
Correlation between Tooth Position Parameters and Apical Fenestration: A Cone-Beam Computed Tomography Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
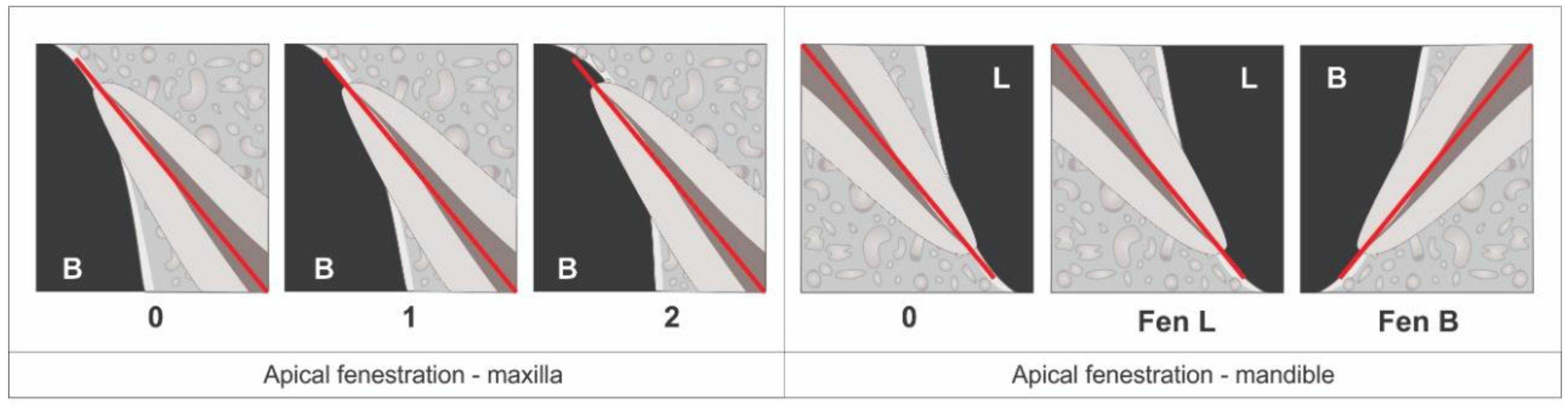
2.3. Presence of Apical Fenestration
- Score 0 indicates that the tooth exhibits no apical fenestration.
- Score 1 signifies that the tooth displays apical fenestration below the buccal cortical plate.
- Score 2 indicates the presence of apical fenestration that encompasses the entire apex of the tooth.
- Score 0 denotes the absence of apical fenestration.
- Score L indicates lingual apical fenestration.
- Score B denotes buccal/labial apical fenestration.
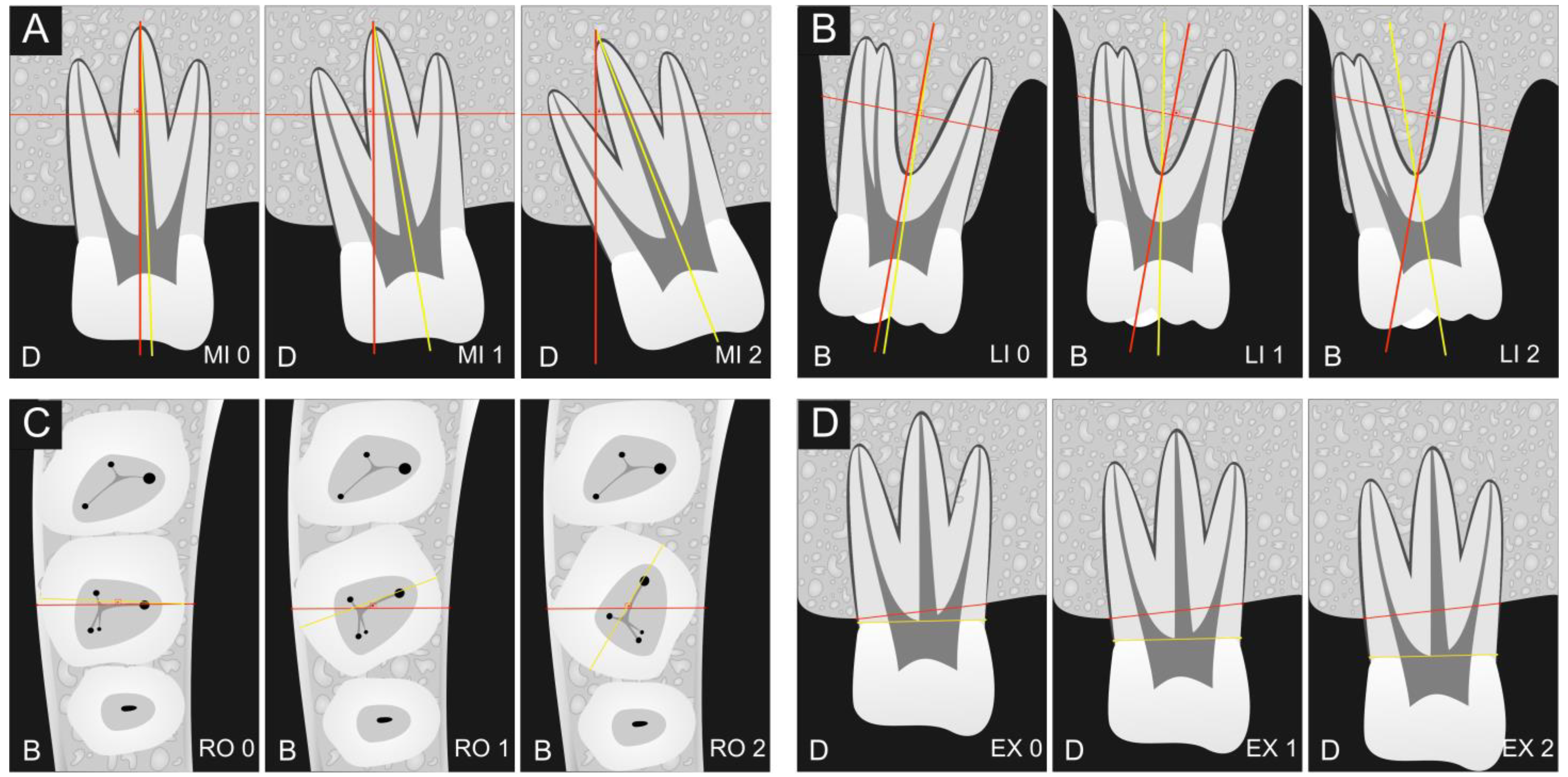
2.4. Assessment of Tooth Positions
- MI0 indicates a mesial crown inclination of up to 5 degrees.
- MI1 denotes a mesial crown inclination ranging from 5 to 15 degrees.
- MI2 signifies a mesial crown inclination exceeding 15 degrees.
- LI0 represents a lingual crown inclination of up to 5 degrees.
- LI1 represents a lingual crown inclination ranging from 5 to 15 degrees.
- LI2 represents a lingual crown inclination exceeding 15 degrees.
- RO0 indicates a crown rotation of up to 15 degrees.
- RO1 denotes a crown rotation ranging from 15 to 30 degrees.
- RO2 signifies a crown rotation exceeding 30 degrees.
- EX0 signifies no extrusion of the tooth.
- EX1 denotes tooth extrusion of 1–2 mm.
- EX2 indicates tooth extrusion exceeding 2 mm.
3. Results
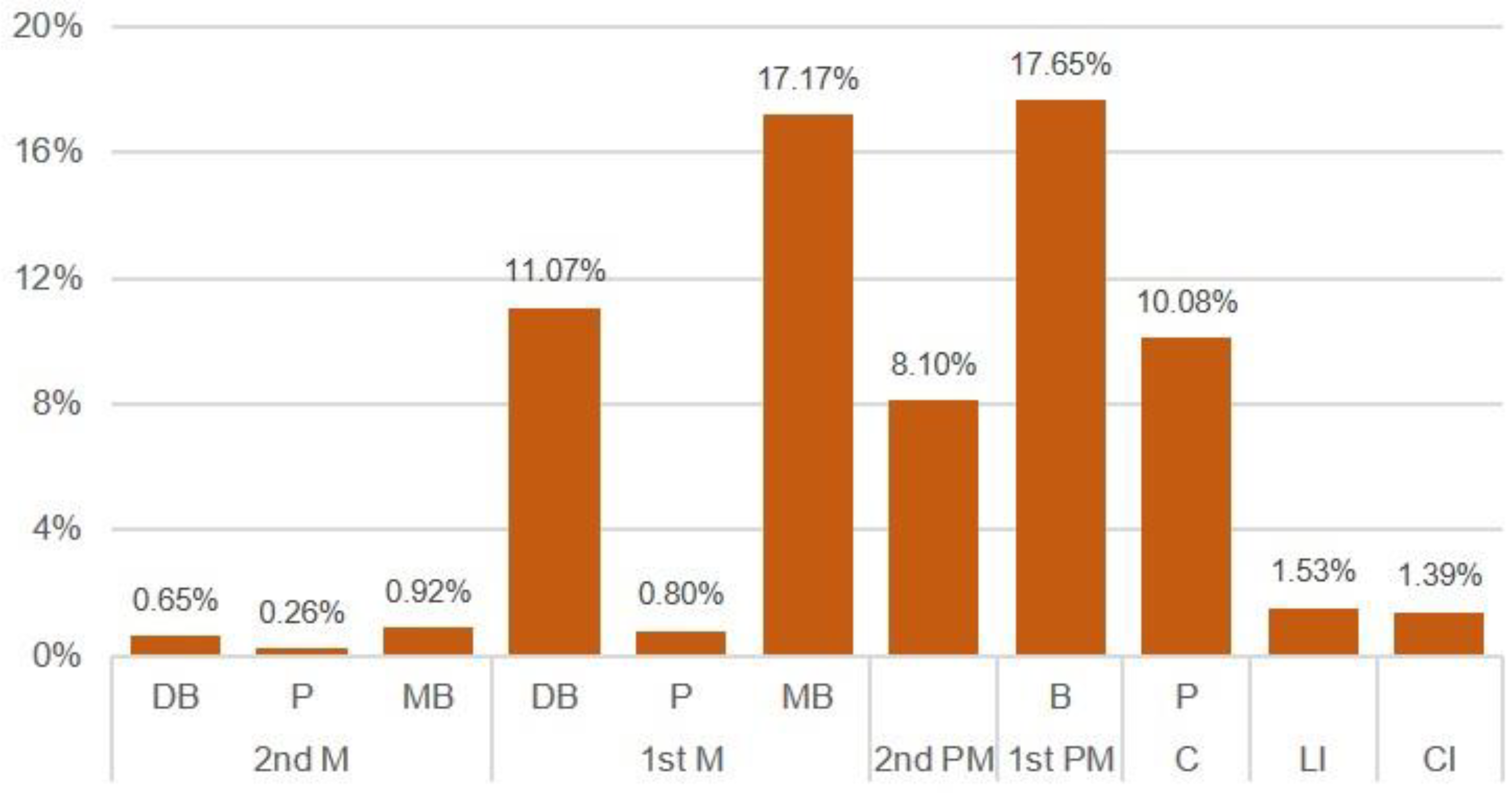
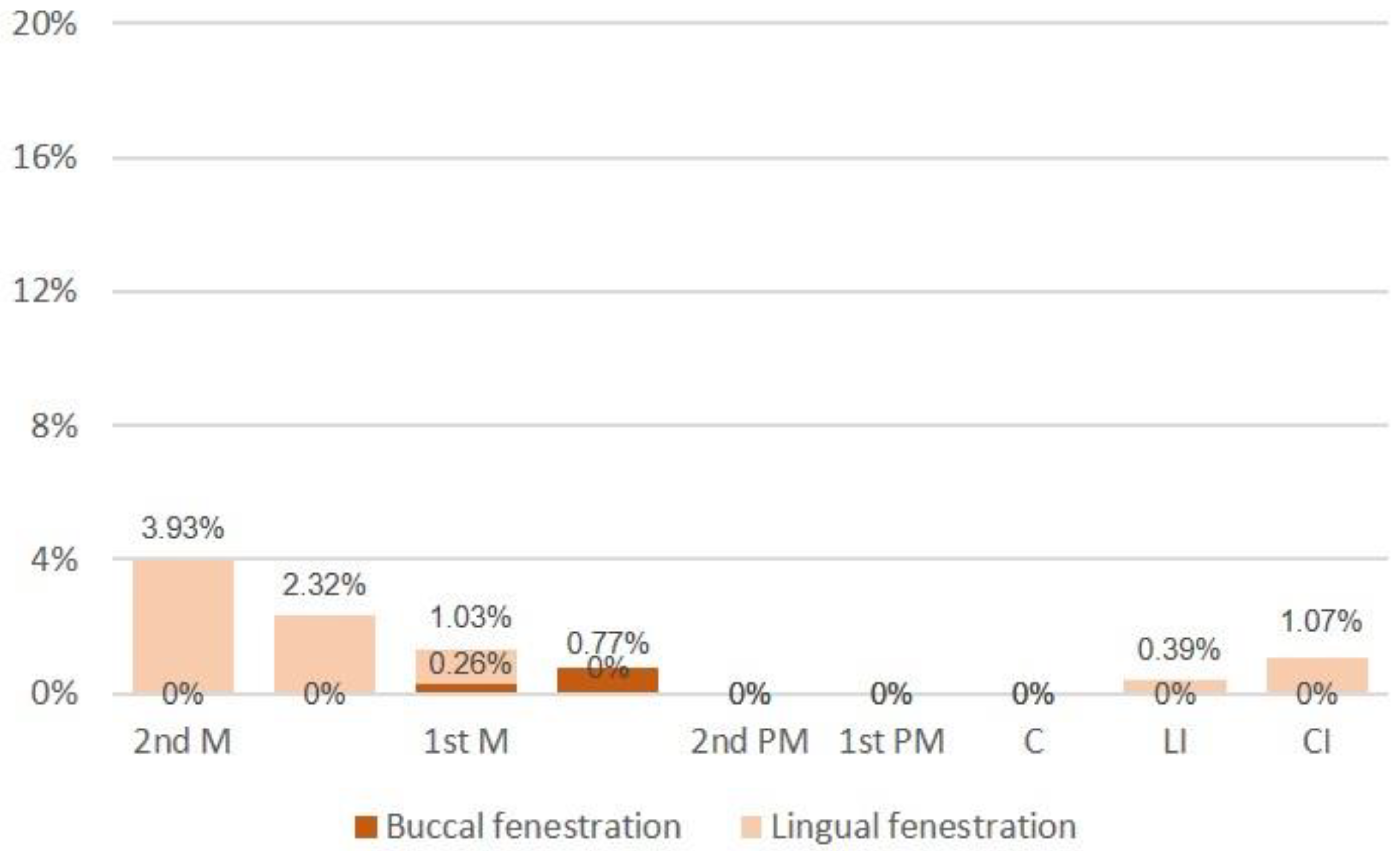
3.1. Presence of Apical Fenestration
3.2. Assessment of Tooth Positions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nimigean, V.R.; Nimigean, V.; Bencze, M.A.; Dimcevici-Poesina, N.; Cergan, R.; Moraru, S. Alveolar bone dehiscences and fenestrations: An anatomical study and review. Rom. J. Morphol. Embryol. 2009, 50, 391–397. [Google Scholar]
- Triches, T.C.; Paula, L.K.; Filho, M.X.; Bolan, M. Apical fenestration and ectopic eruption—Effects from trauma to primary tooth: A clinical case report. Dent. Traumatol. 2011, 27, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Sheng, Y.; Guo, H.-M.; Bai, Y.-X.; Li, S. Dehiscence and fenestration in anterior teeth: Comparison before and after orthodontic treatment. J. Orofac. Orthop. 2020, 81, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Davies, R.M.; Downer, M.C.; Hull, P.S.; Lennon, M.A. Alveolar defects in human skulls. J. Clin. Periodontol. 1974, 1, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Nalbantoğlu, A.M.; Yanık, D. Fenestration and dehiscence defects in maxillary anterior teeth using two classification systems. Aust. Dent. J. 2023, 68, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Consolaro, A. Dehiscences and fenestrations: Methodological care necessary to avoid errors in diagnosis and measurement. Dental Press J. Orthod. 2017, 22, 25–29. [Google Scholar] [CrossRef]
- Pasqualini, D.; Scotti, N.; Ambrogio, P.; Alovisi, M.; Berutti, E. Atypical facial pain related to apical fenestration and overfilling. Int. Endod. J. 2012, 45, 670–677. [Google Scholar] [CrossRef]
- Edney, M.B. Interesting presentation of a retained upper deciduous incisor with apical fenestration. Br. Dent. J. 2000, 188, 369–370. [Google Scholar] [CrossRef]
- Jhaveri, H.M.; Amberkar, S.; Galav, L.; Deshmukh, V.L.; Aggarwal, S. Management of mucosal fenestrations by interdisciplinary approach: A report of three cases. J. Endod. 2010, 36, 164–168. [Google Scholar] [CrossRef]
- Boucher, Y.; Sobel, M.; Sauveur, G. Persistent pain related to root canal filling and apical fenestration: A case report. J. Endod. 2000, 26, 242–244. [Google Scholar] [CrossRef]
- Spasser, H.F.; Wendt, R. Apical fenestration. A cause for recalcitrant post endodontic pain. N. Y. State Dent. J. 1973, 39, 25–26. [Google Scholar] [PubMed]
- Başer Can, E.D.; Karapınar Kazandağ, M.; Kaptan, R.F. Inadvertent apical extrusion of sodium hypochlorite with evaluation by dental volumetric tomography. Case Rep. Dent. 2015, 2015, 247547. [Google Scholar] [CrossRef] [PubMed]
- Furusawa, M.; Hayakawa, H.; Ida, A.; Ichinohe, T. A case of apical fenestration misdiagnosed as persistent apical periodontitis. Bull. Tokyo Dent. Coll. 2012, 53, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Zhou, H.; Zhang, K.; Wang, X.; Zhong, L.; Hou, Y.; Chen, Y. The clinical efficacy of periodontally accelerated osteogenic orthodontics in patients with bone fenestration and dehiscence: A retrospective study. Head Face Med. 2022, 18, 40. [Google Scholar] [CrossRef] [PubMed]
- Scarfe, W.C.; Levin, M.D.; Gane, D.; Farman, A.G. Use of cone beam computed tomography in endodontics. Int. J. Dent. 2009, 2009, 634567. [Google Scholar] [CrossRef]
- Cotton, T.P.; Geisler, T.M.; Holden, D.T.; Schwartz, S.A.; Schindler, W.G. Endodontic applications of cone-beam volumetric tomography. J. Endod. 2007, 33, 1121–1132. [Google Scholar] [CrossRef]
- Ferrari, C.H.; Abu Hasna, A.; Martinho, F.C. Three Dimensional mapping of the root apex: Distances between apexes and anatomical structures and external cortical plates. Braz. Oral Res. 2021, 35, e022. [Google Scholar] [CrossRef]
- Lindhe, J.; Lang, N.P.; Karring, T. The anatomy of periodontal tissue. In Clinical Periodontology and Implant Dentistry; Blackwell Company: Oxford, UK, 2008; p. 3. [Google Scholar]
- Chen, G.; Fang, C.T.; Tong, C. The management of mucosal fenestration: A report of two cases. Int. Endod. J. 2009, 42, 156–164. [Google Scholar] [CrossRef]
- Kalaitzoglou, M.-E.; Lambrianidis, T. Understanding root fenestration: A systematic scoping review of prevalence and clinical factors. Aust. Endod. J. 2023, 49, 428–443. [Google Scholar] [CrossRef]
- Urbani, G.; Lombardo, G.; Filippini, P.; Nocini, F.P. Dehiscence and fenestration: Study of distribution and incidence in a homogeneous population model. Stomatol. Mediterr. 1991, 11, 113–118. [Google Scholar]
- Tal, H. Alveolar dehiscences and fenestrae in dried South African Negro mandibles. Am. J. Phys. Anthropol. 1983, 61, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Yagci, A.; Veli, I.; Uysal, T.; Ucar, F.I.; Ozer, T.; Enhos, S. Dehiscence and fenestration in skeletal Class I, II, and III malocclusions assessed with cone-beam computed tomography. Angle Orthod. 2012, 82, 67–74. [Google Scholar] [CrossRef]
- Kajan, Z.D.; Seyed Monir, S.E.; Khosravifard, N.; Jahri, D. Fenestration and dehiscence in the alveolar bone of anterior maxillary and mandibular teeth in cone-beam computed tomography of an Iranian population. Dent. Res. J. 2020, 17, 380–387. [Google Scholar] [CrossRef]
- Li, C.; Dimitrova, B.; Boucher, N.S.; Chung, C.-H. Buccolingual Inclination of Second Molars in Untreated Adolescents and Adults with Near Normal Occlusion: A CBCT Study. J. Clin. Med. 2022, 11, 6629. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.; Lee, A.; Zhang, C. Diagnosis and Management of Apical Fenestrations Associated with Endodontic Diseases: A Literature Review. Eur. Endod. J. 2021, 6, 25–33. [Google Scholar] [CrossRef]
- Edel, A. Alveolar bone fenestrations and dehiscences in dry Bedouin jaws. J. Clin. Periodontol. 1981, 8, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Rupprecht, R.D.; Horning, G.M.; Nicoll, B.K.; Cohen, M.E. Prevalence of dehiscences and fenestrations in modern American skulls. J. Periodontol. 2001, 72, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Alroomy, R. Apical fenestration in endodontically treated teeth: A report of two cases. Niger. J. Clin. Pract. 2021, 24, 1092–1095. [Google Scholar] [CrossRef]
- Abu Hasna, A.; Theodoro, A.L.; Pereira, L.M.; Ramos, L.D.P.; Campos, T.M.B.; Ala Rachi, M.; Al-Nahalwi, T.; de Oliveira, L.D.; Carvalho, C.A.T. Antimicrobial Action, Genotoxicity, and Morphological Analysis of Three Calcium Silicate-Based Cements. Biomed Res. Int. 2022, 2022, 2155226. [Google Scholar] [CrossRef]
- Ribeiro Camargo, C.H.; Bittencourt, T.S.; Hasna, A.A.; Palo, R.M.; Talge Carvalho, C.A.; Valera, M.C. Cyclic fatigue, torsional failure, and flexural resistance of rotary and reciprocating instruments. J. Conserv. Dent. 2020, 23, 364–369. [Google Scholar] [CrossRef]
- Siqueira Junior, J.F.; Rôças, I.D.N.; Marceliano-Alves, M.F.; Pérez, A.R.; Ricucci, D. Unprepared root canal surface areas: Causes, clinical implications, and therapeutic strategies. Braz. Oral Res. 2018, 32, e65. [Google Scholar] [CrossRef] [PubMed]
- Behrents, K.T.; Speer, M.L.; Noujeim, M. Sodium hypochlorite accident with evaluation by cone beam computed tomography. Int. Endod. J. 2012, 45, 492–498. [Google Scholar] [CrossRef]
- Alfouzan, K.; Jamleh, A. Fracture of nickel titanium rotary instrument during root canal treatment and re-treatment: A 5-year retrospective study. Int. Endod. J. 2018, 51, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Bürklein, S.; Benten, S.; Schäfer, E. Quantitative evaluation of apically extruded debris with different single-file systems: Reciproc, F360 and OneShape versus Mtwo. Int. Endod. J. 2014, 47, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Coskunses, F.M.; Sinanoglu, A.; Helvacioglu-Yigit, D.; Abbott, P.V. The extrusion of root canal cement containing paraformaldehyde into the inferior alveolar nerve canal resulting in infection and numbness. Int. Endod. J. 2016, 49, 610–617. [Google Scholar] [CrossRef]
- Tilotta-Yasukawa, F.; Millot, S.; El Haddioui, A.; Bravetti, P.; Gaudy, J.-F. Labiomandibular paresthesia caused by endodontic treatment: An anatomic and clinical study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 102, e47–e59. [Google Scholar] [CrossRef]
- Bromberg, N.; Brizuela, M. Dental cone beam computed tomography. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Corte-Real, A.; Nunes, T.; Caetano, C.; Almiro, P.A. Cone Beam Computed Tomography (CBCT) Technology and Learning Outcomes in Dental Anatomy Education: E-Learning Approach. Anat. Sci. Educ. 2021, 14, 711–720. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maxilla | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mesial Inclination | Lingual Inclination | Rotation | Extrusion | ||||||||||||||||
| 0 | 1 | 2 | Total | 0 | 1 | 2 | Total | 0 | 1 | 2 | Total | 0 | 1 | 2 | Total | ||||
| MI0 | 5115 | 322 | 64 | 5501 | LI0 | 4587 | 34 | 4 | 4625 | RO0 | 5451 | 340 | 73 | 5864 | EX0 | 5445 | 315 | 69 | 5829 |
| MI1 | 843 | 53 | 30 | 926 | LI1 | 1363 | 214 | 45 | 1622 | RO1 | 522 | 37 | 24 | 583 | EX1 | 447 | 61 | 28 | 536 |
| MI2 | 52 | 6 | 5 | 63 | LI2 | 60 | 133 | 50 | 243 | RO2 | 37 | 4 | 2 | 43 | EX2 | 118 | 5 | 2 | 125 |
| Mandible | |||||||||||||||||||
| 0 | L | B | Total | 0 | L | B | Total | 0 | L | B | Total | 0 | L | B | Total | ||||
| DI | 77 | 0 | 0 | 77 | BI | 411 | 45 | 2 | 458 | ||||||||||
| MI0 | 3813 | 47 | 4 | 3864 | LI0 | 3822 | 5 | 0 | 3827 | RO0 | 3988 | 44 | 2 | 4034 | EX0 | 4442 | 50 | 4 | 4496 |
| MI1 | 466 | 2 | 0 | 468 | LI1 | 273 | 0 | 2 | 275 | RO1 | 460 | 6 | 2 | 468 | EX1 | 65 | 0 | 0 | 65 |
| MI2 | 155 | 1 | 0 | 156 | L12 | 5 | 0 | 0 | 5 | RO2 | 63 | 0 | 0 | 63 | EX2 | 4 | 0 | 0 | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrari, C.H.; de Carvalho, L.S.; Rocha, C.T.; Abu Hasna, A. Correlation between Tooth Position Parameters and Apical Fenestration: A Cone-Beam Computed Tomography Study. Methods Protoc. 2024, 7, 14. https://doi.org/10.3390/mps7010014
Ferrari CH, de Carvalho LS, Rocha CT, Abu Hasna A. Correlation between Tooth Position Parameters and Apical Fenestration: A Cone-Beam Computed Tomography Study. Methods and Protocols. 2024; 7(1):14. https://doi.org/10.3390/mps7010014
Chicago/Turabian StyleFerrari, Carlos Henrique, Lara Steffany de Carvalho, Caroline Trefiglio Rocha, and Amjad Abu Hasna. 2024. "Correlation between Tooth Position Parameters and Apical Fenestration: A Cone-Beam Computed Tomography Study" Methods and Protocols 7, no. 1: 14. https://doi.org/10.3390/mps7010014