
Post-Artesunate Delayed Hemolysis: A Review of Current Evidence
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Epidemiology
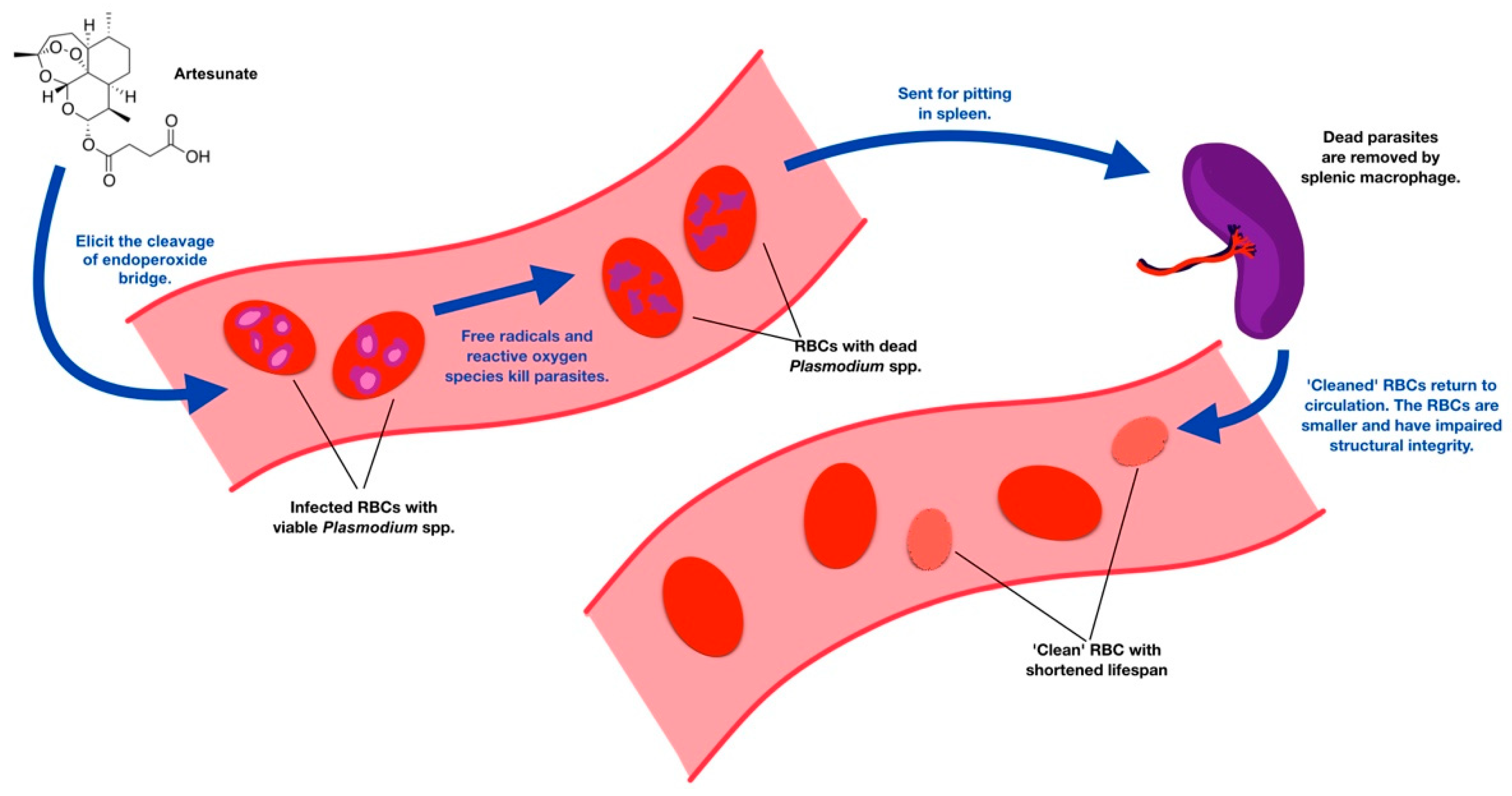
3. Pathophysiology
4. Clinical Features and Laboratory Results

{kind=link}
{kind=link}
| Acquired | Hereditary |
|---|---|
|
|
| Test | Finding | Cause |
|---|---|---|
| Haptoglobin concentrations | Low or absent | Binds free hemoglobin (Hb) |
| Lactate dehydrogenase concentration | High | Released from lysis of RBCs |
| Reticulocyte count | High | Marrow response to anemia |
| Unconjugated bilirubin | High | Increased Hb breakdown |
| Urinalysis | Urobilinogen, positive for blood | Free Hb and its metabolites |
| Jarvis et al. [50] | Raffray et al. [23] | Paczkowski et al. [51] | Plewes et al. [52] | Boillat et al. [27] | Salehi et al. [53] | Conlon et al. [20] | Patel et al. [54] | Matsee et al. [45] | Martino et al. [46] | |
|---|---|---|---|---|---|---|---|---|---|---|
| Participant(s) | 1 adult returned traveler | 1 adult returned traveler | 2 adults returned traveler | 1 adult endemic area | 4 adults returned traveler | 1 adult returned traveler | 1 adult returned traveler | 1 child endemic area | 1 adult returned traveler | 1 child returned traveler |
| Year | 2013 | 2014 | 2014 | 2015 | 2015 | 2019 | 2020 | 2020 | 2021 | 2022 |
| Day of hemolysis detection | 8 | 8 | 9–11 | 14 | 8–28 | 12 | 8 | 11 | 15 | 7 |
| Severity | Severe without hyperparasitemia | Severe without hyperparasitemia | Severe with hyperparasitemia | Severe with hyperparasitemia | Severe with and without hyperparasitemia | Severe with hyperparasitemia | Severe with hyperparasitemia | Severe without hyperparasitemia | Not severe | Severe with hyperparasitemia |
| Sign/Symptom | Fever, dyspnea, ankle swelling, anemia, jaundice, tachycardia, hepatosplenomegaly, dark urine | Fever, fatigue | Weakness, fatigue, SOB, leg edema | Fever, rigors, headache, N/V, abdominal pain, jaundice | Fever, fatigue, jaundice, SOB | Fever, jaundice, headache, dark urine | Fever, N/V | Fever, weakness, loss of appetite, headache, anemia, jaundice, tachycar-dia, dark urine | Malaise, fatigue | Asymptomatic |
| Laboratory findings | Hb 4.1 g/dL, haptoglobin < 0.1 g/L, Normal LFT, High LDH | Hb 4.6 g/dL, high LDH, absent haptoglobin | Hb 5.7–6.8 g/dL, high LDH, TB, and reticulocyte count | Hb 4.9 g/dL, high LDH, decreased haptoglobin, normal G6PD | Hb 5.6–12.4 g/dL, high LDH, low haptoglobin, high reticulocyte count | Hb 4.7 g/dL, high TB, LDH, 3994 U/L negative Coombs test, normal reticulocyte count | Hb 10.2 g/dL, low haptoglobin < 0.1 g/L, high LDH 1759 U/L, rising TB | Hb 10 g/dL, hemolytic blood picture, high reticulocyte count, high LDH, parasitemia | Hb 9.1 g/dL LDH 1706 U/L, low haptoglobin (<0.024 mg/mL), high reticulocyte count | Hb 7.7 g/dL, high reticulocyte count, haptoglobin < 0.08 g/dL |
| Laboratory findings at the follow-up | No data | Follow-up Day 52 Hb > 12 g/dL Haptoglobin and LDH were within normal limits | Follow-up Day 19 Hb 9.8 g/dL in one case No data of another case | No data | Follow-up Day 28–35 Hb 10.5–14 g/dL Low LDH | No data | No data | Follow-up after 1 month Hb 134 g/L Other hematological parameters returned to normal range | Follow-up Day 29 Hb 10.2 g/dL Follow-up 2 months Hb 13.3 g/dL LDH 355 U/L | Follow-up day 21 Hb 9.2 mg/dL |
| Blood transfusion | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | No | N/A |
5. Role of the P. falciparum-Histidine-Rich Protein 2 Rapid Diagnostic Test for Predicting Subsequent PADH
6. Implementation
7. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Malaria Report; World Health Organization: Geneva, Switzerland, 2021.
- Kotepui, M.; Kotepui, K.U.; Milanez, G.D.; Masangkay, F.R. Severity and mortality of severe Plasmodium ovale infection: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0235014. [Google Scholar] [CrossRef]
- Rajahram, G.S.; Barber, B.E.; William, T.; Menon, J.; Anstey, N.M.; Yeo, T.W. Deaths due to Plasmodium knowlesi malaria in Sabah, Malaysia: Association with reporting as Plasmodium malariae and delayed parenteral artesunate. Malar. J. 2012, 11, 284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahimi, B.A.; Thakkinstian, A.; White, N.J.; Sirivichayakul, C.; Dondorp, A.M.; Chokejindachai, W. Severe vivax malaria: A systematic review and meta-analysis of clinical studies since 1900. Malar. J. 2014, 13, 481. [Google Scholar] [CrossRef] [Green Version]
- Brown, G.D. The Biosynthesis of Artemisinin (Qinghaosu) and the Phytochemistry of Artemisia annua L. (Qinghao). Molecules 2010, 15, 7603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Guidelines for Malaria Treatment. 2010. Available online: https://apps.who.int/medicinedocs/documents/s19105en/s19105en.pdf (accessed on 12 November 2022).
- Dondorp, A.; Nosten, F.; Stepniewska, K.; Day, N.; White, N. South East Asian Quinine Artesunate Malaria Trial (SEAQUAMAT) group Artesunate versus quinine for treatment of severe falciparum malaria: A randomised trial. Lancet 2005, 366, 717–725. [Google Scholar] [CrossRef] [Green Version]
- Dondorp, A.M.; Fanello, C.I.; Hendriksen, I.C.; Gomes, E.; Seni, A.; Chhaganlal, K.D.; Bojang, K.; Olaosebikan, R.; Anunobi, N.; Maitland, K.; et al. Artesunate versus quinine in the treatment of severe falciparum malaria in African children (AQUAMAT): An open-label, randomised trial. Lancet 2010, 376, 1647–1657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurth, F.; Develoux, M.; Mechain, M.; Malvy, D.; Clerinx, J.; Antinori, S.; Gjørup, I.E.; Gascon, J.; Mørch, K.; Nicastri, E.; et al. Severe malaria in Europe: An 8-year multi-centre observational study. Malar. J. 2017, 16, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Committee to Advise on Tropical Medicine and Travel. Canadian Recommendations for the Prevention and Treatment of Malaria. 2020. Available online: https://www.canada.ca/en/public-health/services/catmat/canadian-recommendations-prevention-treatment-malaria.html (accessed on 12 November 2022).
- Centers for Disease Control and Prevention. CDC Yellow Book 2020: Health Information for International Travel; Oxford University Press: New York, NY, USA, 2017.
- Scheu, K.; Adegnika, A.A.; Addo, M.M.; Ansong, D.; Cramer, J.P.; Fürst, S.; Kremsner, P.G.; Kurth, F.; Jacobs, T.; May, J.; et al. Determinants of post-malarial anemia in African children treated with parenteral artesunat. Nat. Rev. 2019, 9, 18134. [Google Scholar]
- Savargaonkar, D.; Das, M.K.; Verma, A.; Mitra, J.K.; Yadav, C.P.; Srivastava, B.; Anvikar, A.R.; Valecha, N. Delayed haemolysis after treatment with intravenous artesunate in patients with severe malaria in India. Malar. J. 2020, 19, ciac719. [Google Scholar] [CrossRef] [PubMed]
- Rolling, T.; Agbenyega, T.; Issifou, S.; Adegnika, A.A.; Sylverken, J.; Spahlinger, D.; Ansong, D.; Löhr, S.J.; Burchard, G.D.; May, J.; et al. Delayed hemolysis after treatment with parenteral artesunate in African children with severe malariaea double-center prospective study. J. Infect. Dis. 2014, 209, 1921–1928. [Google Scholar] [CrossRef] [Green Version]
- Jauréguiberry, S.; Thellier, M.; Ndour, P.A.; Ader, F.; Roussel, C.; Sonneville, R.; Mayaux, J.; Matheron, S.; Angoulvant, A.; Wyplosz, B.; et al. Delayed-Onset Hemolytic Anemia in Patients with Travel-Associated Severe Malaria Treated with Artesunate, France, 2011–2013. Emerg. Infect. Dis. 2015, 21, 804–812. [Google Scholar] [CrossRef] [PubMed]
- Roussel, C.; Ndour, P.A.; Kendjo, E.; Larréché, S.; Taieb, A.; Henry, B.; Lebrun-Vignes, B.; Chambrion, C.; Argy, N.; Houzé, S.; et al. Intravenous Artesunate for the Treatment of Severe Imported Malaria: Implementation, Efficacy, and Safety in 1391 Patients. Clin. Infect. Dis. 2021, 73, 1795–1804. [Google Scholar] [CrossRef] [PubMed]
- Roussel, M.C.; Caumes, E.; Thellier, M.; Ndour, P.A.; Buffet, P.; Jauréguiberry, S. Artesunate to treat severe malaria in travellers: Review of efficacy and safety and practical implications. J. Travel Med. 2017, 24, taw093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Information Note on Delayed Haemolytic Anaemia Following Treatment with Artesunate. 2013. Available online: https://www.who.int/malaria/publications/atoz/who_note_delayed_haemolytic_anaemia_oct13.pdf?ua=1 (accessed on 16 November 2022).
- Rolling, T.; Wichmann, D.; Schmiedel, S.; Burchard, G.D.; Kluge, S.; Cramer, J.P. Artesunate versus quinine in the treatment of severe imported malaria: Comparative analysis of adverse events focussing on delayed haemolysis. Malar. J. 2013, 12, 241–248. [Google Scholar] [CrossRef] [Green Version]
- Conlon, C.C.; Stein, A.; Colombo, R.E.; Schofield, C. Post-artemisinin delayed hemolysis after oral therapy for P. falciparum infection. Idcases 2020, 20, e00741. [Google Scholar] [CrossRef]
- Rehman, K.; Lötsch, F.; Kremsner, P.G.; Ramharter, M. Haemolysis associated with the treatment of malaria with artemisinin derivatives: A systematic review of current evidence. Int. J. Infect. Dis. 2014, 29, 268–273. [Google Scholar] [CrossRef] [Green Version]
- Kurth, F.; Lingscheid, T.; Steiner, F.; Stegemann, M.S.; Bélard, S.; Menner, N.; Pongratz, P.; Kim, J.; von Bernuth, H.; Mayer, B.; et al. Hemolysis after Oral Artemisinin Combination Therapy for Uncomplicated Plasmodium falciparum Malaria. Emerg. Infect. Dis. 2016, 22, 1381–1386. [Google Scholar] [CrossRef] [Green Version]
- Raffray, L.; Receveur, M.; Beguet, M.; Lauroua, P.; Pistone, T.; Malvy, D. Severe delayed autoimmune haemolytic anaemia following artesunate administration in severe malaria: A case report. Malar. J. 2014, 13, 398. [Google Scholar] [CrossRef]
- Chotivanich, K.; Udomsangpetch, R.; Dondorp, A.; Williams, T.; Angus, B.; Simpson, J.A.; Pukrittayakamee, S.; Looareesuwan, S.; Newbold, C.I.; White, N.J. The Mechanisms of Parasite Clearance after Antimalarial Treatment of Plasmodium falciparum Malaria. J. Infect. Dis. 2000, 182, 629–633. [Google Scholar] [CrossRef] [Green Version]
- Rolling, T.; Agbenyega, T.; Krishna, S.; Kremsner, P.; Cramer, J. Delayed haemolysis after artesunate treatment of severe malaria e Review of the literature and perspective. Travel Med. Infect Dis. 2015, 13, 143–149. [Google Scholar] [CrossRef]
- Arguin, P.M. Case definition: Postartemisinin delayed hemolysis. Blood 2014, 124, 157–158. [Google Scholar] [CrossRef] [PubMed]
- Boillat, O.; Spechbach, H.; Chalandon, Y.; Eperon, G. Post-artesunate delayed haemolysis–report of four cases and review of the literature. Swiss Med. Wkly. 2015, 145, w14181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jauréguiberry, S.; Ndour, P.A.; Roussel, C.; Ader, F.; Safeukui, I.; Nguyen, M.; Biligui, S.; Ciceron, L.; Mouri, O.; Kendjo, E.; et al. Postartesunate delayed hemolysis is a predictable event related to the lifesaving effect of artemisinins. Blood 2014, 124, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Ndour, P.A.; Larréché, S.; Mouri, O.; Argy, N.; Gay, F.; Roussel, C.; Jauréguiberry, S.; Perillaud, C.; Langui, D.; Biligui, S.; et al. Measuring the Plasmodium falciparum HRP2 protein in blood from artesunate-treated malaria patients predicts post-artesunate delayed hemolysis. Sci. Transl. Med. 2017, 9, eaaf9377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medicines for Malaria Ventures. Experts Group Meeting on Delayed Haemolytic Anaemia Following Treatment with Injectable Artesunate. 2013. Available online: https://www.mmv.org/sites/default/files/uploads/docs/events/2013/InjectableArtesunateExpertGroupMeeting.pdf (accessed on 16 November 2022).
- Efferth, T.; Kaina, B. Toxicity of the antimalarial artemisinin and its dervatives. Crit. Rev. Toxicol. 2010, 40, 405–421. [Google Scholar] [CrossRef] [PubMed]
- Finaurini, S.; Ronzoni, L.; Colancecco, A.; Cattaneo, A.; Cappellini, M.D.; Ward, S.A.; Taramelli, D. Selective toxicity of dihydroartemisinin on human CD34+ erythroid cell differentiation. Toxicology 2010, 276, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Finaurini, S.; Basilico, N.; Corbett, Y.; D’Alessandro, S.; Parapini, S.; Olliaro, P.; Haynes, R.K.; Taramelli, D. Dihydroartemisinin inhibits the human erythroid cell differentiation by altering the cell cycle. Toxicology 2012, 300, 57–66. [Google Scholar] [CrossRef]
- Camprubí, D.; Pereira, A.; Rodriguez-Valero, N.; Almuedo, A.; Varo, R.; Casals-Pascual, C.; Bassat, Q.; Malvy, D.; Muñoz, J. Positive direct antiglobulin test in post-artesunate delayed haemolysis: More than a coincidence? Malar. J. 2019, 18, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lebrun, D.; Floch, T.; Brunet, A.; Julien, G.; Romaru, J.; N’Guyen, Y.; Cousson, J.; Giltat, A.; Toubas, D.; Bani-Sadr, F. Severe post-artesunate delayed onset anaemia responding to corticotherapy: A case report. J. Travel Med. 2017, 25, tax091. [Google Scholar] [CrossRef] [Green Version]
- Parker, V.; Tormey, C.A. The Direct Antiglobulin Test: Indications, Interpretation, and Pitfalls. Arch. Pathol. Lab. Med. 2017, 141, 305–310. [Google Scholar] [CrossRef] [Green Version]
- Garratty, G. Immune hemolytic anemia associated with drug therapy. Blood Rev. 2010, 24, 143–150. [Google Scholar] [CrossRef]
- Barber, B.E.; Grigg, M.J.; Piera, K.; Amante, F.H.; William, T.; Boyle, M.J.; Minigo, G.; Dondorp, A.M.; McCarthy, J.; Anstey, N.M. Antiphosphatidylserine Immunoglobulin M and Immunoglobulin G Antibodies Are Higher in Vivax than Falciparum Malaria, and Associated with Early Anemia in Both Species. J. Infect. Dis. 2019, 220, 1435–1443. [Google Scholar] [CrossRef]
- Ascoli Bartoli, T.; Lepore, L.; D’Abramo, A.; Adamo, G.; Corpolongo, A.; Scorzolini, L.; Giancola, M.L.; Bevilacqua, N.; Palazzolo, C.; Mariano, A.; et al. Systematic analysis of direct antiglobulin test results in post-artesunate delayed haemolysis. Malar. J. 2021, 1, 206. [Google Scholar] [CrossRef] [PubMed]
- Weina, P.J.; Haeberle, A.S.; Milhous, W.K. Intravenous Artesunate: The New Generation of Lifesaving Treatment for Severe Malaria in the Warfighter; Walter Reed Army Institute of Research: Silver Spring, MD, USA, 2006. [Google Scholar]
- Clark, R.L. Hypothesized cause of delayed hemolysis associated with intravenous artesunate. Med. Hypotheses 2014, 82, 167–170. [Google Scholar] [CrossRef]
- Knights, P. Artesunate: 14 Days Preliminary Oral (Gavage Administration) Toxicity Study in the Rat. Covance Report No. 1552/051-D6154, 2002. [Google Scholar]
- Knights, P. Artesunate: 4 Weeks Oral (Gavage Administration) Toxicity Study in the Rat. Covance Report No. 1552/059-D6154, 2002. [Google Scholar]
- Gómez-Junyent, J.; Ruiz-Panales, P.; Calvo-Cano, A.; Gascón, J.; Muñoz, J. Delayed haemolysis after artesunate therapy in a cohort of patients with severe imported malaria due to Plasmodium falciparum. Enferm. Infecc. Microbiol. Clin. 2017, 35, 516–519. [Google Scholar] [CrossRef] [Green Version]
- Matsee, W.; Hiranrusme, T.; Pisutsan, P.; Hanboonkunupakarn, B.; Chotivanich, K. Returned traveller presenting with anaemia: Clinical challenge of post-artesunate delayed haemolysis. J. Travel Med. 2021, 28, taab171. [Google Scholar] [CrossRef] [PubMed]
- Martino, M.; Liberati, C.; Bua, B.; Barbieri, E.; Costenaro, P.; Di Chiara, C.; Giaquinto, C.; De Canale, E.; Rampon, O.; Donà, D. Treatment for Severe Malaria: Post-Artesunate Delayed Haemolysis and Neutropenia. Healthcare 2022, 10, 413. [Google Scholar] [CrossRef] [PubMed]
- Phillips, J.; Henderson, A.C. Hemolytic Anemia: Evaluation and Differential Diagnosis. Am. Fam. Physician 2018, 98, 354–361. [Google Scholar]
- Packman, C. William Hematology, 9th ed.; McGraw-Hill: New York, NY, USA, 2016. [Google Scholar]
- Bethell, D.; Se, Y.; Lon, C.; Khemawoot, P.; Darapiseth, S.; Sriwichai, S.; Kuntawungin, W.; Surasri, S.; Sarim, S.; Tyner, S.; et al. Dose?Dependent Risk of Neutropenia after 7? Day Courses of Artesunate Monotherapy in Cambodian Patients with Acute Plasmodium falciparum Malaria. Clin. Infect. Dis. 2010, 51, e105–e114. [Google Scholar] [CrossRef] [Green Version]
- Jarvis, J.N.; Coltart, C.E.; Pule, M.; Chiodini, P.; Doherty, T. Artemisinin therapy and severe delayed haemolysis. Lancet 2013, 382, 180. [Google Scholar] [CrossRef]
- Paczkowski, M.; Landman, K.; Arguin, P. Update on cases of delayed hemolysis after parenteral artesunate therapy for malaria—United States, 2008 and 2013. MMWR Morb. Mortal Wkly. Rep. 2014, 63, 753. [Google Scholar] [PubMed]
- Plewes, K.; Haider, S.; Kingston, H.W.F.; Yeo, T.W.; Ghose, A.; Hossain, A.; Dondorp, A.M.; Turner, G.D.H.; Anstey, N.M. Severe falciparum malaria treated with artesunate complicated by delayed onset haemolysis and acute kidney injury. Malar. J. 2015, 14, 246. [Google Scholar] [CrossRef] [PubMed]
- Salehi, M.; Masoumi-Asl, H.; Assarian, M.; Khoshnam-Rad, N.; Haghi, A.M.; Nikbakht, M.; Khalili, H. Delayed Hemolytic Anemia after Treatment with Artesunate: Case Report and Literature Review. Curr. Drug Saf. 2019, 14, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Thomson, J.; Ferre, L.R. Delayed haemolysis following artesunate in a child with profound anaemia and Coca-Cola-coloured urine. BMJ Case Rep. 2020, 13, e2383. [Google Scholar]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaita, S.; Madsalae, K.; Charoensakulchai, S.; Hanboonkunapakarn, B.; Chotivanit, K.; McCarthy, A.E.; Matsee, W. Post-Artesunate Delayed Hemolysis: A Review of Current Evidence. Trop. Med. Infect. Dis. 2023, 8, 49. https://doi.org/10.3390/tropicalmed8010049
Jaita S, Madsalae K, Charoensakulchai S, Hanboonkunapakarn B, Chotivanit K, McCarthy AE, Matsee W. Post-Artesunate Delayed Hemolysis: A Review of Current Evidence. Tropical Medicine and Infectious Disease. 2023; 8(1):49. https://doi.org/10.3390/tropicalmed8010049
Chicago/Turabian StyleJaita, Sawettachai, Krit Madsalae, Sakarn Charoensakulchai, Borimas Hanboonkunapakarn, Kesinee Chotivanit, Anne E. McCarthy, and Wasin Matsee. 2023. "Post-Artesunate Delayed Hemolysis: A Review of Current Evidence" Tropical Medicine and Infectious Disease 8, no. 1: 49. https://doi.org/10.3390/tropicalmed8010049