
Information and Parental Consent for French Neonatal Screening: A Qualitative Study on Parental Opinion


Abstract
:1. Introduction
2. Materials and Methods
2.1. Population and Recruitment
2.2. Interviews
2.3. Data Collection and Analysis
2.4. Objectives
- (1).
- Quality-delivered information, orally and in writing, by a health professional containing understandable explanations about the purpose of screening, the diseases screened, and the method of communicating results.
- (2).
- Free consent, oral and written, for the genetic analysis of cystic fibrosis, after a period of consideration and with the awareness of having a choice.
3. Results
3.1. Population
3.2. Thematic Analysis
3.2.1. Knowledge of Neonatal Screening
- Mother 5:
- What I understood was that there was a lot of screening grouped together. There was cystic fibrosis, there were other diseases. And that we did this three days after the birth.
- Mother 19:
- Basically, if it’s negative, you won’t get any news, but if it’s positive, it’s within 6 weeks.
- Father 2:
- But no, it was because of the reflux that they did the blood test, I think.
- Mother 3:
- So the pediatrician at the hospital still told us to monitor, especially before these ten years to see if he has any symptoms.
- Mother 1:
- But he had two screenings in fact? No, but they also did a screening with the platelet while we were there. (addressing the child’s father).
- Father 5:
- I don’t know if it’s specific to babies born with a problem or if it’s systematic.
3.2.2. Information Received by Parents
- Mother 12:
- The midwife gave it to me, and yes it helped me explain to my partner who couldn’t be there. Otherwise I wouldn’t have remembered anything (laughter).
- Mother 15:
- I think what was done well at the clinic was that they gave us a pamphlet. That of course, we don’t read or necessarily read very quickly at the maternity ward, but there was this pamphlet.
- Mother 13:
- In any case, during the childbirth preparation course, I was the one who asked the questions because I had already informed myself on the Internet.
- Mother 3:
- Afterwards, I knew a little bit because we already have an older son, so the test had already been done.
- Mother 4:
- In fact, I have a cousin who is very close to me who had a similar problem with her child revealed by the Guthrie test.
- Mother 10:
- I wish someone had explained it to me a bit more [...], and especially in simpler terms because it can be explained in very technical terms which are difficult to understand.
3.2.3. Parental Choice
- Mother 13:
- It’s not mandatory but it’s strongly recommended so that if there’s a problem, it can be taken care of quickly.
- Father 15:
- We didn’t think much about it in the sense that it seemed like a good thing. And it was pretty obvious to agree to do the research.
- Mother 11:
- We consider it normal. We do it because it has to be done.
- Mother 15:
- Anyway, Guthrie was mandatory, right? Is that it?
- Mother 15:
- At the maternity ward, everything happens very quickly and then you are tired. It’s true that you don’t necessarily take the time to read or there is information that gets lost.
- Mother 3:
- Because it’s true that when you are presented with a done deal. Well, we tell ourselves it’s for our child, we can sign without really realizing what paper we are signing because we are also in the euphoria of the birth.
3.2.4. The Experience of the Screening Process
- Mother 4:
- It’s true that I didn’t pay too much attention. I was more in the mindset that he was doing well when he was doing things like heel prick and all that... Since it was a basic test that was done for all babies. I didn’t really ask too many questions.
- Mother and father 2:
- The day we got the letter with the child’s name in our mailbox, we didn’t understand what it was.
- Mother 17:
- Because when you don’t know, when they call you, and tell the mother that her daughter needs to do some tests, you can’t just stay calm.
- Mother 8:
- Even though she is doing great now. But it’s true that there is always that anxiety behind.
3.2.5. Wishes and Evolutionary Perspectives
- Mother 7:
- Maybe they could take more time to explain things to us. Actually, I find that there are a lot of technical terms used at the maternity ward.
- Father 1:
- After that, we would have liked to know a deadline. How long would it have taken to get results if it was bad. In fact, just to know in general and not to know if there was something. [...] At least, to have a positive or negative response.
- Father 11:
- In writing, I would find it interesting to put this in the childbirth folder of the first days, the classic steps that happen with photos. I even find that for people who do not necessarily have access to reading or something, having something with pictograms can be quite nice.
- Mother 13:
- A website could also be useful. It’s true that nowadays we rely a lot on the internet for information, so it could be helpful.
- Mother 1:
- I think it would be a good idea to have the information in advance because after all it comes all at once and then there can be complications like we had.
- Mother 10:
- And then we say it several times. That the dad is there, it would be really appreciated, I think.
- Mother 10:
- Maybe arrive the day before, explain that there will be a blood test and then give time to think about it and arrive the next day with the paper saying here, we talked about it the day before. Now, are you okay with it or not?
- Mother Family 7:
- Well maybe by signing, that, people would be interested. Well that’s not what I mean. Maybe they would feel more involved.
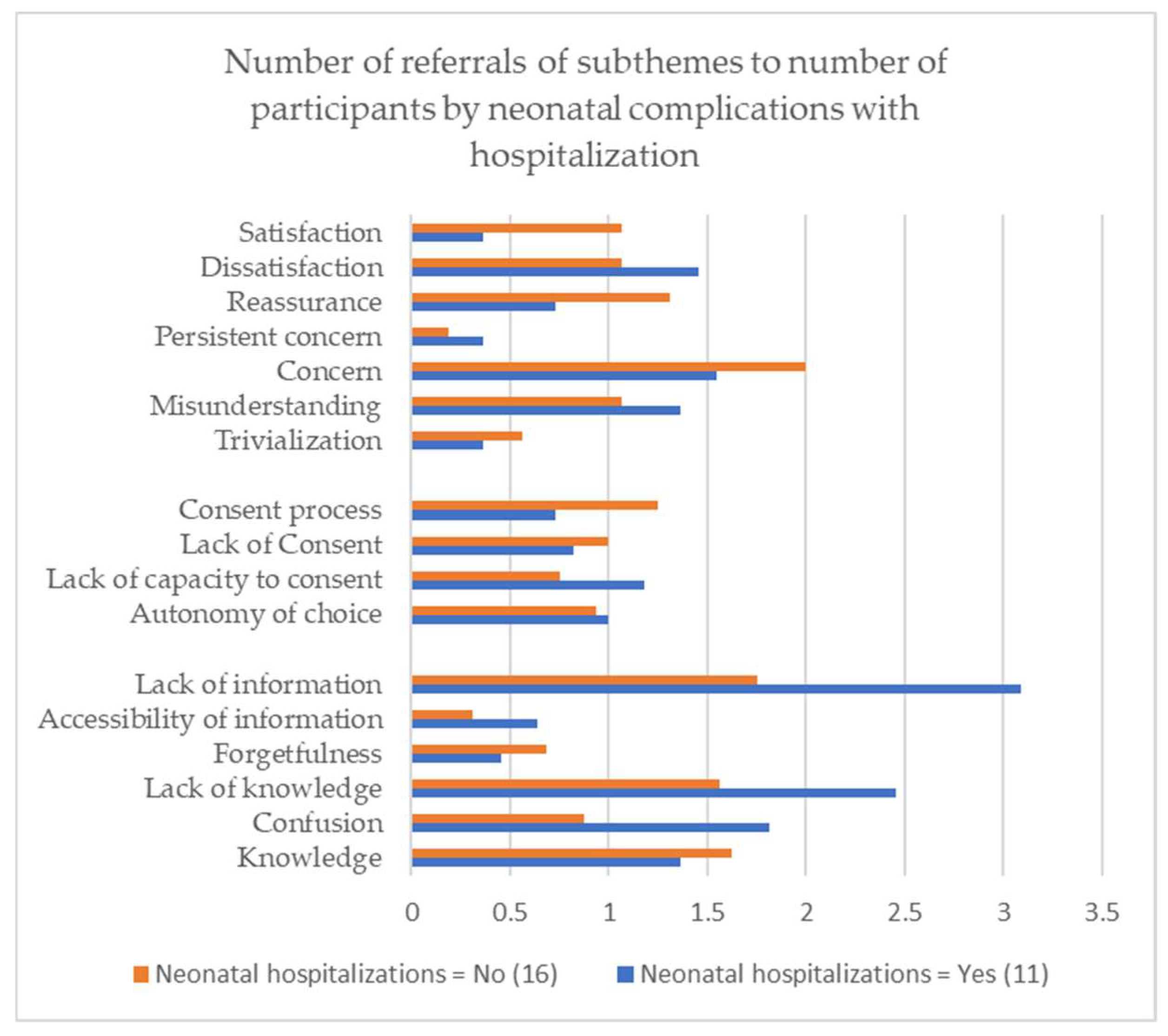
3.3. The Limits of Informed Consent and Hospitalization of the Newborn
4. Discussion
4.1. Information
4.2. Consent
4.3. The Experience of Abnormal Screening
4.4. Improvement Perspective
4.5. Limitations and Strengths of the DENICE Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Guide for Parent Semi-Directive Interviews
- Introduction:
- Explanation of the purpose of the study:
- Collection of non-opposition and response to participant questions.
- Explanation of the Process:
- Signature of consent to audio recording.
- Interview guide:
- (1)
- Can you tell me where and when your child was born?
- Investigator: If the parent has not addressed the place of birth.In which hospital was your child born?
- Investigator: If the parent has not addressed the postnatal period.After the birth, where was your child hospitalized?
- Investigator: If the parent has not addressed the child’s age.How old is your child today?
- (2)
- Can you tell me how you were informed about the neonatal screening for your child?
- Investigator: If the parent has not addressed the moment when they were informed.When did you first hear about neonatal screening?
- Investigator: If the parent has not discussed how they were informed (leaflet, oral, etc.)How were you informed about this screening?
- Investigator: If the parent has not approached the professional who informed them.Who informed you about this screening?
- Investigator: If the parent has not discussed the presence of both parents during the information session.Were you and the father/mother present at the information session for this screening?
- Investigator: If the parent has not discussed their prior knowledge.Did you know about neonatal screening before arriving at the maternity ward?
- (3)
- What did you understand about neonatal screening at the time of this information?
- Investigator: If the parent has not addressed his knowledge of the diseases tested.Have you understood what diseases are screened for and why?
- Investigator: If the parent did not approach the possibility of asking the professional for additional information or seeking additional information.
- Investigator: If the parent has not addressed the possibility of being contacted or how they will be informed of dubious or negative results.What did you understand about how the screening results would be communicated?
- Investigator: If the parent has not discussed the meaning of further contact.What did you understand about the possibility of being contacted?
- (4)
- Have you accepted this screening? If so, how did you give your consent?
- Investigator: If the parent has not addressed a consent requested.Have you understood that this screening is not mandatory?
- Investigator: If the parent has not approached the person or the fact that we are looking for their consent.Did anyone ask for your permission to perform this blood test?
- Investigator: If the parent has not addressed signing the consent for cystic fibrosis molecular biology.Did you sign a document about the test, do you know why?
- Investigator: If the parent has not addressed the fact that the other parent has consented.Has the father/mother of your child been asked for their consent for the screening?
- (5)
- Can you tell me about the moment you were contacted after this screening?
- Investigator: If the parent has not discussed the illness for which the screening is positive.What is the illness for which your child needed a screening check?
- Investigator: If the parent has not approached the person who contacted them.Who contacted you to inform you of this abnormal screening?
- Investigator: If the parent has not addressed the contact timeline.
- Investigator: If the parent has not discussed the fact that their child is diagnosed as ill.Is your child a carrier of the disease for which the screening was positive?
- (6)
- How did you experience this contact for an abnormal screening?
- Investigator: If the parent has not addressed the notion of anxiety.Were you worried about your child?
- Investigator: If the parent has not addressed the fact that an abnormal screening does not mean being sick.
- Investigator: If the parent has not discussed having look for information after being contacted.Have you looked for additional information? If so, what did you use?
- (7)
- Now that the screening has been performed on your child and with your perspective as a parent who has had a positive screening, how would you have liked to be informed about the neonatal screening?
- Investigator: If the parent has not discussed the information procedures.Would you have wanted oral or written information, or both?
- Investigator: If the parent has not approached the professional they wish to have informed the parents.Which type of healthcare professional should inform you about this screening?
- Investigator: If the parent has not addressed the moment of the information.What is the most opportune time to inform you of this screening?
- Investigator: If the parent has not discussed the content of the information.What relevant information about this screening would you have liked to receive?
- (8)
- How would you have liked to be asked for your consent for this screening?
- Investigator: If the parent has not addressed the consent form.Do you prefer to give your consent for this screening orally or in writing?
- Investigator: If the parent has not addressed the moment to give consent.When should we ask for your consent to do this screening?
- Investigator: If the parent has not approached the people who must give consent.Do you think the opinion of both parents should be taken before the sample is taken?
- (9)
- I am now going to ask you more personal questions to better understand your situation:
What is your age? What is the age of the child’s father/mother?What is your profession? What is the profession of the child’s father/mother?Do you have any other children?
Appendix B

{kind=link}
| Themes | Subthemes |
|---|---|
| Knowledge | Confusion |
| Lack of knowledge | |
| Acquired knowledge | |
| Forgetfulness | |
| Consent | Autonomy of choice |
| Reflection period | |
| Method of consent | |
| Lack of capacity to consent | |
| Lack of consent | |
| Person consenting | |
| Consent process | |
| Information | Accessibility of information |
| Experience | |
| Recipient of information | |
| Lack of information | |
| Timing of information | |
| Source of information | |
| Perspective | Desired consent |
| Desired content | |
| Ideal time for information | |
| Desired source of information | |
| Experience | Trivialization |
| Misunderstanding | |
| Concern | |
| Persistent concern | |
| Dissatisfaction | |
| Reassurance | |
| Satisfaction |
Appendix C
References
- Botler, J.; Camacho, L.A.B.; da Cruz, M.M.; George, P. Neonatal Screening: The Challenge of an Universal and Effective Coverage. Ciênc. Amp Saúde Coletiva 2010, 15, 493–508. [Google Scholar] [CrossRef] [PubMed]
- National Coordination of Neonatal Screening Center. Activity Report of Year 2021—National Neonatal Screening Program; France. 2022. Available online: https://depistage-neonatal.fr/wp-content/uploads/2023/01/Rapport-Activite-2021.pdf (accessed on 29 March 2023).
- American College of Medical Genetics Newborn Screening Expert Group Newborn Screening: Toward a Uniform Screening Panel and System--Executive Summary. Pediatrics 2006, 117, S296–S307. [CrossRef] [PubMed]
- Wilson, J.M.G.; Jungner, G.; World Health Organization. Principles and Practice of Screening for Disease; World Health Organization: Geneva, Switzerland, 1968.
- Ministry of Solidarity and Health. Order of February 22, 2018 Regarding the Organization of the National Program for Neonatal Screening Using Medical Biology Tests. 2018. Available online: https://www.legifrance.gouv.fr/eli/ar-725rete/2018/2/22/SSAS1805078A/jo/texte (accessed on 12 October 2019).
- Ministry of Solidarity and Health. Order of November 12, 2020 Amending the Order of February 22, 2018 Regarding the Organization of the National Program for Neonatal Screening Using Medical Biology Tests. 2020. Available online: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000042572858/ (accessed on 21 February 2021).
- French Parliament. Public Health Code—Article L1111-4; 2016; Volume L1111-4, Available online: https://www.legifrance.gouv.fr/codes/article_lc/LEGIARTI000006687659/2016-01-26/ (accessed on 6 February 2020).
- National Coordination of Neonatal Screening Center Leaflet “3 Days, the Age of Screening”. Available online: https://depistage-neonatal.fr/wp-content/uploads/2021/04/J3-depistage.pdf (accessed on 12 January 2021).
- French Parliament. Public Health Code—Article R1131-4; 2016; Volume R1131-4, Available online: https://www.le-733gifrance.gouv.fr/codes/article_lc/LEGIARTI000019579733/ (accessed on 6 February 2020).
- The AAP Newborn Screening Task Force. Illinois Serving the Family From Birth to the Medical Home: Newborn Screening: A Blueprint for the Future—A Call for a National Agenda on State Newborn Screening Programs. Pediatrics 2000, 106, 389–422. [Google Scholar]
- Ulph, F.; Wright, S.; Dharni, N.; Payne, K.; Bennett, R.; Roberts, S.; Lavender, T.; Walshe, K. Provision of Information about Newborn Screening Antenatally: A Sequential Exploratory Mixed-Methods Project. Health Technol. Assess. 2017, 21, 9–55. [Google Scholar] [CrossRef] [PubMed]
- Hargreaves, K.M.; Stewart, R.J.; Oliver, S.R. Informed Choice and Public Health Screening for Children: The Case of Blood Spot Screening. Health Expect. 2005, 8, 161–171. [Google Scholar] [CrossRef]
- Araia, M.H.; Wilson, B.J.; Chakraborty, P.; Gall, K.; Honeywell, C.; Milburn, J.; Ramsay, T.; Potter, B.K. Factors Associated with Knowledge of and Satisfaction with Newborn Screening Education: A Survey of Mothers. Genet. Med. 2012, 14, 963–970. [Google Scholar] [CrossRef]
- Moody, L.; Choudhry, K. Parental Views on Informed Consent for Expanded Newborn Screening. Health Expect. Int. J. Public Particip. Health Care Health Policy 2013, 16, 239–250. [Google Scholar] [CrossRef]
- Nicholls, S.G.; Southern, K.W. Parental Information Use in the Context of Newborn Bloodspot Screening. An Exploratory Mixed Methods Study. J. Community Genet. 2012, 3, 251–257. [Google Scholar] [CrossRef]
- Davis, T.C.; Humiston, S.G.; Arnold, C.L.; Bocchini, J.A.; Bass, P.F.; Kennen, E.M.; Bocchini, A.; Kyler, P.; Lloyd-Puryear, M. Recommendations for Effective Newborn Screening Communication: Results of Focus Groups with Parents, Providers, and Experts. Pediatrics 2006, 117, S326–S340. [Google Scholar] [CrossRef]
- Tluczek, A.; Orland, K.M.; Nick, S.W.; Brown, R.L. Newborn Screening: An Appeal for Improved Parent Education. J. Perinat. Neonatal Nurs. 2009, 23, 326–334. [Google Scholar] [CrossRef]
- Nicholls, S.G. Proceduralisation, Choice and Parental Reflections on Decisions to Accept Newborn Bloodspot Screening. J. Med. Ethics 2012, 38, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.G.; Southern, K.W. Parental Decision-Making and Acceptance of Newborn Bloodspot Screening: An Exploratory Study. PLoS ONE 2013, 8, e79441. [Google Scholar] [CrossRef] [PubMed]
- Etchegary, H.; Nicholls, S.G.; Tessier, L.; Simmonds, C.; Potter, B.K.; Brehaut, J.C.; Pullman, D.; Hayeems, R.; Zelenietz, S.; Lamoureux, M.; et al. Consent for Newborn Screening: Parents’ and Health-Care Professionals’ Experiences of Consent in Practice. Eur. J. Hum. Genet. 2016, 24, 1530–1534. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.G.; Southern, K.W. Informed Choice for Newborn Blood Spot Screening in the United Kingdom: A Survey of Parental Perceptions. Pediatrics 2012, 130, e1527–e1533. [Google Scholar] [CrossRef] [PubMed]
- Hewlett, J.; Waisbren, S.E. A Review of the Psychosocial Effects of False-Positive Results on Parents and Current Communication Practices in Newborn Screening. J. Inherit. Metab. Dis. 2006, 29, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Gurian, E.A.; Kinnamon, D.D.; Henry, J.J.; Waisbren, S.E. Expanded Newborn Screening for Biochemical Disorders: The Effect of a False-Positive Result. Pediatrics 2006, 117, 1915–1921. [Google Scholar] [CrossRef]
- Sorenson, J.R.; Levy, H.L.; Mangione, T.W.; Sepe, S.J. Parental Response to Repeat Testing of Infants with ‘False-Positive’ Results in a Newborn Screening Program. Pediatrics 1984, 73, 183–187. [Google Scholar] [CrossRef]
- van der Burg, S.; Verweij, M. Maintaining Trust in Newborn Screening. Hastings Cent. Rep. 2012, 42, 41–47. [Google Scholar] [CrossRef]
- Hamers, F.F. Prior Assessment of Expanding Neonatal Screening to One or More Inborn Errors of Metabolism Using Tandem Mass Spectrometry in the General Population in France; The French National Authority for Health, HAS: Saint-Denis la Plaine, France, 2009; p. 62. Available online: https://www.has-sante.fr/upload/docs/application/pdf/2009-12/cadrage_spectro_msms_vf_2009-12-22_14-50-77222_231.pdf (accessed on 13 July 2019).
- Vailly, J.; Ensellem, C. Consent to Neonatal Screening or the Ambiguous Subjects of Genetics. Public Reason. 2012. Available online: https://www.raison-publique.fr/article528.html (accessed on 21 February 2021).
- Bellamy, V. The 784,000 Births in 2016 Took Place in 2800 Municipalities. Available online: https://www.insee.fr/fr/statistiques/3047024 (accessed on 22 November 2021).
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups. Int. J. Qual. Health Care J. Int. Soc. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Stewart, R.; Oliver, S.; Hagreaves, K. Telling Parents about the Heel-Prick Test: Consultation Results and Resources Development; UK Newborn Screening Programme Centre: London, UK, 2004; pp. 1–47.
- Nicholls, S.G.; Etchegary, H.; Tessier, L.; Simmonds, C.; Potter, B.K.; Brehaut, J.C.; Pullman, D.; Hayeems, R.Z.; Zelenietz, S.; Lamoureux, M.; et al. What Is in a Name? Parent, Professional and Policy-Maker Conceptions of Consent-Related Language in the Context of Newborn Screening. Public Health Ethics 2019, 12, 158–175. [Google Scholar] [CrossRef] [PubMed]
- Helgesson, G.; Swartling, U. Views on Data Use, Confidentiality and Consent in a Predictive Screening Involving Children. J. Med. Ethics 2008, 34, 206–209. [Google Scholar] [CrossRef] [PubMed]
- Fagot-Largeault, A. The Bioethical Human: Toward a Deontology of Research on Living Beings; Maloine: Paris, France, 1985; ISBN 978-2-224-01056-0. [Google Scholar]
- Dhondt, J.-L. Implementation of Informed Consent for a Cystic Fibrosis Newborn Screening Program in France: Low Refusal Rates for Optional Testing. J. Pediatr. 2005, 147, S106–S108. [Google Scholar] [CrossRef] [PubMed]
- Liebl, B.; Nennstiel-Ratzel, U.; von Kries, R.; Fingerhut, R.; Olgemöller, B.; Zapf, A.; Roscher, A.A. Very High Compliance in an Expanded MS-MS-Based Newborn Screening Program despite Written Parental Consent. Prev. Med. 2002, 34, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Holtzman, N.A.; Faden, R.; Chwalow, A.J.; Horn, S.D. Effect of Informed Parental Consent on Mothers’ Knowledge of Newborn Screening. Pediatrics 1983, 72, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Cooke, R.W.I. Good Practice in Consent. Semin. Fetal. Neonatal Med. 2005, 10, 63–71. [Google Scholar] [CrossRef] [PubMed]
- French Association for the Screening and Prevention of Childhood Disabilities Practical Guidelines for Health Professionals—Newborn Screening 2017. Available online: https://chu-martinique.manuelprelevement.fr/DocumentNew.aspx?idDoc=14439& (accessed on 21 February 2021).
- ISNS. Statements as Agreed at the Third International Society for Neonatal Scrrening European Regional Meeting; ISNS: Sevilla, Spain, 2004. [Google Scholar]
- ACOG Committee Opinion No. 778: Newborn Screening and the Role of the Obstetrician-Gynecologist. Obstet. Gynecol. 2019, 133, e357–e361. [CrossRef]
- Campbell, E.D.; Ross, L.F. Incorporating Newborn Screening into Prenatal Care. Am. J. Obstet. Gynecol. 2004, 190, 876–877. [Google Scholar] [CrossRef] [PubMed]
- Clayton, E.W. Talking with Parents before Newborn Screening. J. Pediatr. 2005, 147, S26–S29. [Google Scholar] [CrossRef]
- Araia, M.H.; Potter, B.K. Newborn Screening Education on the Internet: A Content Analysis of North American Newborn Screening Program Websites. J. Community Genet. 2011, 2, 127–134. [Google Scholar] [CrossRef]

| Characteristics | Number (%) | Minimum/Maximum | Standard Deviation |
|---|---|---|---|
| Parent | 27 (100%) | ||
| Father | 8 (29.6%) | ||
| Mother | 19 (70.3%) | ||
| First-time parent | 16 (59.3%) | ||
| The mean age of parents (years) | 33.04 | 25/45 | 5.192 |
| Health-related profession | 5 (18.5%) | ||
| Maternity | |||
| Public hospital | 19 (70.4%) | ||
| Levels of neonatal care * | |||
| 1 | 0 (0%) | ||
| 2A | 12 (44.4%) | ||
| 2B | 2 (7.4%) | ||
| 3 | 13 (48%) | ||
| Newborn | 20 (100%) | ||
| Newborn hospitalization | 8 (29.6%) | ||
| The mean age of children at the interview (months) | 3.65 | 2/5 | 1.45 |
| True Positive | 4 (20%) | ||
| Congenital hypothyroidism confirmed | 2 | ||
| Cystic fibrosis confirmed | 2 | ||
| False Positive | 16 (80%) | ||
| Congenital adrenal hyperplasia suspected | 5 | ||
| Congenital hypothyroidism suspected ** | 6 | ||
| Cystic fibrosis suspected ** | 5 | ||
| Phenylketonuria suspected | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinel, J.; Bellanger, A.; Jamet, C.; Moreau, C. Information and Parental Consent for French Neonatal Screening: A Qualitative Study on Parental Opinion. Int. J. Neonatal Screen. 2023, 9, 26. https://doi.org/10.3390/ijns9020026
Pinel J, Bellanger A, Jamet C, Moreau C. Information and Parental Consent for French Neonatal Screening: A Qualitative Study on Parental Opinion. International Journal of Neonatal Screening. 2023; 9(2):26. https://doi.org/10.3390/ijns9020026
Chicago/Turabian StylePinel, Julia, Amandine Bellanger, Carole Jamet, and Caroline Moreau. 2023. "Information and Parental Consent for French Neonatal Screening: A Qualitative Study on Parental Opinion" International Journal of Neonatal Screening 9, no. 2: 26. https://doi.org/10.3390/ijns9020026