
Muscle Oxygen Extraction during Vascular Occlusion Test in Physically Very Active versus Inactive Healthy Men: A Comparative Study

 , , ,
, , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Type of Study
2.2. Participants
2.3. Protocol
3. Measurements
3.1. Body Composition
3.2. Physical Activity Level
3.3. Muscle Metabolism and Vascular Response
4. Statistical Analysis
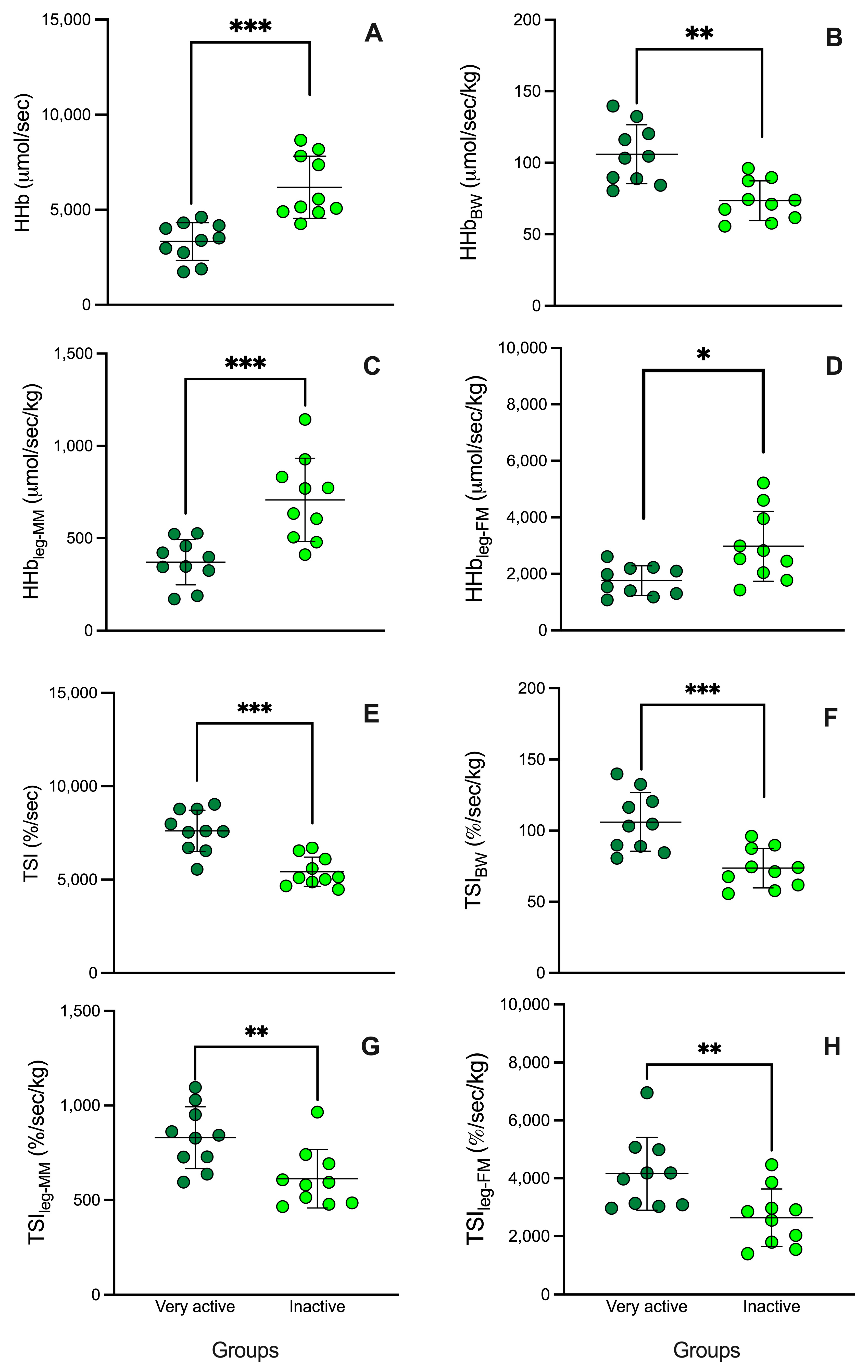
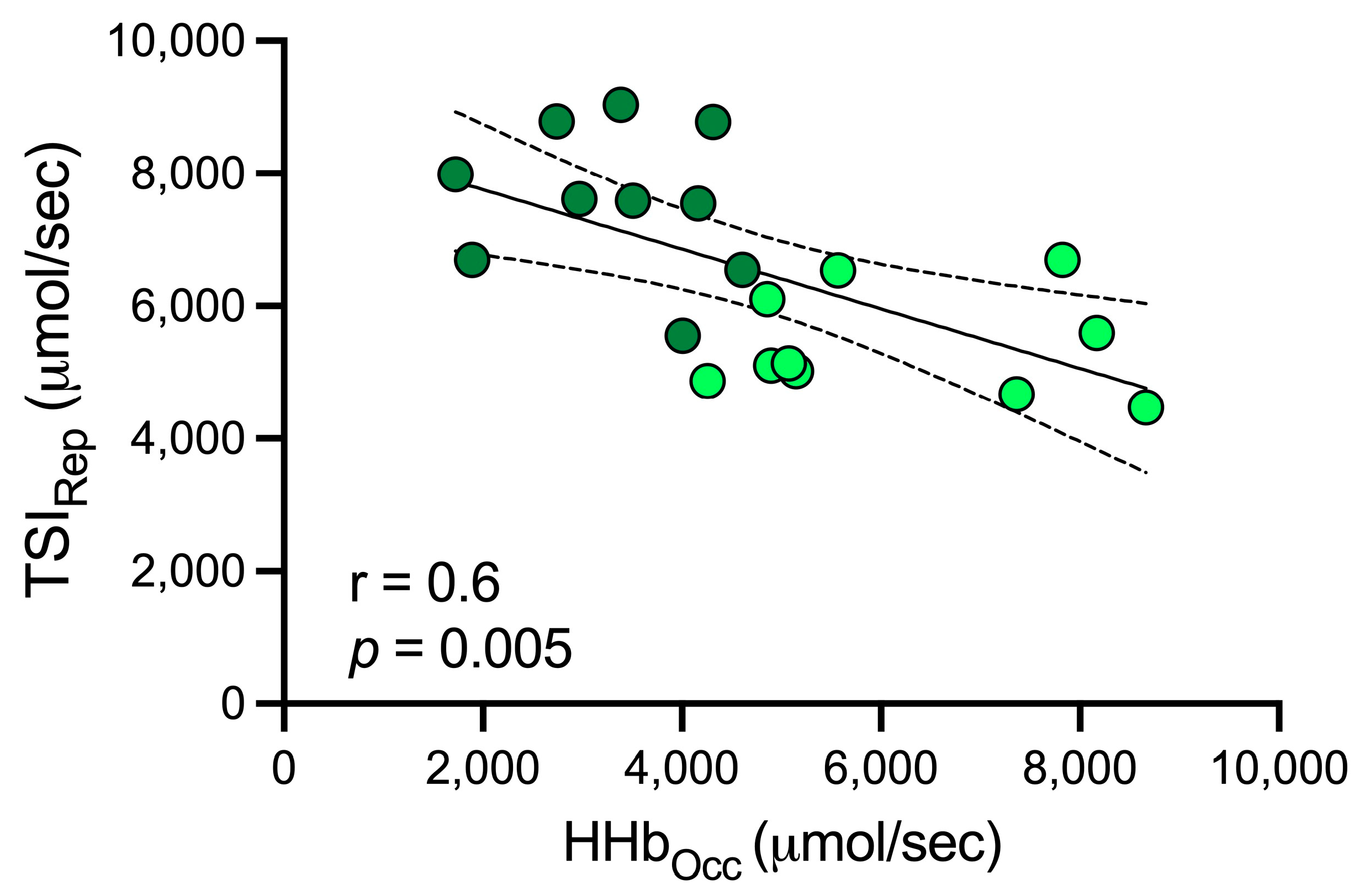
5. Results
6. Discussion
Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of Exercise Is a Major Cause of Chronic Diseases. Compr. Physiol. 2012, 2, 1143. [Google Scholar]
- Paradis-Deschênes, P.; Lapointe, J.; Joanisse, D.R.; Billaut, F. Similar Recovery of Maximal Cycling Performance after Ischemic Preconditioning, Neuromuscular Electrical Stimulation or Active Recovery in Endurance Athletes. J. Sports Sci. Med. 2020, 19, 761. [Google Scholar]
- Warburton, D.E.R.; Nicol, C.W.; Bredin, S.S.D. Health Benefits of Physical Activity: The Evidence. Cmaj 2006, 174, 801–809. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Wichitsranoi, J.; Ladawan, S.; Sirijaichingkul, S.; Settasatian, N.; Leelayuwat, N. Relationship between Aerobic Capacity and Cardiovascular Disease Risk Factors in Thai Men and Women with Normolipidemia and Dyslipidemia. J. Phys. Ther. Sci. 2015, 27, 3503–3509. [Google Scholar] [CrossRef]
- Casey, D.P.; Joyner, M.J. Local Control of Skeletal Muscle Blood Flow during Exercise: Influence of Available Oxygen. J. Appl. Physiol. 2011, 111, 1527–1538. [Google Scholar] [CrossRef]
- Grassi, B.; Quaresima, V. Near-Infrared Spectroscopy and Skeletal Muscle Oxidative Function in Vivo in Health and Disease: A Review from an Exercise Physiology Perspective. J. Biomed. Opt. 2016, 21, 91313. [Google Scholar] [CrossRef]
- Wu, Z.-J.; Han, C.; Wang, Z.-Y.; Li, F.-H. Combined Training Prescriptions for Improving Cardiorespiratory Fitness, Physical Fitness, Body Composition, and Cardiometabolic Risk Factors in Older Adults: Systematic Review and Meta-Analysis of Controlled Trials. Sci. Sports 2023, 39, 1–18. [Google Scholar] [CrossRef]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. Jama 2013, 310, 2191–2194. [Google Scholar]
- Carrion, B.M.; Wells, A.; Mayhew, J.L.; Koch, A.J. Concordance among Bioelectrical Impedance Analysis Measures of Percent Body Fat in Athletic Young Adults. Int. J. Exerc. Sci. 2019, 12, 324. [Google Scholar]
- Ryan, T.E.; Erickson, M.L.; Brizendine, J.T.; Young, H.J.; McCully, K.K. Noninvasive Evaluation of Skeletal Muscle Mitochondrial Capacity with Near-Infrared Spectroscopy: Correcting for Blood Volume Changes. J. Appl. Physiol. 2012, 113, 175–183. [Google Scholar] [CrossRef]
- Rosenberry, R.; Nelson, M.D. Reactive Hyperemia: A Review of Methods, Mechanisms, and Considerations. Am. J. Physiol. Integr. Comp. Physiol. 2020, 318, R605–R618. [Google Scholar] [CrossRef]
- Sanni, A.A.; McCully, K.K. Interpretation of Near-Infrared Spectroscopy (NIRS) Signals in Skeletal Muscle. J. Funct. Morphol. Kinesiol. 2019, 4, 28. [Google Scholar] [CrossRef]
- Skattebo, Ø.; Calbet, J.A.L.; Rud, B.; Capelli, C.; Hallén, J. Contribution of Oxygen Extraction Fraction to Maximal Oxygen Uptake in Healthy Young Men. Acta Physiol. 2020, 230, e13486. [Google Scholar] [CrossRef]
- Ryan, T.E.; Brophy, P.; Lin, C.; Hickner, R.C.; Neufer, P.D. Assessment of in Vivo Skeletal Muscle Mitochondrial Respiratory Capacity in Humans by Near-infrared Spectroscopy: A Comparison with in Situ Measurements. J. Physiol. 2014, 592, 3231–3241. [Google Scholar] [CrossRef]
- Soares, R.N.; McLay, K.M.; George, M.A.; Murias, J.M. Differences in Oxidative Metabolism Modulation Induced by Ischemia/Reperfusion between Trained and Untrained Individuals Assessed by NIRS. Physiol. Rep. 2017, 5, e13384. [Google Scholar] [CrossRef]
- Bull, F.C.; Maslin, T.S.; Armstrong, T. Global Physical Activity Questionnaire (GPAQ): Nine Country Reliability and Validity Study. J. Phys. Act. Health 2009, 6, 790–804. [Google Scholar] [CrossRef]
- Volpi, E.; Nazemi, R.; Fujita, S. Muscle Tissue Changes with Aging. Curr. Opin. Clin. Nutr. Metab. Care 2004, 7, 405. [Google Scholar] [CrossRef]
- Lagerwaard, B.; Nieuwenhuizen, A.G.; de Boer, V.C.J.; Keijer, J. In Vivo Assessment of Mitochondrial Capacity Using NIRS in Locomotor Muscles of Young and Elderly Males with Similar Physical Activity Levels. GeroScience 2020, 42, 299–310. [Google Scholar] [CrossRef]
- Iannetta, D.; Inglis, E.C.; Soares, R.N.; McLay, K.M.; Pogliaghi, S.; Murias, J.M. Reliability of Microvascular Responsiveness Measures Derived from Near-Infrared Spectroscopy across a Variety of Ischemic Periods in Young and Older Individuals. Microvasc. Res. 2019, 122, 117–124. [Google Scholar] [CrossRef]
- Ichimura, S.; Murase, N.; Osada, T.; Kime, R.; Homma, T.; Ueda, C.; Nagasawa, T.; Motobe, M.; Hamaoka, T.; Katsumura, T. Age and Activity Status Affect Muscle Reoxygenation Time after Maximal Cycling Exercise. Med. Sci. Sport. Exerc. 2006, 38, 1277–1281. [Google Scholar] [CrossRef]
- Santana, P.V.; Cardenas, L.Z.; De Albuquerque, A.L.P.; De Carvalho, C.R.R.; Caruso, P. Diaphragmatic Ultrasound Findings Correlate with Dyspnea, Exercise Tolerance, Health-Related Quality of Life and Lung Function in Patients with Fibrotic Interstitial Lung Disease. BMC Pulm. Med. 2019, 19, 1–10. [Google Scholar] [CrossRef]
- Tao, X.; Chen, Y.; Zhen, K.; Ren, S.; Lv, Y.; Yu, L. Effect of Continuous Aerobic Exercise on Endothelial Function: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Physiol. 2023, 14, 1043108. [Google Scholar] [CrossRef] [PubMed]
- Padilla, J.; Simmons, G.H.; Bender, S.B.; Arce-Esquivel, A.A.; Whyte, J.J.; Laughlin, M.H. Vascular Effects of Exercise: Endothelial Adaptations beyond Active Muscle Beds. Physiology 2011, 26, 132–145. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, V.d.S.; da Silva Tavares, A.C.F.; Volino-Souza, M.; de Oliveira, G.V.; Alvares, T.S. Association between Femoral Artery Flow-Mediated Dilation and Muscle Oxygen Saturation Parameters in Healthy, Young Individuals. J. Cardiovasc. Dev. Dis. 2023, 10, 63. [Google Scholar] [CrossRef]
- Alvares, T.S.; Oliveira, G.V.d.; Soares, R.; Murias, J.M. Near-Infrared Spectroscopy-Derived Total Haemoglobin as an Indicator of Changes in Muscle Blood Flow during Exercise-Induced Hyperaemia. J. Sports Sci. 2020, 38, 751–758. [Google Scholar] [CrossRef]
- Beever, A.T.; Tripp, T.R.; Zhang, J.; MacInnis, M.J. NIRS-Derived Skeletal Muscle Oxidative Capacity Is Correlated with Aerobic Fitness and Independent of Sex. J. Appl. Physiol. 2020, 129, 558–568. [Google Scholar] [CrossRef]
- Rasica, L.; Inglis, E.C.; Iannetta, D.; Soares, R.N.; Murias, J.M. Fitness Level-and Sex-Related Differences in Macrovascular and Microvascular Responses during Reactive Hyperemia. Med. Sci. Sports Exerc. 2022, 54, 497–506. [Google Scholar] [CrossRef]
- Soares, R.N.; Murias, J.M. Near-Infrared Spectroscopy Assessment of Microvasculature Detects Difference in Lower Limb Vascular Responsiveness in Obese Compared to Lean Individuals. Microvasc. Res. 2018, 118, 31–35. [Google Scholar] [CrossRef]
- Koutlas, A.; Smilios, I.; Kokkinou, E.M.; Myrkos, A.; Kounoupis, A.; Dipla, K.; Zafeiridis, A. NIRS-Derived Muscle-Deoxygenation and Microvascular Reactivity During Occlusion–Reperfusion at Rest Are Associated With Whole-Body Aerobic Fitness. Res. Q. Exerc. Sport 2023, 1–13. [Google Scholar] [CrossRef]
- Ross, R.; Blair, S.N.; Arena, R.; Church, T.S.; Després, J.P.; Franklin, B.A.; Haskell, W.L.; Kaminsky, L.A.; Levine, B.D.; Lavie, C.J.; et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e653–e699. [Google Scholar] [CrossRef]
- Dipla, K.; Triantafyllou, A.; Grigoriadou, I.; Kintiraki, E.; Triantafyllou, G.A.; Poulios, P.; Vrabas, I.S.; Zafeiridis, A.; Douma, S.; Goulis, D.G. Impairments in Microvascular Function and Skeletal Muscle Oxygenation in Women with Gestational Diabetes Mellitus: Links to Cardiovascular Disease Risk Factors. Diabetologia 2017, 60, 192–201. [Google Scholar] [CrossRef]
- Bauer, T.A.; Reusch, J.E.B.; Levi, M.; Regensteiner, J.G. Skeletal Muscle Deoxygenation after the Onset of Moderate Exercise Suggests Slowed Microvascular Blood Flow Kinetics in Type 2 Diabetes. Diabetes Care 2007, 30, 2880–2885. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Active (n = 10) | Inactive (n = 10) | p-Value |
|---|---|---|---|
| Age (years) | 30.0 ± 7.4 | 25.5 ± 4.2 | 0.11 |
| Weight (kg) | 72.7 ± 8.1 | 74.9 ± 11.8 | 0.63 |
| Height (cm) | 173.7 ± 7.6 | 173.0 ± 6.4 | 0.83 |
| Body mass index (kg/m2) | 24.0 ± 1.4 | 24.9 ± 2.9 | 0.45 |
| Fat mass (kg) | 12.9 ± 3.9 | 15.6 ± 6.5 | 0.28 |
| Muscle mass (kg) | 34.2 ± 3.5 | 33.7 ± 6.2 | 0.85 |
| Non-dominant leg fat mass (kg) | 1.9 ± 0.47 | 2.3 ± 0.88 | 0.29 |
| Non-dominant leg muscle mass (kg) | 9.0 ± 1.4 | 9.2 ± 1.0 | 0.75 |
| MVPA (min/week) | 547.3 ± 31.1 * | 117.3 ± 18.1 | <0.01 |
| Skinfold thigh (mm) | 11.1 ± 2.4 * | 15.6 ± 4.6 | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuesta, M.; Yáñez-Sepúlveda, R.; Monsalves-Álvarez, M.; Vásquez-Bonilla, A.; Olivares-Arancibia, J.; Rojas-Valverde, D.; Alvear-Órdenes, I. Muscle Oxygen Extraction during Vascular Occlusion Test in Physically Very Active versus Inactive Healthy Men: A Comparative Study. J. Funct. Morphol. Kinesiol. 2024, 9, 57. https://doi.org/10.3390/jfmk9020057
Tuesta M, Yáñez-Sepúlveda R, Monsalves-Álvarez M, Vásquez-Bonilla A, Olivares-Arancibia J, Rojas-Valverde D, Alvear-Órdenes I. Muscle Oxygen Extraction during Vascular Occlusion Test in Physically Very Active versus Inactive Healthy Men: A Comparative Study. Journal of Functional Morphology and Kinesiology. 2024; 9(2):57. https://doi.org/10.3390/jfmk9020057
Chicago/Turabian StyleTuesta, Marcelo, Rodrigo Yáñez-Sepúlveda, Matías Monsalves-Álvarez, Aldo Vásquez-Bonilla, Jorge Olivares-Arancibia, Daniel Rojas-Valverde, and Ildefonso Alvear-Órdenes. 2024. "Muscle Oxygen Extraction during Vascular Occlusion Test in Physically Very Active versus Inactive Healthy Men: A Comparative Study" Journal of Functional Morphology and Kinesiology 9, no. 2: 57. https://doi.org/10.3390/jfmk9020057