Ramos-De-La-Medina, A.; Manríquez-Reyes, M. Initial Gastrointestinal Manifestations in Patients With Severe Acute Respiratory Syndrome Coronavirus 2 Infection in 112 Patients From Veracruz in Southeastern Mexico. Gastroenterology 2020, 159, 1179–1181. [Google Scholar] [CrossRef]
- Renelus, B.D.; Khoury, N.; Chandrasekaran, K. Hospitalized coronavirus disease-2019 (COVID-19) patients with gastrointestinal symptoms have improved survival to discharge. Dig. Liver Dis. 2020, 52, 1403–1406. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Han, X.; Jiang, N. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Shi, S.; Qin, M.; Shen, B. Association of Cardiac Injury With Mortality in Hospitalized Patients With COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802–810. [Google Scholar] [CrossRef] [Green Version]
- Shimamura, Y.; Masuda, K.; Anbo, Y. A single-center comparative analysis of outpatients with and without COVID-19 in Sapporo, Japan. J. Gen. Fam. Med. 2021, 23, 61–64. [Google Scholar] [CrossRef]
- Sim, B.L.H.; Chidambaram, S.K.; Wong, X.C. Clinical characteristics and risk factors for severe COVID-19 infections in Malaysia: A nationwide observational study. Lancet Reg. Health—West. Pac. 2020, 4, 100055. [Google Scholar] [CrossRef]
- Song, F.; Shi, N.; Shan, F. Emerging 2019 Novel Coronavirus (2019-nCoV) Pneumonia. Radiology 2020, 295, 210–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sulaiman, T.; Algharawi, A.A.; Idrees, M. The prevalence of gastrointestinal symptoms among patients with COVID -19 and the effect on the severity of the disease. JGH Open 2020, 4, 1162–1166. [Google Scholar] [CrossRef] [PubMed]
- Tu, Y.; Yang, P.; Zhou, Y. Risk factors for mortality of critically ill patients with COVID-19 receiving invasive ventilation. Int. J. Med. Sci. 2021, 18, 1198–1206. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Pan, M.; Zhang, X. Epidemiological and clinical features of 125 Hospitalized Patients with COVID-19 in Fuyang, Anhui, China. Int. J. Infect. Dis. 2020, 95, 421–428. [Google Scholar] [CrossRef]
- Wang, X.; Liu, W.; Zhao, J. Clinical characteristics of 80 hospitalized frontline medical workers infected with COVID-19 in Wuhan, China. J. Hosp. Infect. 2020, 105, 399–403. [Google Scholar] [CrossRef]
- Wang, Z.; Yang, B.; Li, Q. Clinical Features of 69 Cases With Coronavirus Disease 2019 in Wuhan, China. Clin. Infect. Dis. 2020, 71, 769–777. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.-H.; Shu, C.; Ran, X. Critically Ill Patients with Coronavirus Disease 2019 in a Designated ICU: Clinical Features and Predictors for Mortality. Risk Manag. Healthc. Policy 2020, 13, 833–845. [Google Scholar] [CrossRef]
- Wei, X.-S.; Wang, X.; Niu, Y.-R. Diarrhea Is Associated With Prolonged Symptoms and Viral Carriage in Corona Virus Disease 2019. Clin. Gastroenterol. Hepatol. 2020, 18, 1753–1759. [Google Scholar] [CrossRef]
- Wolday, D.; Gebrecherkos, T.; Arefaine, Z.G. Effect of co-infection with intestinal parasites on COVID-19 severity: A prospective observational cohort study. EClinicalMedicine 2021, 39, 101054. [Google Scholar] [CrossRef]
- Wu, J.; Liu, J.; Zhao, X. Clinical Characteristics of Imported Cases of Coronavirus Disease 2019 (COVID-19) in Jiangsu Province: A Multicenter Descriptive Study. Clin. Infect. Dis. 2020, 71, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Wu, X.; Zeng, W.; Chest, C.T. Findings in Patients With Coronavirus Disease 2019 and Its Relationship With Clinical Features. Invest. Radiol. 2020, 55, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Xia, P.; Wen, Y.; Duan, Y. Clinicopathological Features and Outcomes of Acute Kidney Injury in Critically Ill COVID-19 with Prolonged Disease Course: A Retrospective Cohort. J. Am. Soc. Nephrol. 2020, 31, 2205–2221. [Google Scholar] [CrossRef]
- Xiao, F.; Tang, M.; Zheng, X. Evidence for Gastrointestinal Infection of SARS-CoV-2. Gastroenterology 2020, 158, 1831–1833. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Huang, S.; Yan, L. Clinical characteristics of diarrhea in 90 cases with COVID-19: A descriptive study. Int. Emerg. Nurs. 2020, 52, 100912. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Yu, C.; Qu, J. Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1275–1280. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.-W.; Wu, X.-X.; Jiang, X.-G. Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-CoV -2) outside of Wuhan, China: Retrospective case series. BMJ 2020, 368, m792. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.; Cao, Q.; Qin, L. Clinical characteristics and imaging manifestations of the 2019 novel coronavirus disease (COVID-19):A multi-center study in Wenzhou city, Zhejiang, China. J. Infect. 2020, 80, 388–393. [Google Scholar] [CrossRef] [Green Version]
- Zg, F.Z.; Tang, W. Clinical characteristics of 161 cases of corona virus disease 2019 (COVID-19) in Changsha. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 3404–3410. [Google Scholar]
- Zhang, G.; Hu, C.; Luo, L. Clinical features and short-term outcomes of 221 patients with COVID-19 in Wuhan, China. J. Clin. Virol. 2020, 127, 104364. [Google Scholar] [CrossRef]
- Zhang, J.-J.; Dong, X.; Cao, Y.-Y. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; He, Z.; Yu, G. The modified NUTRIC score can be used for nutritional risk assessment as well as prognosis prediction in critically ill COVID-19 patients. Clin. Nutr. 2021, 40, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.; Xu, Y.; Li, J. Sex differences in immune responses to SARS-CoV-2 in patients with COVID-19. Biosci. Rep. 2021, 41, BSR20202074. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Zhong, Z.; Xie, X. Relation Between Chest CT Findings and Clinical Conditions of Coronavirus Disease (COVID-19) Pneumonia: A Multicenter Study. Am. J. Roentgenol. 2020, 214, 1072–1077. [Google Scholar] [CrossRef]
- Zhao, X.-Y.; Xu, X.-X.; Yin, H.-S. Clinical characteristics of patients with 2019 coronavirus disease in a non-Wuhan area of Hubei Province, China: A retrospective study. BMC Infect. Dis. 2020, 20, 311. [Google Scholar] [CrossRef]
- Zheng, M.; Gao, Y.; Wang, G. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell. Mol. Immunol. 2020, 17, 533–535. [Google Scholar] [CrossRef] [Green Version]
- Zheng, T.; Yang, C.; Wang, H.Y. Clinical characteristics and outcomes of COVID-19 patients with gastrointestinal symptoms admitted to Jianghan Fangcang Shelter Hospital in Wuhan, China. J. Med. Virol. 2020, 92, 2735–2741. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Zhou, Z.; Zhao, N.; Shu, Y. Effect of Gastrointestinal Symptoms in Patients With COVID-19. Gastroenterology 2020, 158, 2294–2297. [Google Scholar] [CrossRef]
- Lee, D.S.; Kim, J.W.; Lee, K.L. Significance of digestive symptoms after COVID-19 vaccination: A retrospective single-center study. Am. J. Emerg. Med. 2022, 58, 154–158. [Google Scholar] [CrossRef]
- Zhao, W.; Li, Y.; Xie, R. Real-World Evidence for COVID-19 Delta Variant’s Effects on the Digestive System and Protection of Inactivated Vaccines from a Medical Center in Yangzhou, China: A Retrospective Observational Study. Int. J. Clin. Pract. 2022, 2022, 7405448. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Song, Z.-G.; Liu, C. Gut microbiome alterations and gut barrier dysfunction are associated with host immune homeostasis in COVID-19 patients. BMC Med. 2022, 20, 24. [Google Scholar] [CrossRef] [PubMed]
- Delavari, A.; Asgari, S.; Alimohamadi, Y. Gastrointestinal symptoms are associated with a lower risk of hospitalization and mortality and outcomes in COVID-19. BMC Gastroenterol. 2022, 22, 119. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Ning, M.; Feng, Y. The early stage of COVID-19 pandemic: Gastrointestinal manifestations and liver injury in COVID-19 patients in Wuhan, China. Front. Med. 2022, 9, 997000. [Google Scholar] [CrossRef] [PubMed]
- Belabbes, F.Z.; Maizi, M.; Belghyti, N. Prevalence and Severity of Gastrointestinal Symptoms in COVID-19 Patients in Casablanca: A Retrospective Cohort Study. Cureus 2022, 14, e27815. [Google Scholar] [CrossRef]
- Yang, X.; Zhao, J.; Yan, Q. A case of COVID-19 patient with the diarrhea as initial symptom and literature review. Clin. Res. Hepatol. Gastroenterol. 2020, 44, e109–e112. [Google Scholar] [CrossRef]
- Malik, J.A.; Ahmed, S.; Yaseen, Z. Association of SARS-CoV-2 and Polypharmacy with Gut–Lung Axis: From Pathogenesis to Treatment. ACS Omega 2022, 7, 33651–33665. [Google Scholar] [CrossRef]
- Booth, A.; Reed, A.B.; Ponzo, S. Population risk factors for severe disease and mortality in COVID-19: A global systematic review and meta-analysis. PLoS ONE 2021, 16, e0247461. [Google Scholar] [CrossRef]
- Hu, J.; Wang, Y. The Clinical Characteristics and Risk Factors of Severe COVID-19. Gerontology 2021, 67, 255–266. [Google Scholar] [CrossRef]
- Cha, M.H.; Regueiro, M.; Sandhu, D.S. Gastrointestinal and hepatic manifestations of COVID-19: A comprehensive review. World J. Gastroenterol. 2020, 26, 2323–2331. [Google Scholar] [CrossRef]
- Fang, D.; Ma, J.; Guan, J.; Wang, M.; Song, Y.; Tian, D.; Li, P. Manifestations of digestive system of hospitalized patients with coronavirus disease 2019 in Wuhan, China: A single-center descriptive study. Zhonghua Xiaohua Zazhi. Chin. J. Dig. 2020, 12, 151–156. [Google Scholar]
- D’Amico, F.; Baumgart, D.C.; Danese, S. Diarrhea During COVID-19 Infection: Pathogenesis, Epidemiology, Prevention, and Management. Clin. Gastroenterol. Hepatol. 2020, 18, 1663–1672. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.; Alqusairi, R.; Adams, A. SARS-CoV-2 Gastrointestinal Infection Causing Hemorrhagic Colitis: Implications for Detection and Transmission of COVID-19 Disease. Am. J. Gastroenterol. 2020, 115, 942–946. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Kang, Z.; Gong, H. Digestive system is a potential route of COVID-19: An analysis of single-cell coexpression pattern of key proteins in viral entry process. Gut 2020, 69, 1010–1018. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.; Liu, P.; Shi, X.L. SARS-CoV-2 induced diarrhoea as onset symptom in patient with COVID-19. Gut 2020, 69, 1143–1144. [Google Scholar] [CrossRef] [Green Version]
- Wan, Y.; Li, J.; Shen, L. Enteric involvement in hospitalised patients with COVID-19 outside Wuhan. Lancet Gastroenterol. Hepatol. 2020, 5, 534–535. [Google Scholar] [CrossRef]
- Kaur, R.J.; Charan, J.; Dutta, S. Favipiravir Use in COVID-19: Analysis of Suspected Adverse Drug Events Reported in the WHO Database. Infect. Drug Resist. 2020, 13, 4427–4438. [Google Scholar] [CrossRef]
- Grein, J.; Ohmagari, N.; Shin, D. Compassionate Use of Remdesivir for Patients with Severe COVID-19. N. Engl. J. Med. 2020, 382, 2327–2336. [Google Scholar] [CrossRef]
- Rusu, A.; Arbănaşi, E.-M.; Lungu, I.-A. Perspectives on Antiviral Drugs Development in the Treatment of COVID-19. Acta Biol. Marisiensis 2021, 4, 44–59. [Google Scholar] [CrossRef]
- Painter, W.P.; Holman, W.; Bush, J.A. Human Safety, Tolerability, and Pharmacokinetics of Molnupiravir, a Novel Broad-Spectrum Oral Antiviral Agent with Activity Against SARS-CoV-2. Antimicrob. Agents Chemother. 2021, 65, e02428-20. [Google Scholar] [CrossRef]
- Gottlieb, R.L.; Nirula, A.; Chen, P. Effect of Bamlanivimab as Monotherapy or in Combination With Etesevimab on Viral Load in Patients With Mild to Moderate COVID-19. JAMA 2021, 325, 632–644. [Google Scholar] [CrossRef]
- Graham, M.S.; Sudre, C.H.; May, A. Changes in symptomatology, reinfection, and transmissibility associated with the SARS-CoV-2 variant B.1.1.7: An ecological study. Lancet Public Health 2021, 6, e335–e345. [Google Scholar] [CrossRef] [PubMed]
- Williams, H.; Hutchinson, D.; Stone, H. Watching Brief: The evolution and impact of COVID-19 variants B. 1.1. 7, B. 1.351, P. 1 and B. 1.617. Glob. Biosecurity 2021, 3. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, R.; Hu, F. Transmission, viral kinetics and clinical characteristics of the emergent SARS-CoV-2 Delta VOC in Guangzhou, China. EClinicalMedicine 2021, 40, 101129. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Studies that included case-controls, cohorts, cross-sectional and prospective studies | Children, adolescents and pregnant women |
| Literature search on electronic databases, namely PubMed, PubMed Central, Embase, Scopus, Cochrane library and ProQuest (from 1 January 2020 and last updated on 20 October 2022) by using search terms that included ‘SARCOV-2′, ‘COVID-19′, ‘gastrointestinal symptoms’, ‘diarrhoea’ and ‘nCoV’ | Articles that did not provide information on gastrointestinal symptoms |
| Articles reporting gastrointestinal symptoms associated with the COVID-19 infection that included diarrhoea, nausea, vomiting, abdominal pain and loss of appetite | Case reports, preprints, no full-text articles and no availability of the diarrhoea-associated data |
| Studies comparing severe versus non-severe diarrhoea | No relevant data |
| A patient who met the definition of severe disease as follows: (i) dyspnoea present, (ii) a respiratory rate: 30 or >breaths per minute, (iii) blood oxygen saturation: 93% or less, (iv) ratio of the partial pressure of arterial oxygen to the fraction of inspired oxygen (PaO2:FiO2): <300 mm Hg, (v) infiltrates in more than 50% of lung field, (vi) patient under mechanical ventilation and ICU (intensive care unit) admitted, (vii) APACHE II and SOFA scores higher for critically ill patients with COVID-19 infection, (viii) hyponatraemia or hypokalaemia |
| Authors | Date/Year of Publication | Study Design | Country | Sample Size N (%) | Age, Mean ±SD/Median (IQR) | Male N (%) | Female N (%) | GI Symptoms N (%) | Diarrhoea N (%) | Abdominal Pain N (%) | Nausea or Vomiting N (%) | Loss of Appetite N (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chang D, et al. [17] | March 2020 | Case series | China | 11 | 34 (34–48) | 10 | NA | 1 (7.6) | 1 (7.7) | NA | NA | NA |
| Xiong Y, et al. [74] | 22 February 2020 | Retrospective | China | 35 | 49.5 ± 14.1 | 25 (60) | NA | 10/42 (24) | 10 (24) | NA | NA | NA |
| Liu K, et al. [42] | 29 January 2020 | Retrospective | China | 137 | 57 (20–83) | 61 (44.5) | 76 (55.5) | 11 (8.0) | 11 (8.0) | NA | NA | NA |
| Guan W, et al. [27] | 28 February 2020 | Multicentre | China | 1099 | 47.0 (35.0–58.0) | 640 | 459/1096 (41.9) | ≥55 (5.0) | 42 (3.8) | NA | 55(5.0) | NA |
| Han C, et al. [29] | 31 March 2020 | Retrospective | China | 206 | 62.5 (27–92) | 91 | 115 | 117 (56.7) | 67 (32.5) | 9 (4.4) | 24 (11.7) | 102 (49.5) |
| Huang C, et al. [33] | 24 January 2020 | Prospective | China | 41 | 49.0 (41.0–58.0) | 30 (73) | 11 (27) | 1 (3.0) | 1/38 (3) | NA | NA | NA |
| Jin X, et al. [36] | 24 March 2020 | Retrospective | China | 74 | 46.14 ± 14.19 | 37 (50.0) | 74 | 74 (100) | 53 (71.62) | NA | NA | NA |
| Liu Y, et al. [44] | 9 February 2020 | Case series | China | 12 | 54.34 ± 18.011 | 8 (66.6) | 4 (33.33) | 2 (16.67) | 2 (16.67) | NA | 2 (16.67) | NA |
| Luan Y, et al. [46] | 9 July 2020 | Retrospective | China | 117 | 61.9 ± 17.9 | 62 (53.0) | 55 (47.0) | ≥8 (6.87) | 8 (6.8) | 1 (0.9) | 5(4.2) | 8 (6.8) |
| Luo S, et al. [48] | 20 March 2020 | Retrospective | China | 183 | 53.8 | 102 (56) | 81 (44) | 183 (100) | 68 (37) | 45 (25) | 37 (20) | 180 (98) |
| Ng Y, et al. [50] | 13 February 2020 | Retrospective | China | 21 | 56 (37–65) | 13 (62) | 8 (38) | 2 (9.5) | 2 (10) | NA | NA | NA |
| Pan L, et al. [52] | 14 April 2020 | Cross- sectional | China | 204 | 52.91 ± 15.98 | 107 (52.45) | 97 (47.54) | 103 (50.04) | 35 (33.98) | 2 (1.94) | 4 (3.88) | 81 (78.64) |
| Shi S, et al. [60] | 25 March 2020 | Retrospective, cohort | China | 416 | 64 (21–95) | 205 (49.27) | 211 (50.7) | 16 (3.8) | 16 (3.8) | NA | NA | NA |
| Shi H, et al. [59] | 24 February 2020 | Retrospective | China | 81 | 49.5 (11.0) | 42 (52) | 39 (38) | 4 (4.9) | 3 (4) | NA | 4 (5) | 1 (1) |
| Song F, et al. [63] | 6 February 2020 | Retrospective | China | 51 | 49 ± 16 | 25 (49) | 26 (51) | 5 (9.82) | 5 (10) | NA | 3 (6) | 9 (18) |
| An P, et al. [13] | 6 February 2020 | Retrospective | China | 9 | 35.8 (28–45) | 4 (44.44) | 5 (55.56) | 9 (100) | 1 (11.1) | 0 | 2 (22) | 6 (66.7) |
| Li K, et al. [40] | 29 February 2020 | Retrospective | China | 83 | 45.5 ± 12.3 | 44 (53.0) | 39 (47.0) | 7 (8.4) | 7 (8.4) | 7 (8.4) | NA | NA |
| Wang D, et al. [66] | 7 February 2020 | Retrospective, case series | China | 138 | 56 (42–68) | 75 (54.3) | 63 (45.7) | 55 (39.9) | 14 (10.1) | 3 (2.2) | 5 (3.6) | 55 (39.9) |
| Wang Z, et al. [69] | 16 March 2020 | Retrospective | China | 69 | 42.0 (35.0–62.0) | 32 (46) | 37 (54) | 10 (14.49) | 10 (14) | NA | 3 (4) | 7 (10) |
| Wu J, et al. [73] | 29 February 2020 | Retrospective | China | 80 | 46.1 ± 15.42 | 39 (48.75) | 41 (51.25) | 1 (1.25) | 1 (1.25) | NA | 1 (1.25) | NA |
| Xia P, et al. [75] | 31 September 2020 | Retrospective, cohort | China | 81 | 66.6 ± 11.4 | 54 (66.7) | 27 (33.3) | 26 (32.1) | 20 (24.7) | NA | 8 (9.9) | 26 (32.1) |
| Xiao F, et al. [76] | 3 March 2020 | Case series | China | 73 | 43 (0.83–7) | 41 (56.16) | 32 (43.83) | 26 (35.61) | 26 (35.61) | NA | NA | NA |
| Xu X-W, et al. [79] | 19 February 2020 | Retrospective, case series | China | 62 | 41 (32–52) | 35 (56) | 27 (44) | 3 (8) | 3 (8) | NA | NA | NA |
| Xu X, et al. [78] | 28 February 2020 | Retrospective | China | 90 | 50 (18–86) | 39 (43) | 51 (57) | 5 (6) | 5 (6) | NA | 5 (6) | NA |
| Zhang J, et al. [83] | 19 February 2020 | Retrospective | China | 140 | 57 (25–87) | 71 (50.7) | 69 (49.3) | 55/139 (39.6) | 18/139 (12.9) | 8/139 (5.8) | 24/139 (17.3) | 17/139 (12.2) |
| Zhang P, et al. [84] | 4 June 2020 | Retrospective | China | 136 | 69 (57–77) | 86 (63) | 50 (37) | 28 (21.0) | 28 (21.0) | NA | NA | NA |
| Zhao W, et al. [86] | 3 March 2020 | Retrospective | China | 101 | 44.44 (17–75) | 56 (55.4) | 45 (44.6) | 3 (3.0) | 3 (3.0) | NA | 2 (2.0) | NA |
| Zhao G, et al. [85] | 29 January 2021 | Retrospective | China | 36 | 51.24 | 13 (36.1) | 23 (63.8) | 6 (16.6) | 6 (16.6) | NA | NA | NA |
| Zheng M, et al. [88] | 19 March 2020 | Cohort | China | 68 | 47.13 (11–84) | 36 (52.94) | 32 (47.06) | 3 (4.41) | 3 (4.41) | NA | NA | NA |
| Zhou F, et al. [90] | 11 March 2020 | Retrospective, cohort | China | 191 | 56.0 (46.0–67.0) | 119 (62) | 72 (38) | 9 (4.71) | 9 (5.0) | NA | 7 (4.0) | NA |
| Zhou Z, et al. [91] | 18 March 2020 | Retrospective | China | 254 | 50 (36–65) | 115 (45.3) | 139 (54.7) | 66 (25.9) | 46 (18.1) | 3 (1.2) | 36 (14.17) | NA |
| Yang W, et al. [80] | 26 February 2020 | Retrospective, cohort | China | 149 | 45.11 ± 13.35 | 81 (54.36) | 68 (45.63) | 11 (7.38) | 11 (7.38) | NA | 2 (1.34) | NA |
| Zhang G, et al. [82] | 9 April 2020 | Retrospective, case series | China | 221 | 55.0 (39.0–66.5) | 108 (48.9) | 113 (51.1) | 80 (36.19) | 25 (11.3) | 5 (2.3) | NA | 80 (36.2) |
| Wang R, et al. [67] | 24 March 2020 | Retrospective, descriptive | China | 125 | 38.76 ± 13.799 | 71 (56.8) | 54 (43.2) | 50 (40.0) | 50 (40.0) | NA | 24 (19.2) | NA |
| Du R, et al. [23] | 7 April 2020 | Retrospective | China | 109 | 70.7 ± 10.9 | 74 (67.88) | 35 (32.1) | 29 (26.6) | 29 (26.6) | NA | NA | NA |
| Zheng T, et al. [89] | 4 June 2020 | Retrospective | China | 1320 | 50 (40–57) | 579 (43.9) | 741 (56.1) | 192 (14.54) | 107 (8.1) | 11 (0.8) | 57 (4.3) | 62 (4.7) |
| Zhao X, et al. [87] | 29 April 2020 | Retrospective | China | 91 | 46.0 | 49 (53.8) | 42 (46.2) | 19 (12.1) | 14 (15.4) | 2 (2.2) | 19 (12.1) | 11 (12.1) |
| Zhang J-J, et al. [83] | 18 February 2020 | Retrospective | China | 140 | 57 (25–87) | 71 (50.7) | 69 (49.3) | 31 (22.3) | 18 (12.9) | 8 (5.8) | 31 (22.3) | 17 (12.2) |
| Xiao Y, et al. [77] | 5 August 2020 | Descriptive | China | 90 | 61.0 (48.3–69.0) | 51 (57) | 39 (43) | 37 (41.1) | 8 (9.0) | 6 (7.0) | 37 (41.1) | 22 (24) |
| Wei X, et al. [71] | 18 July 2020 | Retrospective, single centre | China | 84 | 37 (24–74) | 28 (33) | 56 (66.6) | 26 (30.9) | 26 (30.9) | 2 (2) | 22 (26.1) | NA |
| Han J, et al. [30] | 5 August 2020 | Retrospective | China | 120 | 45.4 (15.6) | 43 (36) | 77 (64.17) | 7 (5.83) | 7 (5.83) | NA | NA | NA |
| Jiang Y, et al. [35] | 7 December 2020 | Retrospective | China | 495 | 42.24 ± 16.99 | 515 (41.5) | 723 (58.4) | 76 (15.3) | 29 (5.85) | 10 (2.02) | 35 (7.0) | 7 (1.4) |
| Lin L, et al. [41] | 2 April 2020 | Retrospective | China | 95 | 45.3 ± 18.3 | 45 (47.4) | 50 (52.6) | 58 (61) | 23 (24.2) | NA | 17 (17.9) | 17 (17.9) |
| Liu Y, et al. [43] | 18 May 2020 | Retrospective | China | 148 | 56.5 ± 15.2 | 67 (45.2) | 81 (54.7) | 42 (28.3) | 18 (12.16) | 2 (1.34) | 4 (2.7) | 27 (18.2) |
| Luo S, et al. [47] | 23 July 2020 | Retrospective cohort | China | 183 | NA | 102 (55.7) | 81 (44.2) | 183 (100) | 68 (37.1) | 65 (35.5) | 119 (65.0) | 180 (98.3) |
| Wang X, et al. [68] | 14 April 2020 | Retrospective | China | 80 | 39 (32–48.5) | 31 (38.75) | 49 (61.25) | 15 (18.75) | 15 (18.75) | NA | NA | NA |
| Chen Q, et al. [19] | 28 April 2020 | Retrospective, single centre | China | 145 | 47.5 ± 14.6 | 79 (54.5) | 66 (45.5) | 62 (42.75) | 39 (26.8) | 8 (5.5) | 30 (20.6) | 62 (42.75) |
| He S, et al. [31] | 15 October 2020 | Retrospective | China | 267 | 57 (37–68) | 116 (43) | 151 (56.5) | 20 (7) | 20 (7) | NA | NA | NA |
| Hu C, et al. [32] | 18 March 2021 | Retrospective | China | 32 | NA | 17 (53.1) | 15 (46.8) | 3 (9.4) | 3 (9.4) | NA | NA | NA |
| Tu Y, et al. [65] | 11 January 2021 | Retrospective | China | 74 | 68.0 (61.5–74.0) | 53 (71.6) | 21 (28.3) | 24 (32.4) | 24 (32.4) | 2 (2.7) | 5 (6.8) | NA |
| Wang Z H, et al. [70] | 20 July 2020 | Retrospective | China | 59 | 67.4 ± 11.3 | 38 (64.4) | 21 (35.6) | 22 (37.3) | 22 (37.3) | NA | 4 (6.8) | 11 (18.6) |
| Zheng F, et al. [81] | 10 April 2020 | Retrospective | China | 161 | 45 (33.5–57) | 80 (49.7) | 81 (50.3) | 17 (10.6) | 17 (10.6) | NA | 6 (3.7) | NA |
| Cai Q, et al. [15] | 2 April 2020 | Retrospective | China | 298 | 47.5 (33–61) | 145 (48.6) | 153 (51.3) | 9 (3.02) | 9 (3.02) | NA | NA | NA |
| Duarte-Neto A, et al. [24] | 22 May 2020 | Case Series | Brazil | 10 | 63 (33–83) | 5 (50) | 5 (50) | 2 (20) | 2 (20) | NA | NA | NA |
| Redd W, et al. [56] | 22 April 2020 | Multicentre, cohort | USA | 318 | 63.4 ± 16.6 | 174 (54.7) | 144 (45.3) | 195 (61.3) | 107 (33.7) | 46 (14.5) | 95 (29.8) | 110 (34.8) |
| Chen A, et al. [18] | 15 May 2020 | Prospective, case–control | USA | 340 | 46.89 ± 15.34 | 96 (28) | 244 (71.7) | 201 (59) | 123 (36) | 72 (21) | 135 (39.7) | 117 (34) |
| Cholankeril G, et al. [21] | 28 April 2020 | Retrospective | USA | 207 | 49 (34–65) | 104 (50.2) | 103 (49.8) | 70 (34.5) | 22 (10.8) | 14 (7.1) | 22 (10.8) | NA |
| Ramchandran P, et al. [55] | 29 June 2020 | Retrospective, cohort | USA | 31 | 57.6 ± 17.2 | 19 (61.2) | 12 (38.7) | 31 (20.6) | 15 (10) | NA | 6 (4) | NA |
| Nobel Y, et al. [51] | 12 April 2020 | Retrospective, case–control | USA | 278 | NA | 145 (52) | 133 (48) | 97 (34.8) | 56 (22.31) | NA | 63 (25.09) | NA |
| Elmunzer B, et al. [25] | 30 September 2020 | Observational, cohort | USA | 1992 | 60.1 ± 16.3 | 1128 (56.6) | 864 (43.4) | 1052 (53) | 679 (34) | 220 (11) | 539 (27) | NA |
| Ferm S, et al. [26] | 1 June 2020 | Retrospective | USA | 892 | 59 (47–72) | 534 (59.8) | 358 (40.1) | 219 (24.6) | 177 (19.8) | 70 (7.8) | 148 (16.6) | 105 (11.8) |
| Renelus B, et al. [58] | 4 September 2020 | Retrospective | USA | 734 | 66.1 ± 15.6 | 379 (51.6) | 355 (48.4) | 231 (31.5) | 149 (20.3) | 68 (9.26) | 109 (14.9) | NA |
| Kang M, et al. [37] | 13 July 2020 | Retrospective | South Korea | 118 | 61 (50–70) | 52 (44.1) | 66 (55.9) | 54 (45.8) | 54 (45.8) | NA | NA | NA |
| Banno A, et al. [14] | 9 February 2021 | Retrospective, observational | Japan | 24 | 57.5 (49–68.8) | 19 (79) | 5 (20.8) | 6 (25) | 6 (25) | NA | NA | NA |
| Remes-Troche J, et al. [57] | 21 May 2020 | Cohort | Mexico | 112 | 43.72 ± 15 | 81 (72.3) | 31 (27.7) | 23 (20.5) | 20 (17.8) | 11 (9.8) | 8 (7.1) | NA |
| Namendys-Silva S, et al. [49] | 21 October 2020 | Multicentre observational | Mexico | 164 | 57.3 ± 13.7 | 114 (69.5) | 50 (30.4) | 29 (17.6) | 29 (17.6) | NA | NA | NA |
| Sulaiman T, et al. [64] | 18 September 2020 | Retrospective | Iraq | 140 | 44.99 ± 16.81 | 100 (71.42) | 40 (28.57) | 78 (55.7) | 41 (29.28) | 42 (30) | 31 (22.14) | 40 (28.57) |
| Wolday D, et al. [72] | 14 July 2021 | Prospective, cohort | Ethiopia | 751 | 37 (28-50) | 480 (63.9) | 14 (1.9) | 76 (10.9) | 39 (5.2) | 44 (5.9) | 76 (10.9) | NA |
| Aumpan N, et al. [6] | 6 July 2020 | Retrospective | Thailand | 40 | 30.5 ± 9.2 | 18 (45) | 22 (55) | 12 (30) | 6 (15) | 2 (5) | 2 (5) | 7 (17.5) |
| Puah S, et al. [54] | 5 April 2021 | Prospective, multicentre | Singapore | 60 | 44 (41–47) | 37 (62) | 23 (38.3) | 10 (17) | 10 (17) | NA | NA | NA |
| Jang J, et al. [34] | 2 June 2020 | Retrospective | South Korea | 110 | 56.9 ± 17.0 | 48 (43.6) | 62 (56.4) | 11 (10) | 11 (10.0) | NA | 3 (2.7) | NA |
| Cheung K, et al. [20] | 3 April 2020 | Retrospective | Hong Kong | 59 | 58.5 (43.5–68) | 27 (45.7) | 32 (54.2) | 15 (25.42) | 13 (22.0) | 7 (11.9) | 1 (1.7) | NA |
| Carvalho H, et al. [22] | 4 January 2021 | Case–control | France | 1,188 | 65 (51.5–76) | 663 (55.8) | 524 (44.2) | 202 (17.0) | 202 (17.0) | NA | 137 (10.6) | NA |
| Aghemo A, et al. [12] | 10 May 2020 | Retrospective | Italy | 292 | 65 ± 14.1 | 199 (68.2) | 93 (31.8) | 69/245 (28.2) | 69/255 (27.1) | NA | 11/274 (4.0) | NA |
| Park S, et al. [53] | 10 June 2020 | Prospective | South Korea | 46 | 26 (18–57) | 21 (45.6) | 25 (54.3) | 16 (34.7) | 7 (15.2) | 5 (10.8) | 1 (2.1) | 1 (2.2) |
| Lo I, et al. [45] | 15 March 2020 | Retrospective | Macau | 10 | 54 (27–64) | 3 (30) | 7 (70) | 8 (80) | 8 (80) | 2 (20) | 5 (50) | NA |
| Kashefizadeh A, et al. [38] | 10 November 2020 | Retrospective | Iran | 53 | 58.4 ± 13.0 | 24 (45.3) | 29 (54.7) | 49 (80.8) | 32 (61.5) | 49 (80.8) | 40 (76.9) | 20 (38.5) |
| Hajifathalian K, et al. [28] | 7 May 2020 | Retrospective | USA | 1059 | 61.1 ± 18.3 | 611 (57.7) | 448 (42.3) | 827 (78) | 234 (22.1) | 72 (6.8) | 168 (15.9) | NA |
| Utku A, et al. [16] | 17 August 2020 | Cohort | Turkey | 143 | 55.63 (mean) | 77 (53.8) | 66 (46.1) | 31 (21.7) | 31 (21.7) | NA | NA | NA |
| Kim C, et al. [39] | 21 April 2021 | Retrospective | South Korea | 106 | 28 ± 9.3 | 46 (43.4) | 60 (56.6) | 7 (6.6) | 7 (6.6) | NA | NA | NA |
| Shimamura Y, et al. [61] | 16 July 2021 | Retrospective | Japan | 315 | 60 (41–74) | 179 (57) | 136 (43.1) | 45 (14.0) | 45 (14) | 45 (14) | 5 (2) | 30 (10) |
| Sim B, et al. [62] | 17 November 2020 | Observational | Malaysia | 5889 | 34.0 (24–51) | 4221 (71.7) | 1,668 (28.3) | 298 (5.1) | 298 (5.1) | NA | 108 (1.8) | NA |
| Zhao W, et al. [93] | 19 August 2022 | Retrospective | China | 208 | 53.5 ± 20.9 | 90 (44) | 118 (56) | 24 (12) | 24 (12) | 17 (8) | 15 (7) | NA |
| Lee D-S, et al. [92] | 25 May 2022 | Retrospective | South Korea | 46 | 60 (56–74) | 22 (47.8) | 24 (52.9) | 25 (54) | 25 (54) | 28 (60.8) | 11 (23.9) | NA |
| Delavari A, et al. [95] | 10 March 2022 | Retrospective | Iran | 42,964 | 51.36 ± 19.61 | 22,854 (53.2) | 20,110 (46.8) | 6356 (14.7) | 1198 (2.78) | 688 (1.60) | 1781 (4.14) | 1,638 (3.81) |
| Belabbes F-Z, et al. [97] | 9 September 2022 | Retrospective, cohort | Morocco | 154 | NA | 85 (55.2) | 69 (44.2) | 24 (15.6) | 24 (15.6) | 9 (5.8) | 8 (5.2) | 5 (3.3) |
| Sun Z, et al. [94] | 20 January 2022 | Retrospective | China | 63 | 48.0 ± 21.2 | 39 (61.9) | 24 (38.2) | 9 (14.3) | 9 (14.3) | NA | NA | NA |
| Chen D, et al. [96] | 20 October 2022 | Observational, cross-sectional | China | 93 | 58.0 ± 12.1 | 46 (49.4) | 47 (50.6) | 65 (69.5) | 27 (29.3) | NA | 26 (27.7) | 63 (67.9) |
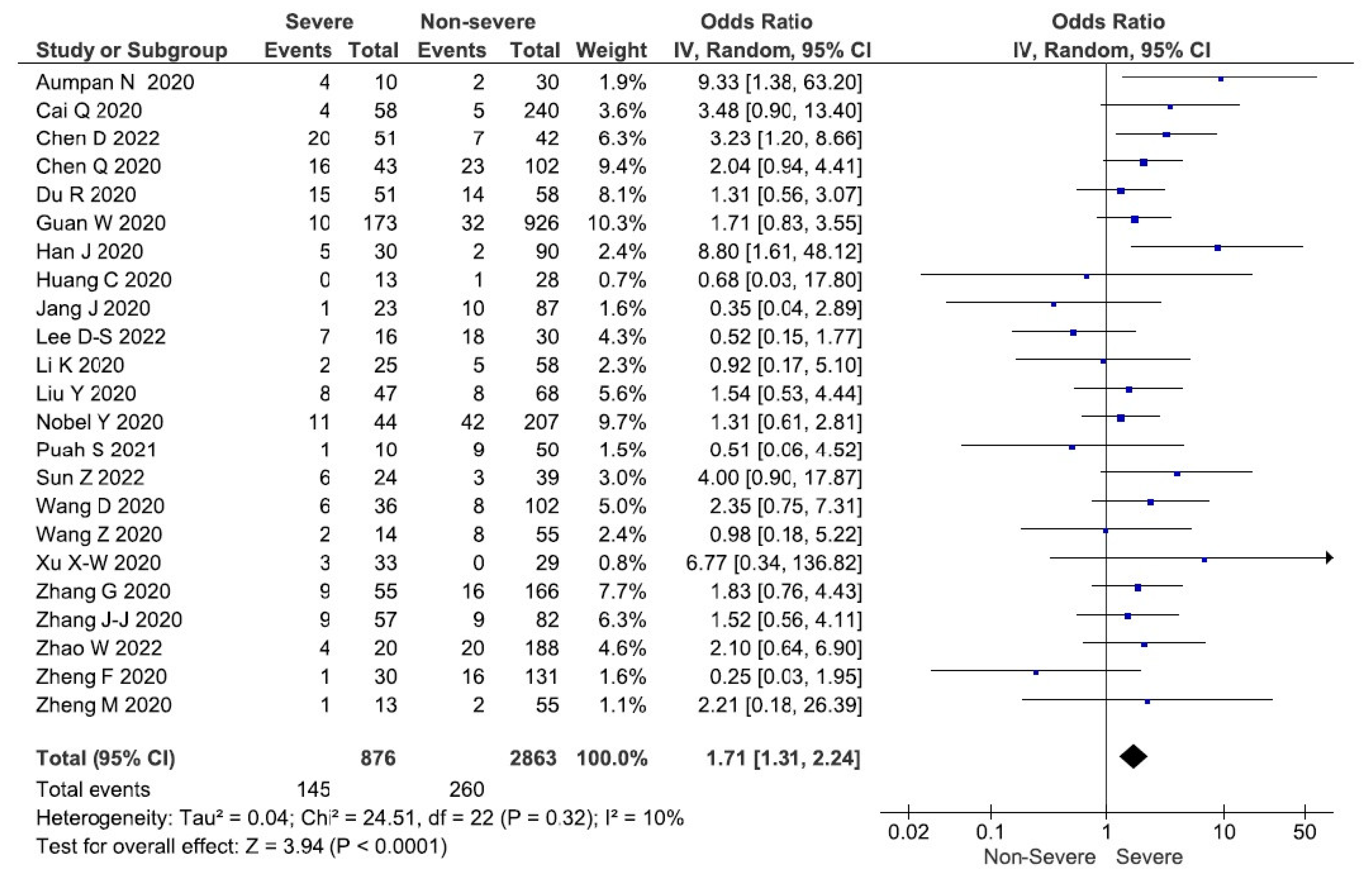
| Authors | Date/Year of Publication | Study Site | Sample Size | Diarrhoea (N) | Severe Diarrhoea | Severe Total | Non-Severe Diarrhoea | Non-Severe Total | Comparison |
|---|---|---|---|---|---|---|---|---|---|
| Guan W, et al. [27] | 28 February 2020 | China | 1099 | 42 | 10 | 173 | 32 | 926 | Severe vs. non-severe |
| Li K, et al. [40] | 29 February 2020 | China | 83 | 7 | 2 | 25 | 5 | 58 | Severe vs. non-severe |
| Wang D, et al. [66] | 7 February 2020 | China | 138 | 14 | 6 | 36 | 8 | 102 | ICU vs. non-ICU |
| Wang Z, et al. [69] | 16 March 2020 | China | 69 | 10 | 2 | 14 | 8 | 55 | SpO2 ≥ 90% vs. SpO2 ≤ 90% |
| Xu X-W, et al. [79] | 19 February 2020 | China | 62 | 3 | 3 | 33 | 0 | 29 | Time since symptom onset >10 days vs. ≤10 days |
| Zheng M, et al. [88] | 19 March 2020 | China | 68 | 3 | 1 | 13 | 2 | 55 | Severe vs. mild |
| Zhang G, et al. [82] | 9 April 2020 | China | 221 | 25 | 9 | 55 | 16 | 166 | Severe vs. non-severe |
| Du R, et al. [23] | 7 April 2020 | China | 109 | 29 | 15 | 51 | 14 | 58 | ICU vs. non-ICU |
| Zhang J-J, et al. [83] | 18 February 2020 | China | 140 | 18 | 9 | 57 | 9 | 82 | Severe vs. non-severe |
| Han J, et al. [30] | 5 August 2020 | China | 120 | 7 | 5 | 30 | 2 | 90 | Severe vs. All (diarrhoea vs. no diarrhoea) |
| Liu Yu, et al. [43] | 18 May 2020 | China | 148 | 16 | 8 | 47 | 8 | 68 | Severe vs. non-severe |
| Chen Q, et al. [19] | 28 April 2020 | China | 145 | 39 | 16 | 43 | 23 | 102 | Severe vs. non-severe |
| Huang C, et al. [33] | 24 January 2020 | China | 41 | 1 | 0 | 13 | 1 | 28 | ICU vs. non-ICU |
| Zheng F, et al. [81] | March 2020 | China | 161 | 17 | 1 | 30 | 16 | 131 | Severe vs. non-severe |
| Cai Q, et al. [15] | 2 April 2020 | China | 298 | 9 | 4 | 58 | 5 | 240 | Severe vs. non-severe |
| Nobel Y, et al. [51] | 12 April 2020 | USA | 278 | 53 | 11 | 44 | 42 | 207 | Hospital admission vs. ICU admission |
| Jang J, et al. [34] | 2 June 2020 | South Korea | 110 | 11 | 1 | 23 | 10 | 87 | Severe vs. non-severe |
| Puah S, et al. [54] | 5 April 2021 | Singapore | 60 | 10 | 1 | 10 | 9 | 50 | Severe vs. mild |
| Aumpan N, et al. [6] | 6 July 2020 | Thailand | 40 | 6 | 4 | 10 | 2 | 30 | ICU vs. non-ICU |
| Zhao W, et al. [93] | 19 August 2022 | China | 208 | 24 | 4 | 20 | 20 | 188 | Severe vs. mild |
| Chen D, et al. [96] | 20 October 2022 | China | 93 | 27 | 20 | 51 | 7 | 42 | Severe vs. moderate |
| Sun Z, et al. [94] | 20 January 2022 | China | 63 | 9 | 6 | 24 | 3 | 39 | Severe vs. mild |
| Lee D-S, et al. [92] | 25 May 2022 | South Korea | 46 | 25 | 7 | 16 | 18 | 30 | Severe vs. mild |
| Total | 3800 | 405 | 145 | 876 | 260 | 2863 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dhakal, S.; Charoen, P.; Pan-ngum, W.; Luvira, V.; Sivakorn, C.; Hanboonkunupakarn, B.; Chirapongsathorn, S.; Poovorawan, K. Severity of COVID-19 in Patients with Diarrhoea: A Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2023, 8, 84. https://doi.org/10.3390/tropicalmed8020084
Dhakal S, Charoen P, Pan-ngum W, Luvira V, Sivakorn C, Hanboonkunupakarn B, Chirapongsathorn S, Poovorawan K. Severity of COVID-19 in Patients with Diarrhoea: A Systematic Review and Meta-Analysis. Tropical Medicine and Infectious Disease. 2023; 8(2):84. https://doi.org/10.3390/tropicalmed8020084
Chicago/Turabian StyleDhakal, Sunita, Pimphen Charoen, Wirichada Pan-ngum, Viravarn Luvira, Chaisith Sivakorn, Borimas Hanboonkunupakarn, Sakkarin Chirapongsathorn, and Kittiyod Poovorawan. 2023. "Severity of COVID-19 in Patients with Diarrhoea: A Systematic Review and Meta-Analysis" Tropical Medicine and Infectious Disease 8, no. 2: 84. https://doi.org/10.3390/tropicalmed8020084