Refractive Effect of Epithelial Remodelling in Myopia after Transepithelial Photorefractive Keratectomy


Abstract
:1. Introduction
2. Materials and Methods
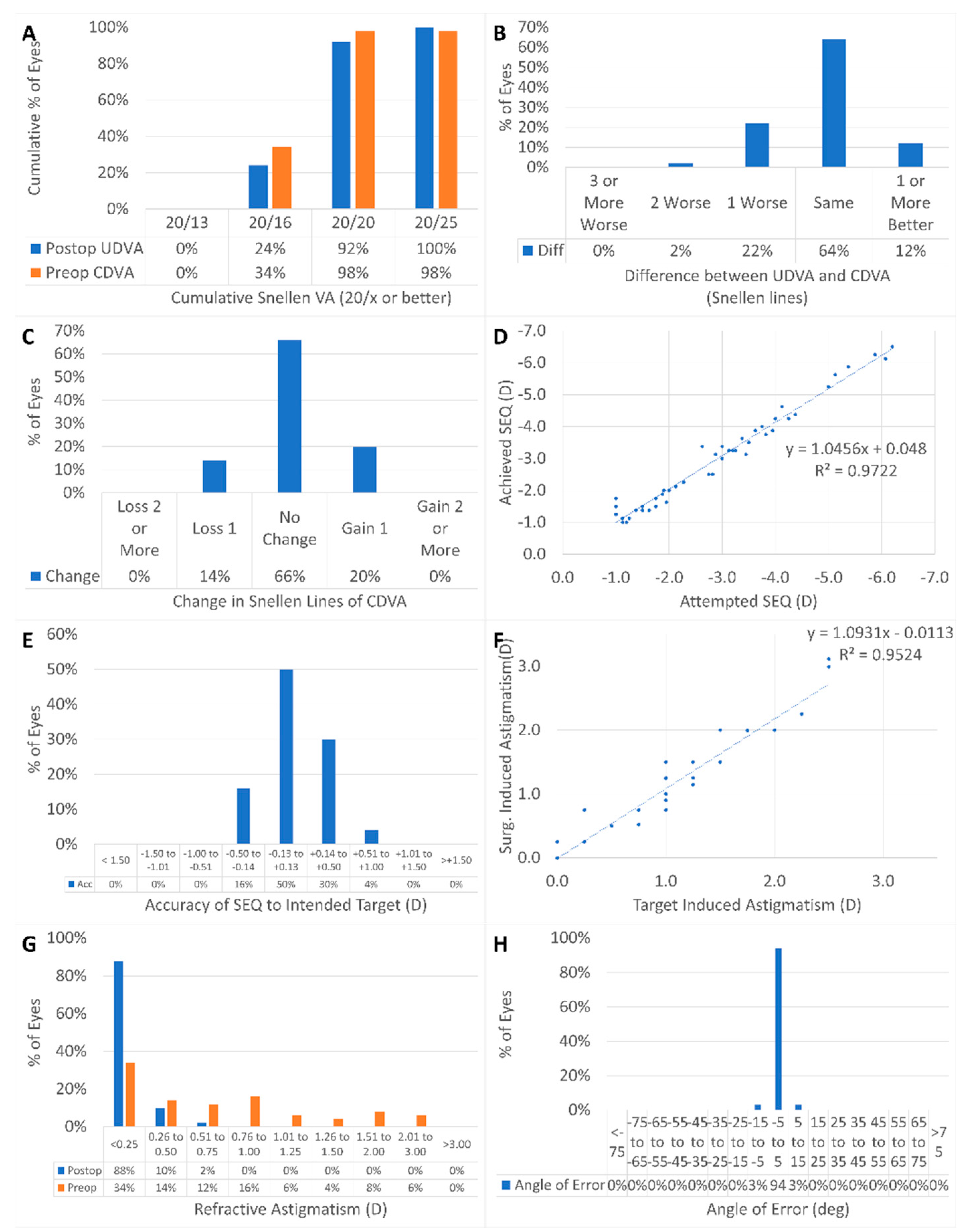
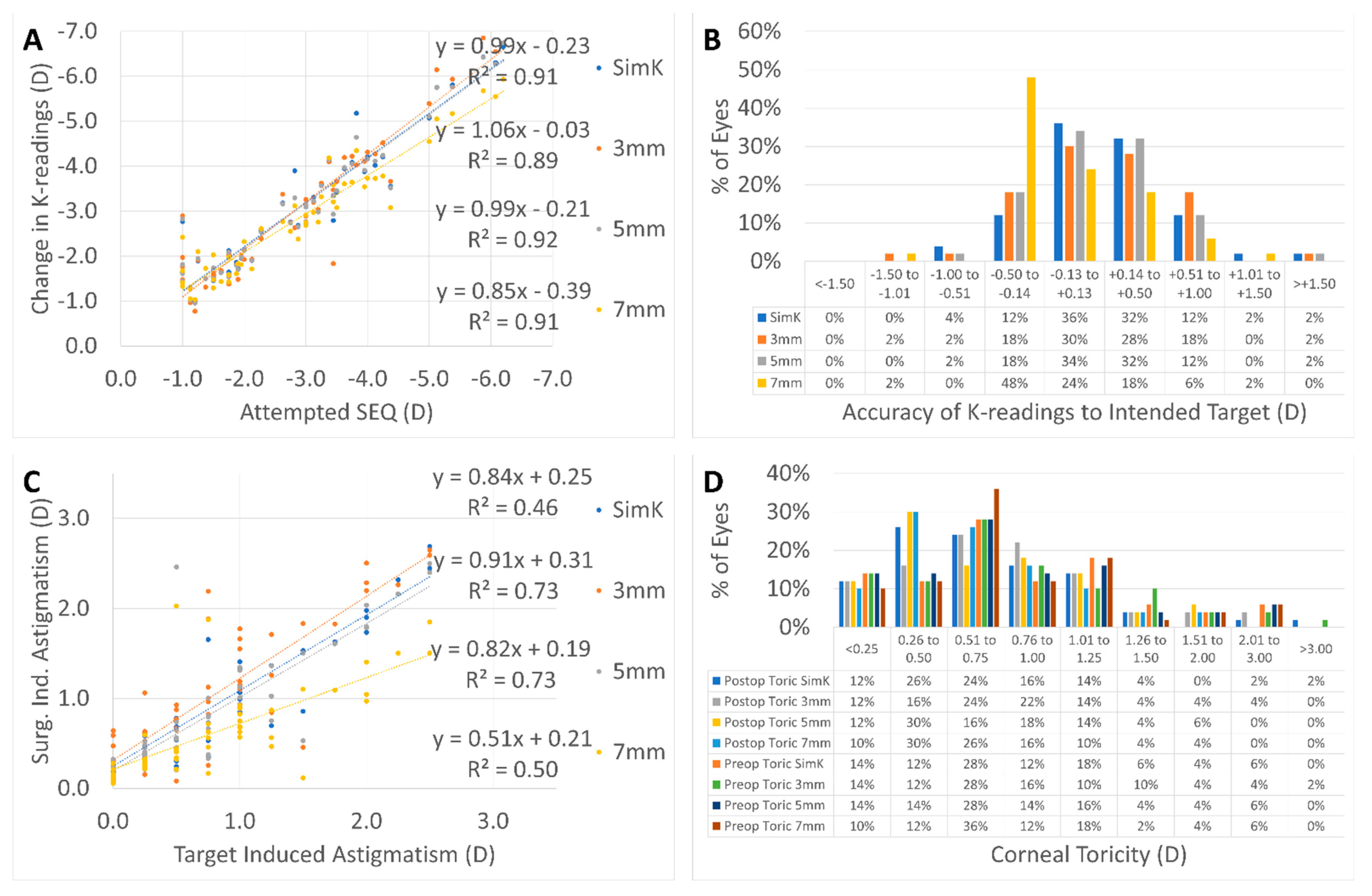
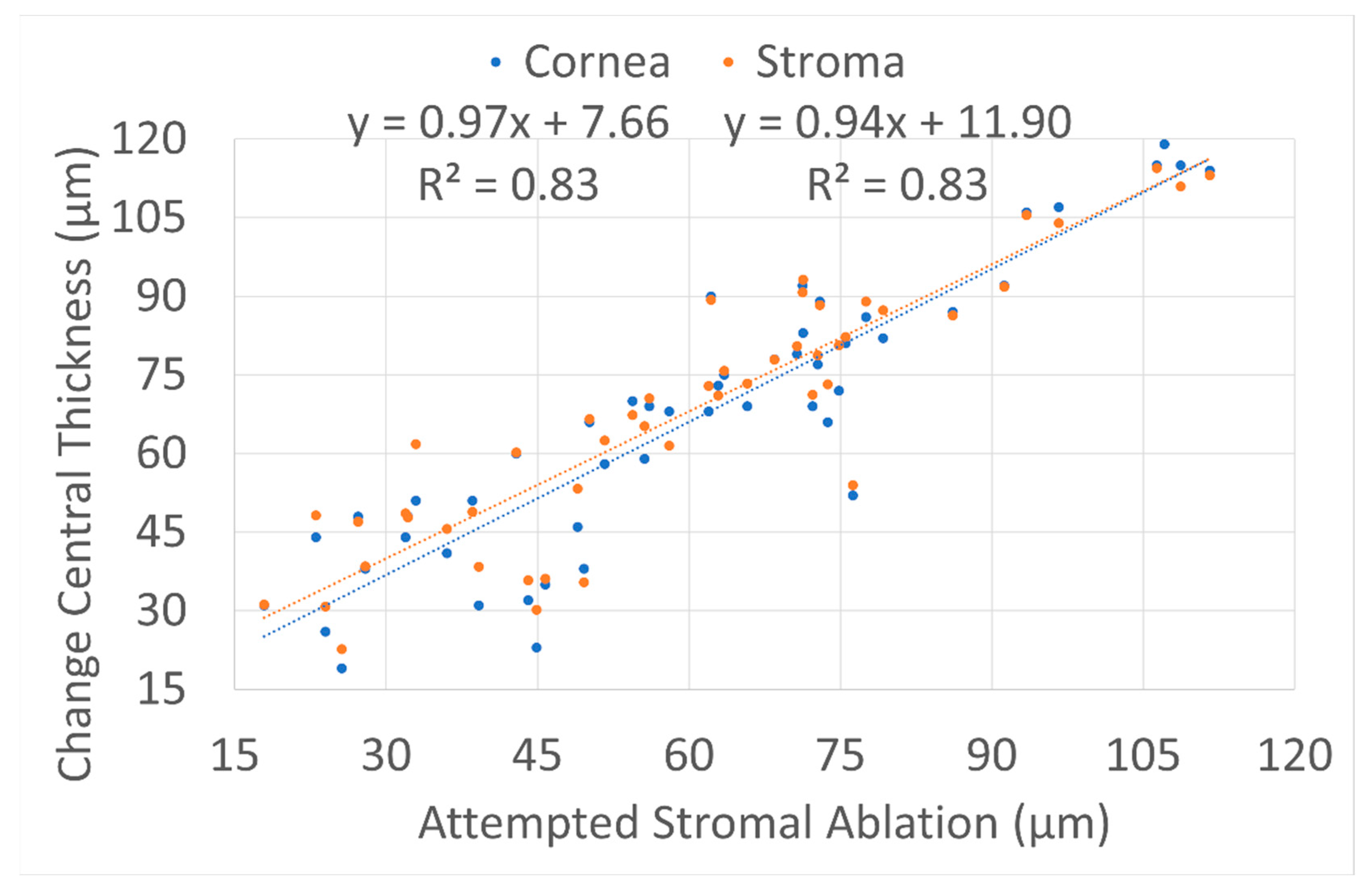
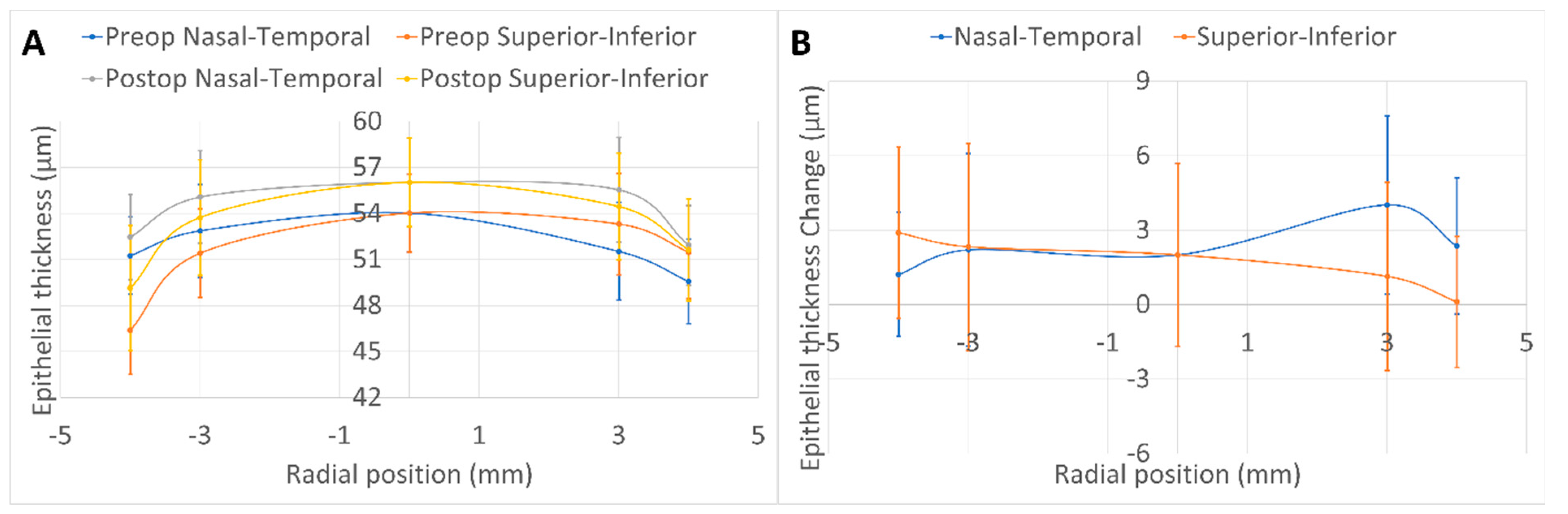
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marshall, J.; Trokel, S.; Rothery, S.; Krueger, R.R. A Comparative Study of Corneal Incisions Induced by Diamond and Steel Knives and Two Ultraviolet Radiations from an Excimer Laser. Br. J. Ophthalmol. 1986, 70, 482–501. [Google Scholar] [CrossRef] [PubMed]
- Munnerlyn, C.R.; Koons, S.J.; Marshall, J. Photorefractive Keratectomy: A Technique for Laser Refractive Surgery. J. Cataract Refract. Surg. 1988, 14, 46–52. [Google Scholar] [CrossRef]
- Buratto, L.; Ferrari, M. Excimer Laser Intrastromal Keratomileusis: Case Reports. J. Cataract Refract. Surg. 1992, 18, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.; Shah, S.; Sengupta, S. Results of Small Incision Lenticule Extraction: All-in-One Femtosecond Laser Refractive Surgery. J. Cataract Refract. Surg. 2011, 37, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Ficker, L.A.; Bates, A.K.; Steele, A.D.M.; Lyons, C.J.; Milliken, A.B.; Astin, C.; Slattery, K.; Kirkness, C.M. Excimer Laser Photorefractive Keratectomy for Myopia: 12 Month Follow-Up. Eye 1993, 7, 617–624. [Google Scholar] [CrossRef] [PubMed]
- Dausch, D.; Klein, R.; Schröder, E.; Dausch, B. Excimer Laser Photorefractive Keratectomy with Tapered Transition Zone for High Myopia: A Preliminary Report of Six Cases. J. Cataract Refract. Surg. 1993, 19, 590–594. [Google Scholar] [CrossRef]
- Seiler, T.; Holschbach, A.; Derse, M.; Jean, B.; Genth, U. Complications of Myopic Photorefractive Keratectomy with the Excimer Laser. Ophthalmology 1994, 101, 153–160. [Google Scholar] [CrossRef]
- Lohmann, C.P.; Guell, J.L. Regression After LASIK for the Treatment of Myopia: The Role of the Corneal Epithelium. Semin. Ophthalmol. 1998, 13, 79–82. [Google Scholar] [CrossRef]
- Reinstein, D.Z.; Archer, T.J.; Gobbe, M. Rate of Change of Curvature of the Corneal Stromal Surface Drives Epithelial Compensatory Changes and Remodeling. J. Refract. Surg. 2014, 30, 800–802. [Google Scholar] [CrossRef] [Green Version]
- Sedaghat, M.-R.; Momeni-Moghaddam, H.; Gazanchian, M.; Reinstein, D.Z.; Archer, T.J.; Randleman, J.B.; Hosseini, S.R.; Nouri-Hosseini, G. Corneal Epithelial Thickness Mapping After Photorefractive Keratectomy for Myopia. J. Refract. Surg. 2019, 35, 632–641. [Google Scholar] [CrossRef]
- Spadea, L.; Fasciani, R.; Necozione, S.; Balestrazzi, E. Role of the Corneal Epithelium in Refractive Changes Following Laser in Situ Keratomileusis for High Myopia. J. Refract. Surg. 2000, 16, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Reinstein, D.Z.; Archer, T.J.; Gobbe, M. Lenticule Thickness Readout for Small Incision Lenticule Extraction Compared to Artemis Three-Dimensional Very High-Frequency Digital Ultrasound Stromal Measurements. J. Refract. Surg. 2014, 30, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Shetty, R.; Narasimhan, R.; Dadachanji, Z.; Patel, P.; Maheshwari, S.; Chabra, A.; Sinha Roy, A. Early Corneal and Epithelial Remodeling Differences Identified by OCT Imaging and Artificial Intelligence Between Two Transepithelial PRK Platforms. J. Refract. Surg. 2020, 36, 678–686. [Google Scholar] [CrossRef] [PubMed]
- de Ortueta, D.; Arba Mosquera, S.; Baatz, H. Comparison of Standard and Aberration-Neutral Profiles for Myopic LASIK with the SCHWIND ESIRIS Platform. J. Refract. Surg. 2009, 25, 339–349. [Google Scholar] [CrossRef]
- Aslanides, I.M.; Padroni, S.; Arba Mosquera, S.; Ioannides, A.; Mukherjee, A. Comparison of Single-Step Reverse Transepithelial All-Surface Laser Ablation (ASLA) to Alcohol-Assisted Photorefractive Keratectomy. Clin. Ophthalmol. 2012, 6, 973–980. [Google Scholar] [CrossRef] [Green Version]
- Reinstein, D.Z.; Archer, T.J.; Randleman, J.B. JRS Standard for Reporting Astigmatism Outcomes of Refractive Surgery. J. Refract. Surg. 2014, 30, 654–659. [Google Scholar] [CrossRef] [Green Version]
- de Ortueta, D.; Arba Mosquera, S.; Baatz, H. Aberration-Neutral Ablation Pattern in Hyperopic LASIK with the ESIRIS Laser Platform. J. Refract. Surg. 2009, 25, 175–184. [Google Scholar] [CrossRef]
- Fan, L.; Xiong, L.; Zhang, B.; Wang, Z. Longitudinal and Regional Non-Uniform Remodeling of Corneal Epithelium After Topography-Guided FS-LASIK. J. Refract. Surg. 2019, 35, 88–95. [Google Scholar] [CrossRef]
- Savini, G.; Schiano-Lomoriello, D.; Hoffer, K.J. Repeatability of Automatic Measurements by a New Anterior Segment Optical Coherence Tomographer Combined with Placido Topography and Agreement with 2 Scheimpflug Cameras. J. Cataract Refract. Surg. 2018, 44, 471–478. [Google Scholar] [CrossRef]
- de Ortueta, D.; Arba Mosquera, S. Topographic Stability after Hyperopic LASIK. J. Refract. Surg. 2010, 26, 547–554. [Google Scholar] [CrossRef]
- Available online: https://www.iso.org/obp/ui/#iso:std:iso:10938:ed-2:v1:en (accessed on 29 September 2021).
- de Ortueta, D.; von Rüden, D.; Verma, S.; Magnago, T.; Arba-Mosquera, S. Transepithelial Photorefractive Keratectomy in Moderate to High Astigmatism With a Non-Wavefront-Guided Aberration-Neutral Ablation Profile. J. Refract. Surg. 2018, 34, 466–474. [Google Scholar] [CrossRef] [PubMed]
- Kato, N.; Toda, I.; Hori-Komai, Y.; Sakai, C.; Tsubota, K. Five-Year Outcome of LASIK for Myopia. Ophthalmology 2008, 115, 839–844.e2. [Google Scholar] [CrossRef]
- el-Agha, M.S.; Johnston, E.W.; Bowman, R.W.; Cavanagh, H.D.; McCulley, J.P. Excimer Laser Treatment of Spherical Hyperopia: PRK or LASIK? Trans. Am. Ophthalmol. Soc. 2000, 98, 59–66; discussion 66–69. [Google Scholar] [PubMed]
- Spadea, L.; Sabetti, L.; D’Alessandri, L.; Balestrazzi, E. Photorefractive Keratectomy and LASIK for the Correction of Hyperopia: 2-Year Follow-Up. J. Refract. Surg. 2006, 22, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.E.; Klyce, S.D.; McDonald, M.B.; Liu, J.C.; Kaufman, H.E. Changes in Corneal Topography after Excimer Laser Photorefractive Keratectomy for Myopia. Ophthalmology 1991, 98, 1338–1347. [Google Scholar] [CrossRef] [PubMed]
- Kanellopoulos, A.J. Comparison of Corneal Epithelial Remodeling Over 2 Years in LASIK Versus SMILE: A Contralateral Eye Study. Cornea 2019, 38, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Ryu, I.-H.; Kim, B.J.; Lee, J.-H.; Kim, S.W. Comparison of Corneal Epithelial Remodeling After Femtosecond Laser-Assisted LASIK and Small Incision Lenticule Extraction (SMILE). J. Refract. Surg. 2017, 33, 250–256. [Google Scholar] [CrossRef]
- Kanellopoulos, A.J.; Asimellis, G. Longitudinal Postoperative Lasik Epithelial Thickness Profile Changes in Correlation with Degree of Myopia Correction. J. Refract. Surg. 2014, 30, 166–171. [Google Scholar] [CrossRef]
- Reinstein, D.Z.; Srivannaboon, S.; Gobbe, M.; Archer, T.J.; Silverman, R.H.; Sutton, H.; Coleman, D.J. Epithelial Thickness Profile Changes Induced by Myopic LASIK as Measured by Artemis Very High-Frequency Digital Ultrasound. J. Refract. Surg. 2009, 25, 444–450. [Google Scholar] [CrossRef] [Green Version]
- Lin, D.T.C.; Holland, S.P.; Verma, S.; Hogden, J.; Arba-Mosquera, S. Postoperative Corneal Asphericity in Low, Moderate, and High Myopic Eyes After Transepithelial PRK Using a New Pulse Allocation. J. Refract. Surg. 2017, 33, 820–826. [Google Scholar] [CrossRef]
- Kaluzny, B.J.; Szkulmowski, M.; Bukowska, D.M.; Wojtkowski, M. Spectral OCT with Speckle Contrast Reduction for Evaluation of the Healing Process after PRK and Transepithelial PRK. Biomed. Opt. Express 2014, 5, 1089–1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jun, I.; Kang, D.S.Y.; Arba-Mosquera, S.; Kim, E.K.; Seo, K.Y.; Kim, T.-I. Clinical Outcomes of Transepithelial Photorefractive Keratectomy According to Epithelial Thickness. J. Refract. Surg. 2018, 34, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Netto, M.V.; Mohan, R.R.; Sinha, S.; Sharma, A.; Dupps, W.; Wilson, S.E. Stromal Haze, Myofibroblasts, and Surface Irregularity after PRK. Exp. Eye Res. 2006, 82, 788–797. [Google Scholar] [CrossRef] [Green Version]
- Vinciguerra, P.; Azzolini, M.; Airaghi, P.; Radice, P.; De Molfetta, V. Effect of Decreasing Surface and Interface Irregularities after Photorefractive Keratectomy and Laser in Situ Keratomileusis on Optical and Functional Outcomes. J. Refract. Surg. 1998, 14, S199–S203. [Google Scholar] [CrossRef] [PubMed]
- Vinciguerra, P.; Camesasca, F.I.; Vinciguerra, R.; Arba-Mosquera, S.; Torres, I.; Morenghi, E.; Randleman, J.B. Advanced Surface Ablation With a New Software for the Reduction of Ablation Irregularities. J. Refract. Surg. 2017, 33, 89–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moshirfar, M.; Desautels, J.D.; Walker, B.D.; Murri, M.S.; Birdsong, O.C.; Hoopes, P.C.S. Mechanisms of Optical Regression Following Corneal Laser Refractive Surgery: Epithelial and Stromal Responses. Med. Hypothesis Discov. Innov. Ophthalmol. 2018, 7, 1–9. [Google Scholar] [PubMed]
- Fantes, F.E.; Waring, G.O. Effect of Excimer Laser Radiant Exposure on Uniformity of Ablated Corneal Surface. Lasers Surg. Med. 1989, 9, 533–542. [Google Scholar] [CrossRef]
- Reinstein, D.Z.; Archer, T.J.; Gobbe, M. Improved Effectiveness of Transepithelial PTK versus Topography-Guided Ablation for Stromal Irregularities Masked by Epithelial Compensation. J. Refract. Surg. 2013, 29, 526–533. [Google Scholar] [CrossRef]
- Huang, D.; Tang, M.; Shekhar, R. Mathematical Model of Corneal Surface Smoothing after Laser Refractive Surgery. Am. J. Ophthalmol. 2003, 135, 267–278. [Google Scholar] [CrossRef]
- Aslanides, I.M.; Kymionis, G.D. Trans Advanced Surface Laser Ablation (TransPRK) Outcomes Using SmartPulseTechnology. Cont Lens Anterior Eye 2017, 40, 42–46. [Google Scholar] [CrossRef]
- Kaluzny, B.J.; Piotrowiak-Slupska, I.; Kaszuba-Modrzejewska, M.; Stachura, J.; Arba-Mosquera, S.; Verma, S. Three-Year Outcomes after High Hyperopia Correction Using Photorefractive Keratectomy with a Large Ablation Zone. Br. J. Ophthalmol. 2019, 103, 849–854. [Google Scholar] [CrossRef] [PubMed]
- Gauthier-Fournet, L.; Penin, F.; Arba Mosquera, S. Six-Month Outcomes After High Hyperopia Correction Using Laser-Assisted In Situ Keratomileusis With a Large Ablation Zone. Cornea 2019, 38, 1147–1153. [Google Scholar] [CrossRef] [PubMed]
- Simon, G.; Ren, Q.; Kervick, G.N.; Parel, J.M. Optics of the Corneal Epithelium. Refract. Corneal Surg. 1993, 9, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Salah-Mabed, I.; Saad, A.; Gatinel, D. Topography of the Corneal Epithelium and Bowman Layer in Low to Moderately Myopic Eyes. J. Cataract Refract. Surg. 2016, 42, 1190–1197. [Google Scholar] [CrossRef]
- Lohmann, C.P.; Patmore, A.; O’Brart, D.; Reischl, U.; Winkler Mohrenfels, C.; Marshall, J. Regression and Wound Healing after Excimer Laser PRK: A Histopathological Study on Human Corneas. Eur. J. Ophthalmol. 1997, 7, 130–138. [Google Scholar] [CrossRef]
- Moller-Pedersen, T.; Cavanagh, H.D.; Petroll, W.M.; Jester, J.V. Stromal Wound Healing Explains Refractive Instability and Haze Development after Photorefractive Keratectomy: A 1-Year Confocal Microscopic Study. Ophthalmology 2000, 107, 1235–1245. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter (Unit) | Preoperative Value | Postoperative Value | p-Value |
|---|---|---|---|
| Number of eyes | 50 | 50 | --- |
| Laterality OD (%) | 48% | 48% | --- |
| UDVA (logMAR) | 0.9 ± 0.5 (0.2 to 2.0) | 0.0 ± 0.1 (−0.1 to 0.1) | <0.0001 |
| Manifest sphere (D) | −2.41 ± 1.49 −6.00 to 0.00) | 0.18 ± 0.23 (−0.25 to 0.75) | <0.0001 |
| Manifest cylinder (D) | −0.80 ± 0.69 (−2.50 to 0.00) | −0.11 ± 0.19 (−0.75 to 0.00) | <0.0001 |
| CDVA (logMAR) | 0.0 ± 0.1 (−0.1 to 0.2) | 0.0 ± 0.1 (−0.1 to 0.1) | 0.2 |
| Target sphere (D) | 0.05 ± 0.11 (−0.10 to 0.32) | --- | --- |
| Optical zone (mm) | 6.9 ± 0.2 (6.5 to 7.5) | --- | --- |
| Ablation depth (µm) | 111 ± 23 (75 to 162) | --- | --- |
| 3 mm flat keratometry (D) | 42.9 ± 1.7 (39.6 to 47.2) | 40.2 ± 2.4 35.6 to 46.4) | <0.0001 |
| 3 mm steep keratometry (D) | 43.8 ± 1.9 (41.1 to 49.7) | 41.0 ± 2.5 (36.0 to 47.0) | <0.0001 |
| Thinnest epithelium (µm) | 47 ± 3 (42 to 53) | 48 ± 4 (39 to 54) | 0.006 |
| X-position thinnest epithelium (µm) | 46 ± 209 (−272 to 280) | 27 ± 176 (−277 to 207) | 0.2 |
| Y-position thinnest epithelium (µm) | 190 ± 123 (−216 to 280) | 32 ± 234 (−280 to 279) | 0.008 |
| Central epithelium thickness (µm) | 54 ± 3 (48 to 58) | 56 ± 3 (47 to 61) | 0.0002 |
| 3 mm nasal epithelium thickness (µm) | 53 ± 3 (47 to 59) | 55 ± 3 (44 to 61) | 0.0001 |
| 3 mm temporal epithelium thickness (µm) | 52 ± 3 (46 to 59) | 56 ± 3 (46 to 63) | <0.0001 |
| 3 mm superior epithelium thickness (µm) | 51 ± 3 (46 to 57) | 54 ± 4 (44 to 61) | 0.0001 |
| 3 mm inferior epithelium thickness (µm) | 53 ± 3 (47 to 60) | 54 ± 3 (44 to 60) | 0.02 |
| 4 mm nasal epithelium thickness (µm) | 51 ± 3 (45 to 56) | 52 ± 3 (46 to 58) | 0.0007 |
| 4 mm temporal epithelium thickness (µm) | 50 ± 3 (44 to 57) | 52 ± 3 (46 to 58) | <0.0001 |
| 4 mm superior epithelium thickness (µm) | 46 ± 3 (40 to 55) | 49 ± 4 (38 to 56) | <0.0001 |
| 4 mm inferior epithelium thickness (µm) | 51 ± 3 (46 to 58) | 52 ± 3 (42 to 58) | 0.4 |
| Central corneal thickness (µm) | 551 ± 30 (490 to 628) | 484 ± 42 (405 to 582) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Ortueta, D.; von Rüden, D.; Arba-Mosquera, S. Refractive Effect of Epithelial Remodelling in Myopia after Transepithelial Photorefractive Keratectomy. Vision 2022, 6, 74. https://doi.org/10.3390/vision6040074
de Ortueta D, von Rüden D, Arba-Mosquera S. Refractive Effect of Epithelial Remodelling in Myopia after Transepithelial Photorefractive Keratectomy. Vision. 2022; 6(4):74. https://doi.org/10.3390/vision6040074
Chicago/Turabian Stylede Ortueta, Diego, Dennis von Rüden, and Samuel Arba-Mosquera. 2022. "Refractive Effect of Epithelial Remodelling in Myopia after Transepithelial Photorefractive Keratectomy" Vision 6, no. 4: 74. https://doi.org/10.3390/vision6040074