
Identifying Strategies to Mitigate Cybersickness in Virtual Reality Induced by Flying with an Interactive Travel Interface



Abstract
:1. Introduction
2. Background
2.1. Theories on what Causes Cybersickness
2.2. Factors That Influence Cybersickness
2.2.1. Posture and Embodiment
2.2.2. Field of View
2.2.3. Flicker
2.2.4. Virtual Movement and Altitude
2.3. Strategies Applied to Mitigate Cybersickness
2.3.1. FOV Manipulation
2.3.2. Resolving Sensory Conflict with Vibration
2.3.3. Visual Blurring
2.4. Measures of Cybersickness
2.4.1. Subjective Measures
2.4.2. Physiological Measures
2.5. Summary
3. Material and Methods
3.1. Hypotheses
- Hypotheses 1: Manipulating FOV in VR with a vignette based on virtual speed and eye-gaze direction mitigates CS.
- Hypotheses 2: Adding a first-person perspective with member representation to a VR experience mitigates CS.
- Hypotheses 3: Simulating vibration and airflow in a VR experience mitigates CS.
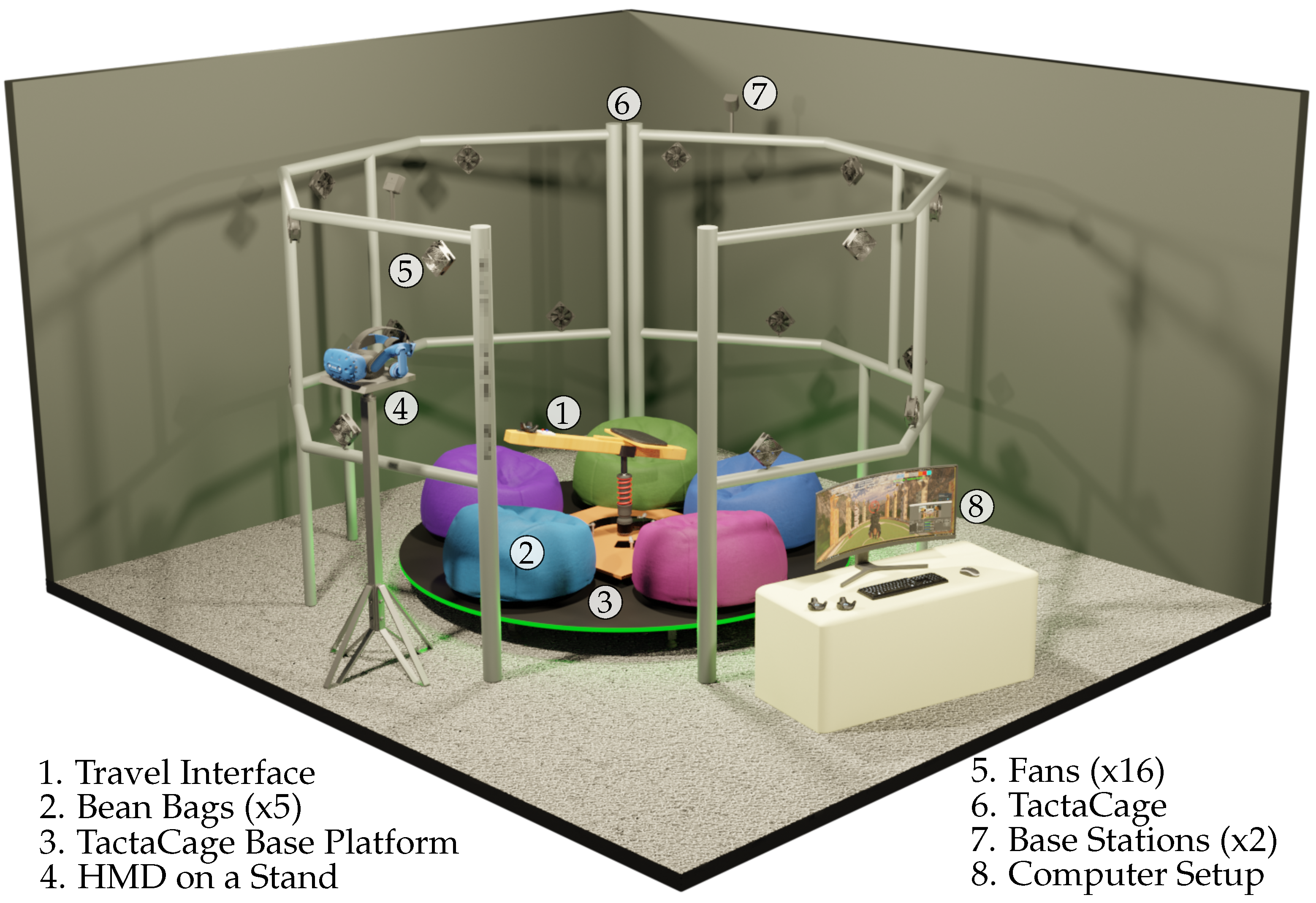
3.2. Experience Design
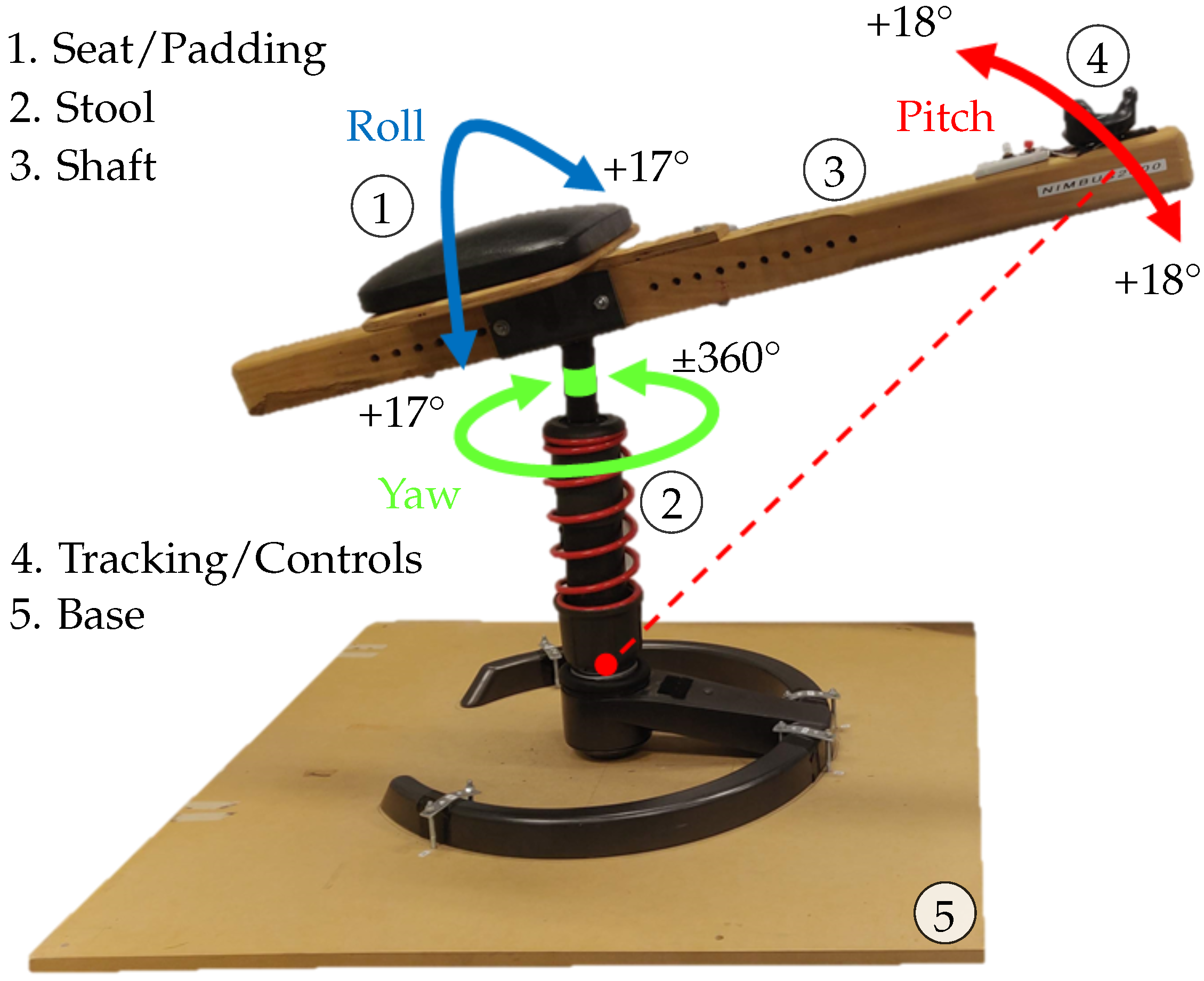
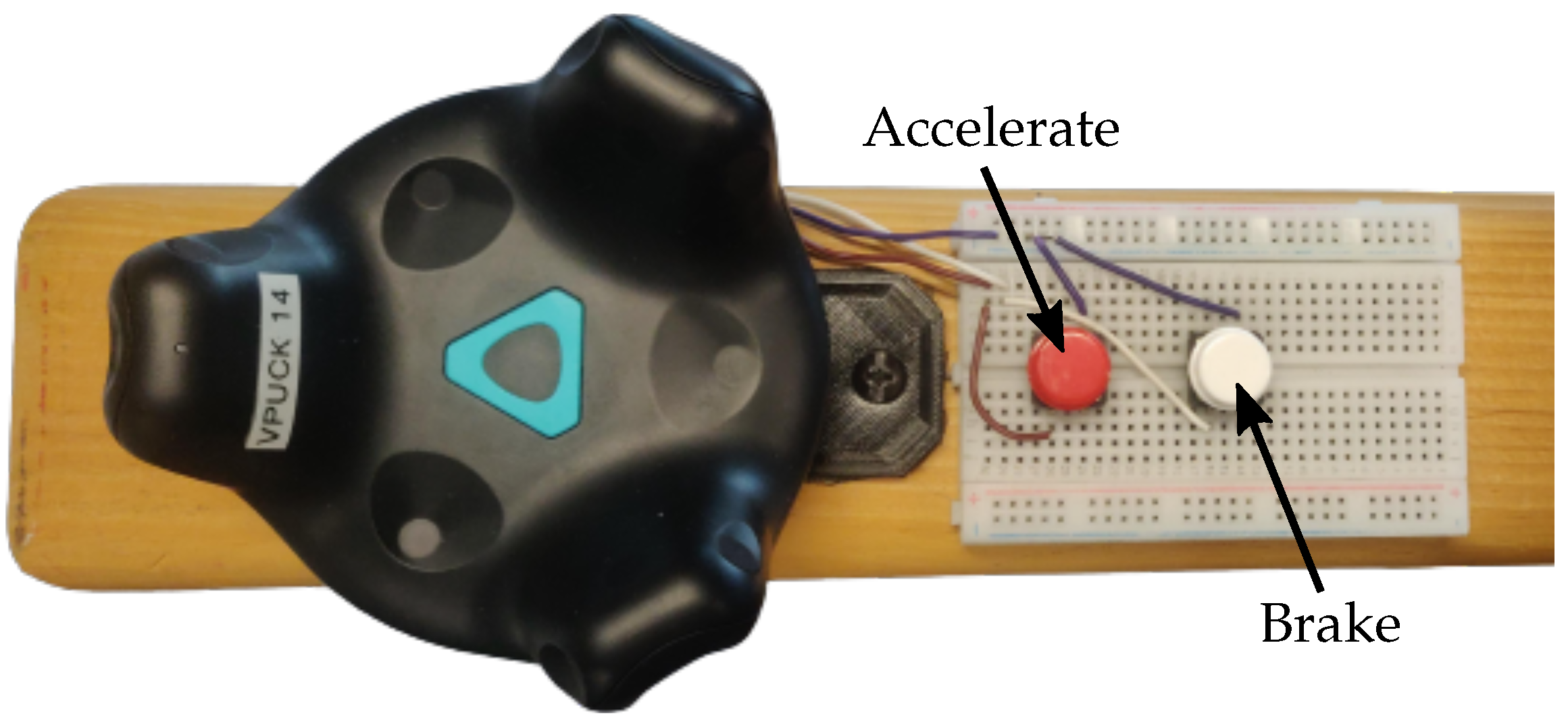
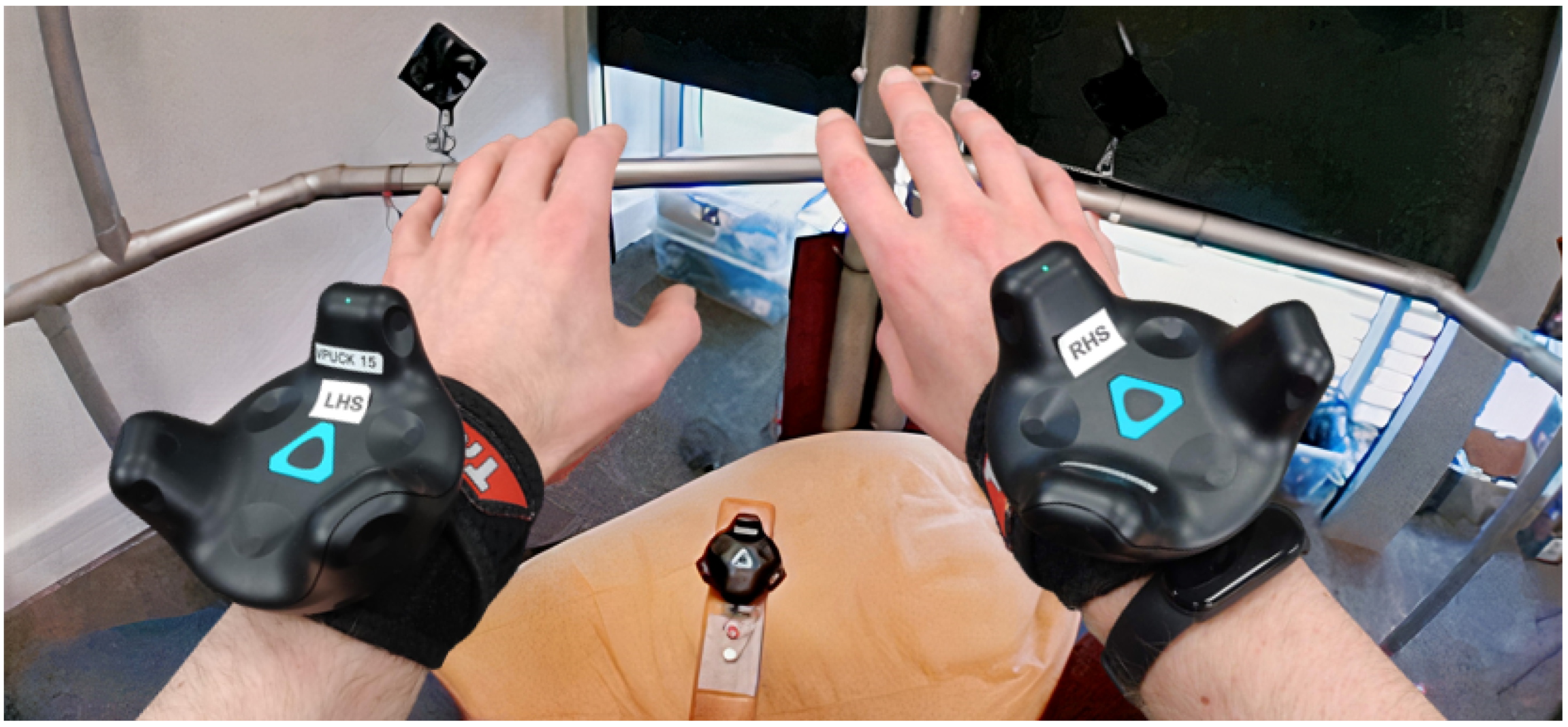
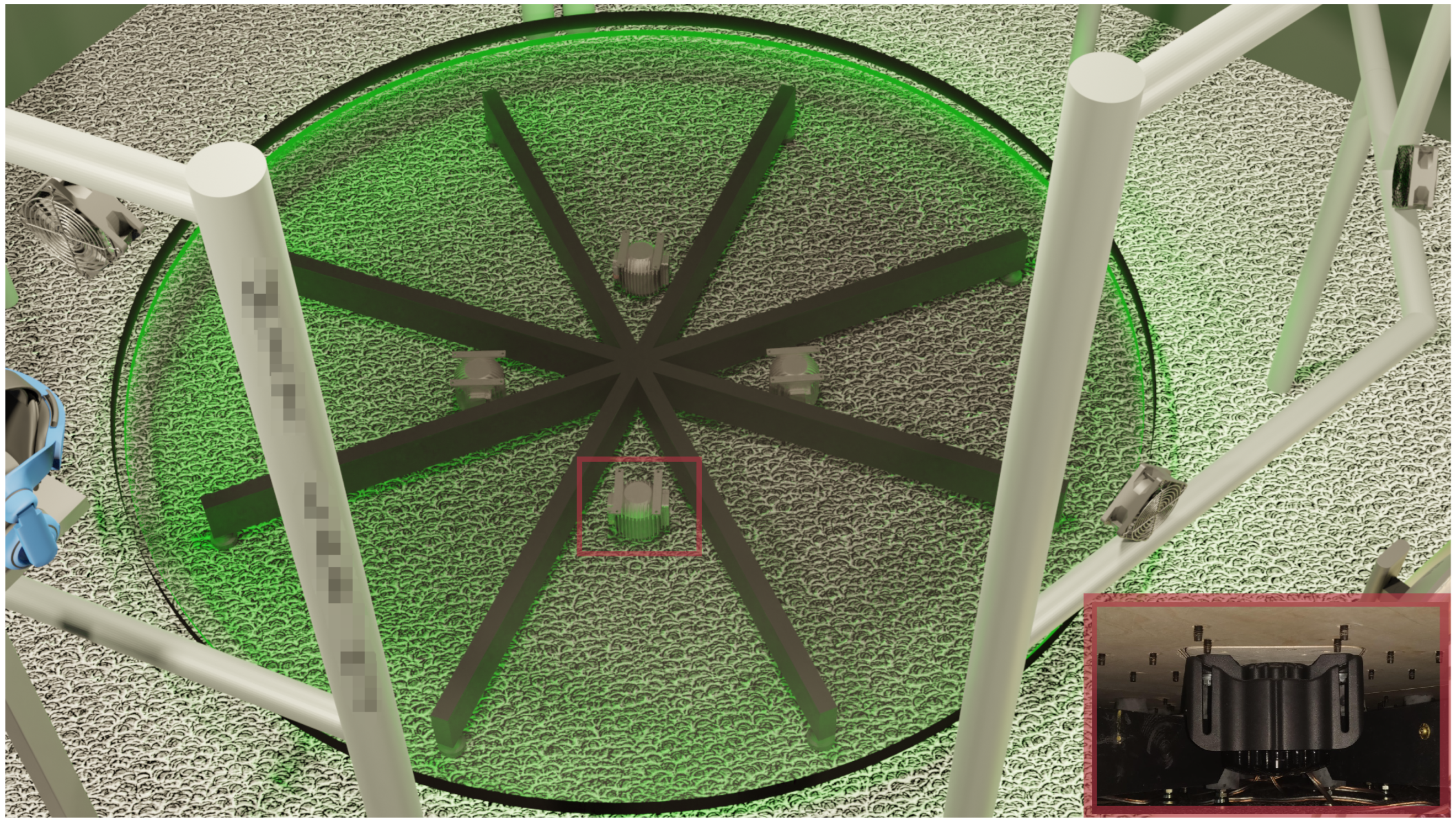
3.3. Travel Interface
3.4. Control System
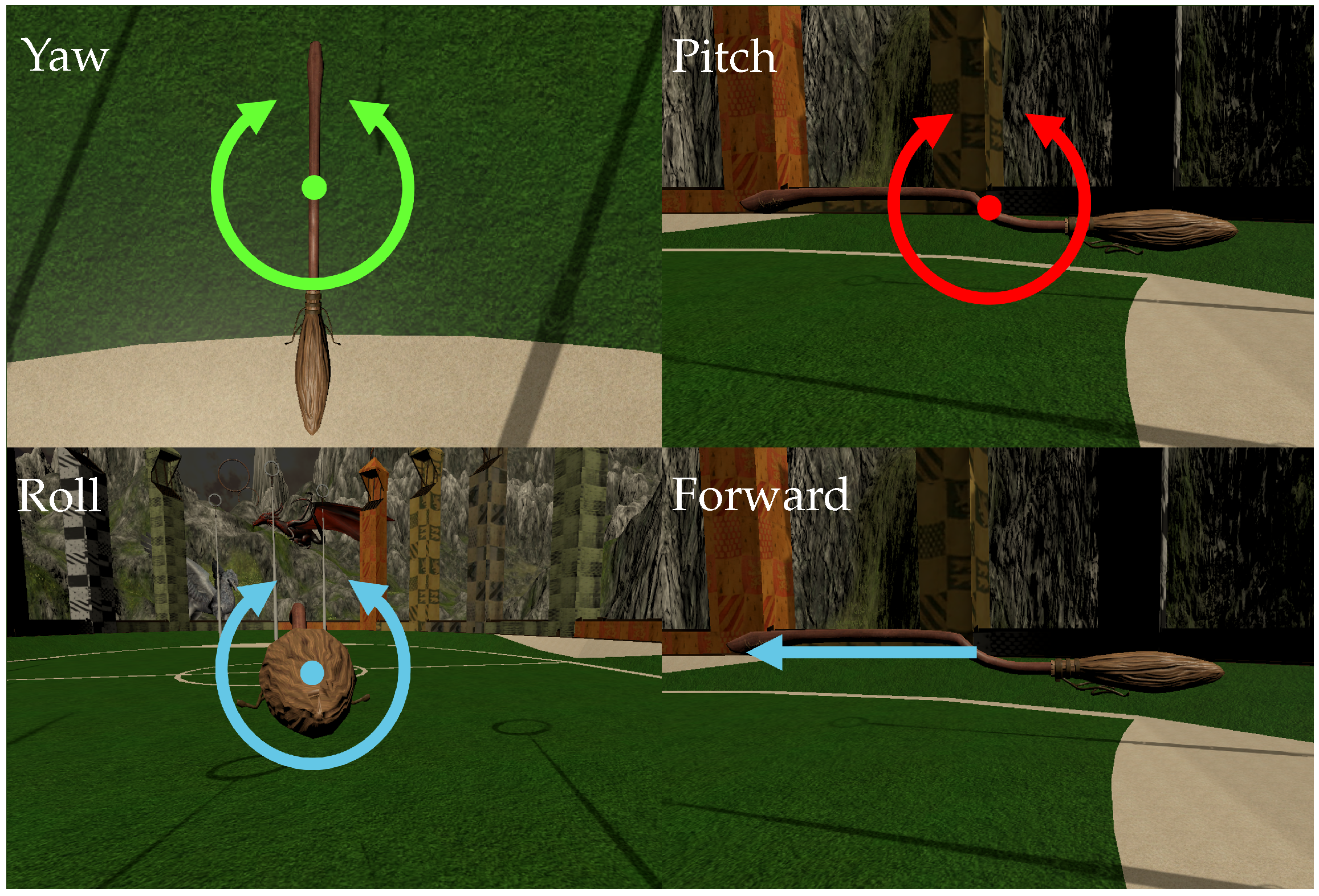
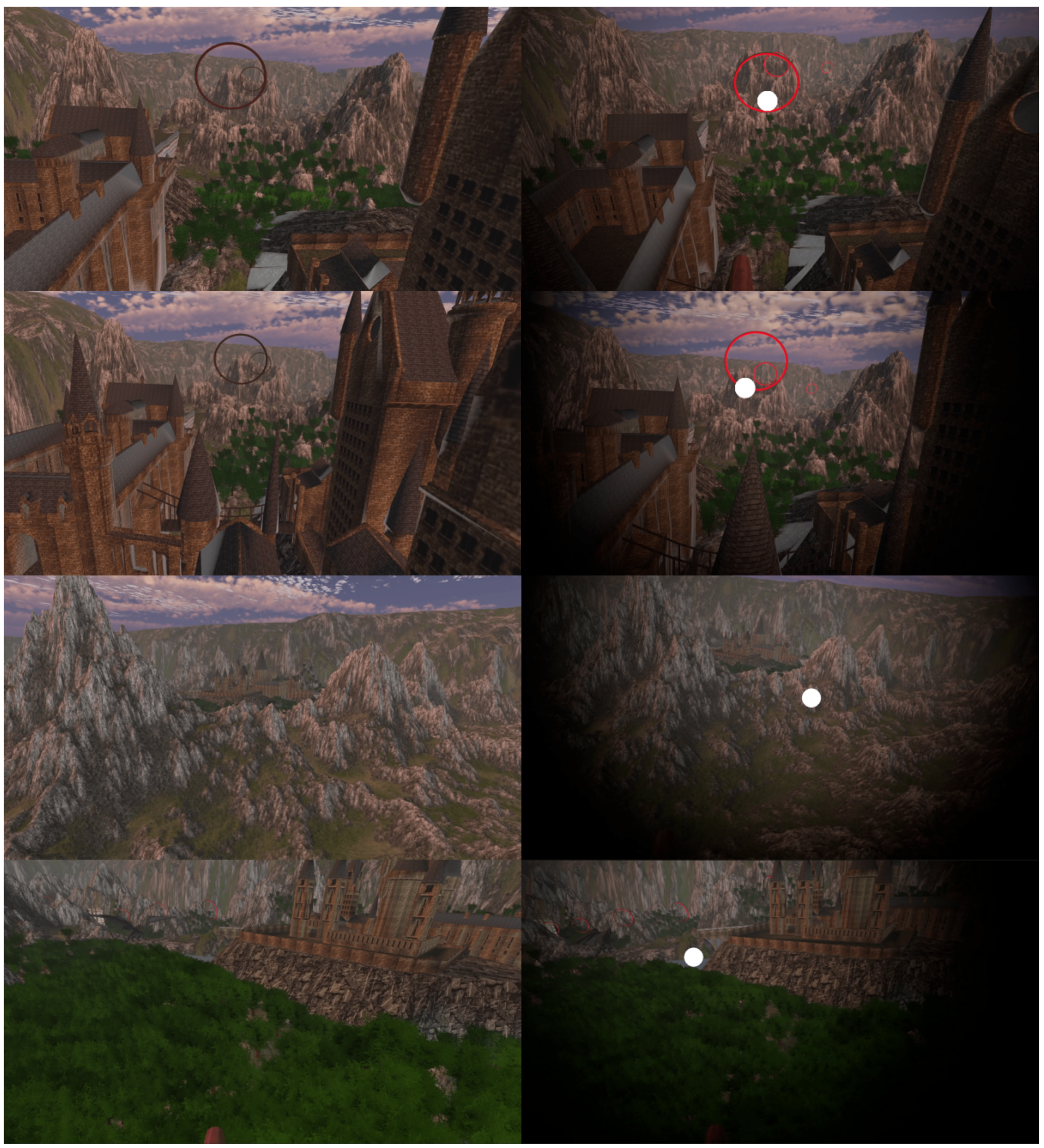
3.5. Virtual Environment
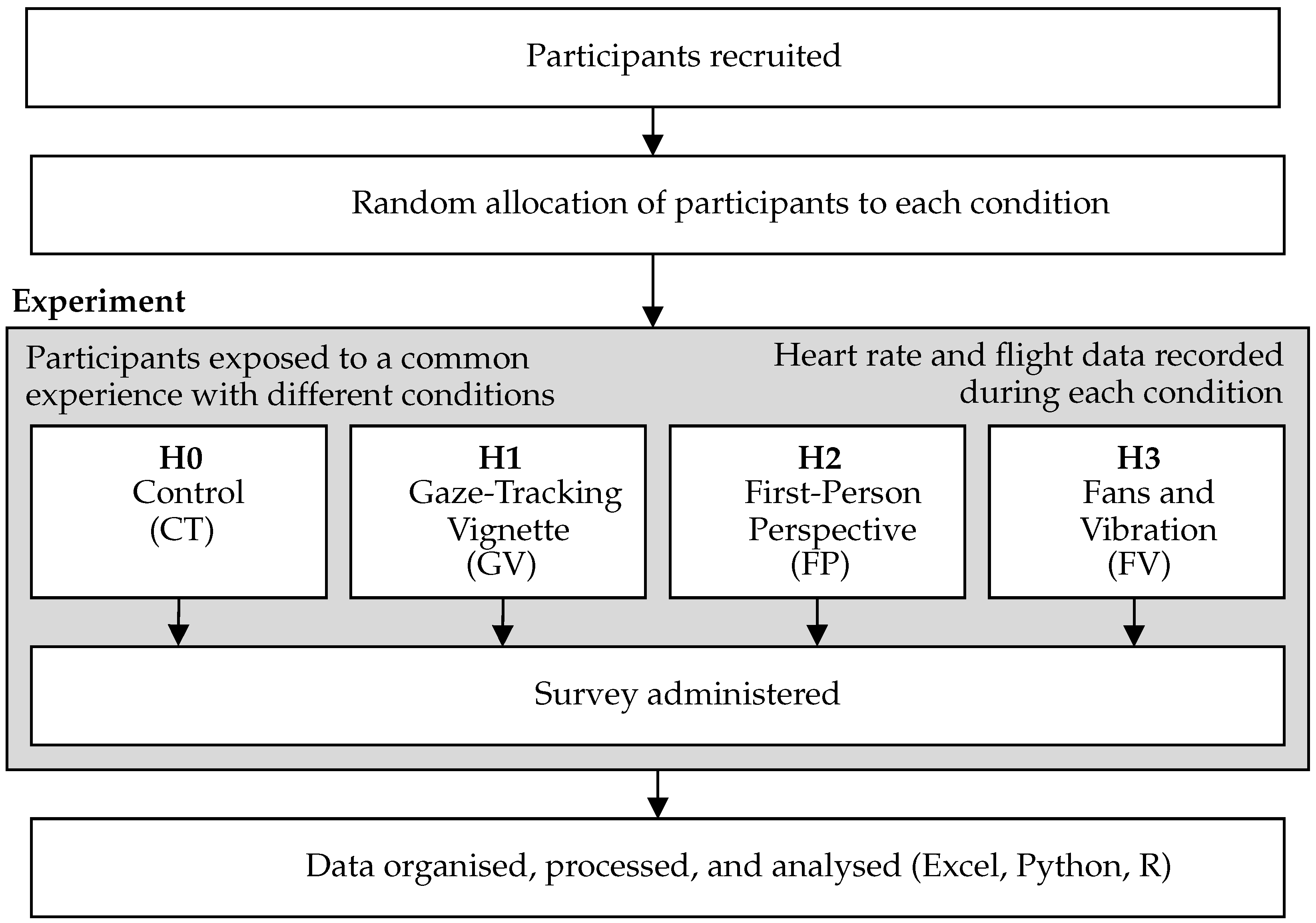
3.6. Experiment Design
3.6.1. Conditions
3.6.2. User Interface
3.6.3. Data Collection
3.6.4. Data Processing
3.6.5. Data Analysis
3.7. Equipment and Software
3.7.1. Computer Hardware
- Processor: Intel Core i7-8700 (3.20–4.20 GHz)
- Baseboard: Gigabyte Technology B360 Aorus
- Physical memory: RAM
- Graphics card: NVIDIA GeForce RTX 2080
- SSD (OS and Programs)
- HDD (Unity Application and Data)
3.7.2. Safety
3.7.3. Application Development
3.8. Participants
3.9. Experimental Procedure
4. Results
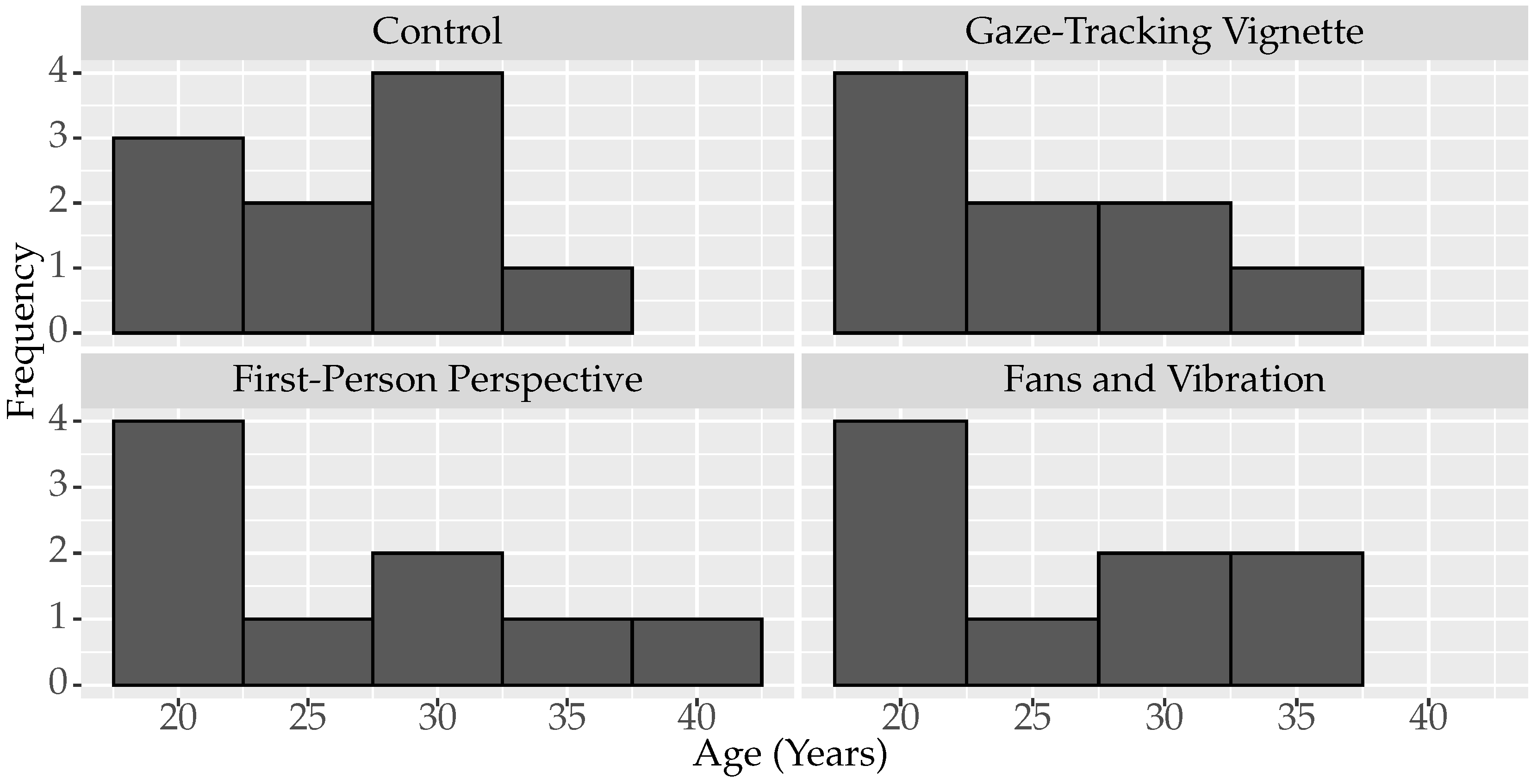
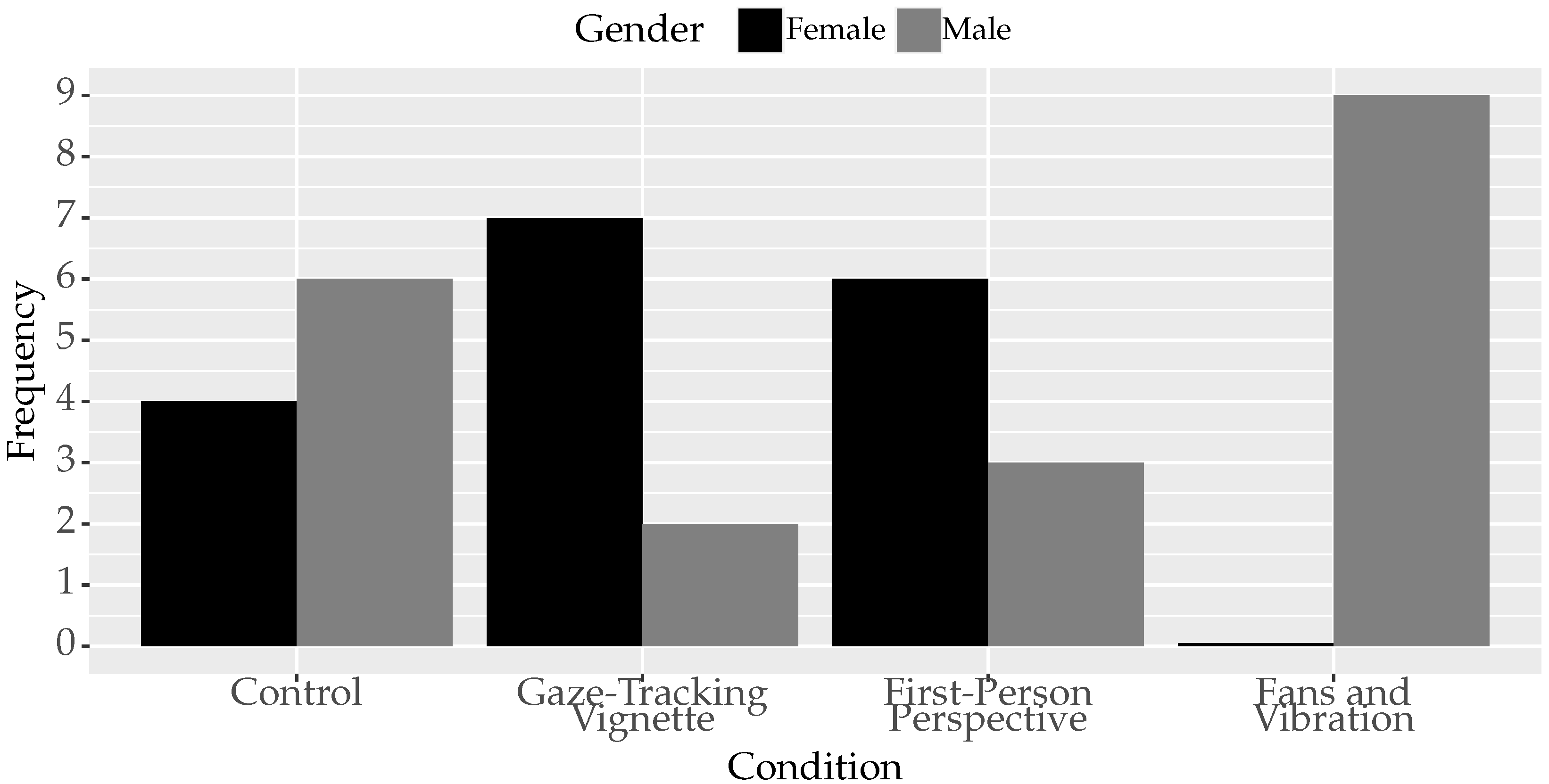
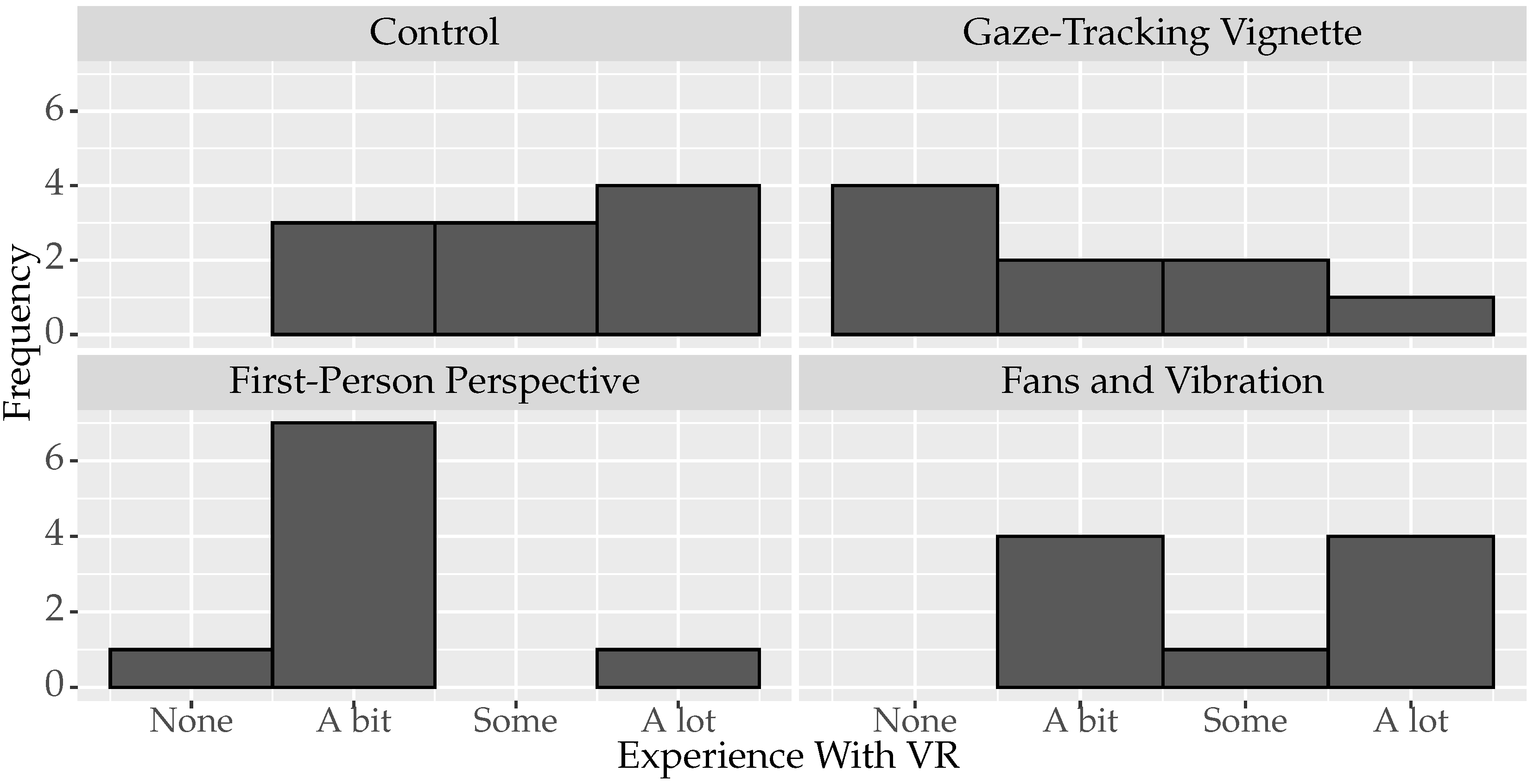
4.1. Participant Information
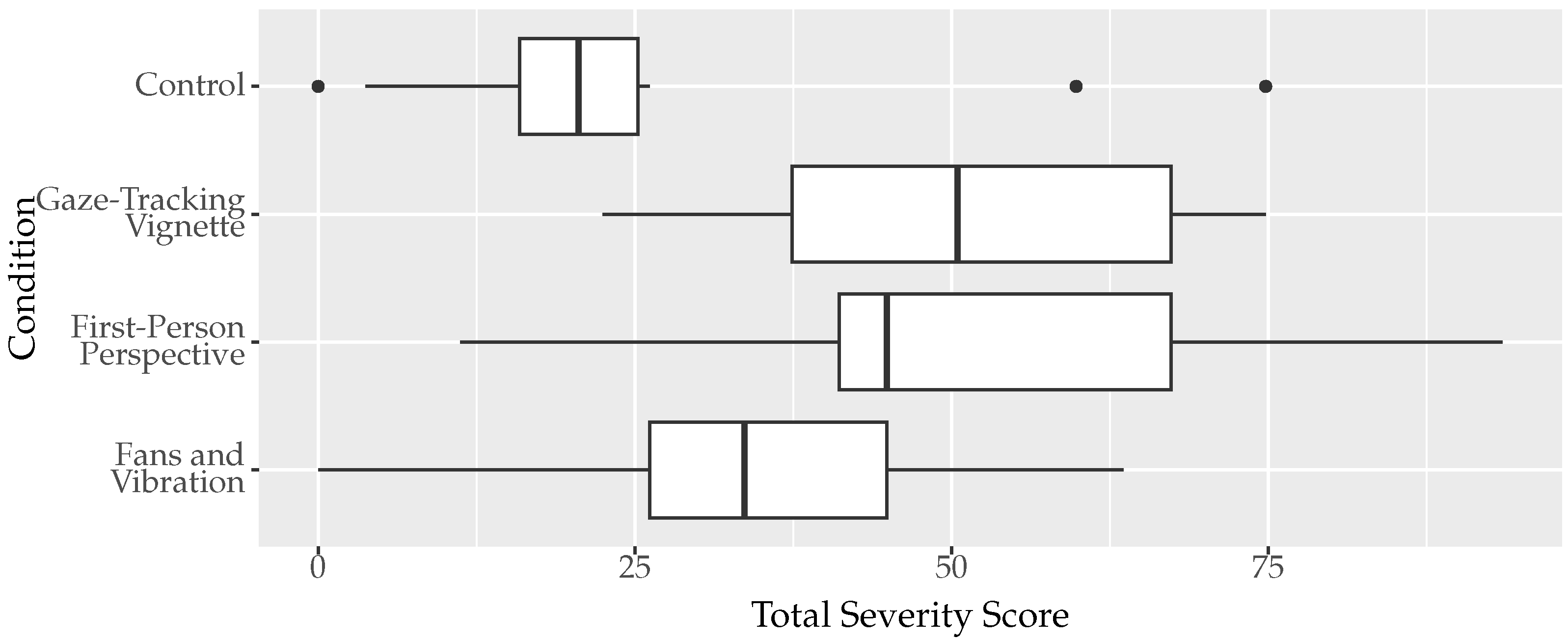
4.2. Simulator Sickness Questionnaire
4.2.1. Analysis of Variance
4.2.2. Post-Hoc Analysis
4.2.3. Effect Size
4.2.4. Correlations with Participant Information
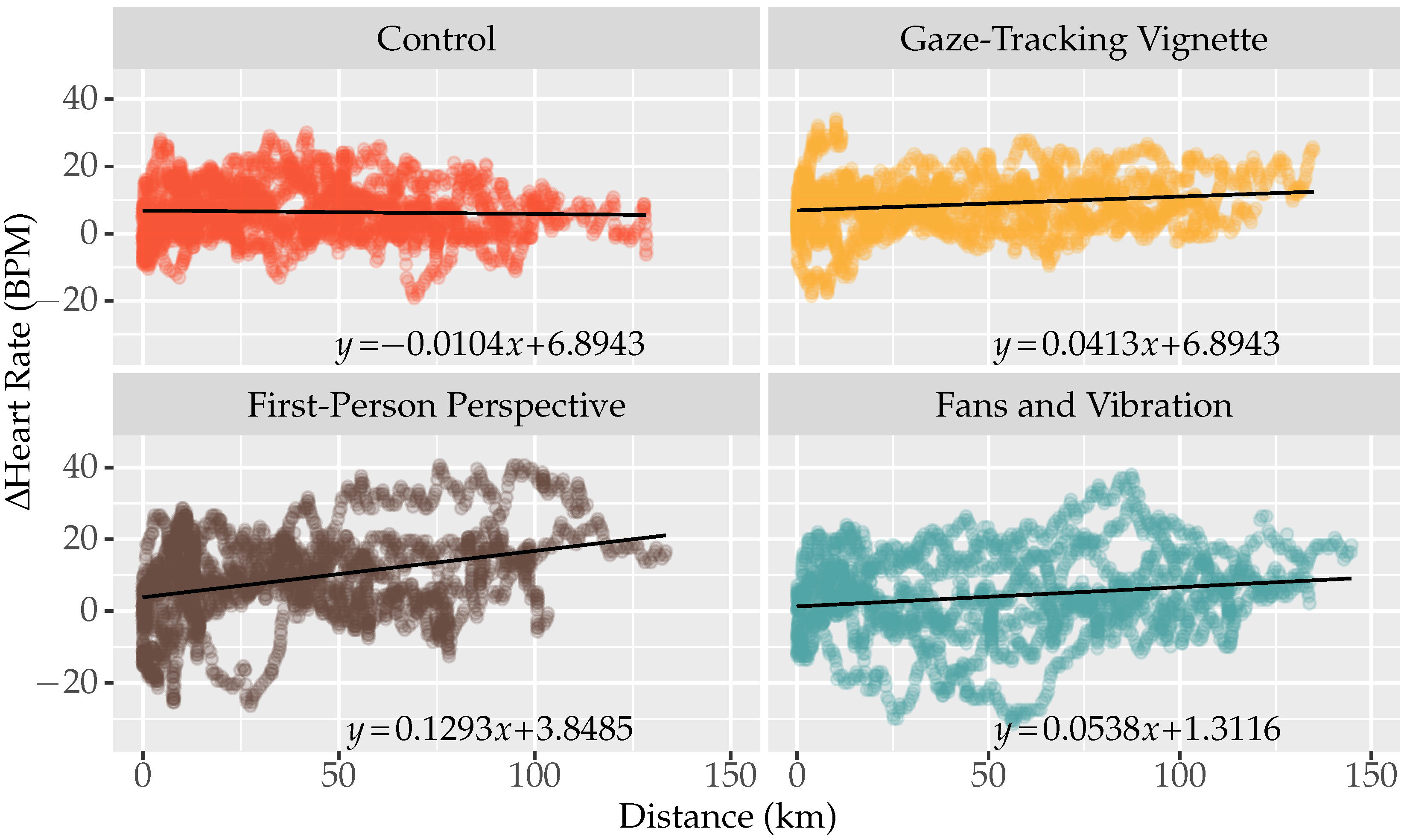
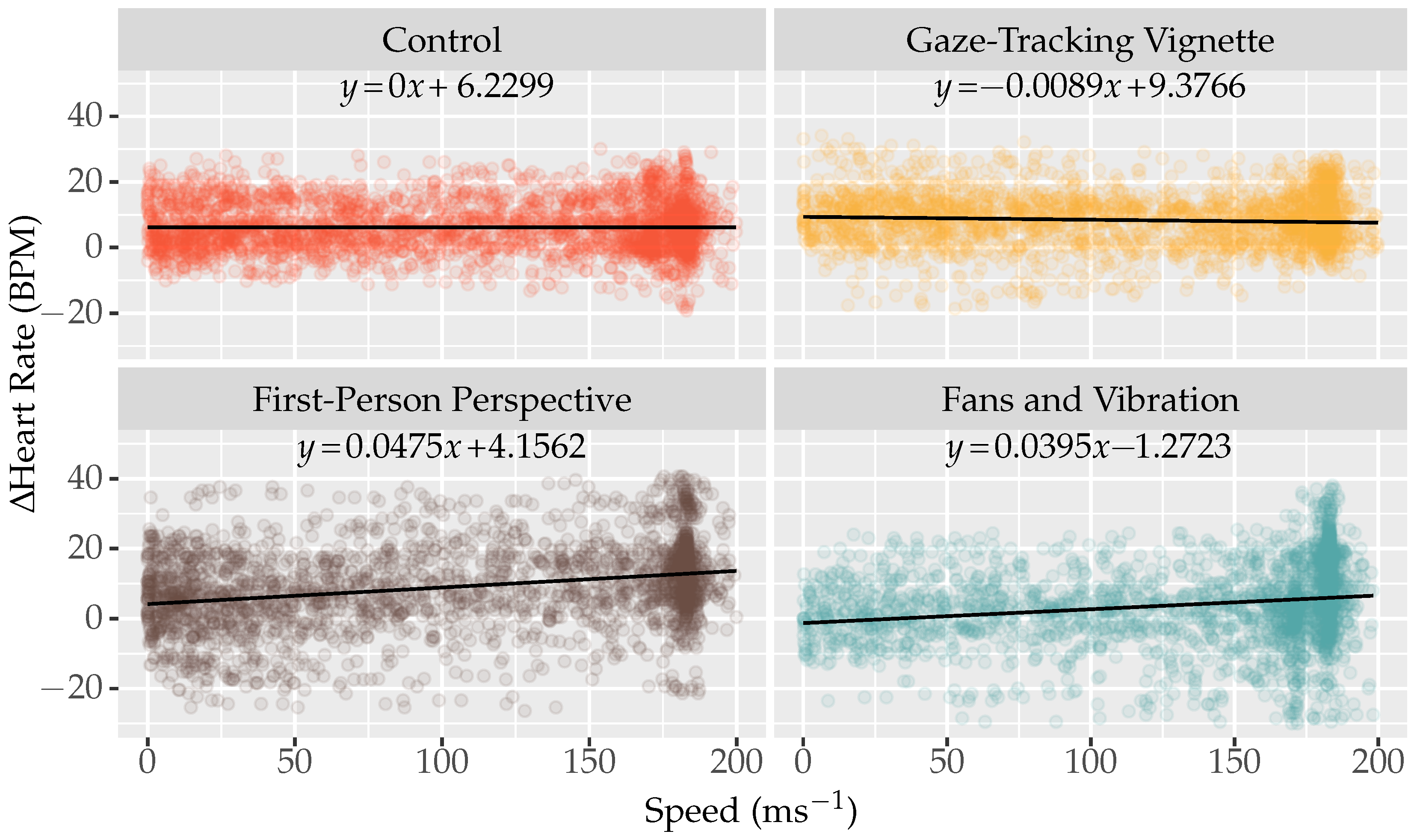
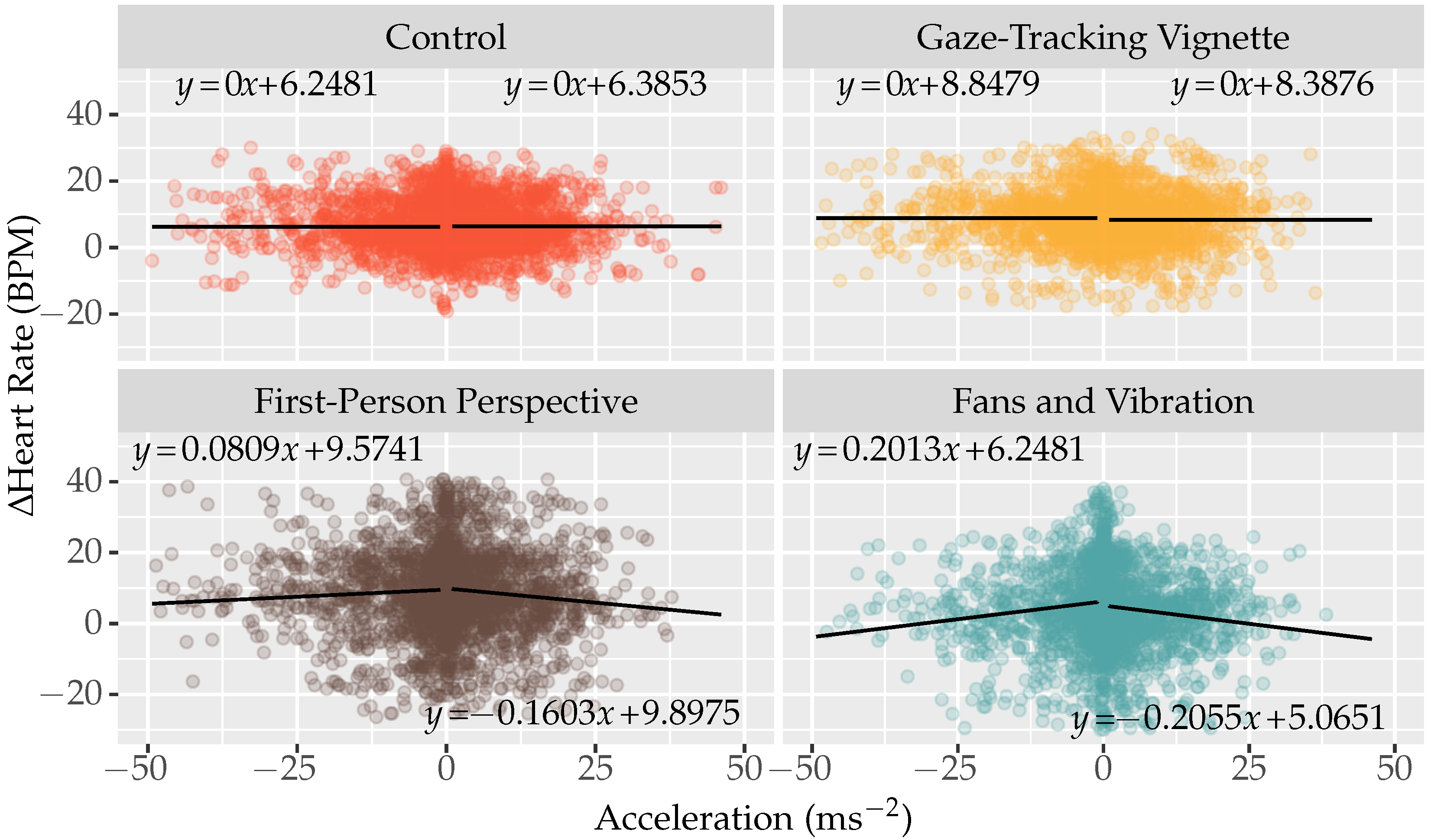
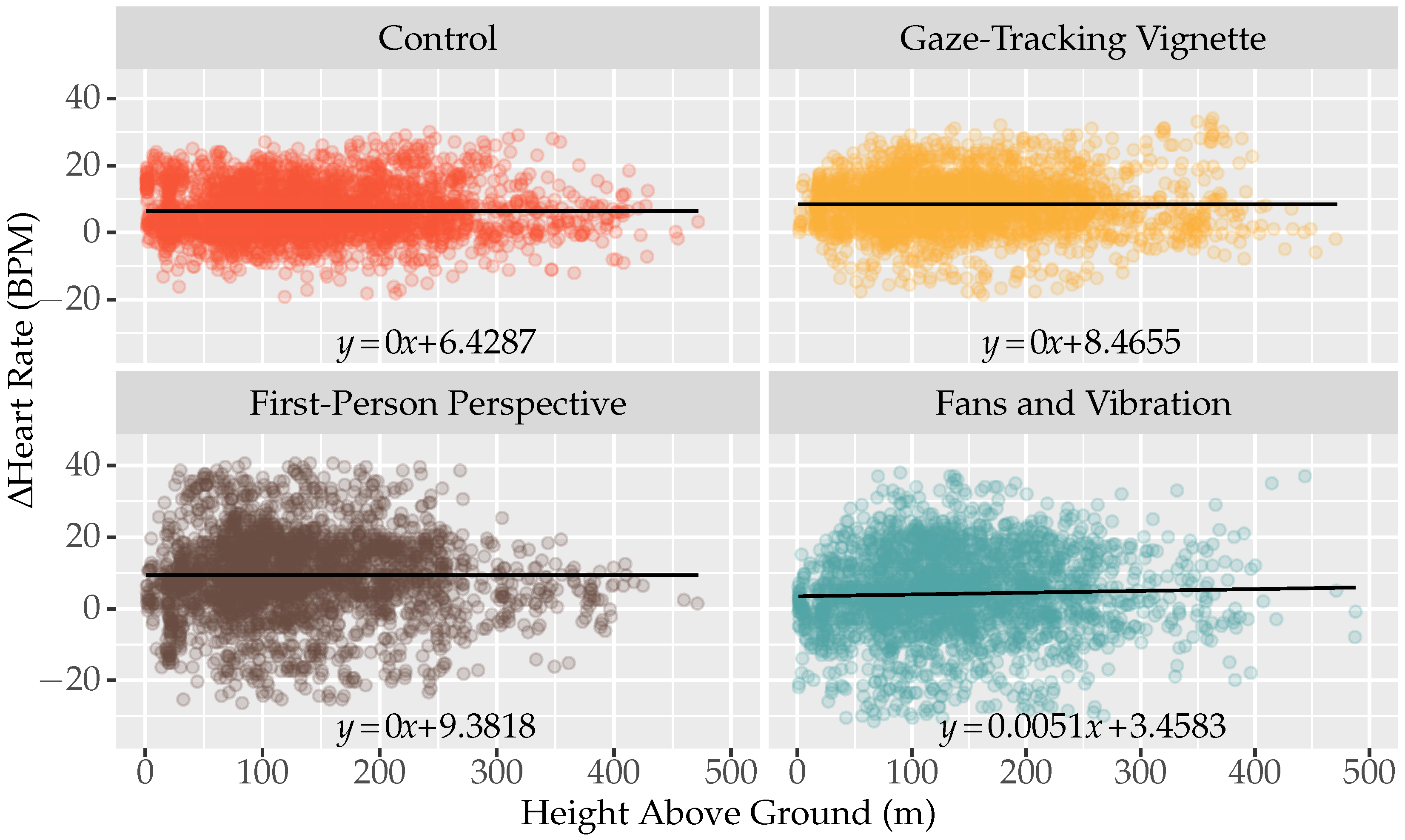
4.3. Physiological Responses
4.4. Observations and Comments
5. Discussion
5.1. The Experience
5.2. Conditions
5.2.1. Control
5.2.2. Gaze-Tracking Vignette
5.2.3. First-Person Perspective
5.2.4. Fans and Vibration
5.3. Experiment Limitations
5.3.1. Systematic Errors
5.3.2. Random Errors
5.4. Significance of Findings
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stanney, K.; Lawson, B.D.; Rokers, B.; Dennison, M.; Fidopiastis, C.; Stoffregen, T.; Weech, S.; Fulvio, J.M. Identifying Causes of and Solutions for Cybersickness in Immersive Technology: Reformulation of a Research and Development Agenda. Int. J. Hum.-Comput. Interact. 2020, 36, 1783–1803. [Google Scholar] [CrossRef]
- LaViola, J.J. A Discussion of Cybersickness in Virtual Environments. SIGCHI Bull. 2000, 32, 47–56. [Google Scholar] [CrossRef]
- Kennedy, R.S.; Stanney, K.M.; Dunlap, W.P. Duration and Exposure to Virtual Environments: Sickness Curves During and Across Sessions. Presence Teleoper. Virtual Environ. 2000, 9, 463–472. [Google Scholar] [CrossRef]
- Chen, S.; Weng, D. The temporal pattern of VR sickness during 7.5-h virtual immersion. Virtual Real. 2022, 26, 817–822. [Google Scholar] [CrossRef]
- Kourtesis, P.; Collina, S.; Doumas, L.A.A.; MacPherson, S.E. Validation of the Virtual Reality Neuroscience Questionnaire: Maximum Duration of Immersive Virtual Reality Sessions Without the Presence of Pertinent Adverse Symptomatology. Front. Hum. Neurosci. 2019, 13, 417. [Google Scholar] [CrossRef]
- Stanney, K.M.; Hale, K.S.; Nahmens, I.; Kennedy, R.S. What to Expect from Immersive Virtual Environment Exposure: Influences of Gender, Body Mass Index, and Past Experience. Hum. Factors 2003, 45, 504–520. [Google Scholar] [CrossRef]
- Caserman, P.; Garcia-Agundez, A.; Gámez Zerban, A.; Göbel, S. Cybersickness in current-generation virtual reality head-mounted displays: Systematic review and outlook. Virtual Real. 2021, 25, 1153–1170. [Google Scholar] [CrossRef]
- Howard, M.C.; Van Zandt, E.C. A meta-analysis of the virtual reality problem: Unequal effects of virtual reality sickness across individual differences. Virtual Real. 2021, 25, 1221–1246. [Google Scholar] [CrossRef]
- Tian, N.; Lopes, P.; Boulic, R. A review of cybersickness in head-mounted displays: Raising attention to individual susceptibility. Virtual Real. 2022, 26, 1409–1441. [Google Scholar] [CrossRef]
- Dużmańska, N.; Strojny, P.; Strojny, A. Can Simulator Sickness Be Avoided? A Review on Temporal Aspects of Simulator Sickness. Front. Psychol. 2018, 9, 2132. [Google Scholar] [CrossRef]
- Lopes, P.; Tian, N.; Boulic, R. Eye Thought You Were Sick! Exploring Eye Behaviors for Cybersickness Detection in VR. In Proceedings of the Motion, Interaction and Games, Charleston, SC, USA, 16–18 October 2020; pp. 1–10. [Google Scholar] [CrossRef]
- Fernandes, A.S.; Feiner, S.K. Combating VR sickness through subtle dynamic field-of-view modification. In Proceedings of the IEEE 3DUI 2016, Greenville, SC, USA, 19–20 March 2016; pp. 201–210. [Google Scholar] [CrossRef]
- Chang, E.; Kim, H.T.; Yoo, B. Virtual Reality Sickness: A Review of Causes and Measurements. Int. J. Hum.-Comput. Interact. 2020, 36, 1658–1682. [Google Scholar] [CrossRef]
- Souchet, A.D.; Lourdeaux, D.; Pagani, A.; Rebenitsch, L. A narrative review of immersive virtual reality’s ergonomics and risks at the workplace: Cybersickness, visual fatigue, muscular fatigue, acute stress, and mental overload. Virtual Real. 2023, 27, 19–50. [Google Scholar] [CrossRef]
- Keshavarz, B.; Hecht, H. Validating an Efficient Method to Quantify Motion Sickness. Hum. Factors 2011, 53, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Norouzi, N.; Bruder, G.; Welch, G. Assessing Vignetting as a Means to Reduce VR Sickness During Amplified Head Rotations. In Proceedings of the SAP 2018, 15th ACM Symposium on Applied Perception, New York, NY, USA, 10–11 August 2018; pp. 1–8. [Google Scholar] [CrossRef]
- Budhiraja, P.; Miller, M.R.; Modi, A.K.; Forsyth, D. Rotation Blurring: Use of Artificial Blurring to Reduce Cybersickness in Virtual Reality First Person Shooters. arXiv 2017, arXiv:1710.02599. [Google Scholar]
- Hussain, R.; Chessa, M.; Solari, F. Mitigating Cybersickness in Virtual Reality Systems through Foveated Depth-of-Field Blur. Sensors 2021, 21, 4006. [Google Scholar] [CrossRef]
- Debarba, H.G.; Perrin, S.; Herbelin, B.; Boulic, R. Embodied Interaction using Non-Planar Projections in Immersive Virtual Reality. In Proceedings of the VRST 2015, Beijing, China, 13–15 November 2015; pp. 125–128. [Google Scholar] [CrossRef]
- Riccio, G.E.; Stoffregen, T.A. An ecological Theory of Motion Sickness and Postural Instability. Ecol. Psychol. 1991, 3, 195–240. [Google Scholar] [CrossRef]
- Jung, S.; Li, R.; McKee, R.; Whitton, M.C.; Lindeman, R.W. Floor-vibration VR: Mitigating Cybersickness Using Whole-body Tactile Stimuli in Highly Realistic Vehicle Driving Experiences. IEEE Trans. Vis. Comput. Graph. 2021, 27, 2669–2680. [Google Scholar] [CrossRef]
- Oman, C.M. Motion sickness: A synthesis and evaluation of the sensory conflict theory. Can. J. Physiol. Pharmacol. 1990, 68, 294–303. [Google Scholar] [CrossRef]
- Chardonnet, J.R.; Mirzaei, M.A.; Mérienne, F. Features of the Postural Sway Signal as Indicators to Estimate and Predict Visually Induced Motion Sickness in Virtual Reality. Int. J. Hum.-Comput. Interact. 2017, 33, 771–785. [Google Scholar] [CrossRef]
- Merhi, O.; Faugloire, E.; Flanagan, M.; Stoffregen, T.A. Motion Sickness, Console Video Games, and Head-Mounted Displays. Hum. Factors 2007, 49, 920–934. [Google Scholar] [CrossRef]
- Zielasko, D.; Riecke, B.E. To Sit or Not to Sit in VR: Analyzing Influences and (Dis)Advantages of Posture and Embodied Interaction. Computers 2021, 10, 73. [Google Scholar] [CrossRef]
- Zielasko, D. Subject 001—A Detailed Self-Report of Virtual Reality Induced Sickness. In Proceedings of the IEEE Conference on Virtual Reality and 3D User Interfaces Abstracts and Workshops (VRW), Lisbon, Portugal, 27 March–3 April 2021; pp. 165–168. [Google Scholar] [CrossRef]
- Dennison, M.S.; D’Zmura, M. Cybersickness without the wobble: Experimental results speak against postural instability theory. Appl. Ergon. 2017, 58, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.J.W.; Duh, H.B.L.; Parker, D.E.; Abi-Rached, H.; Furness, T.A. Effects of field of view on presence, enjoyment, memory, and simulator sickness in a virtual environment. In Proceedings of the IEEE Virtual Reality Conference 2002, Orlando, FL, USA, 24–28 March 2002; pp. 164–171. [Google Scholar] [CrossRef]
- Kolasinski, E.M. Simulator Sickness in Virtual Environments; US Army Research Institute for the Behavioral and Social Sciences: Alexandria, VA, USA, 1995; Volume 1027. [Google Scholar]
- Davis, S.; Nesbitt, K.; Nalivaiko, E. A Systematic Review of Cybersickness. In Proceedings of the 2014 Conference on Interactive Entertainment, Newcastle, Australia, 2–3 December 2014; pp. 1–9. [Google Scholar] [CrossRef]
- Davis, S.; Nesbitt, K.; Nalivaiko, E. Comparing the onset of cybersickness using the Oculus Rift and two virtual roller coasters. In Proceedings of the 11th Australasian Conference on Interactive Entertainment, Sydney, Austrailia, 27–30 January 2015; Volume 167. [Google Scholar]
- So, R.H.Y.; Lo, W.T.; Ho, A.T.K. Effects of Navigation Speed on Motion Sickness Caused by an Immersive Virtual Environment. Hum. Factors 2001, 43, 452–461. [Google Scholar] [CrossRef]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator Sickness Questionnaire: An Enhanced Method for Quantifying Simulator Sickness. Int. J. Aviat. Psychol. 1993, 3, 203–220. [Google Scholar] [CrossRef]
- Kim, Y.Y.; Kim, H.J.; Kim, E.N.; Ko, H.D.; Kim, H.T. Characteristic changes in the physiological components of cybersickness. Psychophysiology 2005, 42, 616–625. [Google Scholar] [CrossRef] [PubMed]
- Nesbitt, K.; Davis, S.; Blackmore, K.; Nalivaiko, E. Correlating reaction time and nausea measures with traditional measures of cybersickness. Displays 2017, 48, 1–8. [Google Scholar] [CrossRef]
- Nalivaiko, E.; Davis, S.L.; Blackmore, K.L.; Vakulin, A.; Nesbitt, K.V. Cybersickness provoked by head-mounted display affects cutaneous vascular tone, heart rate and reaction time. Physiol. Behav. 2015, 151, 583–590. [Google Scholar] [CrossRef]
- Castaneda, D.; Esparza, A.; Ghamari, M.; Soltanpur, C.; Nazeran, H. A review on wearable photoplethysmography sensors and their potential future applications in health care. Int. J. Biosens. Bioelectron. 2018, 4, 195–202. [Google Scholar] [CrossRef]
- Paradiso, C.; Colino, F.; Liu, S. The Validity and Reliability of the Mi Band Wearable Device for Measuring Steps and Heart Rate. Int. J. Exerc. Sci. 2020, 13, 689–701. [Google Scholar]
- Bent, B.; Goldstein, B.A.; Kibbe, W.A.; Dunn, J.P. Investigating sources of inaccuracy in wearable optical heart rate sensors. Npj Digit. Med. 2020, 3, 18. [Google Scholar] [CrossRef]
- Beckhaus, S.; Blom, K.J.; Haringer, M. Intuitive, Hands-free Travel Interfaces for Virtual Environments. In Proceedings of the New Directions in 3D User Interfaces Workshop of IEEE VR, Bonn, Germany, 12 March 2005; Volume 1. [Google Scholar]
- Jung, S.; Karki, N.; Slutter, M.; Lindeman, R.W. On the Use of Multi-sensory Cues in Symmetric and Asymmetric Shared Collaborative Virtual Spaces. Proc. ACM Hum.-Comput. Interact. 2021, 5, 72:1–72:25. [Google Scholar] [CrossRef]
- Knowles, I.; Renka, R.J. Methods for Numerical Differentiation of Noisy Data. Electron. J. Differ. Equ. 2014, 21, 235–246. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Kang, H. Sample size determination and power analysis using the G*Power software. J. Educ. Eval. Health Prof. 2021, 18, 17. [Google Scholar] [CrossRef]
- Hildebrandt, J.; Schmitz, P.; Calero Valdez, A.; Kobbelt, L.; Ziefle, M. Get Well Soon! Human Factors’ Influence on Cybersickness After Redirected Walking Exposure in Virtual Reality. In Proceedings of the Virtual, Augmented and Mixed Reality: Interaction Navigation, Visualization, Embodiment, and Simulation, Las Vegas, NV, USA, 15–20 July 2018; Lecture Notes in Computer Science. Chen, J.Y., Fragomeni, G., Eds.; Springer: Cham, Switzerland, 2018; pp. 82–101. [Google Scholar] [CrossRef]
- Wang, G.; Suh, A. User adaptation to cybersickness in virtual reality: A qualitative study. In Proceedings of the 27th European Conference on Information Systems (ECIS), Stockholm and Uppsala, Stockholm, Sweden, 8–14 June 2019; Association for Information Systems (AIS): Atlanta, GA, USA, 2019. [Google Scholar]
- Nickel, P.; Nachreiner, F. Sensitivity and Diagnosticity of the 0.1-Hz Component of Heart Rate Variability as an Indicator of Mental Workload. Hum. Factors 2003, 45, 575–590. [Google Scholar] [CrossRef]
- Hjortskov, N.; Rissén, D.; Blangsted, A.K.; Fallentin, N.; Lundberg, U.; Søgaard, K. The effect of mental stress on heart rate variability and blood pressure during computer work. Eur. J. Appl. Physiol. 2004, 92, 84–89. [Google Scholar] [CrossRef]
- Sepich, N.C.; Jasper, A.; Fieffer, S.; Gilbert, S.B.; Dorneich, M.C.; Kelly, J.W. The impact of task workload on cybersickness. Front. Virtual Real. 2022, 3, 943409. [Google Scholar] [CrossRef]
- Venkatakrishnan, R.; Venkatakrishnan, R.; Anaraky, R.G.; Volonte, M.; Knijnenburg, B.; Babu, S.V. A Structural Equation Modeling Approach to Understand the Relationship between Control, Cybersickness and Presence in Virtual Reality. In Proceedings of the 2020 IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Atlanta, GA, USA, 22–26 March 2020; pp. 682–691. [Google Scholar] [CrossRef]
- Stanney, K.M.; Kennedy, R.S.; Drexler, J.M. Cybersickness is Not Simulator Sickness. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 1997, 41, 1138–1142. [Google Scholar] [CrossRef]






















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SSQ Component | Condition | Shapiro–Wilk Test (p-Value) | Levene’s Test (p-Value) |
|---|---|---|---|
| Nausea | CT | 0.4800 | 0.4267 |
| GV | 0.4340 | ||
| FP | 0.3190 | ||
| FV | 0.0952 | ||
| Oculomotor | CT | 0.4490 | 0.6372 |
| GV | 0.6690 | ||
| FP | 0.5190 | ||
| FV | 0.0055 | ||
| Disorientation | CT | 0.0715 | 0.8030 |
| GV | 0.1650 | ||
| FP | 0.9270 | ||
| FV | 0.6430 | ||
| Total Severity | CT | 0.3580 | 0.9311 |
| GV | 0.3040 | ||
| FP | 0.8210 | ||
| FV | 0.2700 |
| SSQ Component | Critical Value | F Ratio | p-Value |
|---|---|---|---|
| Nausea | 2.2635 | 2.1270 | 0.1160 |
| Oculomotor | 2.2635 | 2.7050 | 0.0618 |
| Disorientation | 2.2635 | 2.8060 | 0.0554 |
| Total Severity | 2.2635 | 2.9360 | 0.0481 |
| SSQ Component | Control vs. | Confidence Interval | p-Value |
|---|---|---|---|
| Nausea | GV | [−0.6021, 4.4067] | 0.2633 |
| FP | [0.3175, 5.1692] | 0.0548 | |
| FV | [−1.2835, 3.5682] | 0.6290 | |
| Oculomotor | GV | [0.2592, 3.9262] | 0.0519 |
| FP | [−0.0337, 3.5183] | 0.1086 | |
| FV | [−1.2178, 2.3342] | 0.8443 | |
| Disorientation | GV | [0.4569, 6.8004] | 0.0512 |
| FP | [0.3116, 6.4562] | 0.0630 | |
| FV | [−1.6417, 4.5030] | 0.6367 | |
| Total Severity | GV | [0.2161, 4.5678] | 0.0634 |
| FP | [0.3585, 4.5737] | 0.0454 | |
| FV | [−1.2244, 2.9908] | 0.7045 |
| Variables | Correlation Coefficient | p-Value |
|---|---|---|
| Gender vs. Total Severity | −0.0905 | 0.5997 |
| Age vs. Total Severity | −0.3649 | 0.0287 |
| VR Experience vs. Total Severity | −0.3284 | 0.0505 |
| Statistic | Condition | Baseline (Before) | Shift (1st Half) | Shift (2nd Half) |
|---|---|---|---|---|
| Min | CT | 57.0000 | −13.1774 | −19.1774 |
| GV | 63.0000 | −18.6204 | −9.6204 | |
| FP | 68.0000 | −26.3684 | −13.1905 | |
| FV | 63.0000 | −29.9462 | −31.4857 | |
| Max | CT | 118.0000 | 30.0735 | 29.0678 |
| GV | 132.0000 | 34.1279 | 29.1279 | |
| FP | 126.0000 | 31.6316 | 40.6316 | |
| FV | 121.0000 | 26.4107 | 38.0385 | |
| Mean | CT | 85.0573 | 6.6017 | 6.3168 |
| GV | 90.9169 | 8.1231 | 9.2679 | |
| FP | 93.7892 | 6.6104 | 11.8681 | |
| FV | 85.0971 | 3.9319 | 4.5709 | |
| SD | CT | 12.1265 | 7.6874 | 7.6331 |
| GV | 14.5803 | 9.1782 | 6.6824 | |
| FP | 11.1942 | 11.5703 | 11.7055 | |
| FV | 11.8774 | 10.7184 | 12.8420 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Page, D.; Lindeman, R.W.; Lukosch, S. Identifying Strategies to Mitigate Cybersickness in Virtual Reality Induced by Flying with an Interactive Travel Interface. Multimodal Technol. Interact. 2023, 7, 47. https://doi.org/10.3390/mti7050047
Page D, Lindeman RW, Lukosch S. Identifying Strategies to Mitigate Cybersickness in Virtual Reality Induced by Flying with an Interactive Travel Interface. Multimodal Technologies and Interaction. 2023; 7(5):47. https://doi.org/10.3390/mti7050047
Chicago/Turabian StylePage, Daniel, Robert W. Lindeman, and Stephan Lukosch. 2023. "Identifying Strategies to Mitigate Cybersickness in Virtual Reality Induced by Flying with an Interactive Travel Interface" Multimodal Technologies and Interaction 7, no. 5: 47. https://doi.org/10.3390/mti7050047