
Association of Ultrasonography and Health Education during Antenatal Visits among Pregnant Women to Reduce Unnecessary Caesarean Section in Bangladesh: Study Protocol for a Cluster Randomized Control Trial
 , , ,
, , ,  ,
, 
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Study Setting
2.3. Study Participants
2.4. Inclusion Criteria
2.5. Operational Definition of Term
2.6. Recruitment Procedure, Obtaining Consent and Checking Eligibility
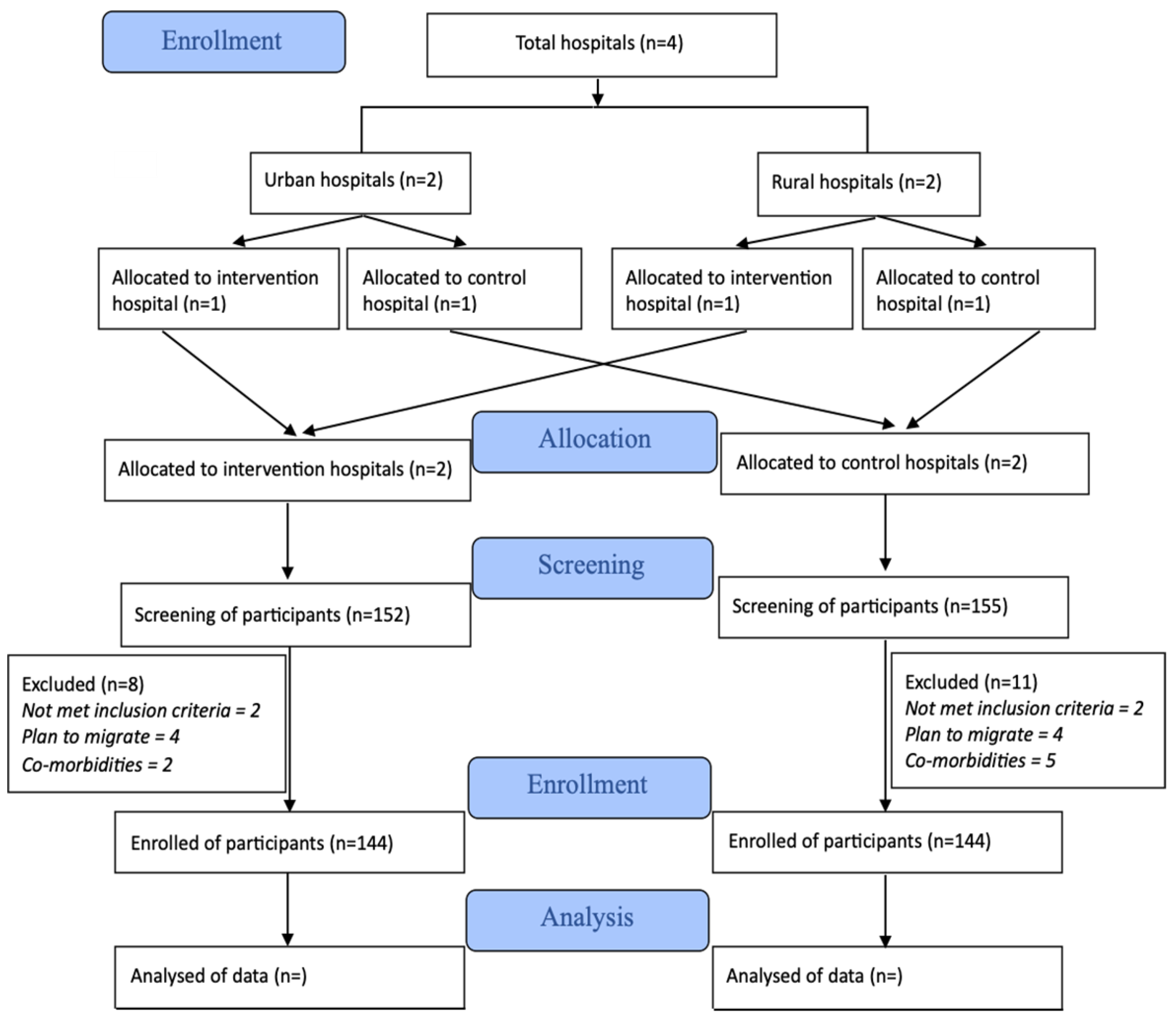
2.7. Allocation and Randomization
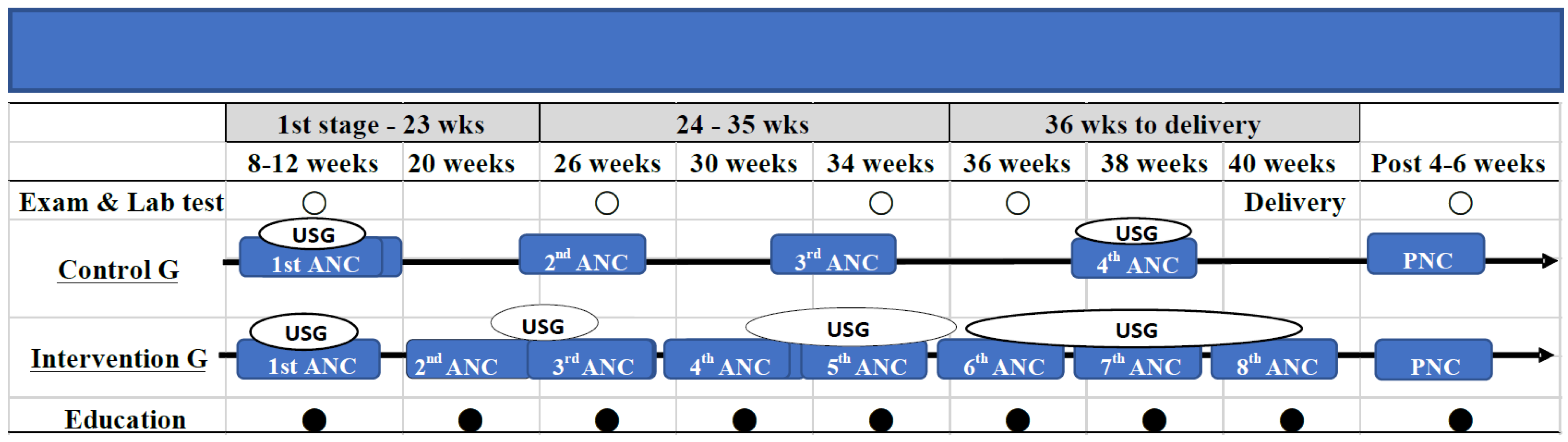
2.8. Health Education Materials
2.9. Quality Control and Quality Assurance for Data Management
2.10. Training of Study Staff
2.11. Data Collection and Entry Procedures
2.12. Sample Size
2.13. Statistical Analyses
2.14. Strengths and Limitations of This Study
- ➢
- As this is a multicenter study, it will give us a broader understanding of the risk factors related to unnecessary C/S and will minimize biases.
- ➢
- For resource poor low-and-middle income countries, this study’s findings will give significant economic relief to pregnant mothers by preventing unnecessary C/S and reduce hospital costs and infections.
- ➢
- The study findings will have a significant impact in reducing maternal and childhood morbidity and mortality and increase the potential of achieving the Sustainable Development Goal (SDGs) by 2030.
- ➢
- According to the study design, pregnant women maybe admitted to any of the hospitals according to their choice. As there are many public-private hospitals and clinics in the study areas, we could not involve all the gynecologists and obstetricians from the study area in our study. According to World Health Organization, there are roles played by gynecologist and obstetrician in C/S, and the outcome might be influenced by these in terms of their decisions to perform C/S.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Sexual and Reproductive Health. Caesarean Sections should Only Be Performed when Medically necessary Says WHO. 2022. Available online: https://www.who.int/reproductivehealth/topics/maternal_perinatal/cs-statement/en/ (accessed on 5 July 2022).
- Boerma, T.; Ronsmans, C.; Melesse, D.Y.; Barros, A.J.D.; Barros, F.C.; Juan, L.; Moller, A.-B.; Say, L.; Hosseinpoor, A.R.; Yi, M.; et al. Global Epidemiology of Use of and Disparities in Caesarean Sections. Lancet 2018, 392, 1341. [Google Scholar] [CrossRef] [PubMed]
- Charvalho, P.d.a.S.; Hansson, B.M.; Stjernholm, V.Y. Indications for Increase in Caesarean Delivery. Reprod. Health 2019, 16, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bangladesh Demographic and Health Survey 2017–2018- Key Indicators. pdf. Available online: https://dhsprogram.com/pubs/pdf/PR104/PR104.pdf (accessed on 24 October 2022).
- Save the Children International 2022. Bangladesh: 51 Percent Increase in “Unnecessary” C-Sections in Two Years. Available online: https://www.savethechildren.net/news/bangladesh-51-cent-increase-“unnecessary”-c-sections-two-years#_edn2 (accessed on 5 August 2022).
- World Health Organization. WHO Recommendations Non-Clinical Interventions to Reduce Unnecessary Caesarean Sections. Infographic-Unnecessary-Caesarean-Section.pdf. Available online: https://www.who.int/reproductivehealth/publications/unnecessary-cs-infographics/en/ (accessed on 8 July 2022).
- Hasan, F.; Alam, M.M.; Hossain, M.G. Associated Factors and Their Individual Contributions to Caesarean Delivery among Married Women in Bangladesh: Analysis of Bangladesh Demographic and Health Survey Data. BMC Pregnancy Childbirth 2019, 19, 433. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization 2022. Pregnant Women Must Be Able to Access the Right Care at the Right Time, Says WHO. Available online: https://www.who.int/news-room/detail/07-11-2016-pregnant-women-must-be-able-to-access-the-right-care-at-the-right-time-says-who (accessed on 28 July 2022).
- Dowswell, T.; Carroli, G.; Duley, L.; Gates, S.; Gülmezoglu, A.M.; Khan-Neelofur, D.; Piaggio, G. Alternative Versus Standard Packages of Antenatal Care for Low-risk Pregnancy. Cochrane Database Syst. Rev. 2015, 7, CD000934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Recommendations on Antenatal Care for A Positive Pregnancy Experience. 2022. Available online: https://www.who.int/publications/i/item/9789241549912 (accessed on 10 July 2022).
- Alland, J.Y.K.; Ali, H.; Mehra, S.; LeFevre, A.E.; Pak, S.E.; Shaikh, S.; Christian, P.; Labrique, A.B. Antenatal Care in Rural Bangladesh: Current State of Costs, Content and Recommendations for Effective Service Delivery. BMC Health Serv. Res. 2019, 19, 861. [Google Scholar] [CrossRef]
- World Health Organization 2022. WHO Guideline Development Group Meeting on WHO Antenatal Care Guidelines: Update on Early Ultrasound Scan Recommendation. Available online: https://www.who.int/news/item/07-06-2021-who-antenatal-care-guidelines-update-on-early-ultrasound-scan-recommendation (accessed on 15 June 2022).
- Ryan, B.L.; Krishnan, R.J.; Terry, A.; Thind, A. Do Four or More Antenatal Care Visits Increase Skilled Birth Attendant Use and Institutional Delivery in Bangladesh? A Propensity-score Matched Analysis. BMC Public Health 2019, 19, 583. [Google Scholar] [CrossRef] [PubMed]
- Pervin, J.; Moran, A.; Rahman, M.; Razzaque, A.; Sibley, L.; Streatfield, P.K.; Reichenbach, L.J.; Koblinsky, M.; Hruschka, D.; Rahman, A. Association of Antenatal Care with Facility Delivery and Perinatal Survival—A Population-based Study in Bangladesh. BMC Pregnancy Childbirth 2012, 12, 111. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization 2015. Success Factors for Women’s and Children’s Health: Bangladesh. Bangladesh_country_report.pdf. Available online: https://www.who.int/pmnch/knowledge/publications/bangladesh_country_report.pdf (accessed on 18 June 2022).
- Chen, I.; Opiyo, N.; Tavender, E.; Mortazhejri, S.; Rader, T.; Petkovic, J.; Yogasingam, S.; Taljaard, M.; Agarwal, S.; Laopaiboon, M.; et al. Non-clinical Interventions for Reducing Unnecessary Caesarean Section. Cochrane Database Syst. Rev. 2018, 9, CD005528. [Google Scholar] [CrossRef] [PubMed]
- Begum, T.; Ellis, C.; Sarker, M.; Rostoker, J.F.; Rahman, A.; Anwar, I.; Reichenbach, L. A Qualitative Study to Explore the Attitudes of Women and Obstetricians Towards Caesarean Delivery in Rural Bangladesh. BMC Pregnancy Childbirth 2018, 18, 368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The World Bank Group 2022. WHO, UNICEF, UNFPA, World Bank Group, and the United Nations Population Division. Trends in Maternal Mortality: 2000 to 2017. Geneva, World Health Organization. 2019. Maternal mortality ratio (modeled estimate, per 100,000 live births)—Bangladesh. Available online: https://data.worldbank.org/indicator/SH.STA.MMRT?locations=BD (accessed on 9 July 2022).
- The United Nations Children’s Fund (UNICEF). UN Inter-Agency Group for Child Mortality Estimation. Levels and Trends in Child Mortality. Available online: https://childmortality.org/files_v20/download/IGME%20Report%202015_9_3%20LR%20Web.pdf (accessed on 12 July 2022).
- The United Nations Children’s Fund (UNICEF). Monitoring the Situation of Children and Women. Maternal Mortality. 2019. Available online: https://data.unicef.org/topic/maternal-health/maternal-mortality/ (accessed on 21 July 2022).
- Novaes, I.C.; Clementino, L.C.; Flores-Mir, C.; Marques, L.S.; Martins-Júnior, P.A. How to Use the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) in Orthodontic Research. Dental Press J. Orthod. 2022, 27, e2220290. [Google Scholar] [CrossRef] [PubMed]
- Ghosn, L.; Boutron, I.; Ravaud, P. Consolidated Standards of Reporting Trials (CONSORT) Extensions Covered Most Types of Randomized Controlled Trials, but the Potential Workload for Authors was High. J. Clin. Epidemiol. 2019, 113, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Ylva Vladic Stjernholm. Caesarean Section: Reasons for and Actions to Prevent Unnecessary Caesareans. Open Access Peer-Reviewed Chapter. 2018. Available online: https://www.intechopen.com/chapters/63427 (accessed on 8 July 2022).
- Charan, J.; Biswas, T. How to Calculate Sample Size for Different Study Designs in Medical Research? Indian J. Psychol. Med. 2013, 35, 121–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, V.A.; Coffman, C.J.; Hudgens, M.G. Interpreting the Results of Intention-to-treat, Per-protocol, and As-treated Analyses of Clinical Trials. JAMA 2021, 326, 433–434. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association 2022. Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 14 August 2022).


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shirin, H.; Moriyama, M.; Huq, K.A.T.M.E.; Rahman, M.M.; Masud, S.B.; Begum, R.A.; Misty, K.; Hawlader, M.D.H. Association of Ultrasonography and Health Education during Antenatal Visits among Pregnant Women to Reduce Unnecessary Caesarean Section in Bangladesh: Study Protocol for a Cluster Randomized Control Trial. Methods Protoc. 2022, 5, 101. https://doi.org/10.3390/mps5060101
Shirin H, Moriyama M, Huq KATME, Rahman MM, Masud SB, Begum RA, Misty K, Hawlader MDH. Association of Ultrasonography and Health Education during Antenatal Visits among Pregnant Women to Reduce Unnecessary Caesarean Section in Bangladesh: Study Protocol for a Cluster Randomized Control Trial. Methods and Protocols. 2022; 5(6):101. https://doi.org/10.3390/mps5060101
Chicago/Turabian StyleShirin, Habiba, Michiko Moriyama, K.A.T.M. Ehsanul Huq, Md Moshiur Rahman, Sumaya Binte Masud, Rowshan Ara Begum, Kamrunnahar Misty, and Mohammad Delwer Hossain Hawlader. 2022. "Association of Ultrasonography and Health Education during Antenatal Visits among Pregnant Women to Reduce Unnecessary Caesarean Section in Bangladesh: Study Protocol for a Cluster Randomized Control Trial" Methods and Protocols 5, no. 6: 101. https://doi.org/10.3390/mps5060101