
Soil-Transmitted Helminth Infections among Antenatal Women in Primary Care Settings in Southern India: Prevalence, Associated Factors and Effect of Anti-Helminthic Treatment
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
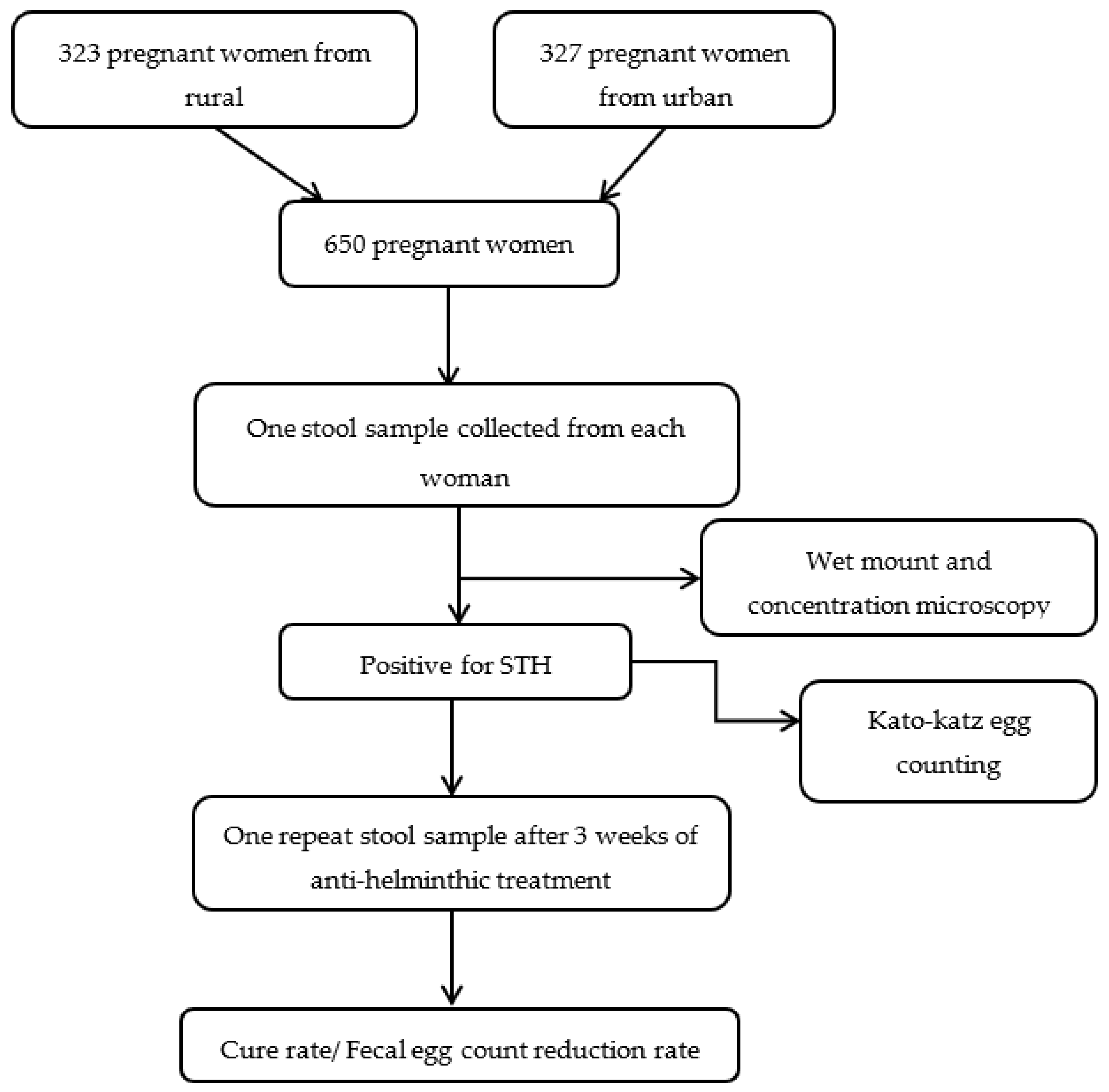
2.1. Study Design and Setting
2.2. Study Population
2.3. Inclusion and Exclusion Criteria
2.4. Sample Size Estimation
2.5. Methods
2.6. Quality Assurance
2.7. Statistical Analysis
3. Results
3.1. Socio-Demographic and Obstetric Characteristics of Pregnant Women
3.2. Behavioral Characteristics of Pregnant Women
3.3. Prevalence of STH Infections
3.4. Factors Associated with STH Infections in Pregnancy
3.5. Efficacy of Anti-Helminthic Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hotez, P.J.; Alvarado, M.; Basáñez, M.-G.; Bolliger, I.; Bourne, R.; Boussinesq, M.; Brooker, S.J.; Brown, A.S.; Buckle, G.; Budke, C.M.; et al. The Global Burden of Disease Study 2010: Interpretation and Implications for the Neglected Tropical Diseases. PLoS Negl. Trop. Dis. 2014, 8, e2865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sitotaw, B.; Mekuriaw, H.; Damtie, D. Prevalence of Intestinal Parasitic Infections and Associated Risk Factors among Jawi Primary School Children, Jawi Town, North-West Ethiopia. BMC Infect. Dis. 2019, 19, 341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salam, R.A.; Das, J.K.; Bhutta, Z.A. Effect of Mass Deworming with Antihelminthics for Soil-Transmitted Helminths during Pregnancy. Cochrane Database Syst. Rev. 2021, 5, CD005547. [Google Scholar] [PubMed]
- Ragunathan, L.; Kalivaradhan, S.K.; Ramadass, S.; Nagaraj, M.; Ramesh, K. Helminthic Infections in School Children in Puducherry. J. Microbiol. Immunol. Infect. 2010, 43, 228–232. [Google Scholar] [CrossRef] [Green Version]
- Narkkul, U.; Na-ek, P.; Kaewkungwal, J.; Punsawad, C. Knowledge, Attitudes, and Practices Regarding Soil-Transmitted Helminthiasis among Village Health Volunteers in Nakhon Si Thammarat Province, Thailand: A Cross-Sectional Study. Trop. Med. Infect. Dis. 2022, 7, 33. [Google Scholar] [CrossRef]
- Rodríguez-Morales, A.J.; Barbella, R.A.; Case, C.; Arria, M.; Ravelo, M.; Perez, H.; Urdaneta, O.; Gervasio, G.; Rubio, N.; Maldonado, A.; et al. Intestinal Parasitic Infections among Pregnant Women in Venezuela. Infect. Dis. Obstet. Gynecol. 2006, 2006, 23125. [Google Scholar] [CrossRef] [Green Version]
- Degarege, A.; Erko, B.; Negash, Y.; Animut, A. Intestinal Helminth Infection, Anemia, Undernutrition and Academic Performance among School Children in Northwestern Ethiopia. Microorganisms 2022, 10, 1353. [Google Scholar] [CrossRef]
- Mengist, H.M.; Zewdie, O.; Belew, A. Intestinal Helminthic Infection and Anemia among Pregnant Women Attending Ante-Natal Care (ANC) in East Wollega, Oromia, Ethiopia. BMC Res. Notes 2017, 10, 440. [Google Scholar] [CrossRef] [PubMed]
- Aderoba, A.K.; Iribhogbe, O.I.; Olagbuji, B.N.; Olokor, O.E.; Ojide, C.K.; Ande, A.B. Prevalence of Helminth Infestation during Pregnancy and Its Association with Maternal Anemia and Low Birth Weight. Int. J. Gynaecol. Obstet. Off. Organ. Int. Fed. Gynaecol. Obstet. 2015, 129, 199–202. [Google Scholar] [CrossRef]
- Loukas, A.; Hotez, P.J.; Diemert, D.; Yazdanbakhsh, M.; McCarthy, J.S.; Correa-Oliveira, R.; Croese, J.; Bethony, J.M. Hookworm Infection. N. Engl. J. Med. 2016, 2, 799–807. [Google Scholar] [CrossRef]
- Salam, N.; Azam, S. Prevalence and Distribution of Soil-Transmitted Helminth Infections in India. BMC Public Health 2017, 17, 201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajjampur, S.S.R.; Kaliappan, S.P.; Halliday, K.E.; Palanisamy, G.; Farzana, J.; Manuel, M.; Abraham, D.; Laxmanan, S.; Aruldas, K.; Rose, A.; et al. Epidemiology of Soil Transmitted Helminths and Risk Analysis of Hookworm Infections in the Community: Results from the DeWorm3 Trial in Southern India. PLoS Negl. Trop. Dis. 2021, 15, e0009338. [Google Scholar] [CrossRef] [PubMed]
- Kaliappan, S.P.; George, S.; Francis, M.R.; Kattula, D.; Sarkar, R.; Minz, S.; Mohan, V.R.; George, K.; Roy, S.; Ajjampur, S.S.R.; et al. Prevalence and Clustering of Soil-Transmitted Helminth Infections in a Tribal Area in Southern India. Trop. Med. Int. Health 2013, 18, 1452–1462. [Google Scholar] [CrossRef] [Green Version]
- Gaidhane, A.; Kirti, V.; Bharadawaj, P.; Gaidhane, S.; Khatib, N.; Saxena, D.; Telrandhe, S.; Patil, M.; Choudhari, S.; Zahiruddin, Q.S. The Burden of Soil-Transmitted Helminths Infections among Pregnant Women in Maharashtra and Rajasthan States of India. J. Fam. Med. Prim. Care 2022, 11, 3161–3166. [Google Scholar] [CrossRef]
- Shrinivas, K.; Sreelatha, R.; Kavitha, K. Study of Helminthiasis in Pregnancy and Its Correlation with Haemoglobin Level. J. Clin. Diagn. Res. 2014, 8, OC07–OC9. [Google Scholar]
- World Health Organization. Soil-Transmitted Helminth Infections. Available online: https://www.who.int/news-room/fact-sheets/detail/soil-transmitted-helminth-infections (accessed on 10 November 2022).
- Government of India. Puducherry Population Sex Ratio in Puducherry Literacy Rate Pondicherry 2011–2022. Available online: https://www.census2011.co.in/census/state/puducherry.html (accessed on 10 November 2022).
- Ministry of Home Affairs Government of India Puducherry City Population Census 2011-2022. Available online: https://www.census2011.co.in/census/city/495-puducherry.html (accessed on 31 December 2022).
- Ministry of Statistics and Program Implementation India: Puducherry per Capita Income 2021|Statista. Available online: https://www.statista.com/statistics/1117826/india-per-capita-income-puducherry/ (accessed on 15 December 2022).
- International Institute for Population Sciences (IIPS) and ICF. National Family Health Survey—4 District Fact Sheet Puducherry, 2015-16; Ministry of Health and Family Welfare, Government of India: New Delhi, India, 2017.
- Leuenberger, A.; Nassoro, T.; Said, K.; Fenner, L.; Sikalengo, G.; Letang, E.; Montresor, A.; Zhou, X.-N.; Steinmann, P.; Marti, H.; et al. Assessing Stool Quantities Generated by Three Specific Kato-Katz Thick Smear Templates Employed in Different Settings. Infect. Dis. Poverty 2016, 5, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krucken, J.; Fraundorfer, K.; Mugisha, J.C.; Ramunke, S.; Sifft, K.C.; Geus, D.; Habarugira, F.; Ndoli, J.; Sendegeya, A.; Mukampunga, C.; et al. Reduced Efficacy of Albendazole against Ascaris Lumbricoides in Rwandan Schoolchildren. Int. J. Parasitol. Drugs Drug Resist. 2017, 7, 262–271. [Google Scholar] [CrossRef]
- StataCorp. 2017 Stata Statiscal Software StataCorp. In Release 15.College Station; StataCorp LLC: College Station, TX, USA.
- Garrison, A.; Boivin, M.; Khoshnood, B.; Courtin, D.; Alao, J.; Mireku, M.; Ibikounle, M.; Massougbodji, A.; Cot, M.; Bodeau-Livinec, F. Soil-Transmitted Helminth Infection in Pregnancy and Long-Term Child Neurocognitive and Behavioral Development: A Prospective Mother-Child Cohort in Benin. PLoS Negl. Trop. Dis. 2021, 15, e0009260. [Google Scholar] [CrossRef]
- Jayaram, S.; Saya, G.K.; Rajkumari, N.; Ulaganeethi, R.; Roy, P.K.; Mathavaswami, V. Prevalence of Intestinal Parasitic Infection and Its Associated Factors among Children in Puducherry, South India: A Community-Based Study. J. Parasit. Dis. 2021, 45, 897–902. [Google Scholar] [CrossRef]
- Ministry of health and Family Welfare. National Deworming Day; Ministry of health and Family Welfare: New Delhi, India, 2016.
- Government of India. Swachh Bharat Mission. Available online: https://swachhbharatmission.gov.in/sbmcms/index.htm (accessed on 10 November 2022).
- Gebrehiwet, M.G.; Medhaniye, A.A.; Alema, H.B. Prevalence and Associated Factors of Soil Transmitted Helminthes among Pregnant Women Attending Antenatal Care in Maytsebri Primary Hospital, North Ethiopia. BMC Res. Notes 2019, 12, 644. [Google Scholar] [CrossRef]
- Brummaier, T.; Tun, N.W.; Min, A.M.; Gilder, M.E.; Archasuksan, L.; Proux, S.; Kiestra, D.; Charunwatthana, P.; Utzinger, J.; Paris, D.H.; et al. Burden of Soil-Transmitted Helminth Infection in Pregnant Refugees and Migrants on the Thailand-Myanmar Border: Results from a Retrospective Cohort. PLoS Negl. Trop. Dis. 2021, 15, e0009219. [Google Scholar] [CrossRef]
- Honkpéhèdji, Y.J.; Adegbite, B.R.; Zinsou, J.F.; Dejon-Agobé, J.C.; Edoa, J.R.; Zoleko Manego, R.; McCall, M.; Mbong Ngwese, M.; Lotola Mougeni, F.; Mombo-Ngoma, G.; et al. Association of Low Birth Weight and Polyparasitic Infection during Pregnancy in Lambaréné, Gabon. Trop. Med. Int. Health 2021, 26, 973–981. [Google Scholar] [CrossRef] [PubMed]
- Strunz, E.C.; Addiss, D.G.; Stocks, M.E.; Ogden, S.; Utzinger, J.; Freeman, M.C. Water, Sanitation, Hygiene, and Soil-Transmitted Helminth Infection: A Systematic Review and Meta-Analysis. PLoS Med. 2014, 11, e1001620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Getachew, M.; Yeshigeta, R.; Tiruneh, A.; Alemu, Y.; Dereje, E.; Mekonnen, Z. Soil-Transmitted Helminthic Infections and Geophagia among Pregnant Women in Jimma Town Health Institutions, Southwest Ethiopia. Ethiop. J. Health Sci. 2021, 31, 1033–1042. [Google Scholar]
- Conterno, L.O.; Turchi, M.D.; Corrêa, I.; Monteiro de Barros Almeida, R.A. Anthelmintic Drugs for Treating Ascariasis. Cochrane Database Syst. Rev. 2020, 4, CD010599. [Google Scholar] [CrossRef]
- Lau, R.; Chris, R.B.; Phuong, M.S.; Khatib, A.; Kopalakrishnan, S.; Bhasker, S.; Raheel, H.; Lecce, C.; Yegorov, S.; Mishra, S.; et al. Treatment of Soil-Transmitted Helminth Infections in Pregnancy: A Systematic Review and Meta-Analysis of Maternal Outcomes. J. Travel Med. 2020, 27, taz079. [Google Scholar] [CrossRef] [PubMed]
- Patel, C.; Coulibaly, J.T.; Hofmann, D.; N’Gbesso, Y.; Hattendorf, J.; Keiser, J. Efficacy and Safety of Albendazole in Hookworm-Infected Preschool-Aged Children, School-Aged Children, and Adults in Côte d’Ivoire: A Phase 2 Randomized, Controlled Dose-Finding Trial. Clin. Infect. Dis. 2021, 73, e494–e502. [Google Scholar] [CrossRef]
- Tee, M.Z.; Lee, S.C.; Er, Y.X.; Yap, N.J.; Ngui, R.; Easton, A.V.; Siow, V.W.Y.; Ng, K.S.; Boey, C.C.M.; Chua, K.H.; et al. Efficacy of Triple Dose Albendazole Treatment for Soil-Transmitted Helminth Infections. PLoS ONE 2022, 17, e0272821. [Google Scholar] [CrossRef]
- Steinmann, P.; Utzinger, J.; Du, Z.-W.; Jiang, J.-Y.; Chen, J.-X.; Hattendorf, J.; Zhou, H.; Zhou, X.-N. Efficacy of Single-Dose and Triple-Dose Albendazole and Mebendazole against Soil-Transmitted Helminths and Taenia Spp.: A Randomized Controlled Trial. PLoS ONE 2011, 6, e25003. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Number | Percentage |
|---|---|---|
| Age categories (Years) | ||
| Up to 25 | 317 | 48.8 |
| 26–30 | 232 | 35.7 |
| >30 | 101 | 15.5 |
| Occupation | ||
| Home maker | 445 | 68.5 |
| Working | 205 | 31.5 |
| Education | ||
| No/Up to primary | 17 | 2.7 |
| Secondary to higher secondary | 252 | 39.3 |
| Bachelor/Master’s | 372 | 58.0 |
| Gravida | ||
| Primi gravida | 385 | 59.2 |
| Multi gravida | 265 | 40.8 |
| No of living children | ||
| None | 402 | 61.9 |
| One | 223 | 34.3 |
| Two or three | 25 | 3.8 |
| Residence | ||
| Rural | 323 | 49.7 |
| Urban | 327 | 50.3 |
| Period of gestation | ||
| first | 282 | 43.4 |
| second | 347 | 53.4 |
| third | 21 | 3.2 |
| Hemoglobin status (g/dl) | ||
| Normal (≥11 gm/dl) | 310 | 48.0 |
| Mild (9–10.9 gm/dl) | 283 | 43.8 |
| Moderate (7–8.9 gm/dl) | 51 | 7.9 |
| Severe (<7 gm/dl) | 2 | 0.3 |
| Parameter | Number | Percentage |
|---|---|---|
| Handwashing after toilet use | ||
| No/sometimes | 52 | 8.0 |
| Always | 598 | 92.0 |
| Handwashing before food | ||
| No/sometimes | 111 | 17.1 |
| Always | 539 | 82.9 |
| Walking barefoot in outdoors | ||
| No | 239 | 36.8 |
| sometime/always | 411 | 63.2 |
| Open defecation | ||
| No | 615 | 94.6 |
| Yes | 35 | 5.4 |
| Drinking water | ||
| Tap | 571 | 87.9 |
| Purified | 79 | 12.2 |
| Nature of water | ||
| Boiled | 150 | 23.1 |
| Un boiled | 500 | 76.9 |
| Pet/Farm animal | ||
| No | 393 | 60.5 |
| Yes | 257 | 39.5 |
| Parameter | Total | Women with STH (n = 49) | Unadjusted PR | Adjusted PR | p Value |
|---|---|---|---|---|---|
| Age categories (Years) | |||||
| 17–25 | 317 | 20 (6.3) | 1 | 1 | |
| 26–30 | 232 | 21 (9.1) | 1.4 (0.8–2.6) | 1.3 (0.7–2.4) | 0.4 |
| >30 | 101 | 8 (7.9) | 1.3 (0.6–2.8) | 1.1 (0.5–2.5) | 0.87 |
| Education | |||||
| Up to primary school | 17 | 0 | |||
| Secondary/Higher secondary | 252 | 20 (7.9) | 1.1 (0.7–1.8) | ||
| Bachelor/Master’s degree | 372 | 28 (7.5) | 1 | ||
| Occupation | |||||
| Working | 205 | 17 (8.3) | 1.2 (0.7–2.0) | ||
| Not working | 445 | 32 (7.2) | 1 | ||
| Gravida | |||||
| Primi | 385 | 27 (7.0) | 1 | ||
| Multi | 243 | 22 (8.3) | 1.2 (0.7–2.0) | ||
| Number of living children | |||||
| None | 402 | 27 (6.7) | 1 | 1 | |
| One | 223 | 18 (8.1) | 1.2 (0.7–2.3) | 1.2 (0.7–2.1) | 0.59 |
| Two or three | 25 | 4 (16.0) | 2.4 (0.9–6.3) | 1.3 (0.4–4.7) | 0.7 |
| Period of gestation | |||||
| First trimester | 282 | 22 (7.8) | 1.2 (0.7–2.1) | 1.3 (0.7–2.3) | 0.42 |
| Second trimester | 347 | 23 (6.6) | 1 | 1 | |
| Third trimester | 21 | 4 (9.1) | 2.9 (1.1–7.6) | 3.1 (0.4–4.7) | 0.02 |
| Residence | |||||
| Rural | 323 | 20 (6.2) | 1 | 1 | |
| Urban | 327 | 29 (8.9) | 1.4 (0.8–2.5) | 1.5 (0.9–2.7) | 0.14 |
| Walking barefoot in outdoors | |||||
| Always/sometime | 411 | 34 (8.3) | 1.3 (0.8–2.4) | ||
| No | 239 | 15 (6.3) | 1 | ||
| Handwashing before meals with soap | |||||
| No/some times | 111 | 10 (9.0) | 1.2 (0.6–2.4) | ||
| Always | 539 | 39 (7.2) | 1 | ||
| Drinking water | |||||
| Tap | 571 | 44 (7.7) | 1.2 (0.5–3.0) | ||
| Purified | 79 | 5 (6.3) | 1 | ||
| Nature of water | |||||
| Boiled | 150 | 11 (7.3) | 1 | ||
| Not boiled | 500 | 38 (7.6) | 1.03 (0.54–2.0) | ||
| Handwashing after toilet use | |||||
| No/some times | 52 | 2 (3.9) | 0.5 (0.1–1.96) | ||
| Always | 598 | 47 (7.9) | 1 | ||
| Raw/unwashed vegetable | |||||
| Sometimes | 295 | 20 (6.8) | 1 | ||
| Never | 355 | 29 (8.2) | 1.2 (0.7–2.1) | ||
| Pet/Farm animals | |||||
| No | 393 | 33 (8.4) | 1.3 (0.8–2.4) | ||
| Yes | 257 | 16 (6.2) | 1 | ||
| Hemoglobin (g/dl) * | |||||
| Normal (≥11) | 310 | 18 (5.8) | 1 | 1 | |
| Mild anemia (9–10.9) | 283 | 24 (8.5) | 1.5 (0.8–2.6) | 1.7 (1.0–3.2) | 0.07 |
| Moderate anemia (7–8.9) | 51 | 5 (9.8) | 1.7 (0.7–4.3) | 2.0 (0.8–5.2) | 0.16 |
| Severe anemia (<7) | 2 | 1 (50.0) | 8.6 (2.0–37.0) | 8.1 (1.3–50.5) | 0.03 |
| H/o deworming in the previous year | |||||
| Yes | 49 | 3 (6.1) | 1 | ||
| No | 601 | 46 (7.7) | 1.3 (0.4–3.9) | ||
| Open defecation | |||||
| No | 615 | 47 (7.6) | 0.7 (0.2–3.0) | ||
| Yes | 35 | 2 (5.7) | 1 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ulaganeethi, R.; Saya, G.K.; Rajkumari, N.; Kumar, S.S.; Ganapathy, K.; Dorairajan, G. Soil-Transmitted Helminth Infections among Antenatal Women in Primary Care Settings in Southern India: Prevalence, Associated Factors and Effect of Anti-Helminthic Treatment. Trop. Med. Infect. Dis. 2023, 8, 48. https://doi.org/10.3390/tropicalmed8010048
Ulaganeethi R, Saya GK, Rajkumari N, Kumar SS, Ganapathy K, Dorairajan G. Soil-Transmitted Helminth Infections among Antenatal Women in Primary Care Settings in Southern India: Prevalence, Associated Factors and Effect of Anti-Helminthic Treatment. Tropical Medicine and Infectious Disease. 2023; 8(1):48. https://doi.org/10.3390/tropicalmed8010048
Chicago/Turabian StyleUlaganeethi, Revathi, Ganesh Kumar Saya, Nonika Rajkumari, Swetha S. Kumar, Kalaiselvan Ganapathy, and Gowri Dorairajan. 2023. "Soil-Transmitted Helminth Infections among Antenatal Women in Primary Care Settings in Southern India: Prevalence, Associated Factors and Effect of Anti-Helminthic Treatment" Tropical Medicine and Infectious Disease 8, no. 1: 48. https://doi.org/10.3390/tropicalmed8010048