
Droplet Digital PCR (ddPCR) Does Not Enhance the Sensitivity of Detection of Cytomegalovirus (CMV) DNA in Newborn Dried Blood Spots Evaluated in the Context of Newborn Congenital CMV (cCMV) Screening

Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Samples
2.2. DNA Extraction
2.3. Viral Load Determination by qPCR
2.4. Viral Load Determination by ddPCR
3. Results
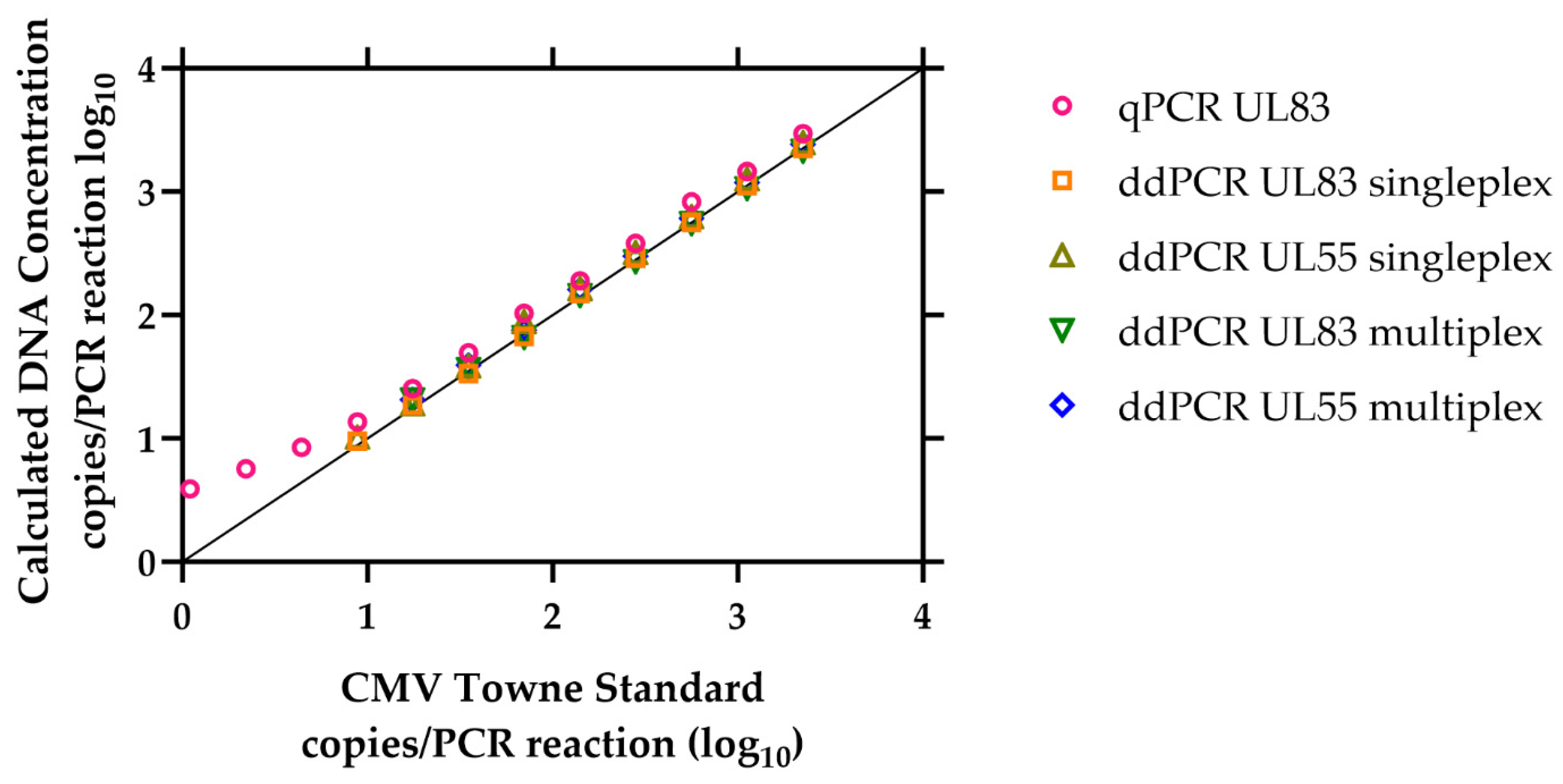
3.1. Limit of Detection of the ddPCR Assay
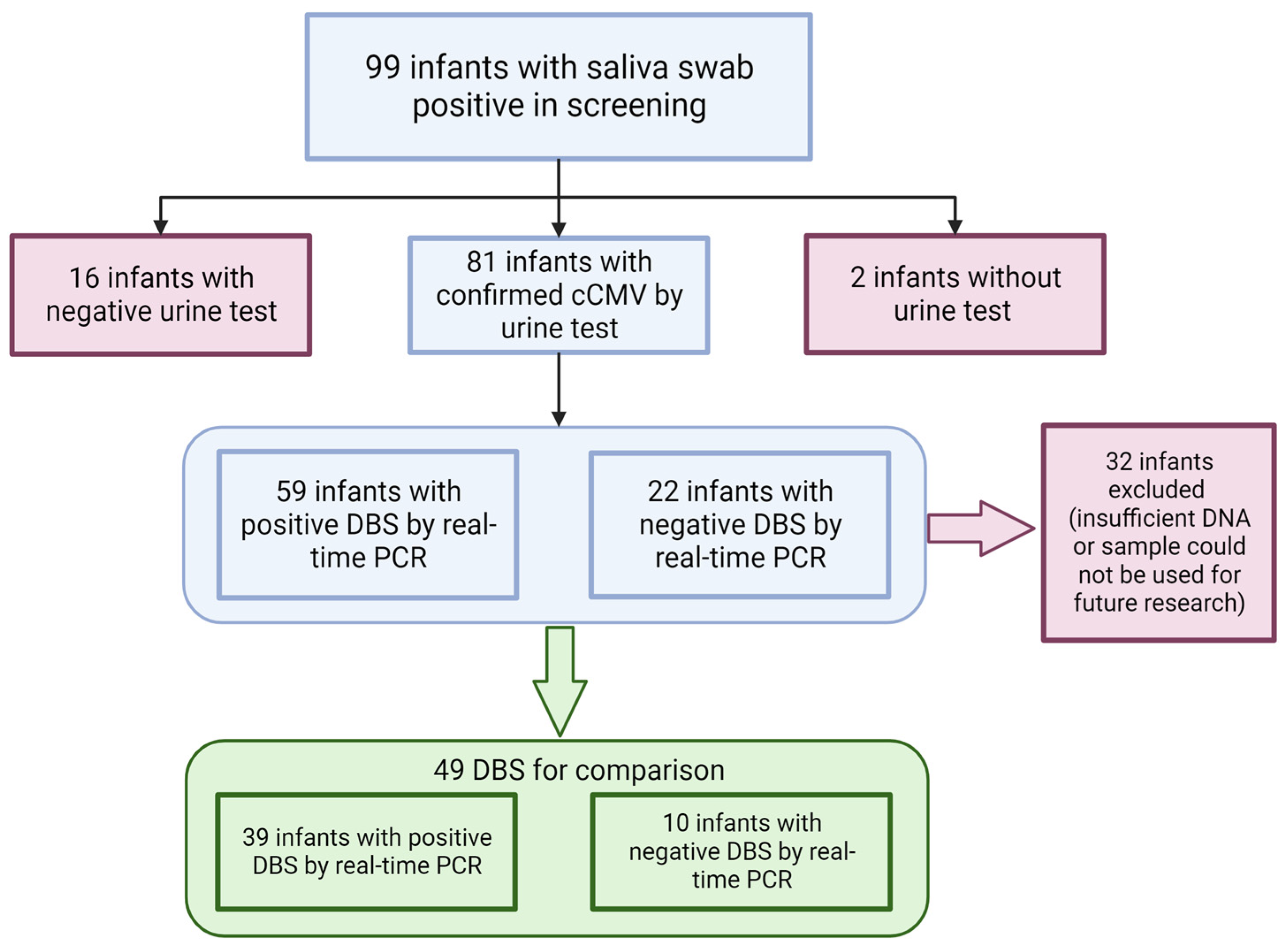
3.2. Clinical Samples
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dollard, S.C.; Grosse, S.D.; Ross, D.S. New Estimates of the Prevalence of Neurological and Sensory Sequelae and Mortality Associated with Congenital Cytomegalovirus Infection. Rev. Med. Virol. 2007, 17, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Rawlinson, W.D.; Boppana, S.B.; Fowler, K.B.; Kimberlin, D.W.; Lazzarotto, T.; Alain, S.; Daly, K.; Doutré, S.; Gibson, L.; Giles, M.L.; et al. Congenital Cytomegalovirus Infection in Pregnancy and the Neonate: Consensus Recommendations for Prevention, Diagnosis, and Therapy. Lancet Infect. Dis. 2017, 17, e177–e188. [Google Scholar] [CrossRef] [PubMed]
- Ross, S.A.; Ahmed, A.; Palmer, A.L.; Michaels, M.G.; Sánchez, P.J.; Bernstein, D.I.; Tolan, R.W.; Novak, Z.; Chowdhury, N.; Fowler, K.B.; et al. Detection of Congenital Cytomegalovirus Infection by Real-Time Polymerase Chain Reaction Analysis of Saliva or Urine Specimens. J. Infect. Dis. 2014, 210, 1415–1418. [Google Scholar] [CrossRef] [PubMed]
- Dollard, S.C.; Schleiss, M.R.; Grosse, S.D. Public Health and Laboratory Considerations Regarding Newborn Screening for Congenital Cytomegalovirus. J. Inherit. Metab. Dis. 2010, 33, S249–S254. [Google Scholar] [CrossRef] [PubMed]
- Diener, M.L.; Zick, C.D.; McVicar, S.B.; Boettger, J.; Park, A.H. Outcomes from a Hearing-Targeted Cytomegalovirus Screening Program. Pediatrics 2017, 139, e20160789. [Google Scholar] [CrossRef] [PubMed]
- Congenital Cytomegalovirus. CHEO NSO. Available online: https://www.newbornscreening.on.ca/en/page/congenital-cytomegalovirus (accessed on 4 December 2023).
- Minnesota Becomes First State to Screen All Newborns for Congenital Cytomegalovirus—MN Department of Health. Available online: https://www.health.state.mn.us/news/pressrel/2023/ccmv020823.html (accessed on 4 December 2023).
- Sedlak, R.H.; Cook, L.; Cheng, A.; Magaret, A.; Jerome, K.R. Clinical Utility of Droplet Digital PCR for Human Cytomegalovirus. J. Clin. Microbiol. 2014, 52, 2844–2848. [Google Scholar] [CrossRef] [PubMed]
- Hindson, B.J.; Ness, K.D.; Masquelier, D.A.; Belgrader, P.; Heredia, N.J.; Makarewicz, A.J.; Bright, I.J.; Lucero, M.Y.; Hiddessen, A.L.; Legler, T.C.; et al. High-Throughput Droplet Digital PCR System for Absolute Quantitation of DNA Copy Number. Anal. Chem. 2011, 83, 8604–8610. [Google Scholar] [CrossRef]
- Pinheiro, L.B.; Coleman, V.A.; Hindson, C.M.; Herrmann, J.; Hindson, B.J.; Bhat, S.; Emslie, K.R. Evaluation of a Droplet Digital Polymerase Chain Reaction Format for DNA Copy Number Quantification. Anal. Chem. 2012, 84, 1003–1011. [Google Scholar] [CrossRef]
- Xu, L.; Zhang, X.; Cao, Y.; Fan, Z.; Tian, Y.; Zou, H.; Ma, Y.; Duan, Z.; Ren, F. Digital Droplet PCR for Detection and Quantitation of Hepatitis Delta Virus. Clin. Transl. Gastroenterol. 2022, 13, e00509. [Google Scholar] [CrossRef]
- Mattox, A.K.; D’Souza, G.; Khan, Z.; Allen, H.; Henson, S.; Seiwert, T.Y.; Koch, W.; Pardoll, D.M.; Fakhry, C. Comparison of next Generation Sequencing, Droplet Digital PCR, and Quantitative Real-Time PCR for the Earlier Detection and Quantification of HPV in HPV-Positive Oropharyngeal Cancer. Oral Oncol. 2022, 128, 105805. [Google Scholar] [CrossRef]
- Vasudevan, H.N.; Xu, P.; Servellita, V.; Miller, S.; Liu, L.; Gopez, A.; Chiu, C.Y.; Abate, A.R. Digital Droplet PCR Accurately Quantifies SARS-CoV-2 Viral Load from Crude Lysate without Nucleic Acid Purification. Sci. Rep. 2021, 11, 780. [Google Scholar] [CrossRef] [PubMed]
- Hayden, R.T.; Gu, Z.; Ingersoll, J.; Abdul-Ali, D.; Shi, L.; Pounds, S.; Caliendo, A.M. Comparison of Droplet Digital PCR to Real-Time PCR for Quantitative Detection of Cytomegalovirus. J. Clin. Microbiol. 2013, 51, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Pavšič, J.; Žel, J.; Milavec, M. Assessment of the Real-Time PCR and Different Digital PCR Platforms for DNA Quantification. Anal. Bioanal. Chem. 2016, 408, 107–121. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Bream, J.H.; Leng, S.X.; Margolick, J.B. Validation of Preamplification to Improve Quantification of Cytomegalovirus DNA Using Droplet Digital Polymerase Chain Reaction. Anal. Chem. 2021, 93, 3710–3716. [Google Scholar] [CrossRef] [PubMed]
- Hema, M.; Konakalla, N.C. Chapter 16—Recent Developments in Detection and Diagnosis of Plant Viruses. In Recent Developments in Applied Microbiology and Biochemistry; Viswanath, B., Ed.; Academic Press: Cambridge, MA, USA, 2021; pp. 163–180. ISBN 978-0-12-821406-0. [Google Scholar]
- Dollard, S.C.; Dreon, M.; Hernandez-Alvarado, N.; Amin, M.M.; Wong, P.; Lanzieri, T.M.; Osterholm, E.A.; Sidebottom, A.; Rosendahl, S.; McCann, M.T.; et al. Sensitivity of Dried Blood Spot Testing for Detection of Congenital Cytomegalovirus Infection. JAMA Pediatr. 2021, 175, e205441. [Google Scholar] [CrossRef]
- Meyer, L.; Sharon, B.; Huang, T.C.; Meyer, A.C.; Gravel, K.E.; Schimmenti, L.A.; Swanson, E.C.; Herd, H.E.; Hernandez-Alvarado, N.; Coverstone, K.R.; et al. Analysis of Archived Newborn Dried Blood Spots (DBS) Identifies Congenital Cytomegalovirus as a Major Cause of Unexplained Pediatric Sensorineural Hearing Loss. Am. J. Otolaryngol. 2017, 38, 565–570. [Google Scholar] [CrossRef]
- Haynes, R.J.; Kline, M.C.; Toman, B.; Scott, C.; Wallace, P.; Butler, J.M.; Holden, M.J. Standard Reference Material 2366 for Measurement of Human Cytomegalovirus DNA. J. Mol. Diagn. JMD 2013, 15, 177–185. [Google Scholar] [CrossRef]
- Forootan, A.; Sjöback, R.; Björkman, J.; Sjögreen, B.; Linz, L.; Kubista, M. Methods to Determine Limit of Detection and Limit of Quantification in Quantitative Real-Time PCR (QPCR). Biomol. Detect. Quantif. 2017, 12, 1–6. [Google Scholar] [CrossRef]
- JCGM (Organization). International Vocabulary of Metrology: Basic and General Concepts and Associated Terms (Vim) = Vocabulaire International de Métrologie: Concepts Fondamentaux et Généraux et Termes Associés (Vim). 2012, 3rd edition 2008 Version with Minor Corrections ed. Paris France: BIPM Bureau International des Poids et Mesures. Available online: http://www.bipm.org/en/publications/guides/vim.html (accessed on 17 December 2023).
- Strain, M.C.; Lada, S.M.; Luong, T.; Rought, S.E.; Gianella, S.; Terry, V.H.; Spina, C.A.; Woelk, C.H.; Richman, D.D. Highly Precise Measurement of HIV DNA by Droplet Digital PCR. PLoS ONE 2013, 8, e55943. [Google Scholar] [CrossRef]
- Renzette, N.; Pokalyuk, C.; Gibson, L.; Bhattacharjee, B.; Schleiss, M.R.; Hamprecht, K.; Yamamoto, A.Y.; Mussi-Pinhata, M.M.; Britt, W.J.; Jensen, J.D.; et al. Limits and patterns of cytomegalovirus genomic diversity in humans. Proc. Natl. Acad. Sci. USA 2015, 112, E4120–E4128. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Kawada, J.-I.; Torii, Y.; Haruta, K.; Suzuki, T.; Horiba, K.; Takahashi, Y.; Ito, Y. Quantitative Assessment of Viral Load in the Blood and Urine of Patients with Congenital Cytomegalovirus Infection Using Droplet Digital PCR. J. Med. Virol. 2022, 94, 4559–4564. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Robles, V.; Weimer, K.E.D.; Gehtland, L.M.; Kucera, K.S. Improved Dried Blood Spot PCR Assay for Universal Congenital Cytomegalovirus Screening in Newborns. Microbiol. Spectr. 2023, 11, e04041-22. [Google Scholar] [CrossRef] [PubMed]
- Vidal-Folch, N.; Guenzel, A.; Espy, M.; Sattler, C.; White, A.; Peck, D.; Bentz Pino, G.; Studinski, A.; Matern, D.; Binnicker, M.; et al. Newborn Screening for Cytomegalovirus in Dried Blood Spots Using a Novel Quantitative Droplet Digital PCR Assay. In Proceedings of the APHL 2021 Newborn Screening Virtual Symposium, Virtual, 5–21 October 2021. [Google Scholar]
- Boppana, S.B.; Ross, S.A.; Novak, Z.; Shimamura, M.; Tolan, R.W., Jr.; Palmer, A.L.; Ahmed, A.; Michaels, M.G.; Sánchez, P.J.; Bernstein, D.I.; et al. Dried blood spot real-time polymerase chain reaction assays to screen newborns for congenital cytomegalovirus infection. JAMA 2010, 303, 1375–1382. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.M.; Wong, P.; McCann, M.; Dollard, S.C. Detection of Cytomegalovirus in Urine Dried on Filter Paper. J. Pediatr. Infect. Dis. Soc. 2021, 10, 958–961. [Google Scholar] [CrossRef]
- Fujii, T.; Oka, A.; Morioka, I.; Moriuchi, H.; Koyano, S.; Yamada, H.; Saito, S.; Sameshima, H.; Nagamatsu, T.; Tsuchida, S.; et al. Newborn Congenital Cytomegalovirus Screening Based on Clinical Manifestations and Evaluation of DNA-Based Assays for In Vitro Diagnostics. Pediatr. Infect. Dis. J. 2017, 36, 942. [Google Scholar] [CrossRef]
- Nagano, N.; Imaizumi, T.; Akimoto, T.; Hijikata, M.; Aoki, R.; Seimiya, A.; Okahashi, A.; Kawakami, K.; Komatsu, A.; Kawana, K.; et al. Clinical Evaluation of a Novel Urine Collection Kit Using Filter Paper in Neonates: An Observational Study. Children 2021, 8, 561. [Google Scholar] [CrossRef]
- Wunderlich, W.; Sidebottom, A.C.; Schulte, A.K.; Taghon, J.; Dollard, S.; Hernandez-Alvarado, N. The Use of Saliva Samples to Test for Congenital Cytomegalovirus Infection in Newborns: Examination of False-Positive Samples Associated with Donor Milk Use. Int. J. Neonatal Screen. 2023, 9, 46. [Google Scholar] [CrossRef]
- Chiereghin, A.; Pavia, C.; Turello, G.; Borgatti, E.C.; Baiesi Pillastrini, F.; Gabrielli, L.; Gibertoni, D.; Marsico, C.; De Paschale, M.; Manco, M.T.; et al. Universal Newborn Screening for Congenital Cytomegalovirus Infection—From Infant to Maternal Infection: A Prospective Multicenter Study. Front. Pediatr. 2022, 10, 909646. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Gene | Primer/Probe | Sequence | Final Concentration | |
|---|---|---|---|---|
| qPCR | ddPCR | |||
| UL83 | Forward | GGA CAC AAC ACC GTA AAG C | 0.4 μM | 0.9 µM |
| Reverse | GTC AGC GTT CGT GTT TCC CA | 0.4 μM | 0.9 µM | |
| Probe | FAM-CCC GCA ACC CGC AAC CCT TCA T-BHQ1 | 0.250 µM | ||
| Probe | CAL610-CCC GCA ACC CGC AAC CCT TCA T-BHQ2 | 0.1 μM | ||
| NRAS | Forward | GCC AAC AAG GAC AGT TGA TAC AAA | 0.4 μM | |
| Reverse | GGC TGA GGT TTC AAT GAA TGG AA | 0.4 μM | ||
| Probe | FAM-ACA AGC CCA CGG AAC TGG CCA AGA-BHQ1 | 0.1 μM | ||
| UL55 | Forward | TGG GCG AGG ACA ACG AA | 0.9 µM | |
| Reverse | TGA GGC TGG GAA GCT GAC AT | 0.9 µM | ||
| Probe | HEX-TGG GCA ACC ACC GCA CTG AGG-BHQ1 | 0.250 µM | ||
| Towne Dilution (Copies/PCR Reaction) | Real-Time UL83 | ddPCR UL83 Singleplex | ddPCR UL55 Singleplex | ddPCR UL83 Multiplex | ddPCR UL55 Multiplex | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Tests | Copies/Reaction | Tests | Copies/Reaction | Tests | Copies/Reaction | Tests | Copies/Reaction | Tests | Copies/Reaction | |
| 2245.0 | 20/20 | 2965.0 | 20/20 | 2252.1 | 20/20 | 2476.9 | 20/20 | 2150.3 | 20/20 | 2423.8 |
| 1122.5 | 20/20 | 1463.1 | 20/20 | 1121.8 | 20/20 | 1262.5 | 20/20 | 1065.8 | 20/20 | 1191.6 |
| 561.3 | 20/20 | 827.4 | 20/20 | 562.8 | 20/20 | 622.0 | 20/20 | 555.9 | 20/20 | 608.3 |
| 280.6 | 20/20 | 381.4 | 20/20 | 289.9 | 20/20 | 321.0 | 20/20 | 272.4 | 20/20 | 300.7 |
| 140.3 | 20/20 | 189.8 | 20/20 | 149.1 | 20/20 | 162.9 | 20/20 | 145.4 | 20/20 | 161.7 |
| 70.2 | 20/20 | 103.2 | 20/20 | 67.5 | 20/20 | 88.2 | 20/20 | 66.1 | 20/20 | 75.7 |
| 35.1 | 20/20 | 49.6 | 20/20 | 33.6 | 20/20 | 38.5 | 20/20 | 36.4 | 20/20 | 39.5 |
| 17.5 | 20/20 | 25.4 | 20/20 | 18.6 | 20/20 | 19.0 | 20/20 | 20.7 | 20/20 | 20.7 |
| 8.8 | 20/20 | 13.6 | 19/20 | 9.5 | 20/20 | 10.2 | 18/20 | 10.2 | 18/20 | 10.2 |
| 4.4 | 20/20 | 8.5 | 17/20 | 5.8 | 12/20 | 5.1 | 17/20 | 5.2 | 16/20 | 6.7 |
| 2.2 | 20/20 | 5.7 | 8/20 | 4.1 | 6/20 | 4.8 | 9/20 | 3.9 | 5/20 | 4.0 |
| 1.1 | 19/20 | 3.9 | 3/20 | 4.5 | 2/20 | 5.1 | 3/20 | 3.9 | 2/20 | 3.3 |
| 0.5 | 6/20 | 3.2 | 2/20 | 3.3 | 0/20 | - | 0/20 | - | 1/20 | 3.2 |
| 0.3 | 4/20 | 2.1 | 1/20 | 3.4 | 0/20 | - | 0/20 | - | 2/20 | 3.3 |
| Real-Time PCR | Multiplex ddPCR | Singleplex ddPCR | |||
|---|---|---|---|---|---|
| Sample Number | UL83-Red610 (Copies/PCR Reaction) | UL83-FAM (Copies/PCR Reaction) | UL55-HEX (Copies/PCR Reaction) | UL83-FAM (Copies/PCR Reaction) | UL55-HEX (Copies/PCR Reaction) |
| 1 | ND | ND | ND | ND | ND |
| 2 | ND | ND | ND | ND | ND |
| 3 | ND | ND | ND | ND | ND |
| 4 | ND | ND | ND | ND | ND |
| 5 | 11.3 | ND | 3.5 | ND | ND |
| 6 | ND | ND | ND | ND | ND |
| 7 | ND | ND | ND | ND | ND |
| 8 | ND | ND | ND | ND | ND |
| 9 | ND | ND | ND | ND | ND |
| 10 | 1630 | 72.8 | 145.5 | 28.3 | 113.5 |
| 11 | 7.2 | ND | ND | ND | ND |
| 12 | ND | ND | ND | ND | ND |
| 13 | 35.5 | ND | ND | 3.1 | 5.2 |
| 14 | 1.5 | 4.8 | 6.4 | 3.1 | 9.9 |
| 15 | ND | ND | ND | ND | ND |
| 16 | 17.7 | 8.3 | 6.7 | 15 | 16.9 |
| 17 | ND | ND | ND | ND | ND |
| 18 | 1.5 | 6 | 14.9 | 11.4 | 13.4 |
| 19 | ND | ND | ND | ND | ND |
| 20 | 1.6 | 3.2 | 9.6 | 3 | 8.1 |
| 21 | ND | ND | ND | ND | ND |
| 22 | 1.4 | 4.5 | 26.8 | 3.4 | 12.9 |
| 23 | ND | ND | ND | ND | ND |
| 24 | ND | ND | ND | ND | ND |
| 25 | ND | ND | ND | ND | ND |
| 26 | ND | ND | ND | ND | ND |
| 27 | ND | ND | ND | ND | ND |
| 28 | ND | ND | ND | ND | ND |
| 29 | 1.5 | ND | ND | ND | ND |
| Real-Time PCR UL83 | ddPCR UL55 | |||
| Positive | Negative | Total | ||
| Positive | 29 | 10 | 39 | |
| Negative | 0 | 10 | 10 | |
| Total | 29 | 20 | 49 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernandez-Alvarado, N.; Bierle, C.J.; Schleiss, M.R. Droplet Digital PCR (ddPCR) Does Not Enhance the Sensitivity of Detection of Cytomegalovirus (CMV) DNA in Newborn Dried Blood Spots Evaluated in the Context of Newborn Congenital CMV (cCMV) Screening. Int. J. Neonatal Screen. 2024, 10, 1. https://doi.org/10.3390/ijns10010001
Hernandez-Alvarado N, Bierle CJ, Schleiss MR. Droplet Digital PCR (ddPCR) Does Not Enhance the Sensitivity of Detection of Cytomegalovirus (CMV) DNA in Newborn Dried Blood Spots Evaluated in the Context of Newborn Congenital CMV (cCMV) Screening. International Journal of Neonatal Screening. 2024; 10(1):1. https://doi.org/10.3390/ijns10010001
Chicago/Turabian StyleHernandez-Alvarado, Nelmary, Craig J. Bierle, and Mark R. Schleiss. 2024. "Droplet Digital PCR (ddPCR) Does Not Enhance the Sensitivity of Detection of Cytomegalovirus (CMV) DNA in Newborn Dried Blood Spots Evaluated in the Context of Newborn Congenital CMV (cCMV) Screening" International Journal of Neonatal Screening 10, no. 1: 1. https://doi.org/10.3390/ijns10010001