
Establishment of Diagnostic Reference Levels in Cone Beam Computed Tomography Scans in the United Arab Emirates

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. CBCT Unit
2.3. Radiation Dosimetry
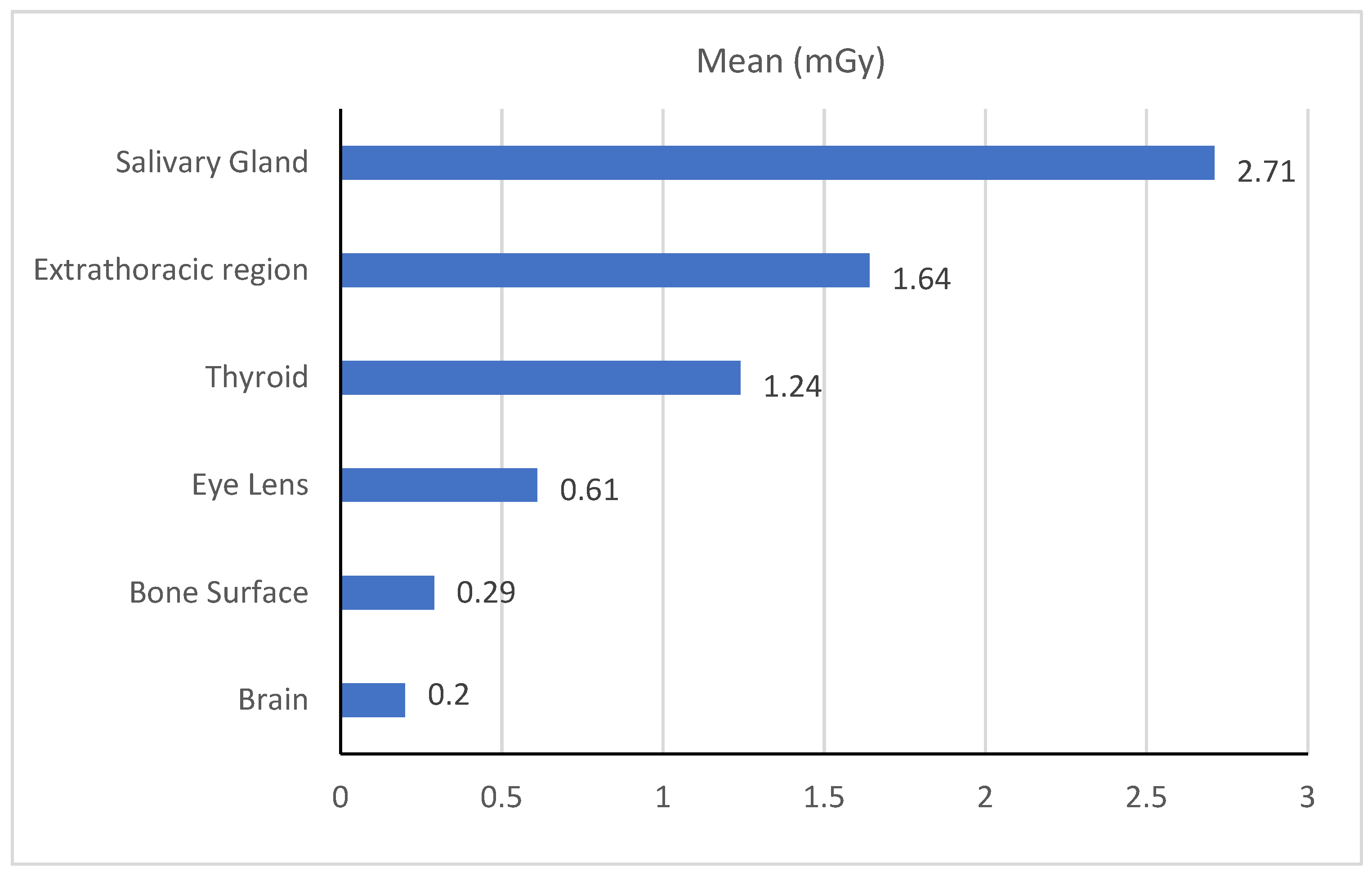
2.4. Organ Dose
3. Results
4. Discussion
5. Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR). Report of the United Nations Scientific Committee on the Effects of Atomic Radiation; United Nations: New York, NY, USA, 2021. [Google Scholar]
- Lin, E.C. Radiation risk from medical imaging. Mayo Clin. Proc. 2010, 85, 1142–1146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarfe, W.; Farman, A.; Sukovic, P. Clinical Applications of Cone-Beam Computed in Dental Pratice. J. Can. Dent. Assoc. 2006, 72, 75–80. [Google Scholar] [PubMed]
- Vassileva, J.; Rehani, M. Diagnostic reference levels. Am. J. Roentgenol. 2015, 204, W1–W3. [Google Scholar] [CrossRef] [PubMed]
- McCollough, C.H. Diagnostic Reference Levels—Image Wisely. American College of Radiology. 2010. Available online: http://www.imagewisely.org/Imaging-Modalities/Computed-Tomography/Medical-Physicists/Articles/Diagnostic-Reference-Levels (accessed on 8 February 2022).
- Venkatesh, E.; Elluru, S.V. CBCT: Basics and Applications in Dentistry. J. Istanb. Univ. Fac. Dent. 2017, 51, 102–121. [Google Scholar] [CrossRef]
- ICRP. The 2007 Recommendations of the International Commission on Radiological Protection. Ann. ICRP 2007, 37, 1–332. [Google Scholar]
- Vañó, E.; Miller, D.L.; Martin, C.J.; Rehani, M.M.; Kang, K.; Rosenstein, M.; Ortiz-López, P.; Mattsson, S.; Padovani, R.R.A. ICRP Publication 135: Diagnostic Reference Levels in Medical Imaging. Ann ICRP 2017, 46, 1–144. [Google Scholar] [CrossRef]
- Abuzaid, M.M.; Elshami, W.; El Serafi, A.; Hussien, T.; McConnell, J.R.; Tekin, H.O. Toward National Ct Diagnostic Reference Levels in the United Arab Emirates: A Multicenter Review of Ct Dose Index and Dose Area Product. Radiat. Prot. Dosim. 2020, 190, 243–249. [Google Scholar] [CrossRef]
- Abuzaid, M.M.; Elshami, W.; Tekin, H.O.; Ghonim, H.; Shawki, M.; Salama, D.H. Computed tomography radiation doses for common computed tomography examinations: A nationwide dose survey in United Arab Emirates. Insights Imaging 2020, 11, 88. [Google Scholar] [CrossRef]
- Liang, B.; Gao, Y.; Chen, Z.; Xu, X.G. Evaluation of effective dose from ct scans for overweight and obese adult patients using the virtualdose software. Radiat. Prot. Dosim. 2017, 174, 216–225. [Google Scholar] [CrossRef]
- Ding, A.; Gao, Y.; Liu, H.; Caracappa, P.F.; Long, D.J.; Bolch, W.E.; Liu, B.; Xu, X.G. VirtualDose: A software for reporting organ doses from CT for adult and pediatric patients. Phys. Med. Biol. 2015, 60, 5601–5625. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.; Quinn, B.; Mahmood, U.; Long, D.; Erdi, Y.; Germain, J.S.; Pandit-Taskar, N.; Xu, X.G.; Bolch, W.E.; Dauer, L.T. A comparison of pediatric and adult CT organ dose estimation methods. BMC Med. Imaging 2017, 17, 28. [Google Scholar] [CrossRef] [PubMed]
- Lorenzoni, D.C.; Bolognese, A.M.; Garib, D.G.; Guedes, F.R.; Sant’Anna, E.F. Cone-beam computed tomography and radiographs in dentistry: Aspects related to radiation dose. Int. J. Dent. 2012, 2012, 813768. [Google Scholar] [CrossRef] [PubMed]
- Lofthag-Hansen, S.; Huumonen, S.; Gröndahl, K.; Gröndahl, H.G. Limited cone-beam CT and intraoral radiography for the diagnosis of periapical pathology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Ludlow, J.B.; Timothy, R.; Walker, C.; Hunter, R.; Benavides, E.; Samuelson, D.B.; Scheske, M.J. Ffective dose of dental CBCT—A meta analysis of published data and additional data for nine CBCT units. Dentomaxillofacial Radiol. 2015, 44, 20140197. [Google Scholar] [CrossRef] [Green Version]
- Almuqrin, A.H.; Tamam, N.; Abdelrazig, A.; Elnour, A.; Sulieman, A. Organ dose and radiogenic risk in dental cone-beam computed tomography examinations. Radiat. Phys. Chem. 2020, 176, 108971. [Google Scholar] [CrossRef]
- Al-Okshi, A.; Horner, K.; Rohlin, M. A meta-review of effective doses in dental and maxillofacial cone beam CT using the ROBIS tool. Br. J. Radiol. 2021, 94, 20210042. [Google Scholar] [CrossRef]
- Berris, T.; Gupta, R.; Rehani, M.M. Radiation dose from cone-beam CT in neuroradiology applications. Am. J. Roentgenol. 2013, 200, 755–761. [Google Scholar] [CrossRef]
- Deleu, M.; Dagassan, D.; Berg, I.; Bize, J.; Dula, K.; Lenoir, V.; Ott, B.; Ott, J.G.; Verdun, F.R.; Weber, R.; et al. Establishment of national diagnostic reference levels in dental cone beam computed tomography in Switzerland. Dentomaxillofacial Radiol. 2020, 49, 20190468. [Google Scholar] [CrossRef]
- Endo, A.; Katoh, T.; Vasudeva, S.B.; Kobayashi, I.; Okano, T. A preliminary study to determine the diagnostic reference level using dose–area product for limited-area cone beam CT. Dentomaxillofacial Radiol. 2013, 42, 20120097. [Google Scholar] [CrossRef] [Green Version]
- Edmonds, K. Diagnostic reference levels as a quality assurance tool. Radiographer 2009, 56, 32–37. [Google Scholar] [CrossRef]
- Pauwels, R.; Zhang, G.; Theodorakou, C.; Walker, A.; Bosmans, H.; Jacobs, R.; Bogaerts, R.; Horner, K.; SEDENTEXCT Project Consortium. Effective radiation dose and eye lens dose in dental cone beam CT: Effect of field of view and angle of rotation. Br. J. Radiol. 2014, 87, 20130654. [Google Scholar] [CrossRef] [PubMed]
- Qiang, W.; Qiang, F.; Lin, L. ESTIMATION OF EFFECTIVE DOSE OF DENTAL X-RAY DEVICES. Radiat. Prot. Dosim. 2019, 183, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Kofler, J.M.; Cody, D.D.; Morin, R.L. CT protocol review and optimization. J. Am. Coll. Radiol. 2014, 11, 267–270. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | Characteristics |
|---|---|
| Resolution | Normal |
| Isotropic voxel size (mm) | 0.16–0.32 |
| Tube voltage, mA | 90 (kVp), 16 mA |
| Tube current-time product | 158 ± 2.6 (16.0–196.0) (mAs) |
| Filtration | 2.8 (mm Al) |
| Degree of rotation | 3600 |
| Dimension of collimator area | 8 × 13 (cm2) |
| Dose optimisation | Ultra-Low Dose™ imaging protocol, Pulsed X-ray radiography |
| Dose (mGy.cm2) | |
|---|---|
| Current Study | 1000 |
| IAEA | 1000 |
| Japan (2013) | 414 |
| Finland (2016) | 380 |
| UK (2017) | 265 |
| Switzerland (2020) | 638 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abuzaid, M.M.; Elshami, W.; Jayachandran, D.; Korappil, N.; Tekin, H.O. Establishment of Diagnostic Reference Levels in Cone Beam Computed Tomography Scans in the United Arab Emirates. Tomography 2022, 8, 2939-2945. https://doi.org/10.3390/tomography8060247
Abuzaid MM, Elshami W, Jayachandran D, Korappil N, Tekin HO. Establishment of Diagnostic Reference Levels in Cone Beam Computed Tomography Scans in the United Arab Emirates. Tomography. 2022; 8(6):2939-2945. https://doi.org/10.3390/tomography8060247
Chicago/Turabian StyleAbuzaid, Mohamed M., Wiam Elshami, Deepa Jayachandran, Noushad Korappil, and Huseyin O. Tekin. 2022. "Establishment of Diagnostic Reference Levels in Cone Beam Computed Tomography Scans in the United Arab Emirates" Tomography 8, no. 6: 2939-2945. https://doi.org/10.3390/tomography8060247