

Barriers to Gait Training among Stroke Survivors: An Integrative Review
 and
and 
Abstract
:1. Introduction
2. Methods
2.1. Design
2.2. Search Methods
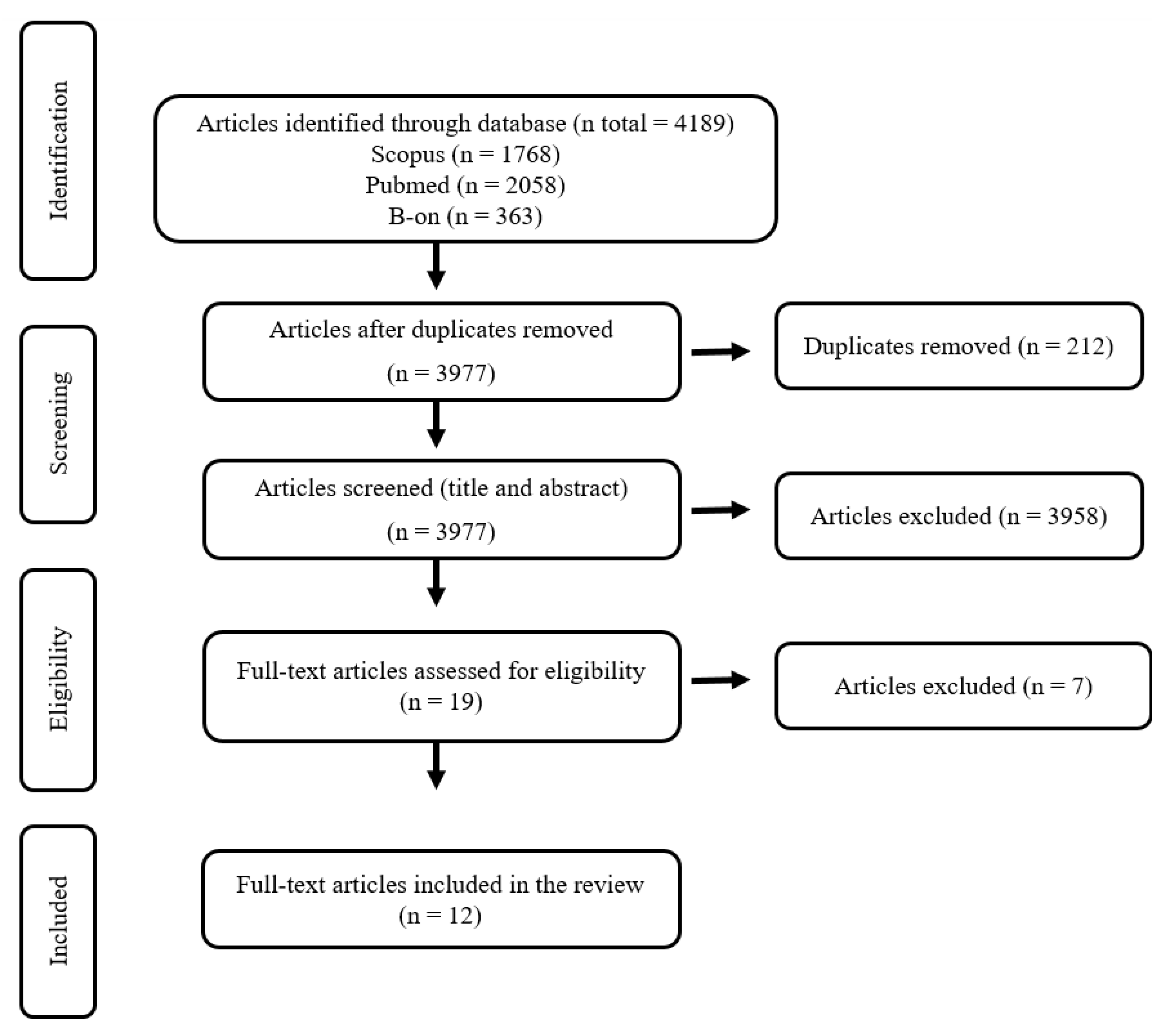
2.3. Study Selection
2.4. Data Evaluation
2.5. Data Analysis
3. Results
3.1. Category 1: Individual Barriers
3.2. Category 2: Environmental Barriers
3.3. Category 3: Rehabilitation Workforce Barriers
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/stroke/about.htm#:~:text=A%20stroke%2C%20sometimes%20called%20a,term%20disability%2C%20or%20even%20death (accessed on 20 August 2022).
- World Stroke Organization. Global Stroke Fact Sheet 2022. Available online: https://www.world-stroke.org/assets/downloads/WSO_Global_Stroke_Fact_Sheet.pdf (accessed on 26 August 2022).
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; de Ferranti, S.; Després, J.P.; Fullerton, H.J.; Howard, V.J.; et al. Heart disease and stroke statistics--2015 update: A report from the American Heart Association. Circulation 2015, 131, e29–e322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flach, C.; Muruet, W.; Wolfe, C.; Bhalla, A.; Douiri, A. Risk and Secondary Prevention of Stroke Recurrence: A Population-Base Cohort Study. Stroke 2020, 51, 2435–2444. [Google Scholar] [CrossRef]
- Stahmeyer, J.T.; Stubenrauch, S.; Geyer, S.; Weissenborn, K.; Eberhard, S. The Frequency and Timing of Recurrent Stroke: An Analysis of Routine Health Insurance Data. Dtsch. Arztebl. Int. 2019, 116, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Béjot, Y.; Bailly, H.; Durier, J.; Giroud, M. Epidemiology of stroke in Europe and trends for the 21st century. Presse Med. 2016, 45 Pt 2, e391–e398. [Google Scholar] [CrossRef]
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Global Burden of Stroke. Circ. Res. 2017, 120, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Schwamm, L.H.; Pancioli, A.; Acker, J.E.; Goldstein, L.B.; Zorowitz, R.D.; Shephard, T.J.; Moyer, P.; Gorman, M.; Johnston, S.C.; Duncan, P.W.; et al. Recommendations for the establishment of stroke systems of care: Recommendations from the American Stroke Association’s Task Force on the Development of Stroke Systems. Stroke 2005, 36, 690–703. [Google Scholar] [CrossRef] [PubMed]
- Wasti, S.A.; Surya, N.; Stephan, K.M.; Owolabi, M. Healthcare Settings for Rehabilitation After Stroke. In Clinical Pathways in Stroke Rehabilitation; Platz, T., Ed.; Springer: Cham, Switzerland, 2021. [Google Scholar] [CrossRef]
- Platz, T. Evidence-Based Guidelines and Clinical Pathways in Stroke Rehabilitation-An International Perspective. Front. Neurol. 2019, 10, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van de Port, I.G.; Kwakkel, G.; Lindeman, E. Community ambulation in patients with chronic stroke: How is it related to gait speed? J. Rehabil. Med. 2008, 40, 23–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKevitt, C.; Fudge, N.; Redfern, J.; Sheldenkar, A.; Crichton, S.; Rudd, A.R.; Forster, A.; Young, J.; Nazareth, I.; Silver, L.E.; et al. Self-reported long-term needs after stroke. Stroke 2011, 42, 1398–1403. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001.
- Fritz, S.; Lusardi, M. White paper: “walking speed: The sixth vital sign”. J. Geriatr. Phys. Ther. 2009, 32, 46–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jette, D.U.; Latham, N.K.; Smout, R.J.; Gassaway, J.; Slavin, M.D.; Horn, S.D. Physical therapy interventions for patients with stroke in inpatient rehabilitation facilities. Phys. Ther. 2005, 85, 238–248. [Google Scholar] [CrossRef] [Green Version]
- Cirstea, C.M. Gait Rehabilitation After Stroke: Should We Re-Evaluate Our Practice? Stroke 2020, 51, 2892–2894. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Methods and Data Sources for Life Tables 1990–2019; World Health Organization: Geneva, Switzerland, 2020.
- Nilsen, P.; Seing, I.; Ericsson, C.; Birken, S.A.; Schildmeijer, K. Characteristics of successful changes in health care organizations: An interview study with physicians, registered nurses and assistant nurses. BMC Health Serv. Res. 2020, 20, 147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horntvedt, M.T.; Nordsteien, A.; Fermann, T.; Severinsson, E. Strategies for teaching evidence-based practice in nursing education: A thematic literature review. BMC Med. Educ. 2018, 18, 172. [Google Scholar] [CrossRef]
- Westerlund, A.; Sundberg, L.; Nilsen, P. Implementation of Implementation Science Knowledge: The Research-Practice Gap Paradox. Worldviews Evid.-Based Nurs. 2019, 16, 332–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, J.B.; Fernandes, S.B.; Almeida, A.S.; Cunningham, R.C. Barriers to Family Resilience in Caregivers of People Who Have Schizophrenia. J. Nurs. Sch. 2021, 53, 393–399. [Google Scholar] [CrossRef]
- Fernandes, J.B.; Fernandes, S.B.; Almeida, A.S.; Vareta, D.A.; Miller, C.A. Older Adults’ Perceived Barriers to Participation in a Falls Prevention Strategy. J. Pers. Med. 2021, 11, 450. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, J.B.; Vareta, D.; Fernandes, S.; Almeida, A.S.; Peças, D.; Ferreira, N.; Roldão, L. Rehabilitation Workforce Challenges to Implement Person-Centered Care. Int. J. Environ. Res. Public Health 2022, 19, 3199. [Google Scholar] [CrossRef]
- Domingos, J.; Dean, J.; Fernandes, J.B.; Godinho, C. Professionals’ Self-Reported Difficulties towards Integrating Dual Task Training in Care for People with Parkinson’s Disease. Int. J. Environ. Res. Public Health. 2022, 19, 1281. [Google Scholar] [CrossRef] [PubMed]
- Hammel, J.; Jones, R.; Gossett, A.; Morgan, E. Examining barriers and supports to community living and participation after a stroke from a participatory action research approach. Top. Stroke Rehabil. 2006, 13, 43–58. [Google Scholar] [CrossRef] [PubMed]
- Simpson, L.A.; Eng, J.J.; Tawashy, A.E. Exercise perceptions among people with stroke: Barriers and facilitators to participation. Int. J. Ther. Rehabil. 2011, 18, 520–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, J.B.; Fernandes, S.; Almeida, A.; Almeida, J.M.; Peças, D. Factors associated with non-compliance to walking aids in older adults at high risk of falling. Cult. Cuid. 2022, 26, 191–205. [Google Scholar] [CrossRef]
- Domingos, J.; Dean, J.; Cruickshank, T.M.; Śmiłowska, K.; Fernandes, J.B.; Godinho, C. A Novel Boot Camp Program to Help Guide Personalized Exercise in People with Parkinson Disease. J. Pers. Med. 2021, 11, 938. [Google Scholar] [CrossRef] [PubMed]
- Boysen, G.; Krarup, L.H.; Zeng, X.; Oskedra, A.; Kõrv, J.; Andersen, G.; Gluud, C.; Pedersen, A.; Lindahl, M.; Hansen, L.; et al. ExStroke Pilot Trial of the effect of repeated instructions to improve physical activity after ischaemic stroke: A multinational randomised controlled clinical trial. BMJ 2009, 339, b2810. [Google Scholar] [CrossRef] [Green Version]
- Adeoye, O.; Nyström, K.V.; Yavagal, D.R.; Luciano, J.; Nogueira, R.G.; Zorowitz, R.D.; Khalessi, A.A.; Bushnell, C.; Barsan, W.G.; Panagos, P.; et al. Recommendations for the Establishment of Stroke Systems of Care: A 2019 Update. Stroke 2019, 50, e187–e210. [Google Scholar] [CrossRef]
- Rimmer, J.H.; Wang, E.; Smith, D. Barriers associated with exercise and community access for individuals with stroke. J. Rehabil. Res. Dev. 2008, 45, 315–322. [Google Scholar] [CrossRef]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Damush, T.M.; Plue, L.; Bakas, T.; Schmid, A.; Williams, L.S. Barriers and facilitators to exercise among stroke survivors. Rehabil. Nurs. 2007, 32, 253–262. [Google Scholar] [CrossRef]
- Zalewski, K.R.; Dvorak, L. Barriers to physical activity between adults with stroke and their care partners. Top. Stroke Rehabil. 2011, 18 (Suppl. 1), 666–675. [Google Scholar] [CrossRef]
- Jurkiewicz, M.T.; Marzolini, S.; Oh, P. Adherence to a home-based exercise program for individuals after stroke. Top. Stroke Rehabil. 2011, 18, 277–284. [Google Scholar] [CrossRef]
- Nicholson, S.; Sniehotta, F.F.; van Wijck, F.; Greig, C.A.; Johnston, M.; McMurdo, M.E.; Dennis, M.; Mead, G.E. A systematic review of perceived barriers and motivators to physical activity after stroke. Int. J. Stroke 2013, 8, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, S.L.; Greig, C.A.; Sniehotta, F.; Johnston, M.; Lewis, S.J.; McMurdo, M.E.; Johnston, D.; Scopes, J.; Mead, G.E. Quantitative data analysis of perceived barriers and motivators to physical activity in stroke survivors. J. R. Coll. Physicians Edinb. 2017, 47, 231–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goffredo, M.; Infarinato, F.; Pournajaf, S.; Romano, P.; Ottaviani, M.; Pellicciari, L.; Galafate, D.; Gabbani, D.; Gison, A.; Franceschini, M. Barriers to sEMG Assessment During Overground Robot-Assisted Gait Training in Subacute Stroke Patients. Front. Neurol. 2020, 11, 564067. [Google Scholar] [CrossRef] [PubMed]
- Tole, G.; Raymond, M.J.; Williams, G.; Clark, R.A.; Holland, A.E. Strength training to improve walking after stroke: How physiotherapist, patient and workplace factors influence exercise prescription. Physiother. Theory Pract. 2022, 38, 1198–1206. [Google Scholar] [CrossRef] [PubMed]
- Débora Pacheco, B.; Guimarães Caetano, L.C.; Amorim Samora, G.; Sant’Ana, R.; Fuscaldi Teixeira-Salmela, L.; Scianni, A.A. Perceived barriers to exercise reported by individuals with stroke, who are able to walk in the community. Disabil. Rehabil. 2021, 43, 331–337. [Google Scholar] [CrossRef]
- de Rooij, I.; van de Port, I.; van der Heijden, L.; Meijer, J.G.; Visser-Meily, J. Perceived barriers and facilitators for gait-related participation in people after stroke: From a patients’ perspective. Physiother. Theory Pract. 2021, 37, 1337–1345. [Google Scholar] [CrossRef] [Green Version]
- Tang, E.; Price, C.; Stephan, B.; Robinson, L.; Exley, C. Gaps in care for patients with memory deficits after stroke: Views of healthcare providers. BMC Health Serv. Res. 2017, 17, 634. [Google Scholar] [CrossRef] [Green Version]
- Guzik, A.; Bushnell, C. Stroke Epidemiology and Risk Factor Management. Continuum 2017, 23, 15–39. [Google Scholar] [CrossRef]
- Oyake, K.; Suzuki, M.; Otaka, Y.; Tanaka, S. Motivational Strategies for Stroke Rehabilitation: A Descriptive Cross-Sectional Study. Front. Neurol. 2020, 11, 553. [Google Scholar] [CrossRef]
- Cheong, M.J.; Kang, Y.; Kang, H.W. Psychosocial Factors Related to Stroke Patients’ Rehabilitation Motivation: A Scoping Review and Meta-Analysis Focused on South Korea. Healthcare 2021, 9, 1211. [Google Scholar] [CrossRef]
- Walker, M.F.; Sunnerhagen, K.S.; Fisher, R.J. Evidence-based community stroke rehabilitation. Stroke 2013, 44, 293–297. [Google Scholar] [CrossRef] [Green Version]
- Ontario Health (Quality). Continual Long-Term Physiotherapy After Stroke: A Health Technology Assessment. Ont. Health Technol. Assess. Ser. 2020, 20, 1–70. [Google Scholar]
- Marotta, N.; Ammendolia, A.; Marinaro, C.; Demeco, A.; Moggio, L.; Costantino, C. International Classification of Functioning, Disability and Health (ICF) and correlation between disability and finance assets in chronic stroke patients. Acta Biomed. 2020, 91, e2020064. [Google Scholar] [CrossRef] [PubMed]
- Horton, K.; Dickinson, A. The role of culture and diversity in the prevention of falls among older Chinese people. Can. J. Aging 2011, 30, 57–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creasy, K.R.; Lutz, B.J.; Young, M.E.; Stacciarini, J.M. Clinical Implications of Family-Centered Care in Stroke Rehabilitation. Rehabil. Nurs. 2015, 40, 349–359. [Google Scholar] [CrossRef] [Green Version]
- Nayeri, N.; Mohammadi, S.; Razi, S.; Kazemnejad, A. Investigating the effects of a family-centered care program on stroke patients’ adherence to their therapeutic regimens. Contemp. Nurse 2014, 47, 88–96. [Google Scholar] [CrossRef]
- World Health Organization. World Report on Disability; World Health Organization: Geneva, Switzerland, 2011.
- Saadi, A.; Okeng’o, K.; Biseko, M.R.; Shayo, A.F.; Mmbando, T.N.; Grundy, S.J.; Xu, A.; Parker, R.A.; Wibecan, L.; Iyer, G.; et al. Post-stroke social networks, depressive symptoms, and disability in Tanzania: A prospective study. Int. J. Stroke 2018, 13, 840–848. [Google Scholar] [CrossRef]
- World Health Organization. Framework on Integrated, People-Centred Health Services. Sixty-Ninth World Health Assembly A69/39 Item 16.1.2016. Available online: http://apps.who.int/gb/ebwha/pdf_files/WHA69/A69_39-en.pdf?ua=1&ua=1 (accessed on 1 June 2022).
- Ventura, F.; Costeira, C.R.B.; Silva, R.; Cardoso, D.; Oliveira, C. Person-Centered Practice in the Portuguese Healthcare Services: A Scoping Review Protocol. Nurs. Rep. 2022, 12, 24. [Google Scholar] [CrossRef]
- Cordon, C.P.; Baxter, P.; Collerman, A.; Krull, K.; Aiello, C.; Lounsbury, J.; MacPhee, M.; Udod, S.; Alvarado, K.; Dietrich, T.; et al. Implementing the Synergy Model: A Qualitative Descriptive Study. Nurs. Rep. 2022, 12, 11. [Google Scholar] [CrossRef]
- Siddiqi, K.; Newell, J.; Robinson, M. Getting evidence into practice: What works in developing countries? Int. J. Qual. Health Care 2005, 17, 447–454. [Google Scholar] [CrossRef]
- Picha, K.J.; Howell, D.M. A model to increase rehabilitation adherence to home exercise programmes in patients with varying levels of self-efficacy. Musculoskelet. Care 2018, 16, 233–237. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author/Year/Title/Country | Study Design/Aim | Categories and Subcategories of Barriers Identified per Study |
|---|---|---|
| Hammel, Jones, Gossett, and Morgan [25] (2006) Examining barriers and supports to community living and participation after a stroke from a participatory action research approach United States of America | Qualitative descriptive study To identify barriers to full participation and exmanie action-planning strategies to address these barriers within community settings and businesses and to implement policy and system changes to effect participation opportunities at the broader societal level. |
|
| Damush, Plue, Bakas, Schmid, and Williams [33] (2007) Barriers and facilitators to exercise among stroke survivors United States of America | Qualitative descriptive study To elicit barriers to and facilitators of exercise after stroke. |
|
| Rimmer, Wang, and Smith [31] (2008) Barriers associated with exercise and community access for individuals with stroke United States of America | Cross-sectional study To examine the multidimensional nature of barriers to physical activity reported by people who suffered stroke. |
|
| Zalewski and Dvorak [34] (2011) Barriers to physical activity between adults with stroke and their care partners United States of America | Cross-sectional study To describe the daily physical activity patterns and perceived barriers to increasing physical activity for adults who have completed their rehabilitation after stroke and for their primary care partners. |
|
| Jurkiewicz, Marzolini, and Oh [35] (2011) Adherence to a home-based exercise program for individuals after stroke Canada | Cross-sectional study To retrospectively identify factors that affect adherence to a home-based exercise program adapted for stroke patients. |
|
| Simpson, Eng, and Tawashy [26] (2011) Exercise perceptions among people with stroke: Barriers and facilitators to participation Canada | Qualitative descriptive study To explore the perceptions of exercise among stroke survivors, including their concepts and definitions of exercise, as well as their perceptions of barriers and facilitators to exercise. |
|
| Nicholson, Sniehotta, van Wijck, Greig, Johnston, McMurdo, Dennis, and Mead [36] (2013) A systematic review of perceived barriers and motivators to physical activity after stroke United Kingdom | Systematic review To systematically review the literature to identify all studies examining perceived barriers and motivators to physical activity after stroke. |
|
| Nicholson, Greig, Sniehotta, Johnston, Lewis, McMurdo, Johnston, Scopes, and Mead (2017) [37] Quantitative data analysis of perceived barriers and motivators to physical activity in stroke survivors United Kingdom | Cross-sectional study To explore stroke survivors’ perceived barriers, motivators, self-efficacy, and intention to undertake physical activity |
|
| Débora Pacheco, Guimarães Caetano, Amorim Samora, Sant’Ana, Fuscaldi Teixeira-Salmela, and Scianni [40] (2021) Perceived barriers to exercise reported by individuals that suffered stroke and who are able to walk in the community. Brazil | Cross-sectional study To identify the perceived barriers to exercise, which could be modified, as well as the associated factors in people at the sub-acute post-stroke stages, who were able to walk in the community. |
|
| Goffredo, Infarinato, Pournajaf, Romano, Ottaviani, Pellicciari, Galafate, Gabbani, Gison, and Franceschini [38] (2020) Barriers to sEMG Assessment During Overground Robot-Assisted Gait Training in Subacute Stroke Patients Italy | Cross-sectional study To assess the barriers to the implementation of a ElectroMyoGraphy-based assessment protocol in a clinical context for evaluating the effects of Robot-Assisted Gait Training in subacute stroke patients. |
|
| Tole, Raymond, Williams, Clark, and Holland [39] (2020) Strength training to improve walking after stroke: how physiotherapist, patient and workplace factors influence exercise prescription Australia | Qualitative descriptive study To explore perceived barriers and facilitators that influence Australian physiotherapeutic practices when prescribing strength training to stroke survivors undergoing gait rehabilitation. |
|
| de Rooij, van de Port, van der Heijden, Meijer, and Visser-Meily [41] (2021) Perceived barriers and facilitators for gait-related participation in people after stroke: From a patients’ perspective Netherlands | Qualitative descriptive study To explore barriers and facilitators for gait-related participation from the perspective of people who suffered stroke. |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tavares, E.; Coelho, J.; Rogado, P.; Correia, R.; Castro, C.; Fernandes, J.B. Barriers to Gait Training among Stroke Survivors: An Integrative Review. J. Funct. Morphol. Kinesiol. 2022, 7, 85. https://doi.org/10.3390/jfmk7040085
Tavares E, Coelho J, Rogado P, Correia R, Castro C, Fernandes JB. Barriers to Gait Training among Stroke Survivors: An Integrative Review. Journal of Functional Morphology and Kinesiology. 2022; 7(4):85. https://doi.org/10.3390/jfmk7040085
Chicago/Turabian StyleTavares, Eveline, Joana Coelho, Patrícia Rogado, Rita Correia, Cidália Castro, and Júlio Belo Fernandes. 2022. "Barriers to Gait Training among Stroke Survivors: An Integrative Review" Journal of Functional Morphology and Kinesiology 7, no. 4: 85. https://doi.org/10.3390/jfmk7040085