
Intense FDG Uptake in the Common Bile Duct Post-ERCP Mimics Acute Infectious Cholangitis


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
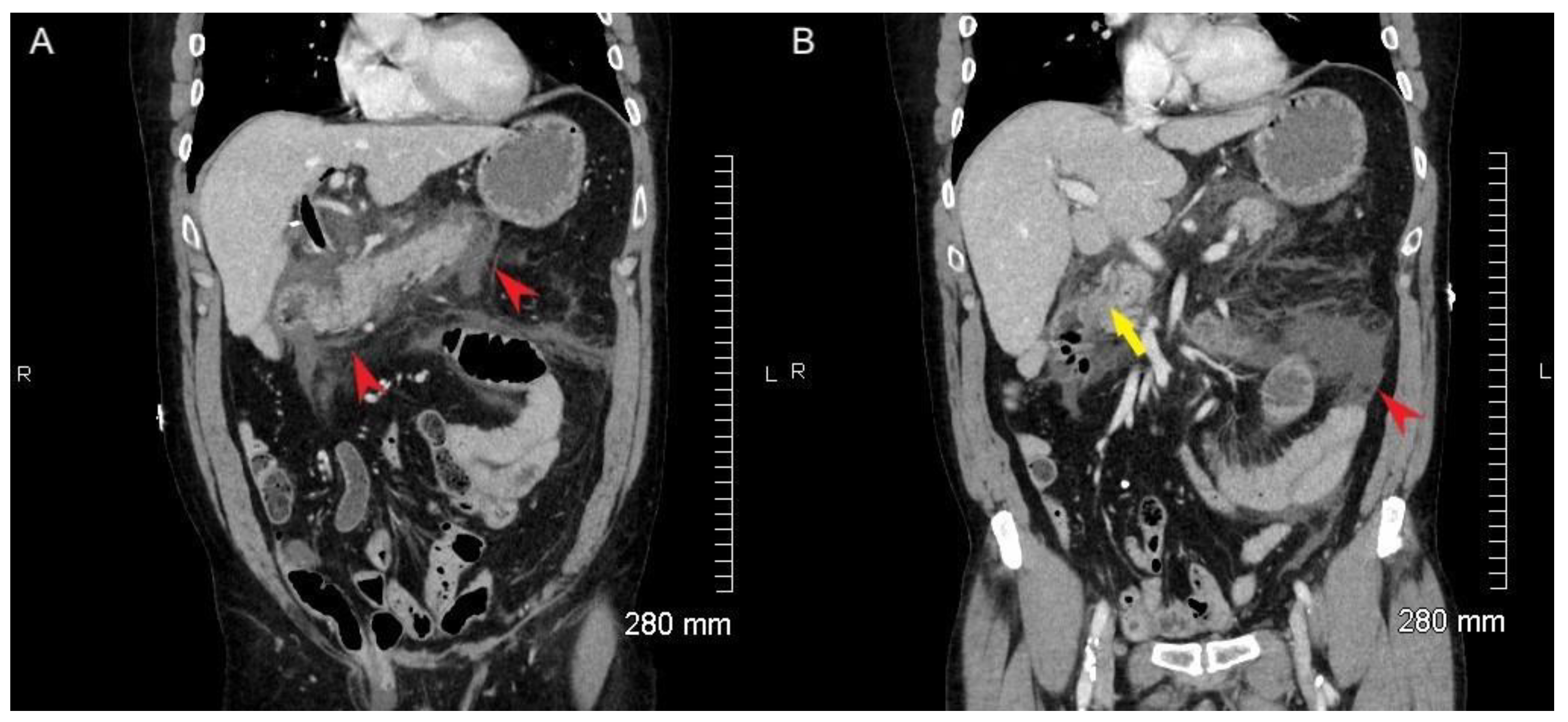
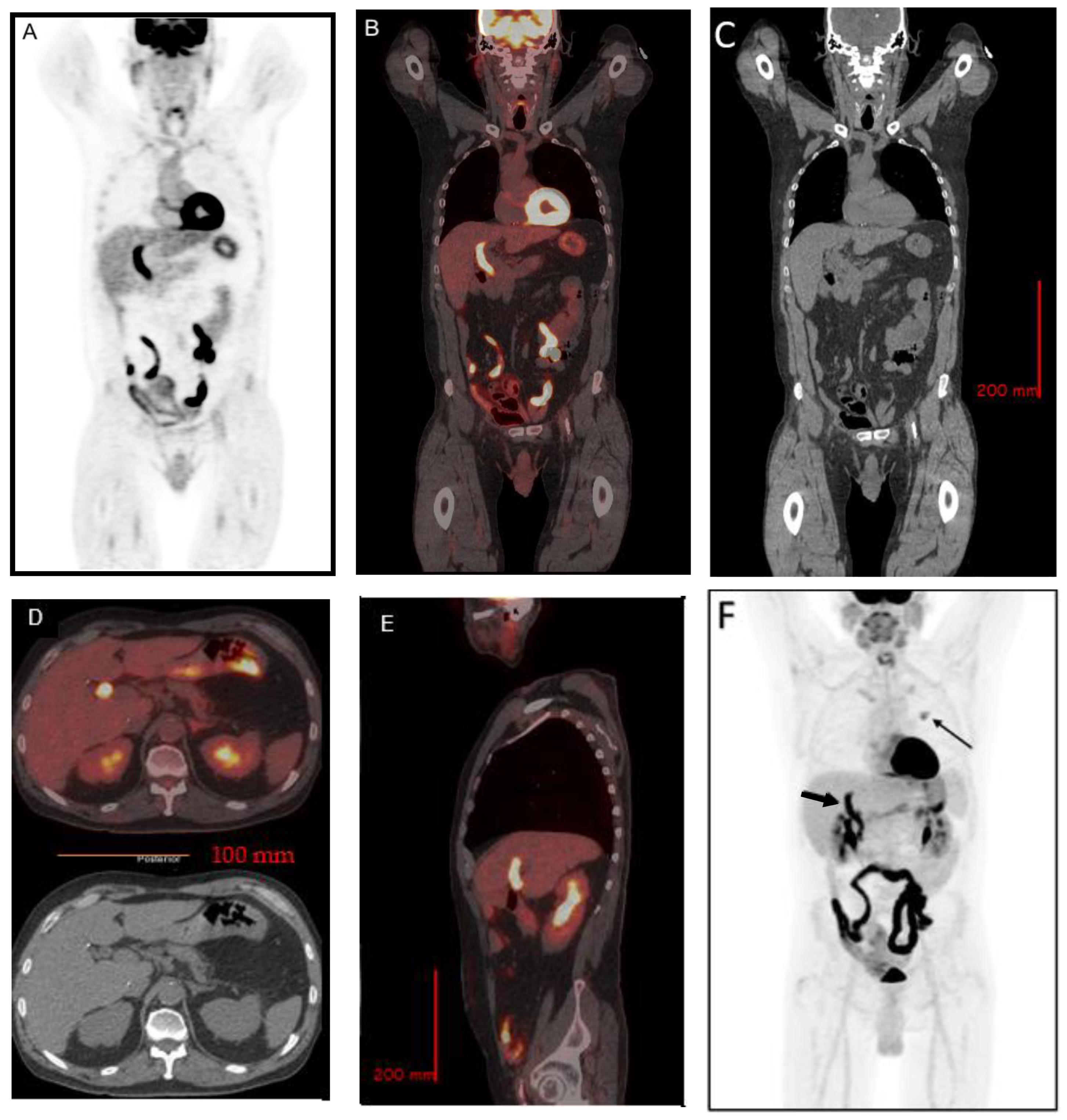
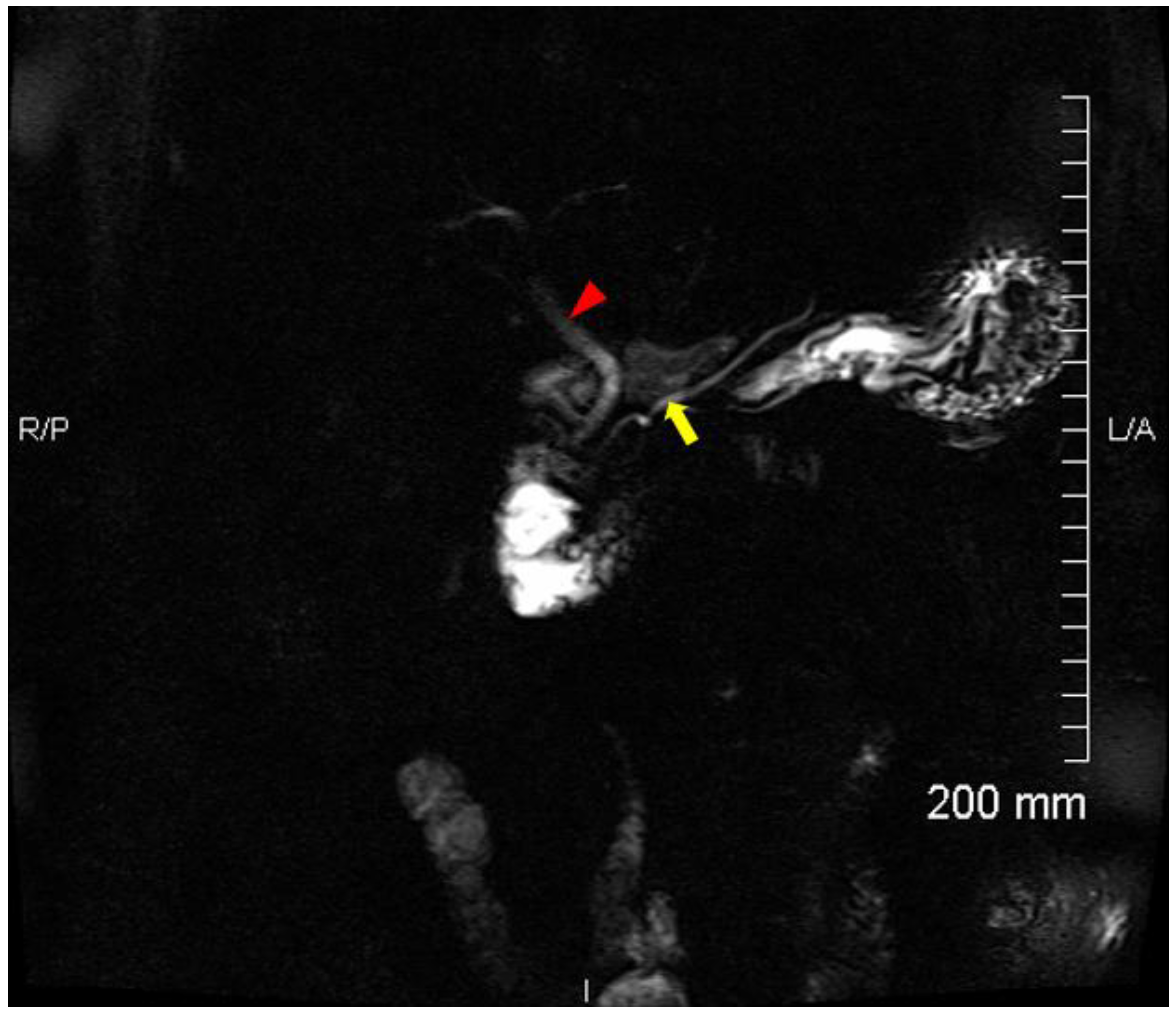
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Masci, E.; Toti, G.; Mariani, A.; Curioni, S.; Lomazzi, A.; Dinelli, M.; Minoli, G.; Crosta, C.; Comin, U.; Fertitta, A.; et al. Complications of Diagnostic and Therapeutic Ercp: A Prospective Multicenter Study. Am. J. Gastroenterol. 2001, 96, 417–423. [Google Scholar] [CrossRef]
- Loperfido, S.; Angelini, G.; Benedetti, G.; Chilovi, F.; Costan, F.; De Berardinis, F.; De Bernardin, M.; Ederle, A.; Fina, P.; Fratton, A. Major early complications from diagnostic and therapeutic ERCP: A prospective multicenter study. Gastrointest Endosc. 1998, 48, 1–10. [Google Scholar] [CrossRef]
- CChandrasekhara, V.; Khashab, M.A.; Muthusamy, V.R.; Acosta, R.D.; Agrawal, D.; Bruining, D.H.; Eloubeidi, M.A.; Fanelli, R.D.; Faulx, A.L.; Gurudu, S.R.; et al. Adverse events associated with ERCP. Gastrointest Endosc. 2017, 85, 32–47. [Google Scholar] [CrossRef] [Green Version]
- An, Z.; Braseth, A.L.; Sahar, N. Acute Cholangitis. Gastroenterol. Clin. N. Am. 2021, 50, 403–414. [Google Scholar] [CrossRef]
- Kiriyama, S.; Kozaka, K.; Takada, T.; Strasberg, S.M.; Pitt, H.A.; Gabata, T.; Hata, J.; Liau, K.-H.; Miura, F.; Horiguchi, A.; et al. Tokyo Guidelines 2018: Diagnostic criteria and severity grading of acute cholangitis (with videos). J. Hepato-Biliary-Pancreat Sci. 2018, 25, 17–30. [Google Scholar] [CrossRef]
- Mohan, R.; Goh, S.W.L.; Tan, G.W.; Tan, Y.P.; Junnarkar, S.P.; Huey, C.W.T.; Low, J.K.; Shelat, V.G. Validation of Tokyo Guidelines 2007 and Tokyo Guidelines 2013/2018 Criteria for Acute Cholangitis and Predictors of In-Hospital Mortality. Visc. Med. 2021, 37, 434–442. [Google Scholar] [CrossRef]
- Neoptolemos, J.P.; Carr-Locke, D.L.; Leese, T.; James, D. Acute cholangitis in association with acute pancreatitis: Incidence, clinical features and outcome in relation to ERCP and endoscopic sphincterotomy. Br. J. Surg. 2005, 74, 1103–1106. [Google Scholar] [CrossRef]
- Ikeno, Y.; Seo, S.; Yamamoto, G.; Nakamoto, Y.; Uemoto, Y.; Fuji, H.; Yoshino, K.; Yoh, T.; Taura, K.; Uemoto, S. Usefulness of Preoperative 18 F-FDG-PET in Detecting Invasive Intraductal Papillary Neoplasm of the Bile Duct. Anticancer. Res. 2018, 38, 3677–3682. [Google Scholar] [CrossRef]
- Choi, J.U.; Hwang, S.; Ahn, C.-S.; Moon, D.-B.; Ha, T.-Y.; Song, G.-W.; Jung, D.-H.; Kim, J.S.; Hong, S.-M. Diagnostic and prognostic impact of fluorodeoxyglucose-positron emission tomography in diagnosing intraductal papillary neoplasms of the bile duct of the liver. Ann. Surg. Treat. Res. 2022, 102, 335. [Google Scholar] [CrossRef]
- Annunziata, S.; Caldarella, C.; Pizzuto, D.A.; Galiandro, F.; Sadeghi, R.; Giovanella, L.; Treglia, G. Diagnostic Accuracy of Fluorine-18-Fluorodeoxyglucose Positron Emission Tomography in the Evaluation of the Primary Tumor in Patients with Cholangiocarcinoma: A Meta-Analysis. BioMed. Res. Int. 2014, 2014, 1–13. [Google Scholar] [CrossRef]
- Takanami, K.; Hiraide, T.; Kaneta, T.; Hayashi, H.; Unno, M.; Fujishima, F.; Fukuda, H.; Yamada, S.; Takahashi, S. FDG PET/CT Findings in Malignant Intraductal Papillary Mucinous Neoplasm of the Bile Ducts. Clin. Nucl. Med. 2010, 35, 83–85. [Google Scholar] [CrossRef]
- Hokonohara, K.; Noda, T.; Hatano, H.; Takata, A.; Hirota, M.; Oshima, K.; Tanida, T.; Komori, T.; Morita, S.; Imamura, H.; et al. Tubular adenoma of the common bile duct with uptake in 18F-FDG PET: A case report. Mol. Clin. Oncol. 2016, 4, 35–38. [Google Scholar] [CrossRef] [Green Version]
- Tu, Z.; Yang, Y.; Ruan, J.; Tu, J. FDG PET/CT Findings in Biliary Papillomatosis. Clin. Nucl. Med. 2020, 45, 798–799. [Google Scholar] [CrossRef]
- Dong, A.; Wang, Y.; Gong, J.; Zuo, C. FDG PET/CT Findings of Common Bile Duct Tuberculosis. Clin. Nucl. Med. 2014, 39, 67–70. [Google Scholar] [CrossRef]
- Zhang, W.; Fang, C.; Liu, H.; Chen, Y. FDG PET/CT Imaging of Hepatocellular Carcinoma With Bile Duct Tumor Thrombus. Clin. Nucl. Med. 2019, 44, 130–132. [Google Scholar] [CrossRef]
- Schönau, V.; Vogel, K.; Englbrecht, M.; Wacker, J.; Schmidt, D.; Manger, B.; Kuwert, T.; Schett, G. The value of 18 F-FDG-PET/CT in identifying the cause of fever of unknown origin (FUO) and inflammation of unknown origin (IUO): Data from a prospective study. Ann. Rheum. Dis. 2018, 77, 70–77. [Google Scholar] [CrossRef]
- Mulders-Manders, C.M.; Kouijzer, I.J.; Janssen, M.J.; Oyen, W.J.; Simon, A.; Bleeker-Rovers, C.P. Optimal use of [18F]FDG-PET/CT in patients with fever or inflammation of unknown origin. Q. J. Nucl. Med. Mol. Imaging 2021, 65, 51–58. [Google Scholar] [CrossRef]
- Vadrucci, M.; Castellani, M.; Longari, V. Acute cholangitis: An unexpected cause of fever of unknown origin diagnosed by 18F-FDG PET/CT. Rev. Esp. Med. Nucl. E Imagen Mol. 2016, 35, 339–340. [Google Scholar] [CrossRef]
- Nagasaki, Y.; Yamane, H.; Ochi, N.; Honda, Y.; Takigawa, N. High Uptake of FDG Along a Biliary Stent. Clin. Nucl. Med. 2016, 41, 890–891. [Google Scholar] [CrossRef] [Green Version]
- Lin, E.C.; Studley, M. Biliary Tract FDG Uptake Secondary to Stent Placement. Clin. Nucl. Med. 2003, 28, 318–319. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mistry, N.P.; Zeng, W. Intense FDG Uptake in the Common Bile Duct Post-ERCP Mimics Acute Infectious Cholangitis. Tomography 2022, 8, 2946-2951. https://doi.org/10.3390/tomography8060248
Mistry NP, Zeng W. Intense FDG Uptake in the Common Bile Duct Post-ERCP Mimics Acute Infectious Cholangitis. Tomography. 2022; 8(6):2946-2951. https://doi.org/10.3390/tomography8060248
Chicago/Turabian StyleMistry, Neel P., and Wanzhen Zeng. 2022. "Intense FDG Uptake in the Common Bile Duct Post-ERCP Mimics Acute Infectious Cholangitis" Tomography 8, no. 6: 2946-2951. https://doi.org/10.3390/tomography8060248