
Prevalence and Risk Factors for Lymphocytic Choriomeningitis Virus Infection in Continental Croatian Regions

 ,
,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
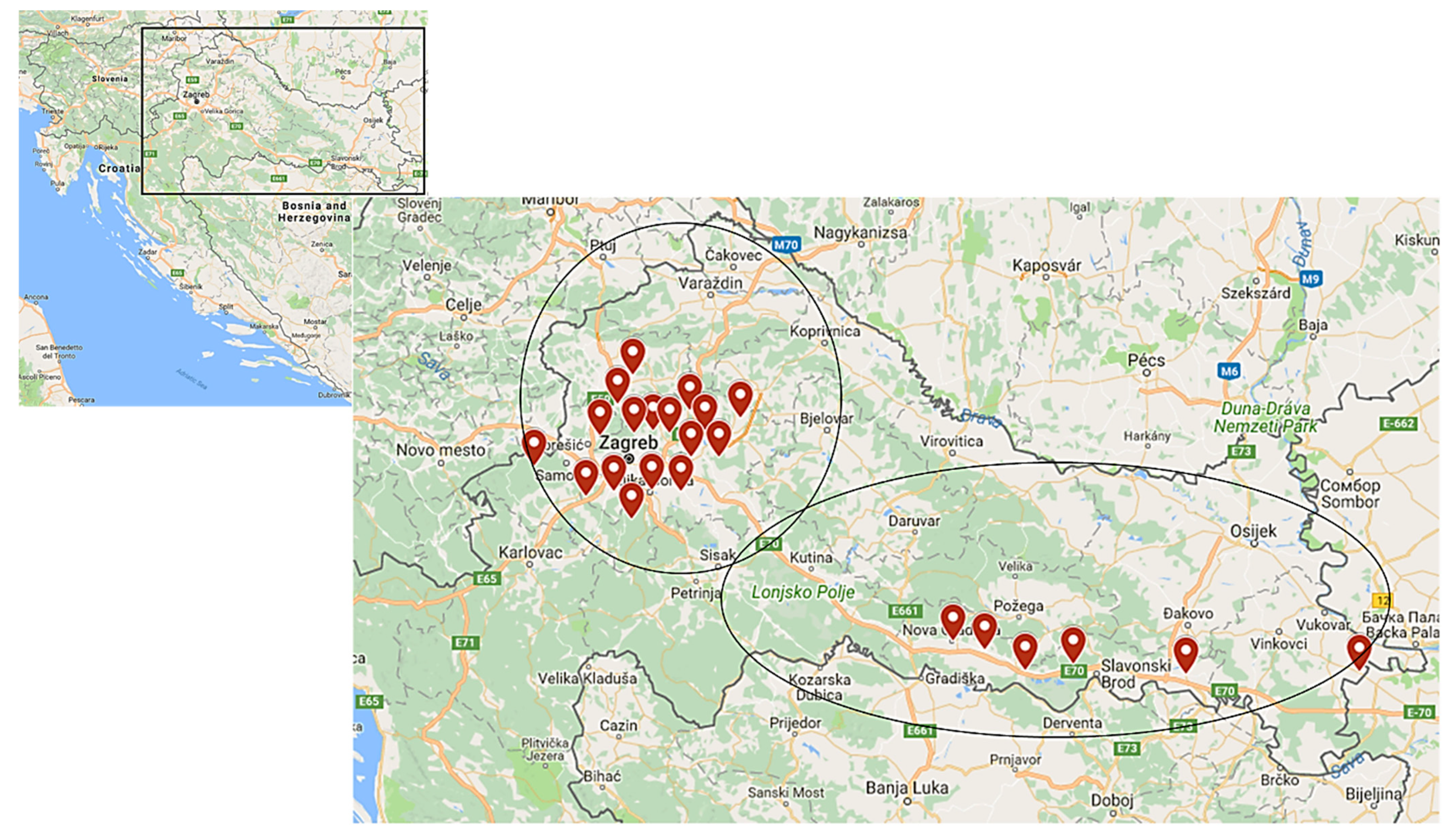
2.2. Geographic Features of the Study Area
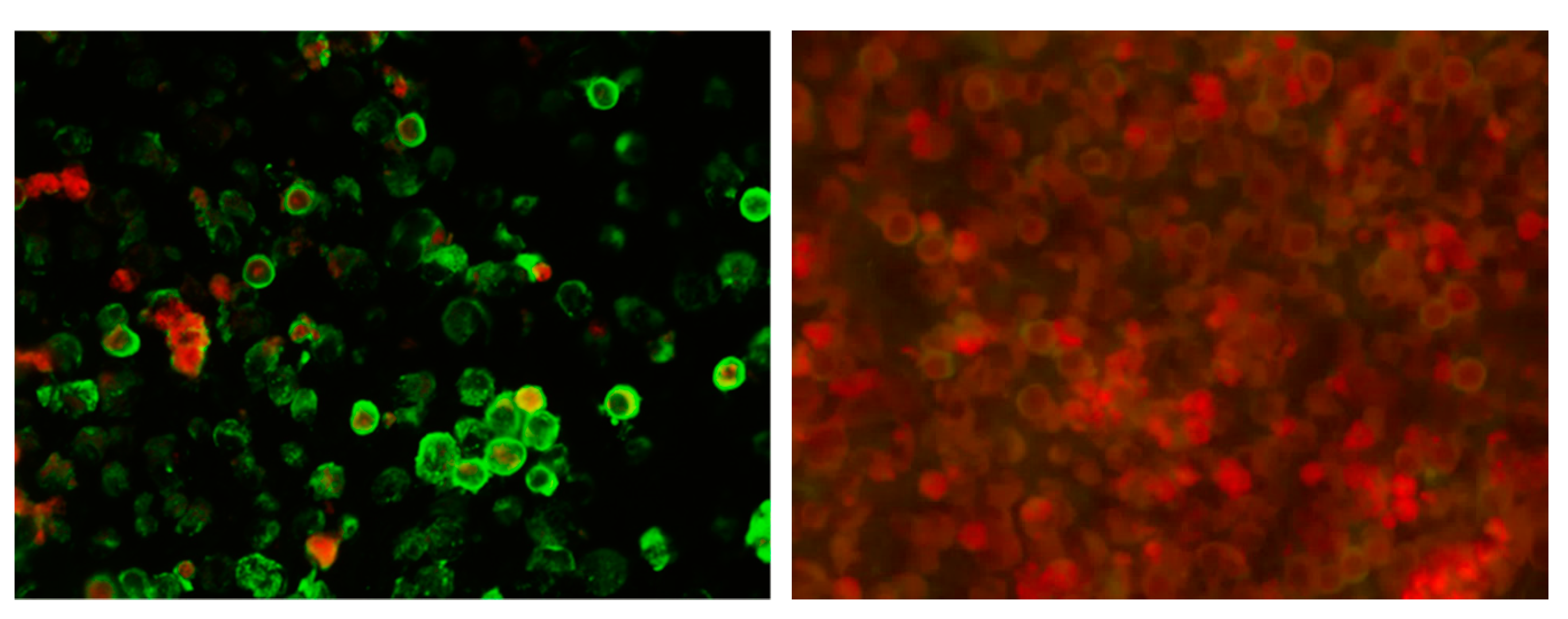
2.3. Serological Testing
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wilson, M.R.; Peters, C.J. Diseases of the central nervous system caused by lymphocytic choriomeningitis virus and other arenaviruses. Handb. Clin. Neurol. 2014, 123, 671–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tagliapietra, V.; Rosa, R.; Hauffe, H.C.; Laakkonen, J.; Voutilainen, L.; Vapalahti, O.; Vaheri, A.; Henttonen, H.; Rizzoli, A. Spatial and temporal dynamics of lymphocytic choriomeningitis virus in wild rodents, northern Italy. Emerg. Infect. Dis. 2009, 15, 1019–1025. [Google Scholar] [CrossRef] [PubMed]
- Amman, B.R.; Pavlin, B.I.; Albariño, C.G.; Comer, J.A.; Erickson, B.R.; Oliver, J.B.; Sealy, T.K.; Vincent, M.J.; Nichol, S.T.; Paddock, C.D.; et al. Pet rodents and fatal lymphocytic choriomeningitis in transplant patients. Emerg. Infect. Dis. 2007, 13, 719–725. [Google Scholar] [CrossRef] [PubMed]
- Lapošová, K.; Pastoreková, S.; Tomášková, J. Lymphocytic choriomeningitis virus: Invisible but not innocent. Acta Virol. 2013, 57, 160–170. [Google Scholar] [CrossRef] [Green Version]
- Mrzljak, A.; Novak, R.; Pandak, N.; Tabain, I.; Franusic, L.; Barbic, L.; Bogdanic, M.; Savic, V.; Mikulic, D.; Pavicic-Saric, J.; et al. Emerging and neglected zoonoses in transplant population. World J. Transplant. 2020, 10, 47–63. [Google Scholar] [CrossRef]
- Kinori, M.; Schwartzstein, H.; Zeid, J.L.; Kurup, S.P.; Mets, M.B. Congenital lymphocytic choriomeningitis virus-an underdiagnosed fetal teratogen. J. AAPOS 2018, 22, 79–81. [Google Scholar] [CrossRef]
- Humbertclaude, V.; Tourtet, S.; Semprino, M.; Roubertie, A.; Rivier, F.; Leboucq, N.; Astruc, J.; Echenne, B. Acute myelitis of an unusual cause in a child: The lymphocytic choriomeningitis virus. Arch. Pediatr. 2001, 8, 282–285. [Google Scholar] [CrossRef]
- Bonthius, D.J. The Arenaviruses. In Neurotropic Viral Infections, 2nd ed.; Reiss, C.S., Ed.; Springer International Publishing: Cham, Switzerland, 2016; Volume 1, pp. 147–174. [Google Scholar] [CrossRef]
- Macneil, A.; Ströher, U.; Farnon, E.; Campbell, S.; Cannon, D.; Paddock, C.D.; Drew, C.P.; Kuehnert, M.; Knust, B.; Gruenenfelder, R.; et al. Solid organ transplant-associated lymphocytic choriomeningitis, United States, 2011. Emerg. Infect. Dis. 2012, 18, 1256–1262. [Google Scholar] [CrossRef]
- Schafer, I.J.; Miller, R.; Ströher, U.; Knust, B.; Nichol, S.T.; Rollin, P.E. Centers for Disease Control and Prevention (CDC). Notes from the field: A cluster of lymphocytic choriomeningitis virus infections transmitted through organ transplantation—Iowa, 2013. Morb. Mortal. Wkly. Rep. 2014, 14, 1459. [Google Scholar] [CrossRef]
- Mathur, G.; Yadav, K.; Ford, B.; Schafer, I.J.; Basavaraju, S.V.; Knust, B.; Shieh, W.J.; Hill, S.; Locke, G.D.; Quinlisk, P.; et al. High clinical suspicion of donor-derived disease leads to timely recognition and early intervention to treat solid organ transplant-transmitted lymphocytic choriomeningitis virus. Transpl. Infect. Dis. 2017, 19, e12707. [Google Scholar] [CrossRef]
- Barton, L.L.; Mets, M.B.; Beauchamp, C.L. Lymphocytic choriomeningitis virus: Emerging fetal teratogen. Am. J. Obstet. Gynecol. 2002, 187, 1715–1716. [Google Scholar] [CrossRef]
- Bonthius, D.J.; Wright, R.; Tseng, B.; Barton, L.; Marco, E.; Karacay, B.; Larsen, P.D. Congenital lymphocytic choriomeningitis virus infection: Spectrum of disease. Ann. Neurol. 2007, 62, 347–355. [Google Scholar] [CrossRef]
- Bonthius, D.J. Lymphocytic choriomeningitis virus: An underrecognized cause of neurologic disease in the fetus, child, and adult. Semin. Pediatr. Neurol. 2012, 19, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Anderson, J.L.; Levy, P.T.; Leonard, K.B.; Smyser, C.D.; Tychsen, L.; Cole, F.S. Congenital lymphocytic choriomeningitis virus: When to consider the diagnosis. J. Child. Neurol. 2014, 29, 837–842. [Google Scholar] [CrossRef] [Green Version]
- Delaine, M.; Weingertner, A.S.; Nougairede, A.; Lepiller, Q.; Fafi-Kremer, S.; Favre, R.; Charrel, R. Microcephaly Caused by Lymphocytic Choriomeningitis Virus. Emerg. Infect. Dis. 2017, 23, 1548–1550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lledó, L.; Gegúndez, M.I.; Saz, J.V.; Bahamontes, N.; Beltrán, M. Lymphocytic choriomeningitis virus infection in a province of Spain: Analysis of sera from the general population and wild rodents. J. Med. Virol. 2003, 70, 273–275. [Google Scholar] [CrossRef]
- Riera, L.; Castillo, E.; Del Carmen Saavedra, M.; Priotto, J.; Sottosanti, J.; Polop, J.; Ambrosio, A.M. Serological study of the lymphochoriomeningitis virus (LCMV) in an inner city of Argentina. J. Med. Virol. 2005, 76, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Kallio-Kokko, H.; Laakkonen, J.; Rizzoli, A.; Tagliapietra, V.; Cattadori, I.; Perkins, S.E.; Hudson, P.J.; Cristofolini, A.; Versini, W.; Vapalahti, O.; et al. Hantavirus and arenavirus antibody prevalence in rodents and humans in Trentino, Northern Italy. Epidemiol. Infect. 2006, 134, 830–836. [Google Scholar] [CrossRef] [PubMed]
- Barakat, A.M.; Lapahat, O.; Hasoni, H.J. Lymphocytic choriomeningitis virus (LCMV) in southern Iraq. Int. J. Sci. Eng. Res. 2015, 6, 1523–1535. [Google Scholar]
- Van Cuong, N.; Carrique-Mas, J.; Vo Be, H.; An, N.N.; Tue, N.T.; Anh, N.L.; Anh, P.H.; Phuc, N.T.; Baker, S.; Voutilainen, L.; et al. Rodents and risk in the Mekong Delta of Vietnam: Seroprevalence of selected zoonotic viruses in rodents and humans. Vector Borne Zoonotic Dis. 2015, 15, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Fevola, C.; Kuivanen, S.; Smura, T.; Vaheri, A.; Kallio-Kokko, H.; Hauffe, H.C.; Vapalahti, O.; Jääskeläinen, A.J. Seroprevalence of lymphocytic choriomeningitis virus and Ljungan virus in Finnish patients with suspected neurological infections. J. Med. Virol. 2018, 90, 429–435. [Google Scholar] [CrossRef]
- Alburkat, H.; Jääskeläinen, A.J.; Barakat, A.M.; Hasony, H.J.; Sironen, T.; Al-Hello, H.; Smura, T.; Vapalahti, O. Lymphocytic Choriomeningitis Virus Infections and Seroprevalence, Southern Iraq. Emerg. Infect. Dis. 2020, 26, 3002–3006. [Google Scholar] [CrossRef]
- Juncker-Voss, M.; Prosl, H.; Lussy, H.; Enzenberg, U.; Auer, H.; Lassnig, H.; Müller, M.; Nowotny, N. Screening for antibodies against zoonotic agents among employees of the Zoological Garden of Vienna, Schönbrunn, Austria. Berl. Munch. Tierarztl. Wochenschr. 2004, 117, 404–409. [Google Scholar]
- Miletić-Medved, M. Zoonoses in Forestry Workers in Central Posavina. Ph.D. Thesis, School of Medicine University of Zagreb, Zagreb, Croatia, 2006. (In Croatian). [Google Scholar]
- Dobec, M.; Dzelalija, B.; Punda-Polic, V.; Zoric, I. High prevalence of antibodies to lymphocytic choriomeningitis virus in a murine typhus endemic region in Croatia. J. Med. Virol. 2006, 78, 1643–1647. [Google Scholar] [CrossRef]
- Tadin, A.; Tokarz, R.; Markotić, A.; Margaletić, J.; Turk, N.; Habuš, J.; Svoboda, P.; Vucelja, M.; Desai, A.; Jain, K.; et al. Molecular Survey of Zoonotic Agents in Rodents and Other Small Mammals in Croatia. Am. J. Trop. Med. Hyg. 2016, 94, 466–473. [Google Scholar] [CrossRef]
- Cordey, S.; Sahli, R.; Moraz, M.L.; Estrade, C.; Morandi, L.; Cherpillod, P.; Charrel, R.N.; Kunz, S.; Kaiser, L. Analytical validation of a lymphocytic choriomeningitis virus real-time RT-PCR assay. J. Virol. Methods 2011, 177, 118–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tagliapietra, V.; Rosà, R.; Rossi, C.; Rosso, F.; Hauffe, H.C.; Tommasini, M.; Versini, W.; Cristallo, A.F.; Rizzoli, A. Emerging Rodent-Borne Viral Zoonoses in Trento, Italy. Ecohealth 2018, 15, 695–704. [Google Scholar] [CrossRef]
- Ambrosio, A.M.; Saavedra, M.C.; Gamboa Graciela, S.; Maiza, A.S.; Mariani Mauricio, A. Ecological and epidemiological features of lymphocytic choriomeningitis virus activity in Argentina. Curr. Top. Virol. 2014, 12, 53–63. [Google Scholar]
- Stephensen, C.B.; Blount, S.R.; Lanford, R.E.; Holmes, K.V.; Montali, R.J.; Fleenor, M.E.; Shaw, J.F. Prevalence of serum antibodies against lymphocytic choriomeningitis virus in selected populations from two U.S. cities. J. Med. Virol. 1992, 38, 27–31. [Google Scholar] [CrossRef]
- Marrie, T.J.; Saron, M.F. Seroprevalence of lymphocytic choriomeningitis virus in Nova Scotia. Am. J. Trop. Med. Hyg. 1998, 58, 47–49. [Google Scholar] [CrossRef]
- de Lamballerie, X.; Fulhorst, C.F.; Charrel, R.N. Prevalence of antibodies to lymphocytic choriomeningitis virus in blood donors in southeastern France. Transfusion 2007, 47, 172–173. [Google Scholar] [CrossRef]
- Knust, B.; Macneil, A.; Wong, S.J.; Backenson, P.B.; Gibbons, A.; Rollin, P.E.; Nichol, S.T. Exposure to lymphocytic choriomeningitis virus. Emerg. Infect. Dis. 2011, 17, 1324–1325. [Google Scholar] [CrossRef]
- Elbers, A.R.W.; Vecht, U.; Osterhaus, A.D.M.E.; Groen, J.; Wisselink, H.J.; Diepersloot, R.J.A.; Tielen, M.J.M. Low prevalence of antibodies against the zoonotic agents Brucella abortus, Leptospira spp., Streptococcus suis serotype II, Hantavirus, and lymphocytic choriomeningitis virus among veterinarians and pig farmers in the southern part of the Netherlands. Vet. Q. 1999, 21, 50–54. [Google Scholar] [CrossRef]
- Moll van Charante, A.W.; Groen, J.; Osterhaus, A.D. Risk of infections transmitted by arthropods and rodents in forestry workers. Eur. J. Epidemiol. 1994, 10, 349–351. [Google Scholar] [CrossRef] [Green Version]
- Barton, L.L.; Mets, M.B. Congenital lymphocytic choriomeningitis virus infection: Decade of rediscovery. Clin. Infect. Dis. 2001, 33, 370–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadin, A.; Bjedov, L.; Margaletić, J.; Zibrat, B.; Krajinović, L.C.; Svoboda, P.; Kurolt, I.C.; Majetić, Z.S.; Turk, N.; Ðaković Rode, O.; et al. High infection rate of bank voles (Myodes glareolus) with Puumala virus is associated with a winter outbreak of haemorhagic fever with renal syndrome in Croatia. Epidemiol. Infect. 2014, 142, 1945–1951. [Google Scholar] [CrossRef]
- Medved, M.M.; Markotić, A.; Cebalo, L.; Turković, B.; Zupanc, T.A. Haemorrhagic fever with renal syndrome in Croatia. Lancet 2002, 360, 415–416. [Google Scholar] [CrossRef]
- Vilibic-Cavlek, T.; Furic, A.; Barbic, L.; Tabain, I.; Stevanovic, V.; Mlinaric-Galinovic, G. Clinical and virological characteristics of hantavirus infections in a 2014 Croatian outbreak. J. Infect. Dev. Ctries. 2017, 11, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Lovrić, Z.; Kolarić, B.; Kosanović Ličina, M.L.; Tomljenović, M.; Ðaković Rode, O.; Danis, K.; Kaić, B.; Tešić, V. An outbreak of haemorrhagic fever with renal syndrome linked with mountain recreational activities in Zagreb, Croatia, 2017. Epidemiol. Infect. 2018, 146, 1236–1239. [Google Scholar] [CrossRef] [Green Version]
- Vilibic-Cavlek, T.; Barbic, L.; Mrzljak, A.; Brnic, D.; Klobucar, A.; Ilic, M.; Janev-Holcer, N.; Bogdanic, M.; Jemersic, L.; Stevanovic, V.; et al. Emerging and Neglected Viruses of Zoonotic Importance in Croatia. Pathogens 2021, 10, 73. [Google Scholar] [CrossRef]
- Ledina, D.; Bradarić, N.; Borčić, B.; Turković, B.; Ivić, I.; Bakić, J.; Erceg, M.; Tvrtković, N. Dinara—New natural focus of hemorrhagic fever with renal syndrome in Croatia. Croat. Med. J. 2002, 43, 576–580. [Google Scholar] [PubMed]
- Cvetko, L.; Markotić, A.; Plyusnina, A.; Margaletić, J.; Miletić-Medved, M.; Turk, N.; Milas, Z.; Avsic-Zupanc, T.; Plyusnin, A. Puumala virus in Croatia in the 2002 HFRS outbreak. J. Med. Virol. 2005, 77, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Tadin, A.; Turk, N.; Korva, M.; Margaletić, J.; Beck, R.; Vucelja, M.; Habuš, J.; Svoboda, P.; Zupanc, T.A.; Henttonen, H.; et al. Multiple co-infections of rodents with hantaviruses, Leptospira, and Babesia in Croatia. Vector Borne Zoonotic Dis. 2012, 12, 388–392. [Google Scholar] [CrossRef] [Green Version]
- Plyusnina, A.; Krajinović, L.C.; Margaletić, J.; Niemimaa, J.; Nemirov, K.; Lundkvist, Å.; Markotić, A.; Miletić-Medved, M.; Avšič-Županc, T.; Henttonen, H.; et al. Genetic evidence for the presence of two distinct hantaviruses associated with Apodemus mice in Croatia and analysis of local strains. J. Med. Virol. 2011, 83, 108–114. [Google Scholar] [CrossRef] [Green Version]
- Ovčar, D. Seroprevalence of Arthropod-Borne and Rodent-Borne Viral Zoonoses in Continental Regions of Croatia. Master’s Thesis, School of Medicine University of Zagreb, Zagreb, Croatia, 2019. [Google Scholar]
- Childs, J.E.; Klein, S.L.; Glass, G.E. A Case Study of Two Rodent-Borne Viruses: Not Always the Same Old Suspects. Front. Ecol. Evol. 2019, 7, 35. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Population Group | N Tested (%) | LCMV IgG N (%) | 95% CI |
|---|---|---|---|
| Overall | 338 (100) | 23 (6.8) | 4.4–10.0 |
| Exposed persons | 122 (36.1) | 12 (9.8) | 5.2–16.6 |
| General population | 115 (34.0) | 7 (6.1) | 2.5–12.1 |
| Pregnant women | 101 (29.9) | 4 (3.9) | 1.1–9.8 |
| Characteristic | N Tested (%) | N Positive (%) | 95% CI | p Value | |
|---|---|---|---|---|---|
| Population group | Exposed | 122 (36.1) | 12 (9.8) | 5.2–16.6 | 0.116 |
| Non-exposed | 216 (63.9) | 11 (5.1) | 2.6–8.9 | ||
| Gender | Male | 169 (50.0) | 15 (8.9) | 4.6–13.5 | 0.338 |
| Female | 169 (50.0) | 8 (4.7) | 2.5–9.9 | ||
| Age group | ≤30 years | 66 (19.5) | 4 (6.1) | 1.7–15.0 | 0.102 |
| 31–40 years | 127 (37.6) | 5 (3.9) | 0.9–7.9 | ||
| 41–50 years | 56 (16.6) | 7 (12.5) | 5.3–22.4 | ||
| 50+ years | 89 (26.3) | 7 (7.9) | 3.3–15.7 | ||
| Education | ≤Elementary school | 46 (13.6) | 5 (10.9) | 3.6–12.3 | 0.405 |
| High school | 205 (60.7) | 14 (6.8) | 3.8–11.1 | ||
| University | 87 (25.8) | 4 (4.6) | 1.3–11.4 | ||
| Place of residence | Urban | 175 (51.8) | 8 (4.6) | 2.0–8.8 | 0.129 |
| Suburban/rural | 163 (48.2) | 15 (9.2) | 5.2–14.7 | ||
| Water source | Tap | 268 (79.3) | 15 (5.6) | 3.2–9.1 | 0.107 |
| Well | 70 (20.7) | 8 (11.4) | 5.1–21.3 | ||
| Food storage in basement | Yes | 58 (17.2) | 5 (8.6) | 2.9–19.0 | 0.392 |
| No | 280 (82.8) | 18 (6.4) | 3.9–10.0 | ||
| Contact with rodents * | Yes | 32 (9.5) | 5 (15.6) | 5.3–32.8 | 0.054 |
| No | 306 (90.5) | 18 (5.9) | 3.5–9.1 | ||
| Companion animals (dog, cat) | Yes | 173 (51.2) | 12 (6.9) | 3.6–11.8 | 0.922 |
| No | 165 (48.8) | 11 (6.7) | 3.4–11.6 | ||
| Characteristic | OR | 95% CI (OR) |
|---|---|---|
| Male vs. female gender | 1.605 | 0.675−3.817 |
| Age (one-year increase) | 1.017 | 0.986–1.049 |
| ≤Elementary school education | 1 | |
| High school education | 0.601 | 0.205–1.761 |
| University education | 0.395 | 0.100–1.550 |
| Area of residence (suburban/rural vs. urban) | 2.114 | 0.872–5.128 |
| Food storage in basement (yes vs. no) | 1.373 | 0.488–3.861 |
| Water source (well vs. tap) | 2.176 | 0.883–5.363 |
| Presence of rodents in house/yard; cleaning rodents’ nests (yes vs. no) | 2.962 * | 1.019–8.607 * |
| Companion animals: cat/dog (yes vs. no) | 1.043 | 0.447–2.435 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vilibic-Cavlek, T.; Oreski, T.; Korva, M.; Kolaric, B.; Stevanovic, V.; Zidovec-Lepej, S.; Tabain, I.; Jelicic, P.; Miklausic-Pavic, B.; Savic, V.; et al. Prevalence and Risk Factors for Lymphocytic Choriomeningitis Virus Infection in Continental Croatian Regions. Trop. Med. Infect. Dis. 2021, 6, 67. https://doi.org/10.3390/tropicalmed6020067
Vilibic-Cavlek T, Oreski T, Korva M, Kolaric B, Stevanovic V, Zidovec-Lepej S, Tabain I, Jelicic P, Miklausic-Pavic B, Savic V, et al. Prevalence and Risk Factors for Lymphocytic Choriomeningitis Virus Infection in Continental Croatian Regions. Tropical Medicine and Infectious Disease. 2021; 6(2):67. https://doi.org/10.3390/tropicalmed6020067
Chicago/Turabian StyleVilibic-Cavlek, Tatjana, Tena Oreski, Misa Korva, Branko Kolaric, Vladimir Stevanovic, Snjezana Zidovec-Lepej, Irena Tabain, Pavle Jelicic, Bozana Miklausic-Pavic, Vladimir Savic, and et al. 2021. "Prevalence and Risk Factors for Lymphocytic Choriomeningitis Virus Infection in Continental Croatian Regions" Tropical Medicine and Infectious Disease 6, no. 2: 67. https://doi.org/10.3390/tropicalmed6020067