
The Effectiveness of External Verbal Feedback on Balance in Athletes with Chronic Ankle Instability

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
- (a)
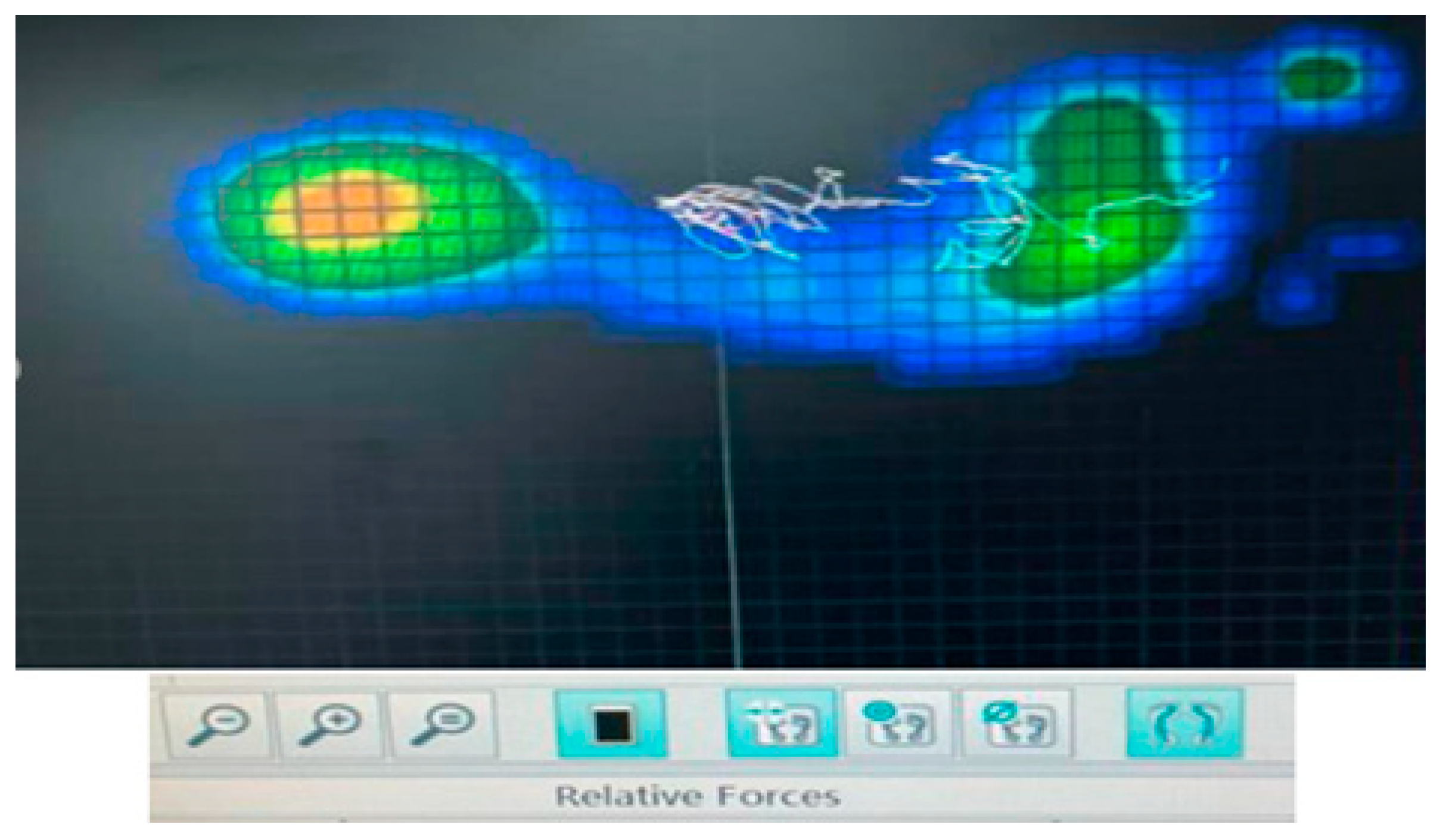
- Y-Balance test on a plantar pressure recording platform:
- (b)
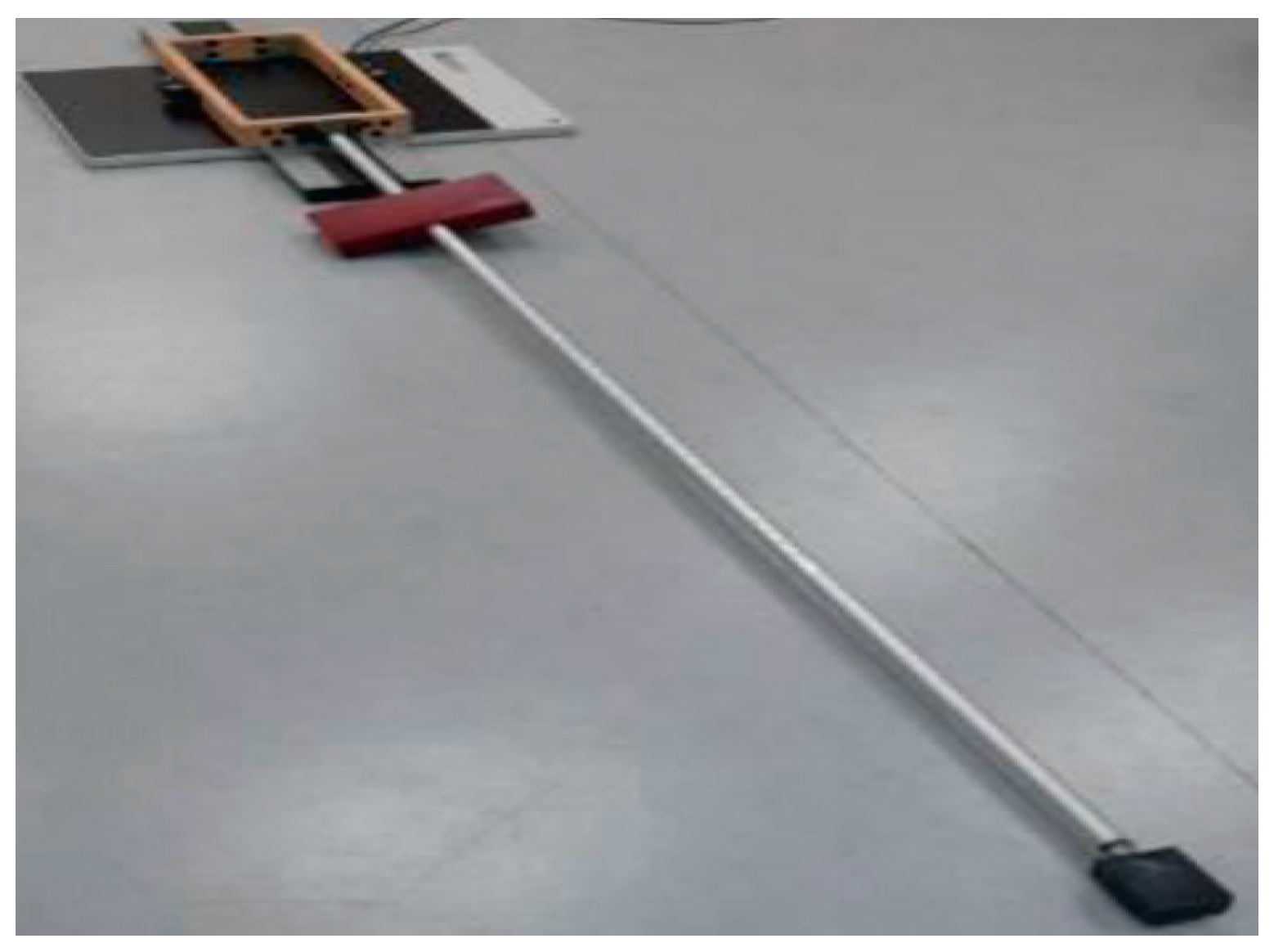
- Balance tray
- (c)
- Cumberland Ankle Joint Instability Tool (CAIT)
2.3. Procedure
2.4. Statistical Analyses
3. Results
3.1. Examining the Comparisons and Retention of Balance Learning with Y-Balance Test
3.2. Examining the Comparisons and Retention of Balance on Center Length and Center Velocity Pressure Distribution during the Y-Balance Test
3.3. Examining the Comparisons and Retention of Learning of Balance on the CAIT
4. Discussion
Limitations and Future Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Waterman, B.R.; Owens, B.D.; Davey, S.; Zacchilli, M.A.; Belmont, P.J., Jr. The epidemiology of ankle sprains in the United States. J. Bone Jt. Surg. Am. Vol. 2010, 92, 2279–2284. [Google Scholar] [CrossRef]
- Chen, E.T.; Borg-Stein, J.; McInnis, K.C. Ankle Sprains: Evaluation, Rehabilitation, and Prevention. Curr. Sports Med. Rep. 2019, 18, 217–223. [Google Scholar] [CrossRef]
- Safran, M.R.; Benedetti, R.S.; Bartolozzi, A.R., 3rd; Mandelbaum, B.R. Lateral ankle sprains: A comprehensive review: Part 1: Etiology, pathoanatomy, histopathogenesis, and diagnosis. Med. Sci. Sports Exerc. 1999, 31, S429–S437. [Google Scholar] [CrossRef]
- Delahunt, E.; Coughlan, G.F.; Caulfield, B.; Nightingale, E.J.; Lin, C.W.; Hiller, C.E. Inclusion criteria when investigating insufficiencies in chronic ankle instability. Med. Sci. Sports Exerc. 2010, 42, 2106–2121. [Google Scholar] [CrossRef] [PubMed]
- Swenson, D.M.; Collins, C.L.; Fields, S.K.; Comstock, R.D. Epidemiology of U.S. high school sports-related ligamentous ankle injuries, 2005/06–2010/11. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2013, 23, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Delahunt, E.; Bleakley, C.M.; Caulfield, B.; Docherty, C.L.; Fong, D.T.; Fourchet, F.; Hertel, J.; Hiller, C.E.; Kaminski, T.W.; et al. Selection criteria for patients with chronic ankle instability in controlled research: A position statement of the International Ankle Consortium. J. Athl. Train. 2014, 49, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Willems, T.; Witvrouw, E.; Verstuyft, J.; Vaes, P.; De Clercq, D. Proprioception and Muscle Strength in Subjects With a History of Ankle Sprains and Chronic Instability. J. Athl. Train. 2002, 37, 487–493. [Google Scholar] [PubMed]
- Drewes, L.K.; McKeon, P.O.; Paolini, G.; Riley, P.; Kerrigan, D.C.; Ingersoll, C.D.; Hertel, J. Altered ankle kinematics and shank-rear-foot coupling in those with chronic ankle instability. J. Sport Rehabil. 2009, 18, 375–388. [Google Scholar] [CrossRef] [PubMed]
- McKeon, P.O.; Ingersoll, C.D.; Kerrigan, D.C.; Saliba, E.; Bennett, B.C.; Hertel, J. Balance training improves function and postural control in those with chronic ankle instability. Med. Sci. Sports Exerc. 2008, 40, 1810–1819. [Google Scholar] [CrossRef] [PubMed]
- McGuine, T.A.; Greene, J.J.; Best, T.; Leverson, G. Balance as a predictor of ankle injuries in high school basketball players. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2000, 10, 239–244. [Google Scholar] [CrossRef]
- Linens, S.W.; Ross, S.E.; Arnold, B.L. Wobble Board Rehabilitation for Improving Balance in Ankles With Chronic Instability. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2016, 26, 76–82. [Google Scholar] [CrossRef]
- Mettler, A.; Chinn, L.; Saliba, S.A.; McKeon, P.O.; Hertel, J. Balance training and center-of-pressure location in participants with chronic ankle instability. J. Athl. Train. 2015, 50, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Sierra-Guzmán, R.; Jiménez, F.; Abián-Vicén, J. Predictors of chronic ankle instability: Analysis of peroneal reaction time, dynamic balance and isokinetic strength. Clin. Biomech. 2018, 54, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Anguish, B.; Sandrey, M.A. Two 4-Week Balance-Training Programs for Chronic Ankle Instability. J. Athl. Train. 2018, 53, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Han, X.G.; Sheng, J.; Ma, S.J. Virtual reality for improving balance in patients after stroke: A systematic review and meta-analysis. Clin. Rehabil. 2016, 30, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Hall, E.A.; Chomistek, A.K.; Kingma, J.J.; Docherty, C.L. Balance- and Strength-Training Protocols to Improve Chronic Ankle Instability Deficits, Part I: Assessing Clinical Outcome Measures. J. Athl. Train. 2018, 53, 568–577. [Google Scholar] [CrossRef]
- Schmidt, R.A.; Wrisberg, C.A. Motor Learning and Performance: A Situation-Based Learning Approach; Human Kinetics: Champaign, IL, USA, 2008. [Google Scholar]
- Gokeler, A.; Benjaminse, A.; Welling, W.; Alferink, M.; Eppinga, P.; Otten, B. The effects of attentional focus on jump performance and knee joint kinematics in patients after ACL reconstruction. Phys. Ther. Sport Off. J. Assoc. Chart. Physiother. Sports Med. 2015, 16, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Gredin, V.; Williams, A.M. The Relative Effectiveness of Various Instructional Approaches During the Performance and Learning of Motor Skills. J. Mot. Behav. 2016, 48, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Orangi, B.M.; Yaali, R.; Bahram, A.; Aghdasi, M.T.; van der Kamp, J.; Vanrenterghem, J.; Jones, P.A. Motor learning methods that induce high practice variability reduce kinematic and kinetic risk factors of non-contact ACL injury. Hum. Mov. Sci. 2021, 78, 102805. [Google Scholar] [CrossRef]
- Benjaminse, A.; Otten, B.; Gokeler, A.; Diercks, R.L.; Lemmink, K.A. Motor learning strategies in basketball players and its implications for ACL injury prevention: A randomized controlled trial. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 2365–2376. [Google Scholar] [CrossRef]
- Forsyth, L.; Bonacci, J.; Childs, C. A pilot randomised control trial of the efficacy of stability-based training with visualisation for people with chronic ankle instability. Med. Biol. Eng. Comput. 2022, 60, 1199–1209. [Google Scholar] [CrossRef]
- Johnson, L.; Burridge, J.H.; Demain, S.H. Internal and external focus of attention during gait re-education: An observational study of physical therapist practice in stroke rehabilitation. Phys. Ther. 2013, 93, 957–966. [Google Scholar] [CrossRef]
- Wulf, G.; Shea, C.; Lewthwaite, R. Motor skill learning and performance: A review of influential factors. Med. Educ. 2010, 44, 75–84. [Google Scholar] [CrossRef]
- Christakou, A.; Gkikopoulou, A.; Iosif, E.; Gioftsos, G. The effectiveness of focus of attention in static balance and functional ability of chronic ankle instability. A pilot study. Iran. Rehabil. J. 2024, accepted. [Google Scholar]
- Winstein, C.J. Knowledge of results and motor learning--Implications for physical therapy. Phys. Ther. 1991, 71, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.I.; Magill, R.A.; Mayo, A.M.; Steel, K.A. Enhancing motor skill acquisition with augmented feedback. In Skill Acquisition in Sport; Routledge: London, UK, 2019; pp. 3–19. [Google Scholar]
- Paraskevopoulos, E.; Simeonidis, T.; Tsolakis, C.; Koulouvaris, P.; Papandreou, M. Mirror cross-exercise on a kinetic chain approach improves throwing performance in professional volleyball athletes with scapular dyskinesis. J. Sport Rehabil. 2021, 31, 131–139. [Google Scholar] [CrossRef]
- Paraskevopoulos, E.; Simeonidis, T.; Tsolakis, C.; Koulouvaris, P.; Papandreou, M. The adjunctive benefits of mirror cross education on kinetic chain exercise approach in volleyball athletes with scapular dyskinesis. J. Sports Med. Phys. Fit. 2021, 62, 98–109. [Google Scholar] [CrossRef]
- RL, E.S.; Maia, D.F.M.; de Oliveira, R.R.; Scattone Silva, R. Simple verbal instructions are able to improve quality of movement during the lateral step-down test in healthy females. J. Bodyw. Mov. Ther. 2021, 27, 207–215. [Google Scholar] [CrossRef]
- Halperin, I.; Chapman, D.W.; Thompson, K.G.; Abbiss, C. False-performance feedback does not affect punching forces and pacing of elite boxers. J. Sports Sci. 2019, 37, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Puce, L.; Trompetto, C.; Currà, A.; Marinelli, L.; Mori, L.; Panascì, M.; Cotellessa, F.; Biz, C.; Bragazzi, N.L.; Ruggieri, P. The Effect of Verbal Encouragement on Performance and Muscle Fatigue in Swimming. Medicina 2022, 58, 1709. [Google Scholar] [CrossRef] [PubMed]
- Jaffri, A.H.; Saliba, S. Does verbal encouragement change dynamic balance? The effect of verbal encouragement on Star Excursion Balance Test performance in chronic ankle Instability. Braz. J. Phys. Ther. 2021, 25, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Rendos, N.K.; Zajac-Cox, L.; Thomas, R.; Sato, S.; Eicholtz, S.; Kesar, T.M. Verbal feedback enhances motor learning during post-stroke gait retraining. Top. Stroke Rehabil. 2021, 28, 362–377. [Google Scholar] [CrossRef] [PubMed]
- Plisky, P.J.; Rauh, M.J.; Kaminski, T.W.; Underwood, F.B. Star Excursion Balance Test as a predictor of lower extremity injury in high school basketball players. J. Orthop. Sports Phys. Ther. 2006, 36, 911–919. [Google Scholar] [CrossRef]
- Zhang, R.; Qi, Q.; Song, W.; Chen, Y. Predicting the success of multimodal rehabilitation in chronic ankle instability based on patient-reported outcomes. BMC Musculoskelet. Disord. 2022, 23, 706. [Google Scholar] [CrossRef]
- Karagiannakis, D.N.; Iatridou, K.I.; Mandalidis, D.G. Ankle muscles activation and postural stability with Star Excursion Balance Test in healthy individuals. Hum. Mov. Sci. 2020, 69, 102563. [Google Scholar] [CrossRef] [PubMed]
- Cobos-Moreno, P.; Astasio-Picado, Á.; Martínez-Nova, A.; Sánchez-Rodríguez, R.; Escamilla-Martínez, E.; Gómez-Martín, B. The Podoprint® plantar pressure platform: Evaluation of reliability and repeatability, and determination of the normality parameters. J. Tissue Viability 2022, 31, 619–624. [Google Scholar] [CrossRef]
- Sipe, C.L.; Ramey, K.D.; Plisky, P.P.; Taylor, J.D. Y-Balance Test: A Valid and Reliable Assessment in Older Adults. J. Aging Phys. Act. 2019, 27, 663–669. [Google Scholar] [CrossRef]
- Mandalidis, D.G.; Karagiannakis, D.N. A comprehensive method for assessing postural control during dynamic balance testing. MethodsX 2020, 7, 100964. [Google Scholar] [CrossRef]
- Bizovska, L.; Janura, M.; Svoboda, Z.; Cerny, M.; Krohova, J.; Smondrk, M. Intra- and inter-session reliability of traditional and entropy-based variables describing stance on a wobble board. Med. Eng. Phys. 2017, 50, 29–34. [Google Scholar] [CrossRef]
- Hou, Z.C.; Huang, H.S.; Ao, Y.F.; Hu, Y.L.; Jiao, C.; Guo, Q.W.; Miao, X.; Li, N.; Jiang, Y.F.; Jiang, D. The effectiveness and sustainability of supervised balance training in chronic ankle instability with grade III ligament injury: A one-year prospective study. J. Foot Ankle Res. 2022, 15, 9. [Google Scholar] [CrossRef]
- Taghavi Asl, A.; Shojaedin, S.S.; Hadadnezhad, M. Comparison of effect of wobble board training with and without cognitive intervention on balance, ankle proprioception and jump landing kinetic parameters of men with chronic ankle instability: A randomized control trial. BMC Musculoskelet. Disord. 2022, 23, 888. [Google Scholar] [CrossRef] [PubMed]
- Tsekoura, M.; Billis, E.; Fousekis, K.; Christakou, A.; Tsepis, E. Cross cultural adaptation, reliability, and validity of the Greek version of the Cumberland Ankle Instability Tool. Physiother. Theory Pract. 2021, 37, 954–962. [Google Scholar] [CrossRef] [PubMed]
- Hiller, C.E.; Refshauge, K.M.; Bundy, A.C.; Herbert, R.D.; Kilbreath, S.L. The Cumberland ankle instability tool: A report of validity and reliability testing. Arch. Phys. Med. Rehabil. 2006, 87, 1235–1241. [Google Scholar] [CrossRef]
- Keith, T.R.; Condon, T.A.; Phillips, A.; McKeon, P.O.; King, D.L. Postural control strategies are dependent on reach direction in the star excursion balance test. Int. J. Athl. Ther. Train. 2016, 21, 33–39. [Google Scholar] [CrossRef]
- Webster, K.A.; Gribble, P.A. Functional rehabilitation interventions for chronic ankle instability: A systematic review. J. Sport Rehabil. 2010, 19, 98–114. [Google Scholar] [CrossRef]
- Shea, C.H.; Wulf, G. Enhancing motor learning through external-focus instructions and feedback. Hum. Mov. Sci. 1999, 18, 553–571. [Google Scholar] [CrossRef]
- Han, S.; Lee, H.; Hopkins, J.T. Acute effects of external visual feedback using cross-line laser on landing neuromechanics and postural control in chronic ankle instability. Sports Biomech. 2022, 1, 1–16. [Google Scholar] [CrossRef]
- Schmidt, R.A.; Lee, T.D. Motor Control and Learning: A Behavioral Emphasis, 4th ed.; Human Kinetics: Champaign, IL, USA, 2005. [Google Scholar]
- Ohno, H.; Wada, M.; Saitoh, J.; Sunaga, N.; Nagai, M. The effect of anxiety on postural control in humans depends on visual information processing. Neurosci. Lett. 2004, 364, 37–39. [Google Scholar] [CrossRef]
- Rozzi, S.L.; Lephart, S.M.; Sterner, R.; Kuligowski, L. Balance training for persons with functionally unstable ankles. J. Orthop. Sports Phys. Ther. 1999, 29, 478–486. [Google Scholar] [CrossRef]
- Ottaviani, R.A.; Ashton-Miller, J.A.; Wojtys, E.M. Inversion and eversion strengths in the weightbearing ankle of young women: Effects of plantar flexion and basketball shoe height. Am. J. Sports Med. 2001, 29, 219–225. [Google Scholar] [CrossRef]
- Greene, J.J.; McGuine, T.A.; Leverson, G.; Best, T.M. Anthropometric and performance measures for high school basketball players. J. Athl. Train. 1998, 33, 229. [Google Scholar] [PubMed]
- Deodato, M.; Coan, L.; Buoite Stella, A.; Ajčević, M.; Martini, M.; Di Lenarda, L.; Ratti, C.; Accardo, A.; Murena, L. Inertial sensors-based assessment to detect hallmarks of chronic ankle instability during single-leg standing: Is the healthy limb “healthy”? Clin. Biomech. 2023, 107, 106036. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age (Years) (Μ ± SD) | Height (cm) (Μ ± SD) | Weight (Kilogram) (Μ ± SD) | BMI (kg/m2) (M ± SD) | Time since the Last Sprain (Months) (Μ ± SD) | History of Sprains (Number) (Μ ± SD) | |
|---|---|---|---|---|---|---|
| Experimental group with feedback | 19.8 ± 1.03 | 172.3 ± 9.31 | 69.10 ± 11.78 | 23.35± 10.24 | 12.6 ± 7.56 | 2.4 ± 1.28 |
| 1st Control group without feedback | 21.4 ± 1.95 | 172.9 ± 10.16 | 70.80± 10.59 | 23.93 ± 10.23 | 6.2 ±4.02 | 2.9 ± 1.13 |
| 2nd Control group without balance training-without feedback | 23.7 ± 1.63 | 181.8 ± 4.96 | 80.10 ± 7.78 | 24.58 ± 6.34 | 11.5 ± 7.89 | 2.6 ± 1.35 |
| Experimental Group with Feedback | 1st Control Group without Feedback | 2nd Control Group without Balance Training—without Feedback | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | 1st measurement | 2nd measurement | 3nd measurement | 1st measurement | 2nd measurement | 3nd measurement | 1st measurement | 2nd measurement | 3nd measurement |
| Y-Balance | 96.13 ± 9.32 | 99.97 ± 7.38 | 100.19 ± 6.18 | 96.13 ± 9.32 | 99.97 ± 7.38 | 100.19 ± 6.18 | 94.32 ± 5.99 | 93.71 ± 7.49 | 95.18 ± 5.68 |
| Centre length pressure distribution | 567.61 ± 168.7 | 514.51 ± 176.26 | 524.44 ± 167.1 | 659.64 ± 205.8 | 671.99 ± 167.3 | 588.46 ± 119.7 | 656.47 ± 211.7 | 624.22 ± 159.7 | 609.7± `186.7 |
| Pressure distribution centre velocity | 56.75 ± 16.87 | 51.44 ± 17.62 | 52.44 ± 16.42 | 56.75 ± 16.87 | 51.44 ± 17.62 | 52.44 ± 16.42 | 56.75 ± 16.87 | 51.44 ± 17.62 | 52.44 ± 16.42 |
| CAIT | 17.40 ± 4.88 | 21.90 ± 1.85 | 22 ± 1.73 | 19.80 ± 3.12 | 22.67 ± 1.5 | 22.11 ± 1.76 | 20.60 ± 3.02 | 20.88 ± 2.58 | 20.86 ± 2.79 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parlakidis, K.; Kontopoulos, L.A.; Mandalidis, D.; Paraskevopoulos, E.; Papandreou, M.; Kapreli, E.; Christakou, A. The Effectiveness of External Verbal Feedback on Balance in Athletes with Chronic Ankle Instability. J. Funct. Morphol. Kinesiol. 2024, 9, 56. https://doi.org/10.3390/jfmk9010056
Parlakidis K, Kontopoulos LA, Mandalidis D, Paraskevopoulos E, Papandreou M, Kapreli E, Christakou A. The Effectiveness of External Verbal Feedback on Balance in Athletes with Chronic Ankle Instability. Journal of Functional Morphology and Kinesiology. 2024; 9(1):56. https://doi.org/10.3390/jfmk9010056
Chicago/Turabian StyleParlakidis, Konstantinos, Lazaros Alexandors Kontopoulos, Dimitris Mandalidis, Eleftherios Paraskevopoulos, Maria Papandreou, Eleni Kapreli, and Anna Christakou. 2024. "The Effectiveness of External Verbal Feedback on Balance in Athletes with Chronic Ankle Instability" Journal of Functional Morphology and Kinesiology 9, no. 1: 56. https://doi.org/10.3390/jfmk9010056