
The Effects of Massage Guns on Performance and Recovery: A Systematic Review

 , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
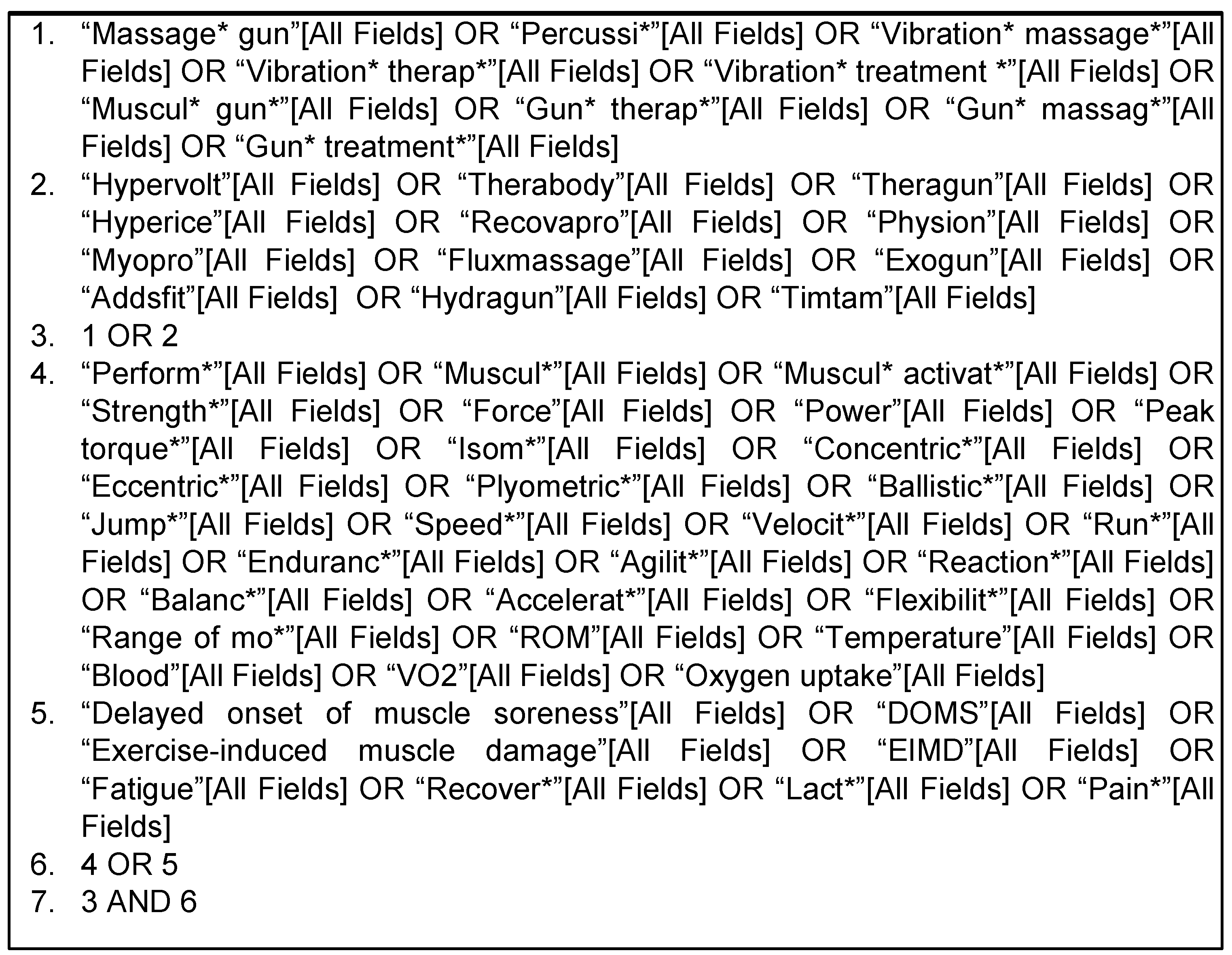
2.1. Search Strategy and Information Sources
2.2. Study Selection Process
2.3. Data Extraction and Syntheses
2.4. Outcomes
- Primary Outcomes:
- Muscular activation, strength, power;
- Speed, endurance, oxygen uptake;
- Agility, reaction, balance;
- Flexibility, range of motion, myofascial release;
- Kinetics, kinematics;
- Blood flow, lymphatic flow;
- Biomarkers of fatigue, recovery, pain, exercise-induced muscle damage, delayed-onset muscle soreness.
- Secondary Outcomes:
- Adverse effects after using massage gun.
2.5. Risk of Bias Assessment
3. Results
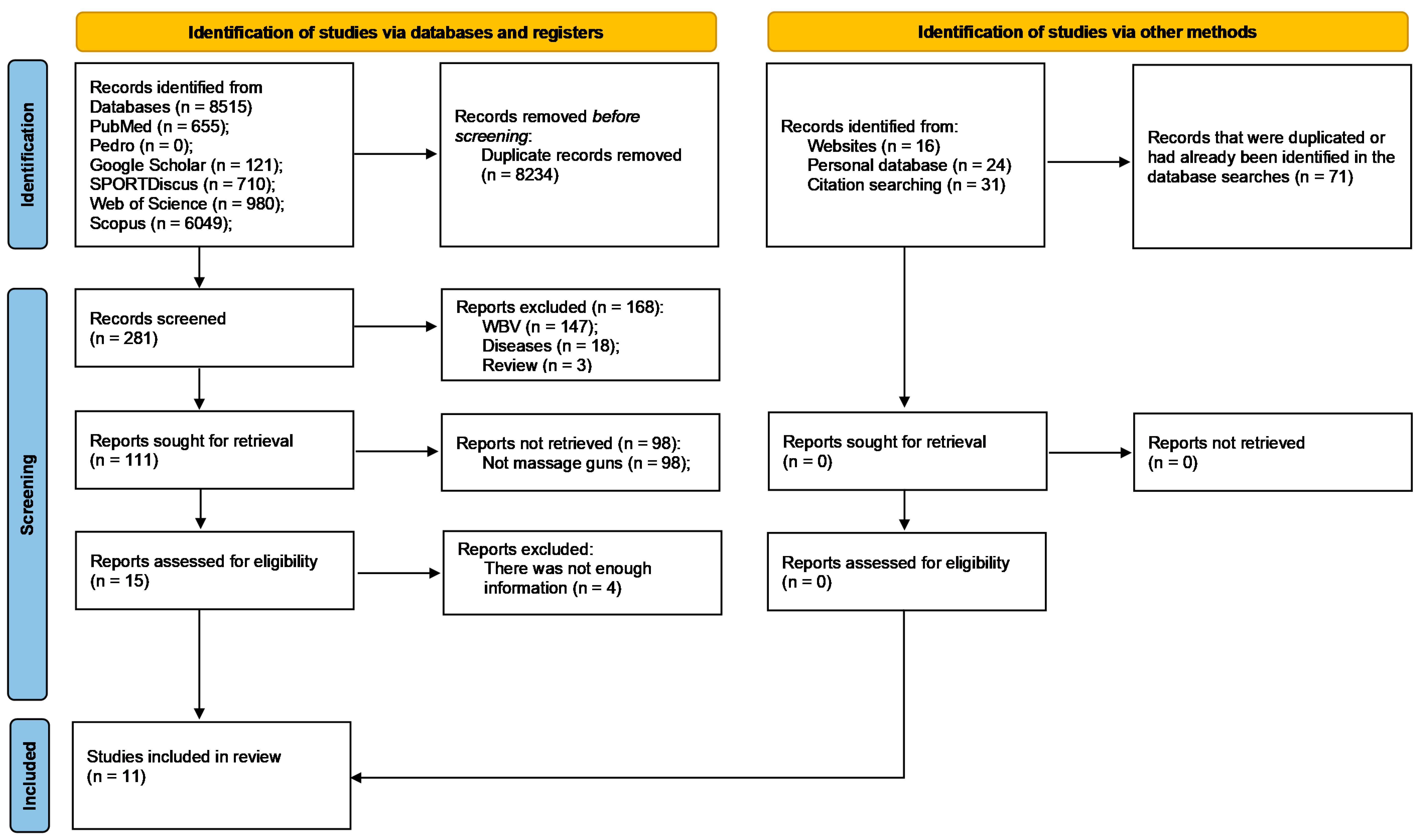
3.1. Studies’ Selection
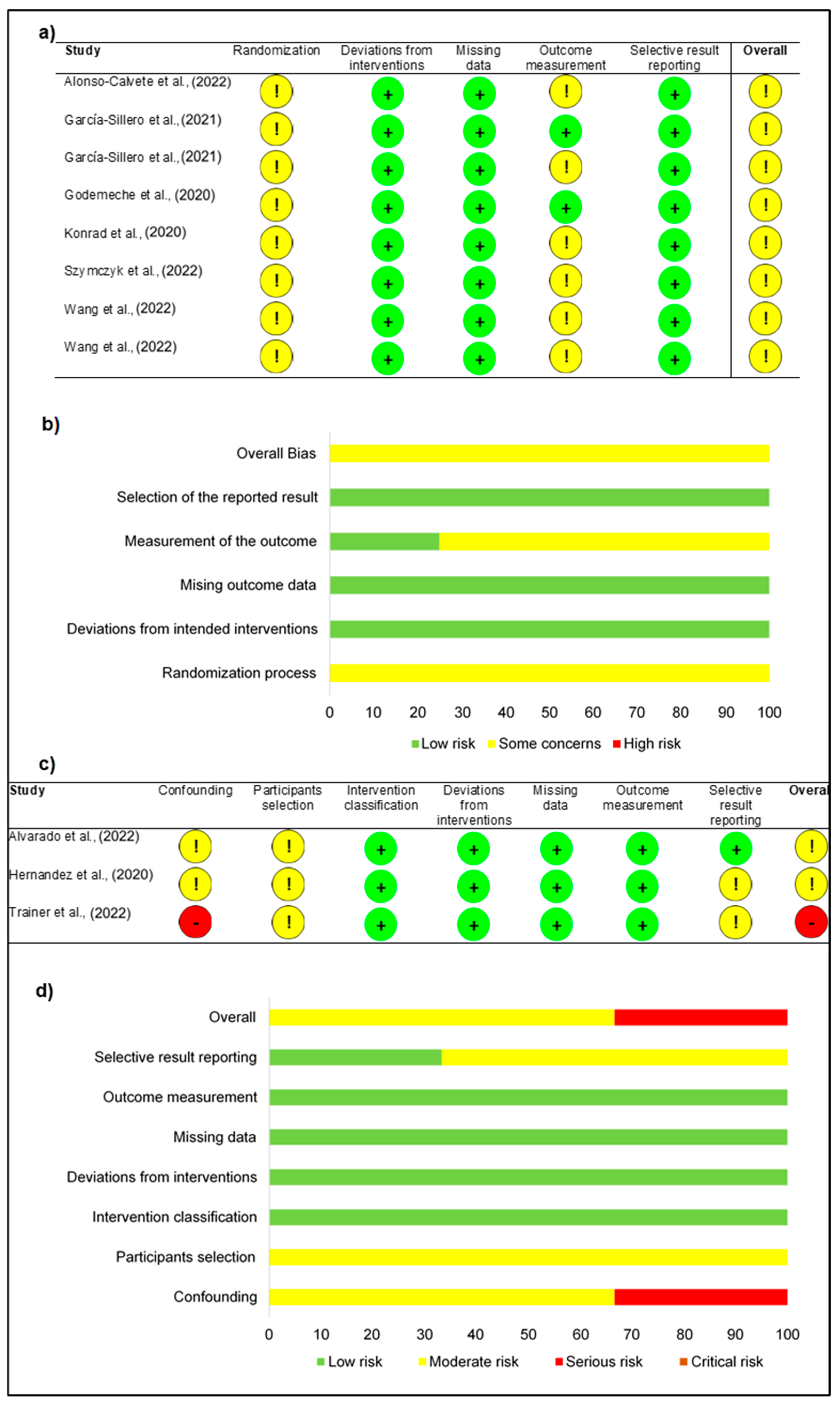
3.2. Risk of Bias
3.3. Studies’ Synthesis
4. Discussion
4.1. Performance
4.2. Recovery
4.3. Physiological Mechanisms
4.3.1. Neuronal
4.3.2. Vascular
4.3.3. Mechanical
4.4. Practical Orientations
4.5. Adverse Effects and Contraindications
5. Limitations and Future Directions
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cochrane, D.J. Good vibrations? The use of vibration therapy for exercise recovery, injury prevention and rehabilitation. Phys. Ther. Rev. 2011, 16, 438–454. [Google Scholar] [CrossRef]
- Swe, M.; Benjamin, B.; Tun, A.A.; Sugathan, S. Role of the whole body vibration machine in the prevention and management of osteoporosis in old age: A systematic review. Malays. J. Med. Sci. 2016, 23, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Reychler, G.; Debier, E.; Contal, O.; Audag, N. Intrapulmonary percussive ventilation as an airway clearance technique in subjects with chronic obstructive airway diseases. Respir. Care 2018, 63, 620–631. [Google Scholar] [CrossRef] [PubMed]
- Rogan, S.; Hilfiker, R.; Schenk, A.; Vogler, A.; Taeymans, J. Effects of whole-body vibration with stochastic resonance on balance in persons with balance disability and falls history—A systematic review. Res. Sports Med. 2014, 22, 294–313. [Google Scholar] [CrossRef] [PubMed]
- Moggio, L.; de Sire, A.; Marotta, N.; Demeco, A.; Ammendolia, A. Vibration therapy role in neurological diseases rehabilitation: An umbrella review of systematic reviews. Disabil. Rehabil. 2022, 44, 5741–5749. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Wang, J.; Duan, K.; Cai, H.; Sun, J. The effect of vibration training on delayed muscle soreness: A meta-analysis. Medicine 2022, 101, e31259. [Google Scholar] [CrossRef]
- Dong, Y.; Wang, W.; Zheng, J.; Chen, S.; Qiao, J.; Wang, X. Whole body vibration exercise for chronic musculoskeletal pain: A systematic review and meta-analysis of randomized controlled trials. Arch. Phys. Med. Rehabil. 2019, 100, 2167–2178. [Google Scholar] [CrossRef]
- Alavinia, S.M.; Omidvar, M.; Craven, B.C. Does whole body vibration therapy assist in reducing fat mass or treating obesity in healthy overweight and obese adults? A systematic review and meta-analyses. Disabil. Rehabil. 2021, 43, 1935–1947. [Google Scholar] [CrossRef]
- Fuller, J.T.; Thomson, R.L.; Howe, P.R.; Buckley, J.D. Effect of vibration on muscle perfusion: A systematic review. Clin. Physiol. Funct. Imaging 2013, 33, 1–10. [Google Scholar] [CrossRef]
- Saquetto, M.; Pereira, F.; Queiroz, R.; Da Silva, C.; Conceição, C.; Gomes Neto, M. Effects of whole-body vibration on muscle strength, bone mineral content and density, and balance and body composition of children and adolescents with Down syndrome: A systematic review. Osteoporos. Int. 2018, 2018, 527–533. [Google Scholar] [CrossRef]
- de Oliveira, R.D.J.; de Oliveira, R.G.; de Oliveira, L.C.; Santos-Filho, S.D.; Sá-Caputo, D.C.; Bernardo-Filho, M. Effectiveness of whole-body vibration on bone mineral density in postmenopausal women: A systematic review and meta-analysis of randomized controlled trials. Osteoporos. Int. 2023, 34, 29–52. [Google Scholar] [CrossRef] [PubMed]
- Zeng, T.; Tiselius, H.-G.; Huang, J.; Deng, T.; Zeng, G.; Wu, W. Effect of mechanical percussion combined with patient position change on the elimination of upper urinary stones/fragments: A systematic review and meta-analysis. Urolithiasis 2020, 2020, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Allan, P.F.; Osborn, E.C.; Chung, K.K.; Wanek, S.M. High-frequency percussive ventilation revisited. J. Burn Care Res. 2010, 31, 510–520. [Google Scholar] [CrossRef]
- Alam, M.M.; Khan, A.A.; Farooq, M. Effect of whole-body vibration on neuromuscular performance: A literature review. Work 2018, 59, 571–583. [Google Scholar] [CrossRef] [PubMed]
- Lauwers, E.; Ides, K.; Van Hoorenbeeck, K.; Verhulst, S. The effect of intrapulmonary percussive ventilation in pediatric patients: A systematic review. Pediatr. Pulmonol. 2018, 53, 1463–1474. [Google Scholar] [CrossRef]
- Cerciello, S.; Rossi, S.; Visonà, E.; Corona, K.; Oliva, F. Clinical applications of vibration therapy in orthopaedic practice. Muscles Ligaments Tendons J. 2016, 6, 147–156. [Google Scholar] [CrossRef]
- Pogwizd, P.; Pasterczyk-Szczurek, A.; Bigosińska, M. Effect of vibrational therapy on muscle tissue. Med. Rehabil. 2018, 22, 11–19. [Google Scholar] [CrossRef]
- Anderson, J.; DeLuca, M.; Haines, M.-E.; Merrick, G. Immediate effects of external vibration vs placebo on vocal function therapy in singers: A randomized clinical trial. JAMA Otolaryngol.-Head Neck Surg. 2018, 144, 187–193. [Google Scholar] [CrossRef]
- Opara, J.A.; Mehlich, K.; Gieremek, K.; Szwejkowski, W. Vibratory massage for complementing training in sports and physiotherapy. Physiother. Fizjoterapia 2010, 18, 61–66. [Google Scholar] [CrossRef]
- Cheatham, S.W.; Baker, R.T.; Behm, D.G.; Stull, K.; Kolber, M.J. Mechanical percussion devices: A survey of practice patterns among healthcare professionals. Int. J. Sports Phys. Ther. 2021, 16, 766–777. [Google Scholar] [CrossRef]
- Goats, G.C. Massage--the scientific basis of an ancient art: Part 1. The techniques. Br. J. Sports Med. 1994, 28, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Comeaux, Z. Dynamic fascial release and the role of mechanical/vibrational assist devices in manual therapies. J. Bodyw. Mov. Ther. 2011, 15, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Osawa, Y.; Oguma, Y.; Ishii, N. The effects of whole-body vibration on muscle strength and power: A meta-analysis. J. Musculoskelet. Neuronal Interact. 2013, 13, 380–390. [Google Scholar]
- Furness, N.D.; Phillips, A.; Gallacher, S.; Beazley, J.C.S.; Evans, J.P.; Toms, A.D.; Thomas, W.; Smith, C.D. Vibration therapy versus standard treatment for tennis elbow: A randomized controlled study. J. Orthop. Surg. 2018, 26, 1–7. [Google Scholar] [CrossRef]
- Cardenas, A.; Gregory, D.E. Can cutaneous vibration affect pain development? Testing the efficacy of a vibrating belt applied intermittently to the low back region during prolonged standing. Int. J. Ind. Ergon. 2018, 66, 95–100. [Google Scholar] [CrossRef]
- Ferreira, R.M.; Martins, P.N.; Goncalves, R.S. Effects of Self-myofascial Release Instruments on Performance and Recovery: An Umbrella Review. Int. J. Exerc. Sci. 2022, 15, 861. [Google Scholar]
- Serritella, E.; Scialanca, G.; Di Giacomo, P.; Di Paolo, C. Local vibratory stimulation for temporomandibular disorder myofascial pain treatment: A randomised, double-blind, placebo-controlled preliminary study. Pain Res. Manag. 2020, 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Fuller, J.T.; Thomson, R.L.; Howe, P.R.; Buckley, J.D. Vibration therapy is no more effective than the standard practice of massage and stretching for promoting recovery from muscle damage after eccentric exercise. Clin. J. Sport Med. 2015, 25, 332–337. [Google Scholar] [CrossRef]
- Germann, D.; El Bouse, A.; Shnier, J.; Abdelkader, N.; Kazemi, M. Effects of local vibration therapy on various performance parameters: A narrative literature review. J. Can. Chiropr. Assoc. 2018, 62, 170–181. [Google Scholar] [PubMed]
- Sackett, D.L.; Rosenberg, W.M.; Gray, J.M.; Haynes, R.B.; Richardson, W.S. Evidence based medicine: What it is and what it isn’t. Br. Med. J. 1996, 312, 71–72. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Br. Med. J. 2021, 372, 1–9. [Google Scholar]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. Br. Med. J. 2019, 366, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. Br. Med. J. 2016, 355, 1–7. [Google Scholar] [CrossRef]
- García-Sillero, M.; Benítez-Porres, J.; García-Romero, J.; Bonilla, D.A.; Petro, J.L.; Vargas-Molina, S. Comparison of interventional strategies to improve recovery after eccentric exercise-induced muscle fatigue. Int. J. Environ. Res. Public Health 2021, 18, 647. [Google Scholar] [CrossRef]
- Konrad, A.; Glashüttner, C.; Reiner, M.M.; Bernsteiner, D.; Tilp, M. The acute effects of a percussive massage treatment with a hypervolt device on plantar flexor muscles’ range of motion and performance. J. Sports Sci. Med. 2020, 19, 690–694. [Google Scholar] [PubMed]
- Wang, F.; Zhang, Z.; Li, C.; Zhu, D.; Hu, Y.; Fu, H.; Zhai, H.; Wang, Y. Acute effects of vibration foam rolling and local vibration during warm-up on athletic performance in tennis players. PLoS ONE 2022, 17, 1–14. [Google Scholar] [CrossRef]
- Hernandez, F.A.; Crussemeyer, J.; Nakajima, M.; Valenzuela, K. Effects of Percussion Therapy (Theragun™) on Range of Motion and Athletic Performance; California State University: Long Beach, CA, USA, 2020. [Google Scholar]
- Alonso-Calvete, A.; Lorenzo-Martínez, M.; Pérez-Ferreirós, A.; Couso-Bruno, A.; Carracedo-Rodríguez, E.; Barcala-Furelos, M.; Barcala-Furelos, R.; Padrón-Cabo, A. Why percussive massage therapy does not improve recovery after a water rescue? A preliminary study with lifeguards. Healthcare 2022, 10, 693. [Google Scholar] [CrossRef] [PubMed]
- García-Sillero, M.; Jurado-Castro, J.M.; Benítez-Porres, J.; Vargas-Molina, S. Acute effects of a percussive massage treatment on movement velocity during resistance training. Int. J. Environ. Res. Public Health 2021, 18, 7726. [Google Scholar] [CrossRef]
- Szymczyk, P.; Węgrzynowicz, K.; Trybulski, R.; Spieszny, M.; Ewertowska, P.; Wilk, M.; Krzysztofik, M. Acute effects of percussive massage treatment on drop jump performance and achilles tendon stiffness. Int. J. Environ. Res. Public Health 2022, 19, 15187. [Google Scholar] [CrossRef] [PubMed]
- Trainer, J.H.; Pascarella, M.; Paul, R.W.; Thomas, S.J. Acute effects of percussive therapy on the posterior shoulder muscles differ based on the athlete’s soreness response. Int. J. Sports Phys. Ther. 2022, 17, 887–895. [Google Scholar] [CrossRef]
- Wang, L.; Fang, M.; Hu, J. The effect of vibration massage on fatigue of the upper trapezius muscle during different tasks. Symmetry 2022, 14, 2158. [Google Scholar] [CrossRef]
- Godemeche, N.; Ribeiro, A.; Amaral, L. Eficácia da Massagem por Vibração Localizada, na Flexibilidade dos Músculos da Cadeia Posterior em Adultos Ativos e Desportistas; Universidade Fernando Pessoa: Porto, Portugal, 2020. [Google Scholar]
- Alvarado, F.; Valenzuela, K.; Finn, A.; Avila, E.L.; Crussemeyer, J.; Nakajima, M. The biomechanical effects of percussive therapy treatment on jump performance. Int. J. Exerc. Sci. 2022, 15, 994–1006. [Google Scholar]
- Davidson, M.J.; Bryant, A.L.; Bower, W.F.; Frawley, H.C. Myotonometry reliably measures muscle stiffness in the thenar and perineal muscles. Physiother. Can. 2017, 69, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Struzik, A.; Karamanidis, K.; Lorimer, A.; Keogh, J.W.; Gajewski, J. Application of leg, vertical, and joint stiffness in running performance: A literature overview. Appl. Bionics Biomech. 2021, 2021, 1–25. [Google Scholar] [CrossRef]
- Wakeling, J.M.; Nigg, B.M.; Rozitis, A.I. Muscle activity damps the soft tissue resonance that occurs in response to pulsed and continuous vibrations. J. Appl. Physiol. 2002, 93, 1093–1103. [Google Scholar] [CrossRef]
- Wakeling, J.M.; Nigg, B.M. Modification of soft tissue vibrations in the leg by muscular activity. J. Appl. Physiol. 2001, 90, 412–420. [Google Scholar] [CrossRef]
- Lupowitz, L. Vibration Therapy–A Clinical Commentary. Int. J. Sports Phys. Ther. 2022, 17, 984–987. [Google Scholar] [CrossRef]
- Imtiyaz, S.; Veqar, Z.; Shareef, M. To compare the effect of vibration therapy and massage in prevention of delayed onset muscle soreness (DOMS). J. Clin. Diagn. Res. 2014, 8, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.M.; Khan, A.A.; Farooq, M. Effects of vibration therapy on neuromuscular efficiency & features of the EMG signal based on endurance test. J. Bodyw. Mov. Ther. 2020, 24, 325–335. [Google Scholar] [PubMed]
- Ghazi, M.; Rippetoe, J.; Chandrashekhar, R.; Wang, H. Focal vibration therapy: Vibration parameters of effective wearable devices. Appl. Sci. 2021, 11, 2969. [Google Scholar] [CrossRef]
- Alghadir, A.; Anwer, S.; Zafar, H.; Iqbal, Z. Effect of localised vibration on muscle strength in healthy adults: A systematic review. Physiotherapy 2018, 104, 18–24. [Google Scholar] [CrossRef]
- Hagbarth, K.-E.; Eklund, G. Tonic vibration reflexes (TVR) in spasticity. Brain Res. 1966, 2, 201–203. [Google Scholar] [CrossRef]
- Delwaide, P.; Oliver, E. Short-latency autogenic inhibition (IB inhibition) in human spasticity. J. Neurol. Neurosurg. Psychiatry 1988, 51, 1546–1550. [Google Scholar] [CrossRef] [PubMed]
- Melzack, R.; Wall, P.D. Pain Mechanisms: A New Theory: A gate control system modulates sensory input from the skin before it evokes pain perception and response. Science 1965, 150, 971–979. [Google Scholar] [CrossRef]
- Ritzmann, R.; Krause, A.; Freyler, K.; Gollhofer, A. Acute whole-body vibration increases reciprocal inhibition. Hum. Mov. Sci. 2018, 60, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Siegmund, L.A.; Barkley, J.E.; Knapp, D.; Peer, K.S. Acute effects of local vibration with biomechanical muscle stimulation on low-back flexibility and perceived stiffness. Athl. Train. Sports Health Care 2014, 6, 37–45. [Google Scholar] [CrossRef]
- Kosar, A.C.; Candow, D.G.; Putland, J.T. Potential beneficial effects of whole-body vibration for muscle recovery after exercise. J. Strength Cond. Res. 2012, 26, 2907–2911. [Google Scholar] [CrossRef] [PubMed]
- Romero Moraleda, B.; González García, J.; Cuéllar Rayo, Á.; Balsalobre Fernández, C.; Muñoz García, D.; Morencos Martínez, E. Effects of vibration and non-vibration foam rolling on recovery after exercise with induced muscle damage. J. Sports Sci. Med. 2019, 18, 172–180. [Google Scholar]
- Cheatham, S.W.; Stull, K.R.; Kolber, M.J. Comparison of a vibration roller and a nonvibration roller intervention on knee range of motion and pressure pain threshold: A randomized controlled trial. J. Sport Rehabil. 2019, 28, 39–45. [Google Scholar] [CrossRef]
- Li, W.; Li, C.; Xu, Q.; Ji, L. Effects of focal vibration over upper limb muscles on the activation of sensorimotor cortex network: An EEG study. J. Healthc. Eng. 2019, 2019, 1–8. [Google Scholar] [CrossRef]
- Murillo, N.; Valls-Sole, J.; Vidal, J.; Opisso, E.; Medina, J.; Kumru, H. Focal vibration in neurorehabilitation. Eur. J. Phys. Rehabil. Med. 2014, 50, 231–242. [Google Scholar] [PubMed]
- Sackner, M.A.; Gummels, E.; Adams, J.A. Nitric oxide is released into circulation with whole-body, periodic acceleration. Chest 2005, 127, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Tzen, Y.-T.; Weinheimer-Haus, E.M.; Corbiere, T.F.; Koh, T.J. Increased skin blood flow during low intensity vibration in human participants: Analysis of control mechanisms using short-time Fourier transform. PLoS ONE 2018, 13, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Mahbub, M.; Hase, R.; Yamaguchi, N.; Hiroshige, K.; Harada, N.; Bhuiyan, A.N.H.; Tanabe, T. Acute effects of whole-body vibration on peripheral blood flow, vibrotactile perception and balance in older adults. Int. J. Environ. Res. Public Health 2020, 17, 1069. [Google Scholar] [CrossRef]
- Lohman III, E.B.; Petrofsky, J.S.; Maloney-Hinds, C.; Betts-Schwab, H.; Thorpe, D. The effect of whole body vibration on lower extremity skin blood flow in normal subjects. Med. Sci. Monit. 2007, 13, 71–76. [Google Scholar]
- Needs, D.; Blotter, J.; Cowan, M.; Fellingham, G.; Johnson, A.W.; Feland, J.B. Effect of localized vibration massage on popliteal blood flow. J. Clin. Med. 2023, 12, 2047. [Google Scholar] [CrossRef]
- Richardson, R.; Mecate, A.C.; Needs, D.; Peterson, A.S.; Adams, T.D.; Merrill, R.M.; Feland, J.B. Massage gun use at a lower frequency does not alter blood flow. In International Journal of Exercise Science: Conference Proceedings; Western Kentucky University: Bowling Green, KY, USA, 2022; p. 75. [Google Scholar]
- Mecate, A.C.; Richardson, R.R.; Needs, D.; Peterson, A.S.; Adams, T.D.; Johnson, A.W.; Merrill, R.M.; Feland, J.B. Effect of Localized Vibration Using Massage Gun at 40hz and 50hz on Blood Flow. In International Journal of Exercise Science: Conference Proceedings; Western Kentucky University: Bowling Green, KY, USA, 2022; p. 55. [Google Scholar]
- Games, K.E.; Sefton, J.M.; Wilson, A.E. Whole-body vibration and blood flow and muscle oxygenation: A meta-analysis. J. Athl. Train. 2015, 50, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Huang, X.; Li, Y.; Sucharit, W.; Sirasaporn, P.; Eungpinichpong, W. Acute effects of percussive massage therapy on thoracolumbar fascia thickness and ultrasound echo intensity in healthy male individuals: A randomized controlled trial. Int. J. Environ. Res. Public Health 2023, 20, 1073. [Google Scholar] [CrossRef] [PubMed]
- Guang, H.; Ji, L.; Shi, Y. Focal vibration stretches muscle fibers by producing muscle waves. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 839–846. [Google Scholar] [CrossRef]
- Chwała, W.; Pogwizd, P. Effects of vibration and passive resting on muscle stiffness and restitution after submaximal exercise analyzed by elastography. Acta Bioeng. Biomech. 2021, 23, 3–11. [Google Scholar] [CrossRef]
- Liang, H.-W.; Wang, T.-G.; Chen, W.-S.; Hou, S.-M. Thinner plantar fascia predicts decreased pain after extracorporeal shock wave therapy. Clin. Orthop. Relat. Res. 2007, 460, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Roehmer, C.; Khan, S.; Sherwood, D. Paracervical Muscle Edema After the Use of High-Percussion Massage Gun. Neuromodulation Technol. Neural Interface 2022, 25, S56. [Google Scholar] [CrossRef]
- Masters, A.; Duarte, R.; Chiang, B.; Sarvottam, K.; Patel, K. Hemothorax After Use of Percussion Massage Gun: A Case Report. In Proceedings of the Case Reports: Pleural Disease Dilemmas; American Thoracic Society: New York, NY, USA, 2022; p. A4172. [Google Scholar]
- Sulkowski, K.; Grant, G.; Brodie, T. Case report: Vertebral artery dissection after use of handheld massage gun. Clin. Pract. Cases Emerg. Med. 2022, 6, 159–161. [Google Scholar] [CrossRef]
- Mu, J.; Fan, W. Lens subluxation after use of a percussion massage gun: A case report. Medicine 2022, 101, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Zhang, F.; Chen, H.; Pan, H. Rhabdomyolysis after the use of percussion massage gun: A case report. Phys. Ther. 2021, 101, pzaa199. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion | Exclusion |
|---|---|
| The studies must: | The studies must not: |
| be randomized and nonrandomized experimental studies | be books, systematic reviews, case reports, expert opinions, observational, interviews or surveys |
| have experimental or control groups with detailed description of the massage guns used methodology | include studies focused only on other devices or hand percussive/vibration interventions |
| include healthy and unhealthy (with acute injuries) individuals | include chronic injuries, illnesses, syndromes or other similar conditions |
| measure outcomes related with performance, injury prevention and health promotion | perform experimental or control groups composed by animals, cadaveric, in vitro or in silico |
| have at least one of the keywords | |
| be published before January 2023 | |
| have their full version |
| Authors (A to Z) | Objectives | Participants’ Characteristics | Cohorts | Outcomes | Results |
|---|---|---|---|---|---|
| Alonso-Calvete et al. [38] | Analyze the effects of percussive massage therapy on lifeguards’ recovery after a water rescue, in comparison with passive recovery | 14 lifeguards
|
|
| There were no differences between percussive therapy and passive recovery in lactate clearance (p > 0.05), finding in both modalities a small but not significant decrease in blood lactate. In perceived fatigue, both methods decreased this variable significantly (p < 0.001), with no significant differences between them (p > 0.05). |
| Alvarado et al. [44] | Assess the effects of percussive therapy treatment on jump performance and passive range of motion | 26 recreationally active college students
|
|
| A significant decrease (p = 0.018–0.008) in peak ankle eversion (2.0° during landing and 2.4° during take-off) was found during the drop jump following the use of percussion therapy. All other frontal/sagittal plane peak joint angle and moment changes were nonsignificant (p > 0.05). Moreover, percussion therapy improved ROM measures: Thomas test (p ≤ 0.001), 90–90 hamstring (p ≤ 0.001), and ankle lunge (p ≤ 0.001). No significance (p > 0.05) was found on the rectus femoris ROM and drop and countermovement jump heights. |
| García-Sillero et al. [34] | Compare the effects of various recovery techniques on muscle tissues after eccentric exercise-induced muscle fatigue | 40 college athletes
|
|
| The application of the different recovery techniques had positive effects for contraction time and radial displacement in the treated leg compared to the untreated leg (F = 50.01, p < 0.01, η2p = 0.58 and F = 27.58, p < 0.01, η2p = 0.43, respectively) and for the interaction of the factors (Time x Leg x Therapy: F = 5.76, p < 0.01, η2p = 0.32 and F = 5.93, p < 0.01, η2p = 0.33, respectively). The results of the various methods used were similar: contraction time (F = 0.17, p = 0.917; η2p = 0.01) and radial displacement (F = 3.30, p = 0.031, η2p = 0.22). |
| García-Sillero et al. [39] | Verify whether the application of percussion therapy during inter-set rest periods increases the number of repetitions during a bench press exercise | 24 university students
|
|
| The percussive therapy performed a greater total number of repetitions compared to control (44.6 ± 4.8 vs. 39.5 ± 6.8; p = 0.047; ES = 0.867). No differences were observed for the different movement velocity, peak power and fatigue variables (p > 0.05). |
| Godemeche et al. [43] | Analyze the effectiveness of vibration massage on the flexibility of posterior chain muscles (lower limbs and lumbar spine) in active and very active | 25 university students
|
|
| Percussive therapy and global postural reeducation showed improvement in the posterior chain flexibility (p < 0.001). When comparing the two techniques, percussive therapy differs from global postural reeducation in the very active group of individuals (p = 0.020). In the active group, the flexibility improvements were similar in both techniques (p = 0.169). Both techniques were superior to the control group (p < 0.000). |
| Hernandez et al. [37] | Access the effects of myofascial release on athletic performance and passive ROM | 20 university students
|
|
| In the strength, kinetic and kinematic measures of the drop and countermovement jumps, no pre-post significant differences were found (p > 0.05). Moreover, percussion therapy improved ROM measures: Thomas test (p ≤ 0.001), 90–90 hamstring (p = 0.001), and ankle lunge (p ≤ 0.001). No significance was found on the rectus femoris ROM (p = 0.399) |
| Konrad et al. [35] | Investigate the effects of a 5 min percussion treatment of the calf muscles on ROM and MVC torque of the plantar flexor muscles | 16 healthy volunteers
|
|
| Maximum dorsiflexion ROM increased with a large magnitude following the massage treatment by 5.4° (+18.4%; p = 0.002; d = 1.36), while there was no change in the control group (+1.6°; +5,3%; p = 0.18; d = 0.51). Moreover, torque did not change following both the percussive therapy and the control groups (p > 0.05). |
| Szymczyk et al. [40] | Investigate the impact of mechanical percussion in the Achilles tendon passive stiffness and kinematics | 11 physically active
|
|
| There were no statistically significant differences in contact time (p = 0.786), reactive strength index (p = 0.914), and relative peak power (p = 0.896). However, statistically significant differences in peak velocity (p = 0.046) and jump height (p = 0.03) were found. Despite that, there were no significant post hoc comparisons for jump height; it slightly decreased 5 min post-percussive therapy (p = 0.136; ES = −0.25; ∆ = −3.1%) compared with the control condition (p = 1.00; ES = 0.11; ∆ = +1.5%). There were no statistically significant differences in dominant (p = 0.073) and nondominant limbs’ (p = 0.091) Achilles tendon stiffness. Although not significant, numerically, the dominant limb Achilles tendon (p = 0.126; ES = −0.64; ∆ = −7.8%) had a larger reduction in stiffness immediately post-percussive therapy compared with the nondominant limb (p = 0.294; ES = −0.26; ∆ = −3.6%). |
| Trainer et al. [41] | Compare the acute effects of percussion therapy on ROM and tissue-specific measures pennation angle and muscle thickness on the dominant arm posterior rotator cuff between individuals responding positively and negatively to percussive therapy | 55 healthy individuals
|
|
| The positive response group had greater improvements than the negative response group in dominant arm internal rotation ROM (2.3° positive vs. −1.3° negative, p = 0.021) and internal rotation strength (1.1 lbs vs. −1.2 lbs, p = 0.011) after percussive therapy. No differences in external rotation strength or ROM were observed between groups (p > 0.05). Regarding muscle architecture, the positive group had a lesser change in teres minor muscle thickness (0.00 mm vs. 0.11 mm, p = 0.019) after percussive therapy. All other muscle architecture changes were not statistically different between groups (p > 0.05). |
| Wang et al., [36] | The effects of 2 different (36 Hz and 46 Hz) percussive therapy levels on upper trapezius muscles under 3 different fatigue conditions | 23 healthy individuals
|
|
| After using the vibration massage at 36 Hz, the MVC percentage of the right upper trapezius showed reductions in the 30 s, the 60 s and the 90 s fatigue task (R1: p = 0.022, R2: p = 0.005, R3: p = 0.049). After using the vibration massage at 46 Hz, the MVC percentage of the right upper trapezius showed a decrease in both the 60 s and the 90 s fatigue task (R2: p = 0.033, R3: p = 0.028). Significant decreases in MVC percentage for the left upper trapezius muscle were found only in the 90 s fatigue task (L3: p = 0.040). |
| Wang et al. [42] | Know if vibration foam rollers and percussion devices have an immediate impact on athletic performance during warm-up | 27 tennis players
|
|
| In the countermovement jump, reactive strength index, and hexagon test, the difference in performance between all interventions was significant (p = 0.007–0.034, η2 = 0.266–0.364). Only those who received vibration foam roller had significantly different countermovement jump and hexagon test results when compared to the control group (53.18 ± 4.49 cm, p = 0.03, d = 1.26; 10.73 ± 0.4 s, p = 0.03, d = 1.12). Participants’ reactive strength index values were significantly different after vibration foam roller (2.01 ± 0.11 cm·mm−1, p = 0.012, d = 1.76) and percussive therapy (1.99 ± 0.11 cm·mm−1, p = 0.025, d = 1.52) compared to the control group. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreira, R.M.; Silva, R.; Vigário, P.; Martins, P.N.; Casanova, F.; Fernandes, R.J.; Sampaio, A.R. The Effects of Massage Guns on Performance and Recovery: A Systematic Review. J. Funct. Morphol. Kinesiol. 2023, 8, 138. https://doi.org/10.3390/jfmk8030138
Ferreira RM, Silva R, Vigário P, Martins PN, Casanova F, Fernandes RJ, Sampaio AR. The Effects of Massage Guns on Performance and Recovery: A Systematic Review. Journal of Functional Morphology and Kinesiology. 2023; 8(3):138. https://doi.org/10.3390/jfmk8030138
Chicago/Turabian StyleFerreira, Ricardo Maia, Rafael Silva, Pedro Vigário, Pedro Nunes Martins, Filipe Casanova, Ricardo Jorge Fernandes, and António Rodrigues Sampaio. 2023. "The Effects of Massage Guns on Performance and Recovery: A Systematic Review" Journal of Functional Morphology and Kinesiology 8, no. 3: 138. https://doi.org/10.3390/jfmk8030138