
Making CT Dose Monitoring Meaningful: Augmenting Dose with Imaging Quality
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Nature of the Data
- Labels and attributes: study description, protocol name, anatomical region, scanner model, etc.
- Patient data: sex, age, body mass index (BMI), effective diameter, water-equivalent diameter (WED), etc.
2.2. Meaningful Quantities to Monitor
2.2.1. Dose Metrics
2.2.2. Image Quality Metrics
2.2.3. Patient Information, Scanner Parameters, and Operational Factors
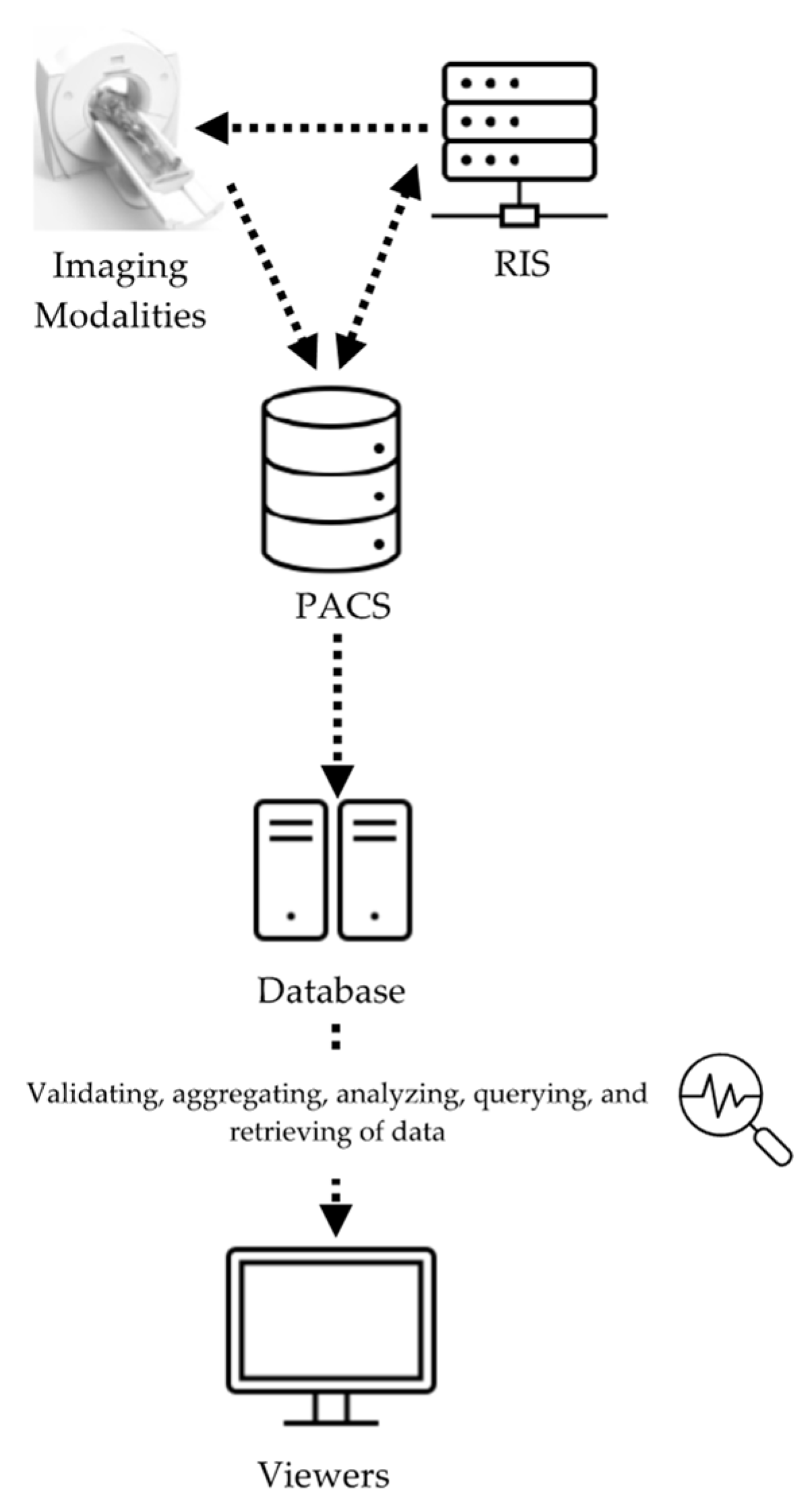
2.3. RDMS Design and Evaluation
2.3.1. RDMS Design
2.3.2. RDMS Interface
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frush, D.; Denham, C.R.; Goske, M.J.; Brink, J.A.; Morin, R.L.; Mills, T.T.; Butler, B.F.; McCollough, C.; Miller, D.L. Radiation protection and dose monitoring in medical imaging: A journey from awareness, through accountability, ability and action...but where will we arrive? J. Patient Saf. 2013, 9, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Schauer, D.A.; Linton, O.W. NCRP Report No. 160, Ionizing Radiation Exposure of the Population of the United States, medical exposure—Are we doing less with more, and is there a role for health physicists? Health Phys. 2009, 97, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Joint Commission. Radiation Risks of Diagnostic Imaging and fluoroscopy. Jt. Comm. Sentin. Event. Alert. 2019, 2019, 1–4. [Google Scholar]
- US Food and Drug Administration. White paper: Initiative to Reduce Unnecessary Radiation Exposure from Medical Imaging. Cent. Devices Radiol. Health. Available online: https://www.fda.gov/radiation-emitting-products/initiative-reduce-unnecessary-radiation-exposure-medical-imaging/white-paper-initiative-reduce-unnecessary-radiation-exposure-medical-imaging (accessed on 28 August 2022).
- Ria, F.; D’Ercole, L.; Origgi, D.; Paruccini, N.; Pierotti, L.; Rampado, O.; Rossetti, V.; Strocchi, S.; Torresin, A.; Association of Medical Physics Task Group. Statement of the Italian Association of Medical Physics (AIFM) task group on radiation dose monitoring systems. Insights Imaging. 2022, 13, 23. [Google Scholar] [CrossRef] [PubMed]
- ICRP. Diagnostic reference levels in medical imaging, ICRP Publication 135. Ann. ICRP. 2017, 46, 1–144. [Google Scholar] [CrossRef] [PubMed]
- Ding, A.; Ria, F.; Samei, E. CT practice monitoring. In Computed Tomography: Approaches, Applications, and Operations, 1st ed.; Samei, E., Pelc, N.J., Eds.; Springer: Cham, Switzerland, 2020; Volume 1, pp. 199–220. [Google Scholar]
- Ria, F.; Fu, W.; Hoye, J.; Segars, W.P.; Kapadia, A.J.; Samei, E. Comparison of 12 surrogates to characterize CT radiation risk across a clinical population. Eur. Radiol. 2021, 31, 7022–7030. [Google Scholar] [CrossRef] [PubMed]
- Frush, D.P.; Samei, E. CT Radiation Dose Monitoring: Current State and New Prospects CME. Medscape. Available online: https://www.medscape.org/viewarticle/839485 (accessed on 28 August 2022).
- McCollough, C.H.; Primak, A.N.; Braun, N.; Kofler, J.; Yu, L.; Christner, J. Strategies for reducing radiation dose in CT. Radiol. Clin. North. Am. 2009, 47, 27–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, W.; Ria, F.; Segars, W.P.; Choudhury, K.R.; Wilson, J.M.; Kapadia, A.J.; Samei, E. Patient-informed organ dose estimation in clinical CT: Implementation and effective dose assessment in 1048 clinical patients. Am. J. Roentgenol. 2021, 216, 824–834. [Google Scholar] [CrossRef] [PubMed]
- McCollough, C.; Cody, D.; Edyvean, S.; Geise, R.; Gould, B.; Keat, N.; Huda, W.; Judy, P.; Kalender, W.; McNitt Gray, M.; et al. AAPM Report n.96. The Measurement, Reporting, and Management of Radiation Dose in CT; American Association of Physicists in Medicine: College Park, MD, USA, 2008; Available online: https://www.aapm.org/pubs/reports/rpt_96.pdf (accessed on 28 August 2022).
- AAPM Report No. 204—Size-Specific Dose Estimates (SSDE) in Pediatric and Adult Body CT Examinations; American Association of Physicists in Medicine: College Park, MD, USA, 2011.
- Sahbaee, P.; Segars, W.P.; Samei, E. Patient-based estimation of organ dose for a population of 58 adult patients across 13 protocol categories. Med. Phys. 2014, 41, 072104. [Google Scholar] [CrossRef] [PubMed]
- ICRP. 2007 Recommendations of the International Commission on Radiological Protection, ICRP Publication 103. Ann. ICRP. 2007, 37, 1–332. [Google Scholar]
- Li, X.; Samei, E.; Segars, W.; Sturgeon, G.; Colsher, J.; Frush, D.P. Patient-specific dose and risk estimation in pediatric chest CT. Radiology 2011, 259, 862–874. [Google Scholar] [CrossRef] [PubMed]
- Christianson, O.; Winslow, J.; Frush, D.P.; Samei, E. Automated technique to measure noise in clinical CT examinations. AJR 2015, 205, W93–W99. [Google Scholar] [CrossRef] [PubMed]
- Abadi, E.; Sanders, J.; Samei, E. Patient-specific quantification of image quality: An automated technique for measuring the distribution of organ Hounsfield units in clinical chest CT images. Med. Phys. 2017, 44, 4736–4746. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.; Hurwitz, L.; Samei, E. Patient-specific quantification of image quality: An automated method for measuring spatial resolution in clinical CT images. Med. Phys. 2016, 43, 5330–5338. [Google Scholar] [CrossRef] [PubMed]
- Kanal, K.M.; Butler, P.F.; Sengupta, D.; Bhargavan-Chatfield, M.; Coombs, L.P.; Morin, R.L. U.S. Diagnostic Reference Levels and Achievable Doses for 10 Adult CT Examinations. Radiology 2017, 284, 120–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ria, F.; Davis, J.T.; Solomon, J.B.; Wilson, J.M.; Smith, T.B.; Frush, D.P.; Samei, E. Expanding the Concept of Diagnostic Reference Levels to Noise and Dose Reference Levels in CT. AJR Am. J. Roentgenol. 2019, 213, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Tsalafoutas, I.A.; Hassan Kharita, M.; Al-Naemi, H.; Kalra, M.K. Radiation dose monitoring in computed tomography: Status, options and limitations. Phys. Med. 2020, 79, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Fitousi, N. Patient dose monitoring systems: A new way of managing patient dose and quality in the radiology department. Phys. Med. 2017, 44, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Samei, E.; Järvinen, H.; Kortesniemi, M.; Simantirakis, G.; Goh, C.; Wallace, A.; Vano, E.; Bejan, A.; Rehani, M.; Vassileva, J. Medical imaging dose optimisation from ground up: Expert opinion of an international summit. J. Radiol. Prot. 2018, 38, 967–989. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.; Liu, X.; Morani, A.C.; Ganeshan, D.; Anderson, M.R.; Samei, E.; Jensen, C.T. Oncology-specific radiation dose and image noise reference levels in adult abdominal-pelvic CT. Clin. Imaging. 2023, 93, 52–59. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Index | Definition | Representing |
|---|---|---|
| CTDIvol | Volume computed tomography dose index | Standardized measure of radiation output of a CT scanner in a specified phantom [12]. |
| DLP | Dose length product | Radiation output of a CT scanner over the length of a scan [12]. |
| SSDE | Size-specific dose estimate | Radiation output of a CT scanner that takes a patient’s attributes of size into account [13]. |
| OD | Organ absorbed dose(s) | Estimated dose absorbed to a specific organ in the body [14]. |
| EOD | Effective dose calculated from the estimated organ doses | Effective dose calculated based on the estimated organ doses of the patient, incorporating organ sensitivities [15]. |
| RI | Risk index | Radiation risk index calculated based on the estimated organ doses of the patient, incorporating weighted sensitivities based on organ, age, and sex [16]. |
| Chart | Description | Question Targeted |
|---|---|---|
| 1 | CTDIvol for patient effective diameter of all CT exams. | Is the administered radiation dose reflective of patient size? |
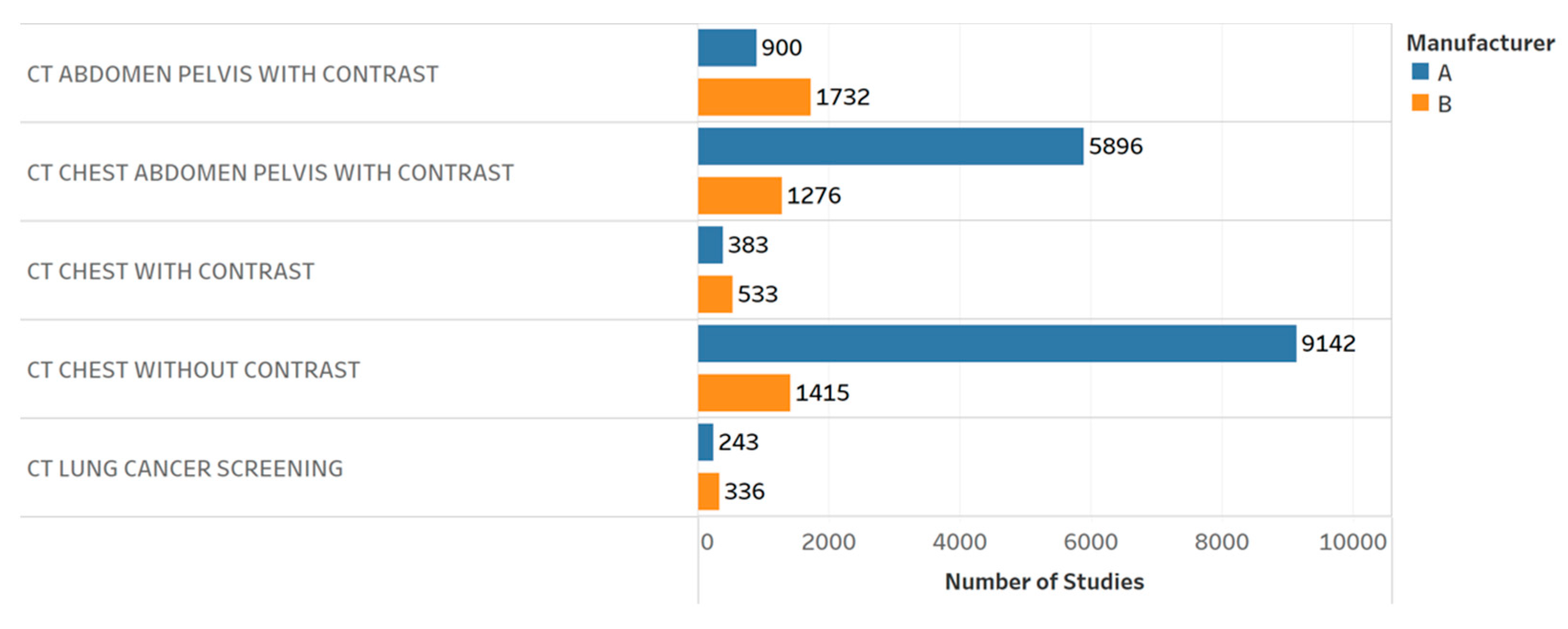
| 2 | Distribution of CT exams by different protocols and manufacturers. | What is the scanners’ workload? |
| 3 | Distribution of the CTDIvol by different protocols, manufacturers, and patient effective diameter. | Is the radiation burden related to different protocols, scanners, and patient size? |
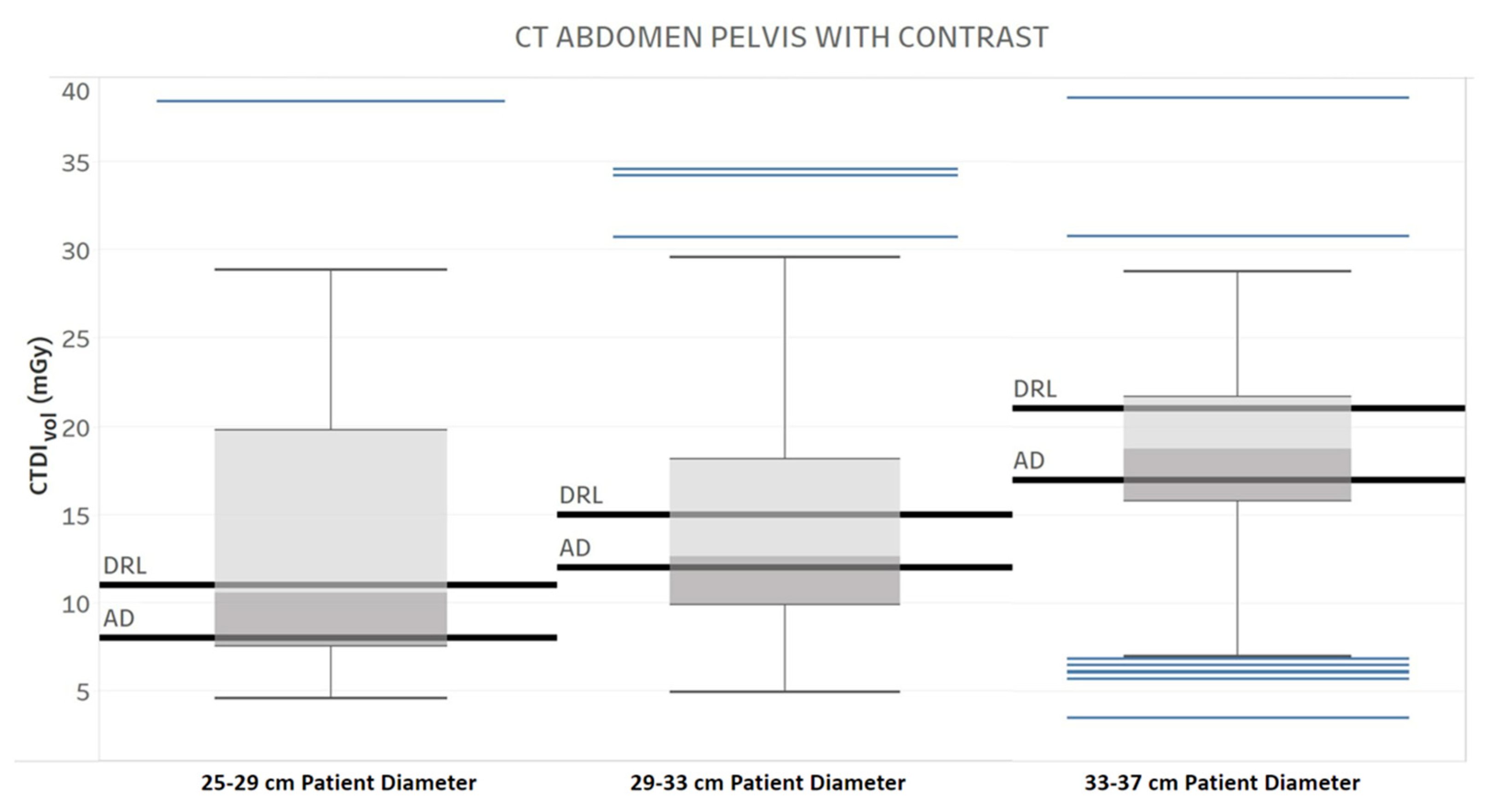
| 4 | Diagnostic reference level (DRL) and achievable dose (AD) for three different patient diameter ranges for one protocol and manufacturer. | How is the radiation output of the scanner compared with the literature and regulatory standards across patient body habitus? [20] |
| 5 | DRL and AD for one protocol and two manufacturers. | How is the radiation output of the scanner compared with the literature and regulatory standards across different scanners? [20] |
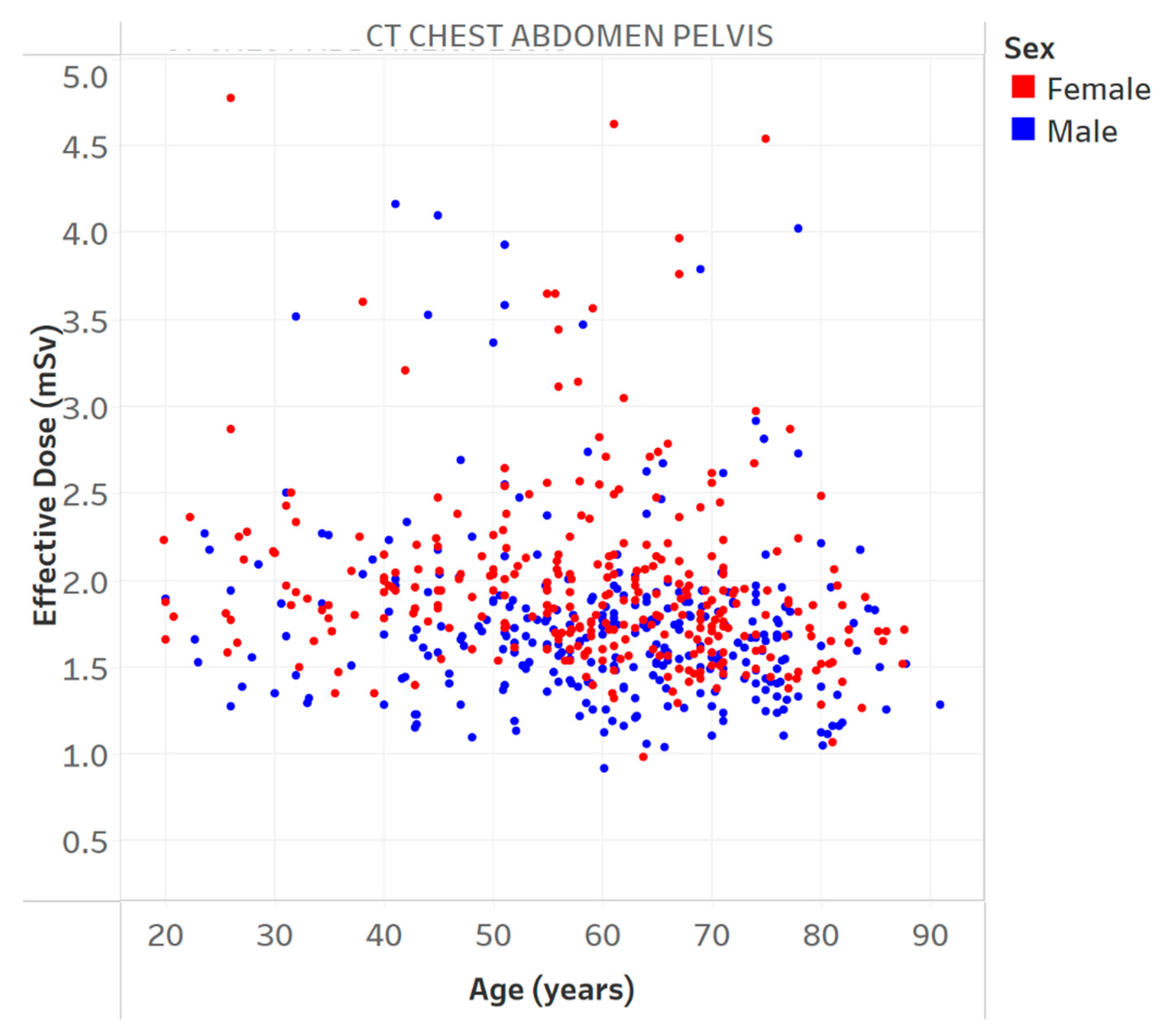
| 6 | Effective dose vs. age for a specific protocol. | Is the effective dose related to patient age? |
| 7 | Distribution of the CTDIvol and effective dose vs. patient diameter for one protocol and one manufacturer. | How are different metrics of the radiation dose related to patient body habitus? |
| 8 | Distribution of noise for different slice thicknesses and CTDIvol vs. patient diameter for one manufacturer across two different protocols. | How does the radiation dose and image quality change with patient size in different protocols and reconstructions? |
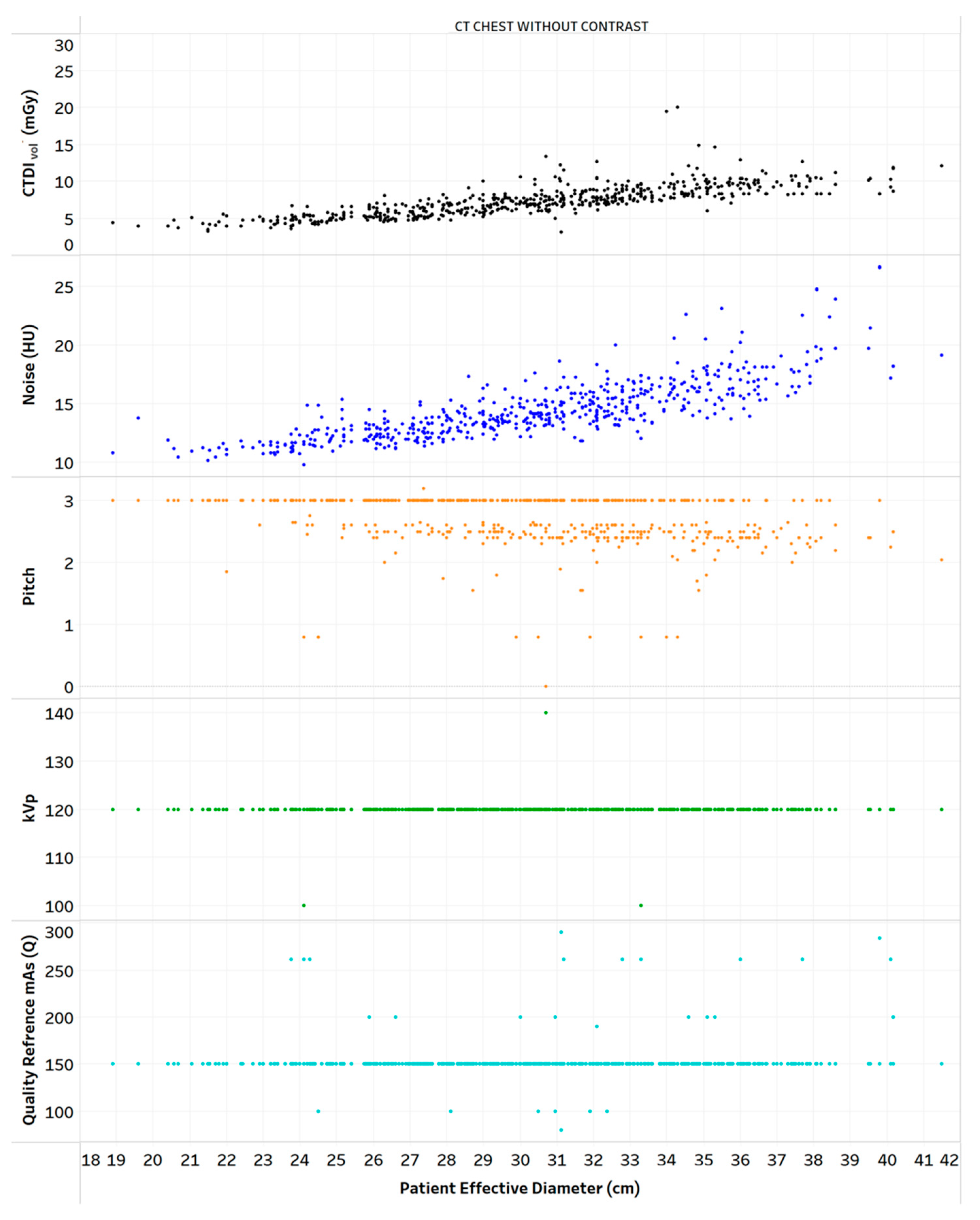
| 9 | Distribution of CTDIvol, noise, and scanning parameters vs. patient diameter for one protocol. | How does the scanner’s parameters affect the radiation dose and image quality in the patient population? |
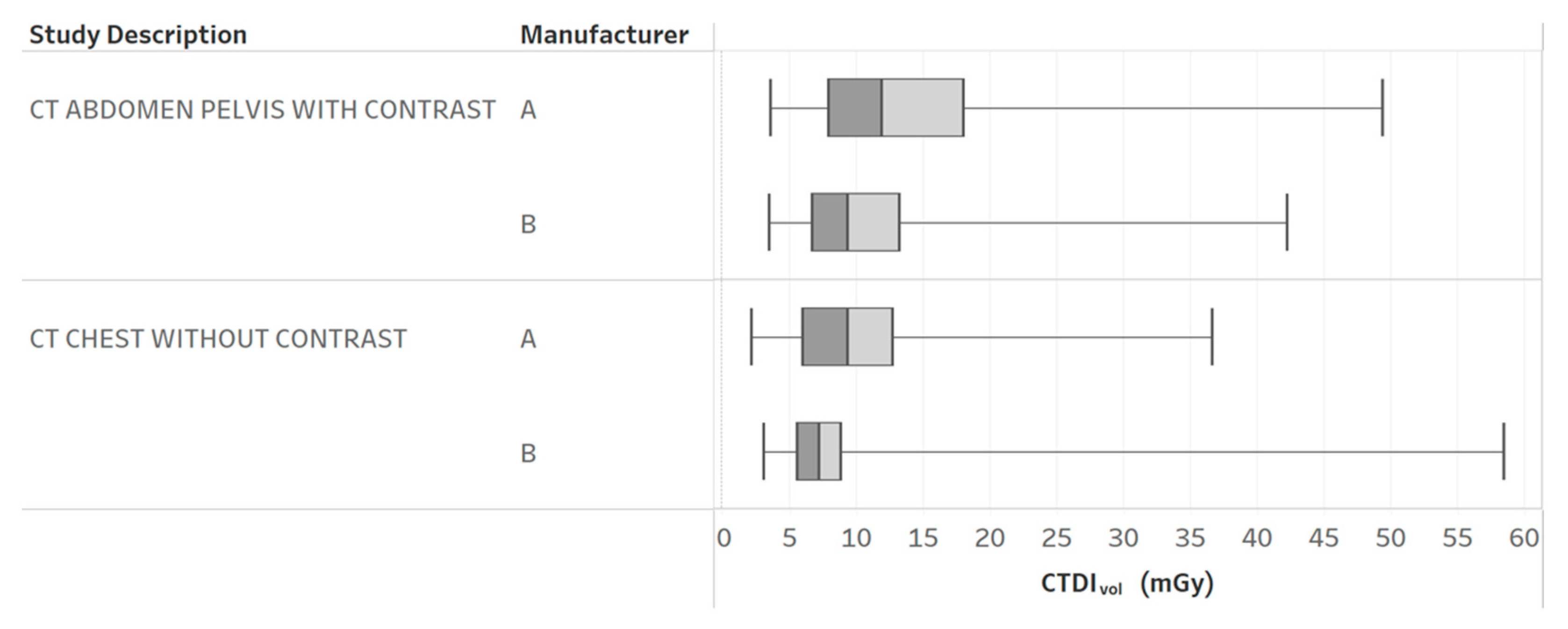
| 10 | CTDIvol boxplots by different protocols and manufacturers. | How does the radiation dose distribution change across scanners and protocols? |
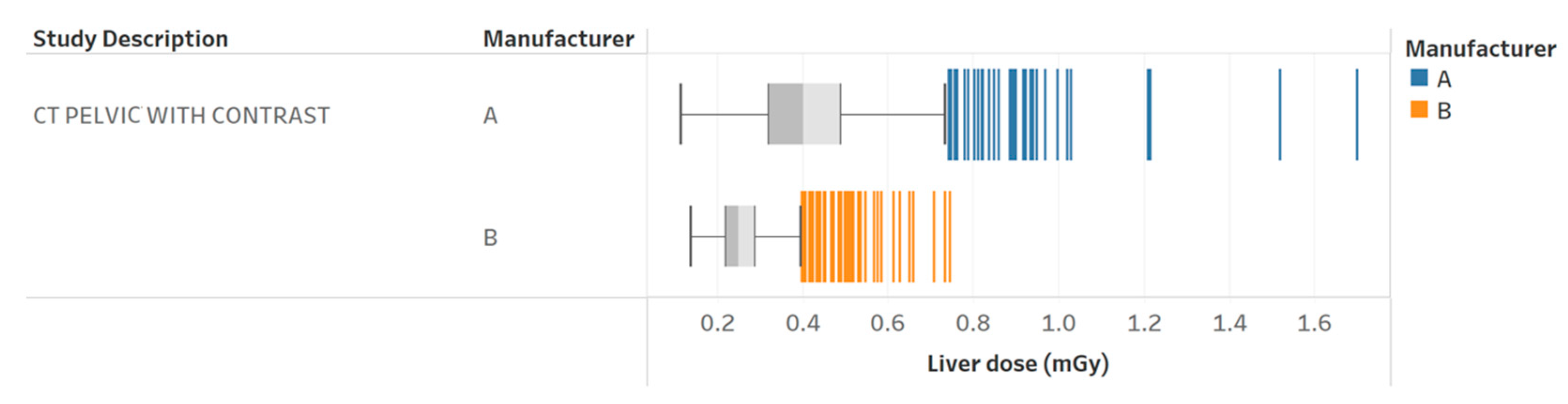
| 11a | Radiation dose to the liver for pelvic CT with contrast exams for two different scanners. | How does the dose to a specific organ change across scanners? |
| 11b | Scanning parameter comparison between a specific patient (outlier) and the whole population. | What is the underlying reason behind an outlier? |
| 12 | Median organ doses and effective dose for chest without contrast and pelvic with contrast CT exams. | How does the organ radiation dose distribution and effective dose change with different protocols? |
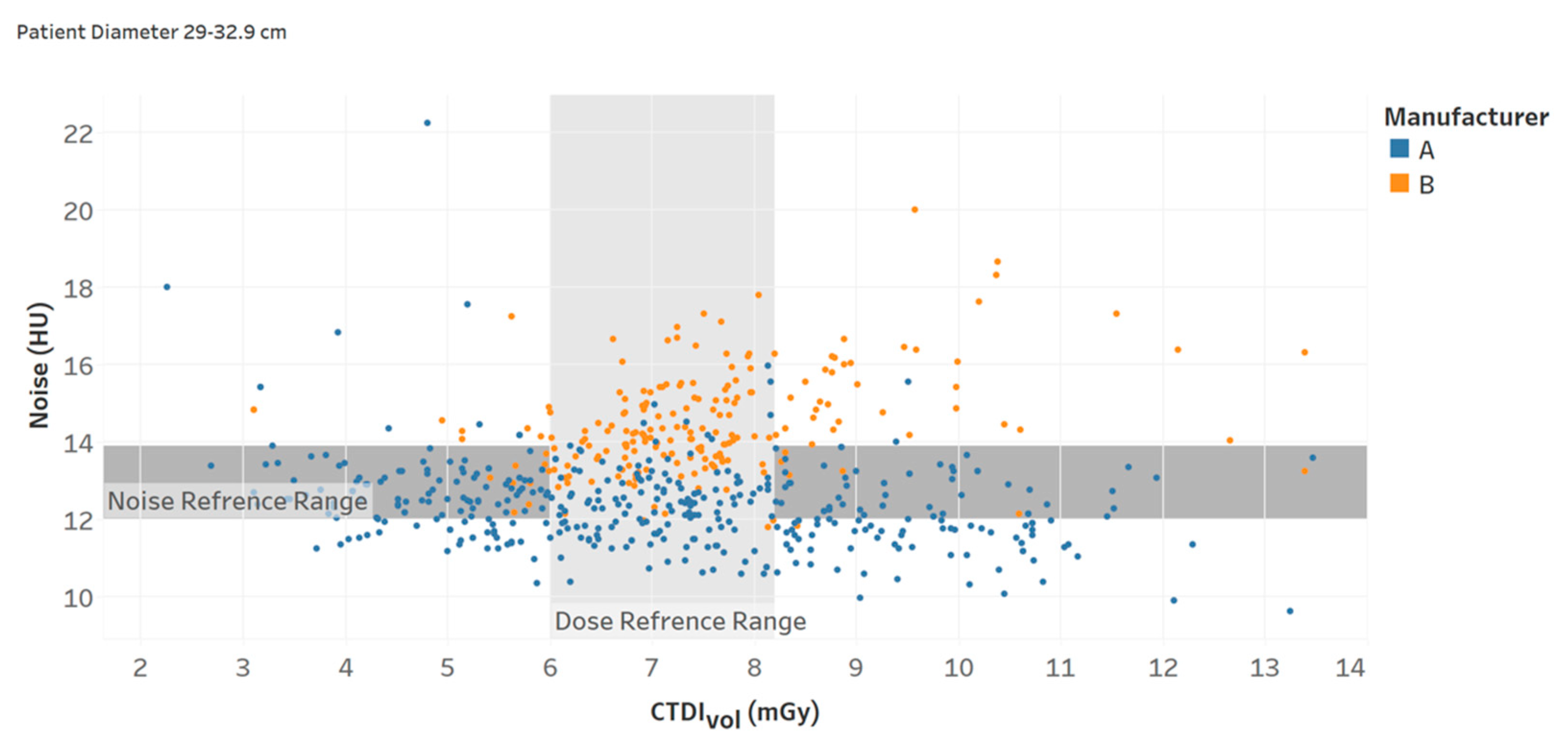
| 13 | Noise and CTDIvol reference ranges (interquartile intervals) for a specific protocol. | How are the radiation dose and noise magnitude compared with the literature and regulatory standards for different patient body habitus? [21] |
| 14 | Comparison of institution average CTDIvol with AD and DRL for one protocol | How is the radiation dose distribution at the institution compared with the regulatory levels in a patient population? [20] |
| Professionals | Charts | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11a | 11b | 12 | 13 | 14 | |
| Radiologists | 10 | 8 | 9 | 10 | 8 | 6.5 | 7 | 8.5 | 7 | 9 | 7 | 9.5 | 8.5 | 9.5 | 8 |
| Technologists | 6 | 7.5 | 9 | 8 | 7.5 | 6.5 | 7.5 | 8 | 5.5 | 9 | 8 | 8 | 7 | 8.5 | 7.5 |
| Medical physicists | 8.5 | 7.5 | 7.5 | 5.5 | 6 | 5.5 | 9 | 7.5 | 6 | 8 | 7.5 | 8 | 10 | 7 | 9 |
| All | 8.2 | 7.7 | 8.5 | 7.8 | 7.2 | 6.2 | 7.8 | 8 | 6.2 | 8.7 | 7.5 | 8.5 | 8.5 | 8.3 | 8.2 |
| Professionals | Average Score (out of 10) | Range | Variability |
|---|---|---|---|
| Radiologists | 8.4 | 6.5–10 | 1.14 |
| Technologists | 7.6 | 5.5–10 | 1.34 |
| Medical physicists | 7.5 | 5.5–9 | 1.00 |
| All | 7.8 | 5.5–10 | 0.79 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsaihati, N.; Ria, F.; Solomon, J.; Ding, A.; Frush, D.; Samei, E. Making CT Dose Monitoring Meaningful: Augmenting Dose with Imaging Quality. Tomography 2023, 9, 798-809. https://doi.org/10.3390/tomography9020065
Alsaihati N, Ria F, Solomon J, Ding A, Frush D, Samei E. Making CT Dose Monitoring Meaningful: Augmenting Dose with Imaging Quality. Tomography. 2023; 9(2):798-809. https://doi.org/10.3390/tomography9020065
Chicago/Turabian StyleAlsaihati, Njood, Francesco Ria, Justin Solomon, Aiping Ding, Donald Frush, and Ehsan Samei. 2023. "Making CT Dose Monitoring Meaningful: Augmenting Dose with Imaging Quality" Tomography 9, no. 2: 798-809. https://doi.org/10.3390/tomography9020065