
Computer-Aided Detection for Chest Radiography to Improve the Quality of Tuberculosis Diagnosis in Vietnam’s District Health Facilities: An Implementation Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Facility 2X Screening and Triage Algorithms
2.4. CXR Interpretation
2.5. CAD Analysis
2.6. Xpert Testing
2.7. Data Sources
2.8. Data Analysis
3. Results
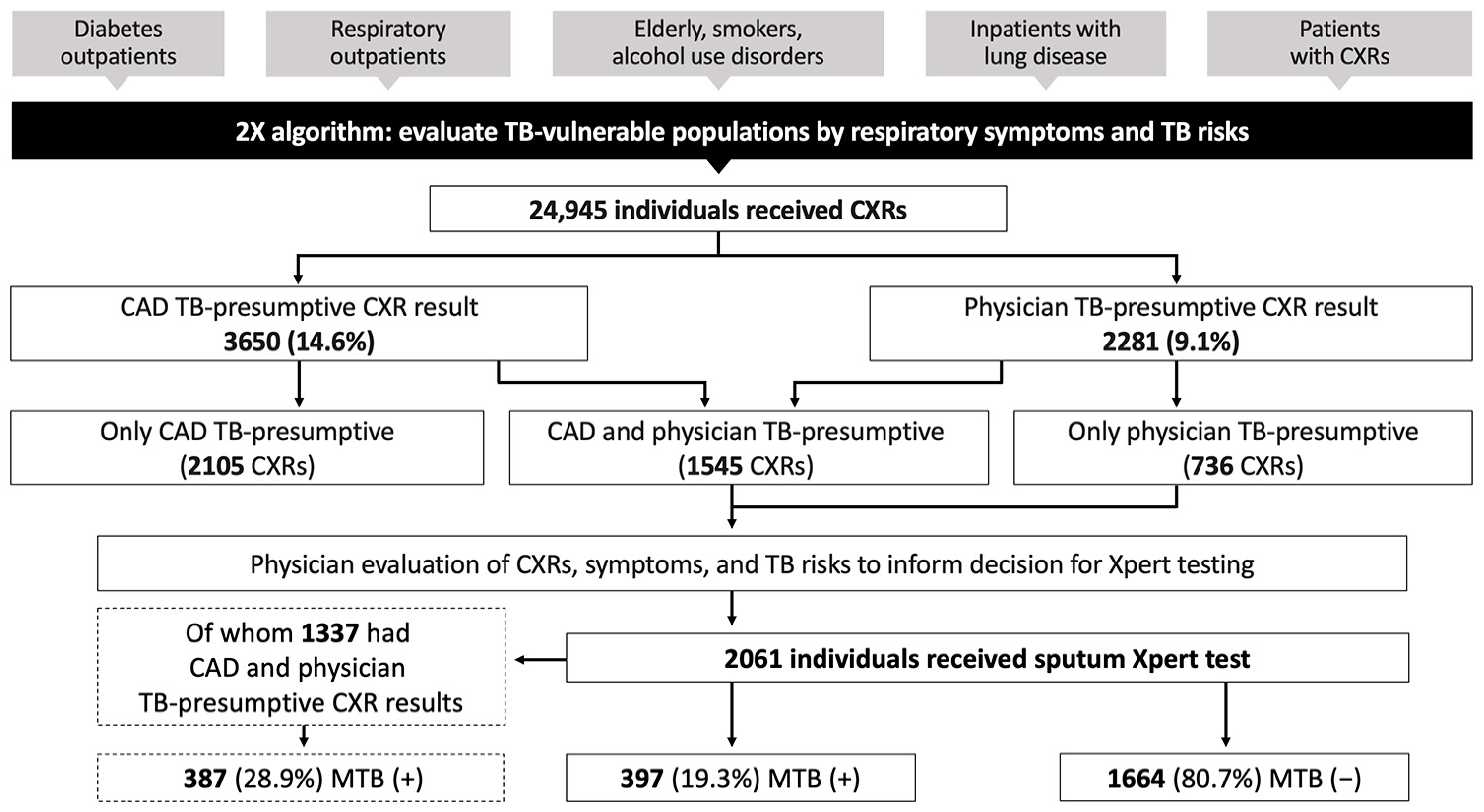
3.1. Results Overall for April–December 2022
3.2. CXR Abnormality and Xpert Positivity Analyzed by CAD and Physician CXR Interpretation
3.3. Analysis of Xpert Testing by CXR Abnormality Scores Relative to the CAD TB Threshold
3.4. Analysis of Agreement between Physician and CAD CXR Results
3.5. Monitoring qXR Performance and Threshold Scores
4. Discussion
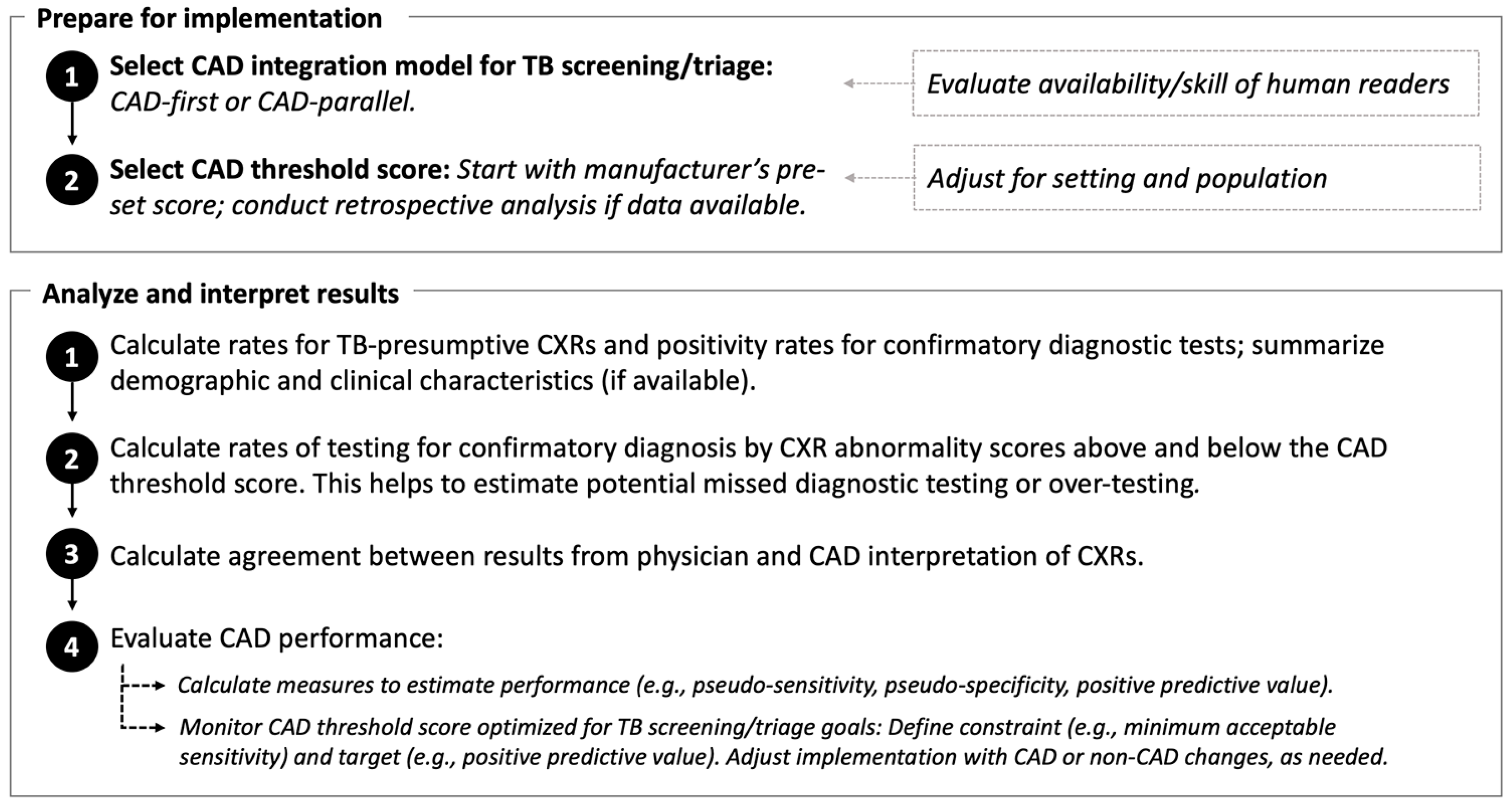
4.1. Using a CAD Programmatic Framework to Guide Non-Research Implementation
4.2. Monitoring the CAD Threshold Score and Evaluating CAD Performance
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Global Tuberculosis Report 2022; WHO: Geneva, Switzerland, 2022.
- Miller, C.; Lonnroth, K.; Sotgiu, G.; Migliori, G.B. The long and winding road of chest radiography for tuberculosis detection. Eur. Respir. J. 2017, 49, 1700364. [Google Scholar] [CrossRef]
- Harris, M.; Qi, A.; Jeagal, L.; Torabi, N.; Menzies, D.; Korobitsyn, A.; Pai, M.; Nathavitharana, R.R.; Ahmad Khan, F. A systematic review of the diagnostic accuracy of artificial intelligence-based computer programs to analyze chest x-rays for pulmonary tuberculosis. PLoS ONE 2019, 14, e0221339. [Google Scholar] [CrossRef]
- Singh, R.; Kalra, M.K.; Nitiwarangkul, C.; Patti, J.A.; Homayounieh, F.; Padole, A.; Rao, P.; Putha, P.; Muse, V.V.; Sharma, A.; et al. Deep learning in chest radiography: Detection of findings and presence of change. PLoS ONE 2018, 13, e0204155. [Google Scholar] [CrossRef]
- Murphy, K.; Habib, S.S.; Zaidi, S.M.A.; Khowaja, S.; Khan, A.; Melendez, J.; Scholten, E.T.; Amad, F.; Schalekamp, S.; Verhagen, M.; et al. Computer aided detection of tuberculosis on chest radiographs: An evaluation of the CAD4TB v6 system. Sci. Rep. 2020, 10, 5492. [Google Scholar] [CrossRef]
- Qin, Z.Z.; Ahmed, S.; Sarker, M.S.; Paul, K.; Adel, A.S.S.; Naheyan, T.; Barrett, R.; Banu, S.; Creswell, J. Tuberculosis detection from chest x-rays for triaging in a high tuberculosis-burden setting: An evaluation of five artificial intelligence algorithms. Lancet Digit. Health 2021, 3, e543–e554. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO CONSOLIDATED GUIDELINES on Tuberculosis. In Module 2: Screening-Systematic Screening for Tuberculosis Disease; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization (WHO). Determining the Local Calibration of Computer-Assisted Detection (CAD) Thresholds and Other Parameters: A Toolkit to Support the Effective Use of CAD for TB Screening; WHO: Geneva, Switzerland, 2021.
- Fanni, S.C.; Marcucci, A.; Volpi, F.; Valentino, S.; Neri, E.; Romei, C. Artificial intelligence-based software with CE mark for chest X-ray interpretation: Opportunities and challenges. Diagnostics 2023, 13, 2020. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.A.; Majidulla, A.; Tavaziva, G.; Nazish, A.; Abidi, S.K.; Benedetti, A.; Menzies, D.; Johnston, J.C.; Khan, A.J.; Saeed, S. Chest x-ray analysis with deep learning-based software as a triage test for pulmonary tuberculosis: A prospective study of diagnostic accuracy for culture-confirmed disease. Lancet Digit. Health 2020, 2, e573–e581. [Google Scholar] [CrossRef]
- Qin, Z.Z.; Sander, M.S.; Rai, B.; Titahong, C.N.; Sudrungrot, S.; Laah, S.N.; Adhikari, L.M.; Carter, E.J.; Puri, L.; Codlin, A.J.; et al. Using artificial intelligence to read chest radiographs for tuberculosis detection: A multi-site evaluation of the diagnostic accuracy of three deep learning systems. Sci. Rep. 2019, 9, 15000. [Google Scholar] [CrossRef] [PubMed]
- Fehr, J.; Gunda, R.; Siedner, M.J.; Hanekom, W.; Ndung, U.T.; Grant, A.; Lippert, C.; Wong, E.B. CAD4TB software updates: Different triaging thresholds require caution by users and regulation by authorities. Int. J. Tuberc. Lung Dis. 2023, 27, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Qin, Z.Z.; Barrett, R.; Ahmed, S.; Sarker, M.S.; Paul, K.; Adel, A.S.S.; Banu, S.; Creswell, J. Comparing different versions of computer-aided detection products when reading chest X-rays for tuberculosis. PLOS Digit. Health 2022, 1, e0000067. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO operational handbook on tuberculosis. In Module 2: Screening-Systematic Screening for Tuberculosis Disease; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Recht, M.P.; Dewey, M.; Dreyer, K.; Langlotz, C.; Niessen, W.; Prainsack, B.; Smith, J.J. Integrating artificial intelligence into the clinical practice of radiology: Challenges and recommendations. Eur. Radiol. 2020, 30, 3576–3584. [Google Scholar] [CrossRef]
- Kapoor, N.; Lacson, R.; Khorasani, R. Workflow applications of artificial intelligence in radiology and an overview of available tools. J. Am. Coll. Radiol. 2020, 17, 1363–1370. [Google Scholar] [CrossRef]
- Duong, M.T.; Rauschecker, A.M.; Rudie, J.D.; Chen, P.H.; Cook, T.S.; Bryan, R.N.; Mohan, S. Artificial intelligence for precision education in radiology. Br. J. Radiol. 2019, 92, 20190389. [Google Scholar] [CrossRef] [PubMed]
- Hadley, T.D.; Pettit, R.W.; Malik, T.; Khoei, A.A.; Salihu, H.M. Artificial intelligence in global health—A framework and strategy for adoption and sustainability. Int. J. MCH AIDS 2020, 9, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Bizzo, B.C.; Almeida, R.R.; Michalski, M.H.; Alkasab, T.K. Artificial Intelligence and Clinical Decision Support for Radiologists and Referring Providers. J. Am. Coll. Radiol. 2019, 16, 1351–1356. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.W.; Jin, K.N.; Oh, S.; Kang, S.Y.; Lee, S.M.; Jeong, I.B.; Son, J.W.; Han, J.H.; Heo, E.Y.; Lee, J.G.; et al. Artificial Intelligence Solution for Chest Radiographs in Respiratory Outpatient Clinics: Multicenter Prospective Randomized Clinical Trial. Ann. Am. Thorac. Soc. 2023, 20, 660–667. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Tuberculosis Profile: Viet Nam. Available online: https://worldhealthorg.shinyapps.io/tb_profiles/?_inputs_&entity_type=%22country%22&lan=%22EN%22&iso2=%22VN%22 (accessed on 18 August 2023).
- Steingart, K.R.; Schiller, I.; Horne, D.J.; Pai, M.; Boehme, C.C.; Dendukuri, N. Xpert® MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults. Cochrane Database Syst. Rev. 2014, 2014, CD009593. [Google Scholar] [CrossRef]
- Nishikiori, N.; Van Weezenbeek, C. Target prioritization and strategy selection for active case-finding of pulmonary tuberculosis: A tool to support country-level project planning. BMC Public Health 2013, 13, 97. [Google Scholar] [CrossRef]
- Mac, T.H.; Phan, T.H.; Nguyen, V.V.; Dong, T.T.T.; Le, H.V.; Nguyen, Q.D.; Nguyen, T.D.; Codlin, A.J.; Mai, T.D.T.; Forse, R.J.; et al. Optimizing Active Tuberculosis Case Finding: Evaluating the Impact of Community Referral for Chest X-ray Screening and Xpert Testing on Case Notifications in Two Cities in Viet Nam. Trop. Med. Infect. Dis. 2020, 5, 181. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Codlin, A.J.; Vo, L.N.Q.; Dao, T.; Tran, D.; Forse, R.J.; Vu, T.N.; Le, G.T.; Luu, T.; Do, G.C.; et al. An Evaluation of Programmatic Community-Based Chest X-ray Screening for Tuberculosis in Ho Chi Minh City, Vietnam. Trop. Med. Infect. Dis. 2020, 5, 185. [Google Scholar] [CrossRef]
- Hoa, N.B.; Sy, D.N.; Nhung, N.V.; Tiemersma, E.W.; Borgdorff, M.W.; Cobelens, F.G. National survey of tuberculosis prevalence in Viet Nam. Bull. World Health Organ. 2010, 88, 273–280. [Google Scholar] [CrossRef]
- Nguyen, H.V.; Tiemersma, E.W.; Nguyen, H.B.; Cobelens, F.G.J.; Finlay, A.; Glaziou, P.; Dao, C.H.; Mirtskhulava, V.; Nguyen, H.V.; Pham, H.T.T.; et al. The second national tuberculosis prevalence survey in Vietnam. PLoS ONE 2020, 15, e0232142. [Google Scholar] [CrossRef]
- The Stop TB Partnership; FIND. Resource Centre on Computer-Aided Detection Products for the Diagnosis of Tuberculosis. Available online: https://www.ai4hlth.org/ (accessed on 18 August 2023).
- StataCorp. Stata Statistical Software: Release 17, 17; StataCorp LLC: College Station, TX, USA, 2021. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing, 4.3.0; R Foundation for Statistical Computing: Vienna, Austria, 2023. [Google Scholar]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Muller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Saito, T.; Rehmsmeier, M. Precrec: Fast and accurate precision-recall and ROC curve calculations in R. Bioinformatics 2017, 33, 145–147. [Google Scholar] [CrossRef]
- The Stop TB Partnership. Screening and Triage for TB Using Computer-Aided Detection (CAD) Technology and Ultra-Portable X-ray Systems: A Practical Guide; The Stop TB Partnership: Grand-Saconnex, Switzerland, 2021. [Google Scholar]
- Philipsen, R.; Sanchez, C.I.; Melendez, J.; Lew, W.J.; van Ginneken, B. Automated chest X-ray reading for tuberculosis in the Philippines to improve case detection: A cohort study. Int. J. Tuberc. Lung Dis. 2019, 23, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Madhani, F.; Maniar, R.; Burfat, A.; Ahmed, M.; Farooq, S.; Sabir, A.; Domki, A.; Page-Shipp, L.; Khowaja, S.; Safdar, N. Automated chest radiography and mass systematic screening for tuberculosis. Int. J. Tuberc. Lung Dis. 2020, 24, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Knop, M.; Weber, S.; Mueller, M.; Niehaves, B. Human Factors and Technological Characteristics Influencing the Interaction of Medical Professionals With Artificial Intelligence-Enabled Clinical Decision Support Systems: Literature Review. JMIR Hum. Factors 2022, 9, e28639. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food & Drug Administration; Health Canada; Medicines & Healthcare Products Regulatory Agency. Good Machine Learning Practice for Medical Device Development: Guiding Principles; 2021. Available online: https://www.fda.gov/medical-devices/software-medical-device-samd/good-machine-learning-practice-medical-device-development-guiding-principles (accessed on 18 August 2023).
- Saito, T.; Rehmsmeier, M. The precision-recall plot is more informative than the ROC plot when evaluating binary classifiers on imbalanced datasets. PLoS ONE 2015, 10, e0118432. [Google Scholar] [CrossRef] [PubMed]
- Nash, M.; Kadavigere, R.; Andrade, J.; Sukumar, C.A.; Chawla, K.; Shenoy, V.P.; Pande, T.; Huddart, S.; Pai, M.; Saravu, K. Deep learning, computer-aided radiography reading for tuberculosis: A diagnostic accuracy study from a tertiary hospital in India. Sci. Rep. 2020, 10, 210. [Google Scholar] [CrossRef]
- Muyoyeta, M.; Maduskar, P.; Moyo, M.; Kasese, N.; Milimo, D.; Spooner, R.; Kapata, N.; Hogeweg, L.; van Ginneken, B.; Ayles, H. The sensitivity and specificity of using a computer aided diagnosis program for automatically scoring chest X-rays of presumptive TB patients compared with Xpert MTB/RIF in Lusaka Zambia. PLoS ONE 2014, 9, e93757. [Google Scholar] [CrossRef]
- Geric, C.; Qin, Z.Z.; Denkinger, C.M.; Kik, S.V.; Marais, B.; Anjos, A.; David, P.M.; Ahmad Khan, F.; Trajman, A. The rise of artificial intelligence reading of chest X-rays for enhanced TB diagnosis and elimination. Int. J. Tuberc. Lung Dis. 2023, 27, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Tavaziva, G.; Harris, M.; Abidi, S.K.; Geric, C.; Breuninger, M.; Dheda, K.; Esmail, A.; Muyoyeta, M.; Reither, K.; Majidulla, A. Chest X-ray analysis with deep learning-based software as a triage test for pulmonary tuberculosis: An individual patient data meta-analysis of diagnostic accuracy. Clin. Infect. Dis. 2022, 74, 1390–1400. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| April–June 2022 | July–September 2022 | October– December 2022 | |
|---|---|---|---|
| Number of district facilities implementing CAD | 5 | 7 | 8 |
| Total number of people with CXRs (N) | 5826 | 9696 | 9423 |
| CAD TB-presumptive CXR result (n [%]) | 749 (12.9) | 1363 (14.1) | 1538 (16.3) |
| Physician TB-presumptive CXR result (n [%]) | 480 (8.2) | 755 (7.8) | 1046 (11.1) |
| Difference of percentages (p-value) * | 4.6 (<0.001) | 6.3 (<0.001) | 5.2 (<0.001) |
| Total number of people with valid Xpert tests (N) | 455 | 703 | 903 |
| Xpert positivity rate overall (n positive/N valid Xpert tests [%]) | 50/455 (11.0) | 148/703 (21.1) | 199/903 (22.0) |
| Xpert positivity rate for CAD and physician TB-presumptive CXRs (n positive/n Xperts with CAD and physician TB-presumptive CXRs [%]) | 48/206 (23.3) | 143/472 (30.3) | 196/659 (29.7) |
| Xpert positivity rate for CAD non-TB and physician TB-presumptive CXRs (n positive/n Xperts with physician TB-presumptive CXRs [%]) | 2/249 (0.8) | 5/229 (2.2) | 3/242 (1.2) |
| April–June 2022 | July–September 2022 | October– December 2022 | |
|---|---|---|---|
| Total number of people with valid Xpert tests (N) | 455 | 703 | 903 |
| Xpert testing rate (N valid Xpert tests/N total CXRs [%]) | 455/5826 (7.8) | 703/9696 (7.3) | 903/9423 (9.6) |
| n Xpert tests not done for CXR abnormality score ≥ 0.60/n CXRs with score ≥ 0.60 (%) | 543/749 (72.5) | 887/1359 (65.3) * | 830/1466 (56.6) * |
| n Xpert tests done for CXR abnormality score < 0.60/N valid Xpert tests (%) | 249/455 (54.7) | 231/703 (32.9) * | 267/903 (29.6) * |
| April–June 2022 | July–September 2022 | October– December 2022 | |
|---|---|---|---|
| Physician TB-presumptive CXR and CAD non-TB CXR (n [%]) | 253 (52.7) | 233 (30.9) * | 250 (23.9) * |
| Physician and CAD TB-presumptive CXR (n [%]) | 227 (47.3) | 522 (69.1) * | 796 (76.1) * |
| Physician non-TB CXR and CAD TB-presumptive CXR (n [%]) | 522 (9.8) | 841 (9.4) | 742 (8.9) |
| Physician non-TB CXR and CAD non-TB CXR (n [%]) | 4824 (90.2) | 8100 (90.6) | 7635 (91.1) |
| Total agreement (%), (Kappa [Standard error]) | 86.7% (0.30 [0.01]) | 88.9% * (0.44 [0.01]) | 89.5% * (0.56 [0.01]) |
| April–June 2022 | July–September 2022 | October–December 2022 | |
|---|---|---|---|
| Total number of people with CXRs | 5826 | 9696 | 9423 |
| Number with CXR and Xpert results | 455 | 703 | 903 |
| Number with Xpert-positive results | 50 | 148 | 199 |
| Yield for Xpert-confirmed TB/100,000 CXRs | 858 | 1526 | 2112 |
| Pseudo-sensitivity at qXR = 0.60 (95% CI) | 96.0% (90.0–100) | 96.6% (93.9–99.3) | 98.5% (96.5–100) |
| Pseudo-specificity at qXR = 0.60 (95% CI) | 61.0% (56.3–65.9) | 40.7% (36.6–45.1) | 37.5% (34.0–41.1) |
| PPV at qXR = 0.60 (95% CI) | 23.4% (21.1–25.9) | 30.3% (28.8–32.1) | 30.8% (29.6–32.1) |
| Pseudo-accuracy at qXR = 0.6 (95% CI) | 64.8% (60.7–69.2) | 52.5% (49.2–56.1) | 50.9% (48.2–53.7) |
| AUROC (95% CI) | 0.8598 (0.8127–0.9068) | 0.8267 (0.7920–0.8614) | 0.8062 (0.7755–0.8368) |
| PRAUC | 0.4375 | 0.5755 | 0.4770 |
| Optimal qXR threshold score at >95% pseudo-sensitivity | 0.615 | 0.677 | 0.654 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Innes, A.L.; Martinez, A.; Gao, X.; Dinh, N.; Hoang, G.L.; Nguyen, T.B.P.; Vu, V.H.; Luu, T.H.T.; Le, T.T.T.; Lebrun, V.; et al. Computer-Aided Detection for Chest Radiography to Improve the Quality of Tuberculosis Diagnosis in Vietnam’s District Health Facilities: An Implementation Study. Trop. Med. Infect. Dis. 2023, 8, 488. https://doi.org/10.3390/tropicalmed8110488
Innes AL, Martinez A, Gao X, Dinh N, Hoang GL, Nguyen TBP, Vu VH, Luu THT, Le TTT, Lebrun V, et al. Computer-Aided Detection for Chest Radiography to Improve the Quality of Tuberculosis Diagnosis in Vietnam’s District Health Facilities: An Implementation Study. Tropical Medicine and Infectious Disease. 2023; 8(11):488. https://doi.org/10.3390/tropicalmed8110488
Chicago/Turabian StyleInnes, Anh L., Andres Martinez, Xiaoming Gao, Nhi Dinh, Gia Linh Hoang, Thi Bich Phuong Nguyen, Viet Hien Vu, Tuan Ho Thanh Luu, Thi Thu Trang Le, Victoria Lebrun, and et al. 2023. "Computer-Aided Detection for Chest Radiography to Improve the Quality of Tuberculosis Diagnosis in Vietnam’s District Health Facilities: An Implementation Study" Tropical Medicine and Infectious Disease 8, no. 11: 488. https://doi.org/10.3390/tropicalmed8110488