
Patient-Reported Measures Associated with the Return to Pre-Injury Levels of Sport 2 Years after Anterior Cruciate Ligament Reconstruction

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.3. Return to Sports
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristic
3.2. Return to Sports
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Griffin, L.Y.; Agel, J.; Albohm, M.J.; Arendt, E.A.; Dick, R.W.; Garrett, W.E.; Garrick, J.G.; Hewett, T.E.; Huston, L.; Ireland, M.L.; et al. Noncontact anterior cruciate ligament injuries: Risk factors and prevention strategies. J. Am. Acad. Orthop. Surg. 2000, 8, 141–150. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, G.K.; Axe, M.J.; Snyder-Mackler, L. A decision-making scheme for returning patients to high-level activity with nonoperative treatment after anterior cruciate ligament rupture. Knee Surg. Sport Traumatol. Arthrosc. 2000, 8, 76–82. [Google Scholar] [CrossRef]
- Beynnon, B.D.; Johnson, R.J.; Abate, J.A.; Fleming, B.C.; Nichols, C.E. Treatment of anterior cruciate ligament injuries, part I. Am. J. Sports Med. 2005, 33, 1579–1602. [Google Scholar] [CrossRef]
- Friel, N.A.; Chu, C.R. The Role of ACL Injury in the Development of Posttraumatic Knee Osteoarthritis. Clin. Sports Med. 2013, 32, 1–12. [Google Scholar] [CrossRef]
- Logerstedt, D.; Lynch, A.; Axe, M.J.; Snyder-Mackler, L. Symmetry restoration and functional recovery before and after anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 859–868. [Google Scholar] [CrossRef] [Green Version]
- Lynch, A.D.; Logerstedt, D.S.; Grindem, H.; Eitzen, I.; Hicks, G.; Axe, M.J.; Engebretsen, L.; Risberg, M.A.; Snyder-Mackler, L. Consensus criteria for defining “successful outcome” after ACL injury and reconstruction: A Delaware-Oslo ACL cohort investigation. Br. J. Sports Med. 2015, 49, 335–342. [Google Scholar] [CrossRef]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: An updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br. J. Sports Med. 2014, 48, 1543–1552. [Google Scholar] [CrossRef] [Green Version]
- Webster, K.E.; Feller, J.A. Expectations for Return to Preinjury Sport Before and After Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2019, 47, 578–583. [Google Scholar] [CrossRef]
- van Eck, C.F.; Kropf, E.J.; Romanowski, J.R.; Lesniak, B.P.; Tranovich, M.J.; van Dijk, C.N.; Fu, F.H. Factors that influence the intra-articular rupture pattern of the ACL graft following single-bundle reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 1243–1248. [Google Scholar] [CrossRef] [Green Version]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. A systematic review of the psychological factors associated with returning to sport following injury. Br. J. Sports Med. 2013, 47, 1120–1126. [Google Scholar] [CrossRef]
- Paterno, M.V.; Schmitt, L.C.; Ford, K.R.; Rauh, M.J.; Myer, G.D.; Huang, B.; Hewett, T.E. Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. Am. J. Sports Med. 2010, 38, 1968–1978. [Google Scholar] [CrossRef] [Green Version]
- Nawasreh, Z.; Logerstedt, D.; Cummer, K.; Axe, M.; Risberg, M.A.M.A.; Snyder-Mackler, L. Functional performance 6 months after ACL reconstruction can predict return to participation in the same preinjury activity level 12 and 24 months after surgery. Br. J. Sports Med. 2018, 52, 375. [Google Scholar] [CrossRef]
- Muller, B.; Yabroudi, M.A.; Lynch, A.; Lai, C.-L.; Van Dijk, C.N.; Fu, F.H.; Irrgang, J.J. Defining Thresholds for the Patient Acceptable Symptom State for the IKDC Subjective Knee Form and KOOS for Patients Who Underwent ACL Reconstruction. Am. J. Sports Med. 2016, 1 (Suppl. 4), 9–11. [Google Scholar] [CrossRef] [Green Version]
- Cox, C.L.; Huston, L.J.; Dunn, W.R.; Reinke, E.K.; Nwosu, S.K.; Parker, R.D.; Wright Rick, W.; Kaeding, C.C.; Marx, R.G.; Harrell, F.E.; et al. Are Articular Cartilage Lesions and Meniscus Tears Predictive of IKDC, KOOS, and Marx Activity Level Outcomes After Anterior Cruciate Ligament Reconstruction?: A 6-Year Multicenter Cohort Study. Am. J. Sports Med. 2014, 42, 1058–1067. [Google Scholar] [CrossRef] [Green Version]
- Irrgang, J.J.; Anderson, A.F.; Boland, A.L.; Harner, C.D.; Kurosaka, M.; Neyret, P.; Richmond, J.C.; Shelborne, K.D. Development and validation of the international knee documentation committee subjective knee form. Am. J. Sports Med. 2001, 29, 600–613. [Google Scholar] [CrossRef]
- Roos, E.M.; Roos, H.P.; Lohmander, L.S.; Ekdahl, C.; Beynnon, B.D. Knee Injury and Osteoarthritis Outcome Score (KOOS)--development of a self-administered outcome measure. J. Orthop. Sports Phys. Ther. 1998, 28, 88–96. [Google Scholar] [CrossRef]
- Andriacchi, T.P.; Mündermann, A. The role of ambulatory mechanics in the initiation and progression of knee osteoarthritis. Curr. Opin. Rheumatol. 2006, 18, 514–518. [Google Scholar] [CrossRef]
- Alfadhel, S.A.; Vennu, V.; Alnahdi, A.H.; Omar, M.T.; Alasmari, S.H.; AlJafri, Z.; Bindawas, S.M. Cross-cultural adaptation and validation of the Saudi Arabic version of the Knee Injury and Osteoarthritis Outcome Score (KOOS). Rheumatol. Int. 2018, 38, 1547–1555. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, K.M.; Said, H.G.; Ramadan, E.K.A.; Abd El-Radi, M.; El-Assal, M.A. Arabic translation and validation of three knee scores, Lysholm Knee Score (LKS), Oxford Knee Score (OKS), and International Knee Documentation Committee Subjective Knee Form (IKDC). SICOT-J 2019, 5, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, A.F.; Irrgang, J.J.; Kocher, M.S.; Mann, B.J.; Harrast, J.J. The International Knee Documentation Committee Subjective Knee Evaluation Form: Normative data. Am. J. Sports Med. 2006, 34, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Higgins, L.D.; Taylor, M.K.; Park, D.; Ghodadra, N.; Marchant, M.; Pietrobon, R.; Cook, C. Reliability and validity of the International Knee Documentation Committee (IKDC) Subjective Knee Form. Jt. Bone Spine 2007, 74, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: Oxfordshire, UK; L. Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar] [CrossRef]
- Gignac, G.E.; Szodorai, E.T. Effect size guidelines for individual differences researchers. Pers. Individ. Dif. 2016, 102, 74–78. [Google Scholar] [CrossRef]
- Nawasreh, Z.; Logerstedt, D.; Cummer, K.; Axe, M.J.; Risberg, M.A.; Snyder-Mackler, L. Do Patients Failing Return-to-Activity Criteria at 6 Months After Anterior Cruciate Ligament Reconstruction Continue Demonstrating Deficits at 2 Years ? Am. J. Sports Med. 2016, 45, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kvist, J.; Ek, A.; Sporrstedt, K.; Good, L. Fear of re-injury: A hindrance for returning to sports after anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2005, 13, 393–397. [Google Scholar] [CrossRef]
- Lee, D.Y.H.H.; Karim, S.A.; Chang, H.C. Return to sports after anterior cruciate ligament reconstruction-A review of patients with minimum 5-year follow-up. Ann. Acad. Med. Singapore 2008, 37, 273–278. [Google Scholar] [CrossRef]
- Frobell, R.B.; Roos, H.P.; Roos, E.M.; Roemer, F.W.; Ranstam, J.; Lohmander, L.S. Treatment for acute anterior cruciate ligament tear: Five year outcome of randomised trial. BMJ 2013, 346, f232. [Google Scholar] [CrossRef] [Green Version]
- Zaffagnini, S.; Bruni, D.; Russo, A.; Takazawa, Y.; Presti, M.L.; Giordano, G.; Marcacci, M. ST/G ACL reconstruction: Double strand plus extra-articular sling vs double bundle, randomized study at 3-year follow-up. Scand. J. Med. Sci. Sports 2008, 18, 573–581. [Google Scholar] [CrossRef]
- Daniel, D.M.; Stone MLou Dobson, B.E.; Fithian, D.C.; Rossman, D.J.; Kaufman, K.R. Fate of the ACL-injured patient. A prospective outcome study. Am. J. Sports Med. 1993, 22, 632–644. [Google Scholar] [CrossRef]
- Ardern, C.L.; Österberg, A.; Tagesson, S.; Gauffin, H.; Webster, K.E.; Kvist, J. The impact of psychological readiness to return to sport and recreational activities after anterior cruciate ligament reconstruction. Br. J. Sports Med. 2014, 48, 1613–1619. [Google Scholar] [CrossRef] [Green Version]
- Hamrin Senorski, E.; Svantesson, E.; Beischer, S.; Thomeé, C.; Thomeé, R.; Karlsson, J.; Samuelsson, K. Low 1-Year Return-to-Sport Rate After Anterior Cruciate Ligament Reconstruction Regardless of Patient and Surgical Factors: A Prospective Cohort Study of 272 Patients. Am. J. Sports Med. 2018, 46, 1551–1558. [Google Scholar] [CrossRef]
- Meredith, S.J.; Rauer, T.; Chmielewski, T.L.; Fink, C.; Diermeier, T.; Rothrauff, B.B.; Svantesson, E.; Senorski, E.H.; Hewett, T.E.; Wilk, K.; et al. Return to sport after anterior cruciate ligament injury: Panther Symposium ACL Injury Return to Sport Consensus Group. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 2403–2414. [Google Scholar] [CrossRef] [PubMed]
- Mardani-Kivi, M.; Azari, Z.; Hasannejad, F. Return to sport activity after anterior cruciate ligament reconstruction: A 6–10 years follow-up. J. Clin. Orthop. Trauma. 2020, 11, S319–S325. [Google Scholar] [CrossRef] [PubMed]
- Dunn, W.R.; Spindler, K.P.; Consortium, M. Predictors of activity level 2 years after anterior cruciate ligament reconstruction (ACLR): A multicenter orthopaedic outcomes network (MOON) ACLR cohort study. Am. J. Sports Med. 2010, 38, 2040–2050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mardani-Kivi, M.; Leili, E.K.; Shirangi, A.; Azari, Z. Return to sports activity in the revision of anterior cruciate ligament reconstruction: A 2–6 Year follow-up study. J. Clin. Orthop. Trauma. 2021, 16, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.-H.; Fan, C.-H.; Yu, P.-A.; Chen, C.-L.; Kuo, L.-T.; Hsu, R.W.-W. Effect of high body mass index on knee muscle strength and function after anterior cruciate ligament reconstruction using hamstring tendon autografts. BMC Musculoskelet. Disord. 2018, 19, 363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derraik, J.G.B.; de Bock, M.; Hofman, P.L.; Cutfield, W.S. Increasing BMI is associated with a progressive reduction in physical quality of life among overweight middle-aged men. Sci. Rep. 2014, 4, 3677. [Google Scholar] [CrossRef] [Green Version]
- Giuli, C.; Papa, R.; Bevilacqua, R.; Felici, E.; Gagliardi, C.; Marcellini, F.; Boscaro, M.; De Robertis, M.; Mocchegiani, E.; Tirabassi, G.; et al. Correlates of perceived health related quality of life in obese, overweight and normal weight older adults: An observational study. BMC Public Health 2014, 14, 35. [Google Scholar] [CrossRef]
- Shelbourne, K.D.; Benner, R.W.; Gray, T. Return to Sports and Subsequent Injury Rates After Revision Anterior Cruciate Ligament Reconstruction with Patellar Tendon Autograft. Am. J. Sports Med. 2014, 42, 1395–1400. [Google Scholar] [CrossRef]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Whitehead, T.S.; Webster, K.E. Psychological responses matter in returning to preinjury level of sport after anterior cruciate ligament reconstruction surgery. Am. J. Sports Med. 2013, 41, 1549–1558. [Google Scholar] [CrossRef]
- Webster, K.E.; Feller, J.A. Who passes return-to-sport tests, and which tests are most strongly associated with return to play after anterior cruciate ligament reconstruction? Orthop. J. Sport Med. 2020, 8, 2325967120969425. [Google Scholar] [CrossRef]
- Webster, K.E.; Feller, J.A. Return to Level I Sports After Anterior Cruciate Ligament Reconstruction: Evaluation of Age, Sex, and Readiness to Return Criteria. Orthop. J. Sport Med. 2018, 6, 2325967118788045. [Google Scholar] [CrossRef] [Green Version]
- Logerstedt, D.; Di Stasi, S.; Grindem, H.; Lynch, A.; Eitzen, I.; Engebretsen, L.; Risberg, M.A.; Axe, M.J.; Snyder-Mackler, L. Self-Reported Knee Function Can Identify Athletes Who Fail Return-to-Activity Criteria up to 1 Year After Anterior Cruciate Ligament Reconstruction: A Delaware-Oslo ACL Cohort Study. J. Orthop. Sports Phys. Ther. 2014, 44, 914–923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filbay, S.R.; Ackerman, I.N.; Russell, T.G.; Crossley, K.M. Return to sport matters—Longer-term quality of life after ACL reconstruction in people with knee difficulties. Scand. J. Med. Sci. Sports 2017, 27, 514–524. [Google Scholar] [CrossRef]
- Anand, B.S.; Feller, J.A.; Richmond, A.K.; Webster, K.E. Return-to-Sport Outcomes After Revision Anterior Cruciate Ligament Reconstruction Surgery. Am. J. Sports Med. 2016, 44, 580–584. [Google Scholar] [CrossRef] [PubMed]
- van Meer, B.L.; Meuffels, D.E.; Vissers, M.M.; Bierma-Zeinstra, S.M.; Verhaar, J.A.; Terwee, C.B.; Reijman, M. Knee Injury and Osteoarthritis Outcome Score or International Knee Documentation Committee Subjective Knee Form: Which Questionnaire Is Most Useful to Monitor Patients With an Anterior Cruciate Ligament Rupture in the Short Term? Arthroscopy. 2013, 29, 701–715. [Google Scholar] [CrossRef] [PubMed]
- Flanigan, D.C.; Everhart, J.S.; Pedroza, A.; Smith, T.; Kaeding, C.C. Fear of reinjury (Kinesiophobia) and persistent knee symptoms are common factors for lack of return to sport after anterior cruciate ligament reconstruction. Arthrosc.-J. Arthrosc. Relat. Surg. 2013, 29, 1322–1329. [Google Scholar] [CrossRef]
- Andrade AndrLLDe Sardeli, A.V.; Livani, B.; Belangero, W.D. Determinants of Return to Play After Anterior Cruciate Ligament Reconstruction. Acta Ortop. Bras. 2020, 28, 303–310. [Google Scholar] [CrossRef]
- Lepley, A.S.; Pietrosimone, B.; Cormier, M.L. Quadriceps function, knee pain, and self-reported outcomes in patients with anterior cruciate ligament reconstruction. J. Athl. Train. 2018, 53, 337–346. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Did Not Return to Any Sports (n = 11) | Returned to Any Sport (n = 29) | p-Value (95%CI) | |
|---|---|---|---|
| Age | 28.36 (5.33) | 25.54 (4.42) | 0.113 (−6.35–0.70) |
| BMI | 26.71 (2.97) | 24.54 (2.47) | 0.026 (−4.05–−0.30) * |
| Time from injury to surgery (month) | 23.50 (6.26) | 13.19 (2.70) | 0.084 (−22.10–1.47) |
| Time from surgery to study participation (month) | 26.64 (4.63) | 25.89 (5.65) | 0.701 (−4.63–3.14) |
| Meniscus injury (Yes/No) | (6/5) | (11/17) | 0.022 |
| KOOS-pain score | 85.86 (13.52) | 88.29 (17.38) | 0.679 (−14.28–9.41) |
| KOOS-symptoms | 57.47 (14.76) | 64.67 (14.13) | 0.166 (−17.51–3.11) |
| KOOS-ADLs | 91.44 (10.82) | 92.33 (14.66) | 0.857 (−10.79–9.01) |
| KOOS-Sport/Rec score | 75.00 (21.45) | 82.14 (22.09) | 0.366 (−22.94–8.66) |
| KOOS-QOL score | 41.47 (27.43) | 57.81 (24.63) | 0.079 (−34.65–1.99) |
| IKDC2000 score | 71.20 (16.53) | 83.21 (16.78) | 0.051 (−24.40–0.37) |
| Return to Any Sport | Return to the Same Pre-Injury Sport Levels | |
|---|---|---|
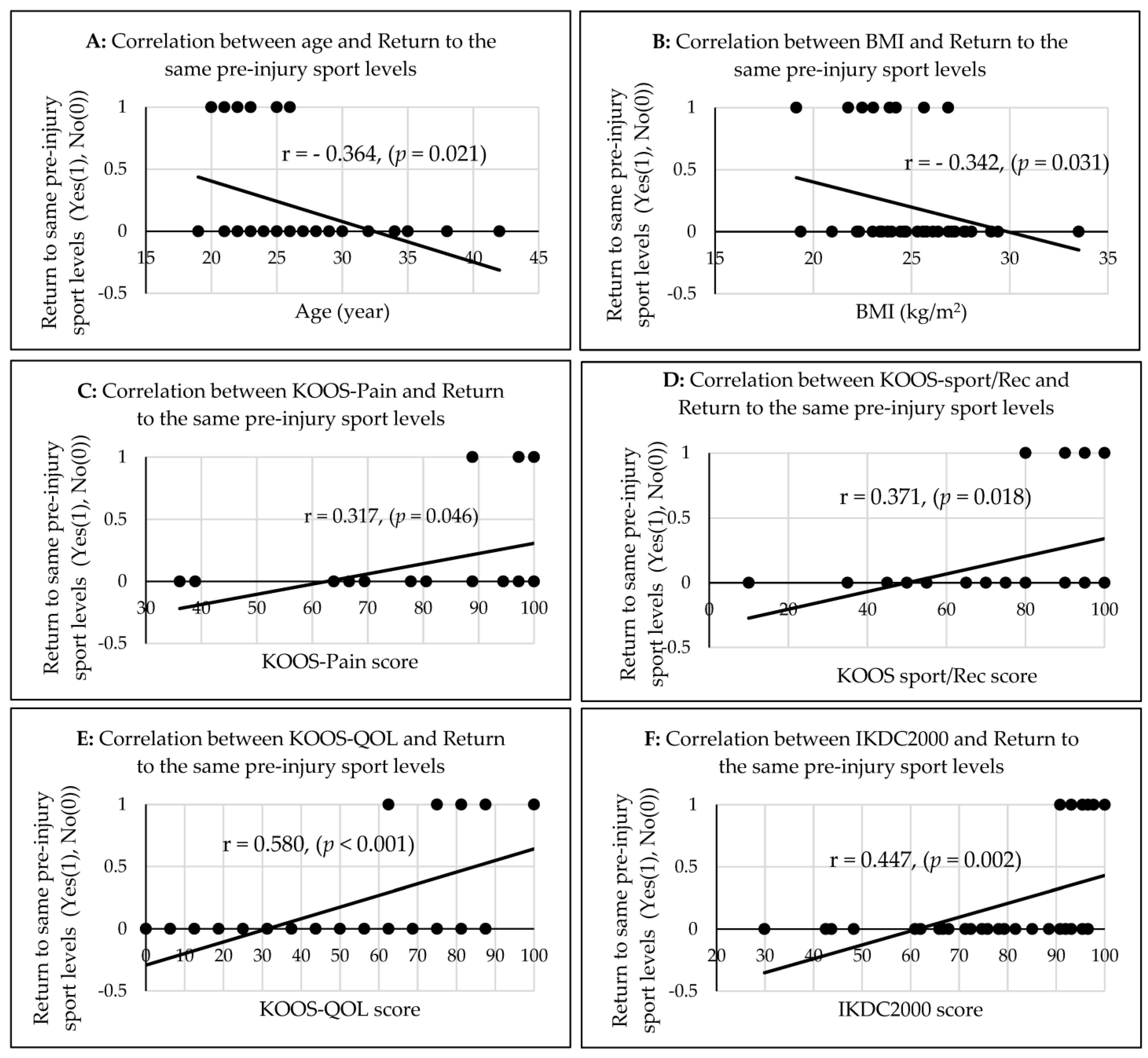
| Age | (r = −0.221 (p = 0.171)) | (r = −0.364 (p = 0.021)) * |
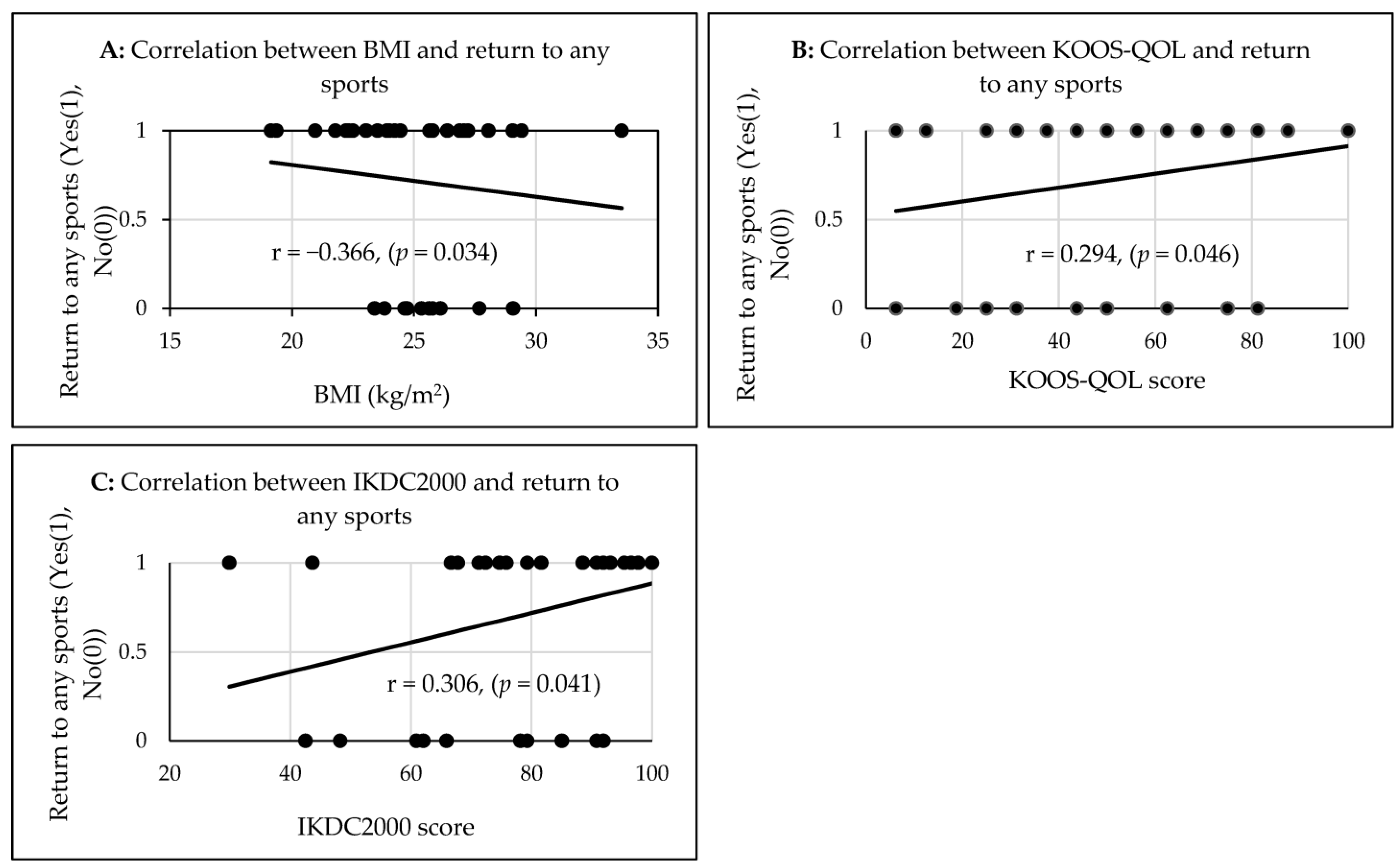
| BMI | (r = −0.366 (p = 0.034)) * | (r = −0.342 (p = 0.031)) * |
| KOOS-Pain score | (r = 0.077 (p = 0.638)) | (r = 0.317 (p = 0.046)) * |
| KOOS-Symptoms | (r = 0.178 (p = 0.273)) | (r = 0.217 (p = 0.178)) |
| KOOS ADLs | (r = 0.025 (p = 0.879)) | (r = 0.268 (p = 0.094)) |
| KOOS-Sport/Rec score | (r = 0.132 (p = 0.416)) | (r = 0.371 (p = 0.018)) * |
| KOOS-QOL score | (r = 0.294 (p = 0.046)) * | (r = 0.580 (p < 0.001)) * |
| IKDC2000 score | (r = 0.306 (p = 0.041)) * | (r = 0.447 (p = 0.002)) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nawasreh, Z.H.; Yabroudi, M.A.; Al-Shdifat, A.B.; Obaidat, S.M.; Daradkeh, S.M.; Kassas, M.N.; Bashaireh, K.M. Patient-Reported Measures Associated with the Return to Pre-Injury Levels of Sport 2 Years after Anterior Cruciate Ligament Reconstruction. J. Funct. Morphol. Kinesiol. 2023, 8, 28. https://doi.org/10.3390/jfmk8010028
Nawasreh ZH, Yabroudi MA, Al-Shdifat AB, Obaidat SM, Daradkeh SM, Kassas MN, Bashaireh KM. Patient-Reported Measures Associated with the Return to Pre-Injury Levels of Sport 2 Years after Anterior Cruciate Ligament Reconstruction. Journal of Functional Morphology and Kinesiology. 2023; 8(1):28. https://doi.org/10.3390/jfmk8010028
Chicago/Turabian StyleNawasreh, Zakariya H., Mohammad A. Yabroudi, Anan B. Al-Shdifat, Sakher M. Obaidat, Sharf M. Daradkeh, Mohamed N. Kassas, and Khaldoon M. Bashaireh. 2023. "Patient-Reported Measures Associated with the Return to Pre-Injury Levels of Sport 2 Years after Anterior Cruciate Ligament Reconstruction" Journal of Functional Morphology and Kinesiology 8, no. 1: 28. https://doi.org/10.3390/jfmk8010028