
Investigation of the Wetting Properties of Thalassemia Patients’ Blood Samples on Grade 5 Titanium Implant Surfaces: A Pilot Study
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Patient Selection and Study Materials
- High-resolution camera with a macro lens - Nikon D750, Nikon 105 mm Macro Lens (Nikon, Tokyo, Japan)
- Camera tripod for the stabilization of the camera
- Fixed medical pipette to drop the blood sample on the titanium surface
- Base to fix the Grade 5 titanium discs
- An illuminating system
- Titanium implant discs (see Section 2.3).
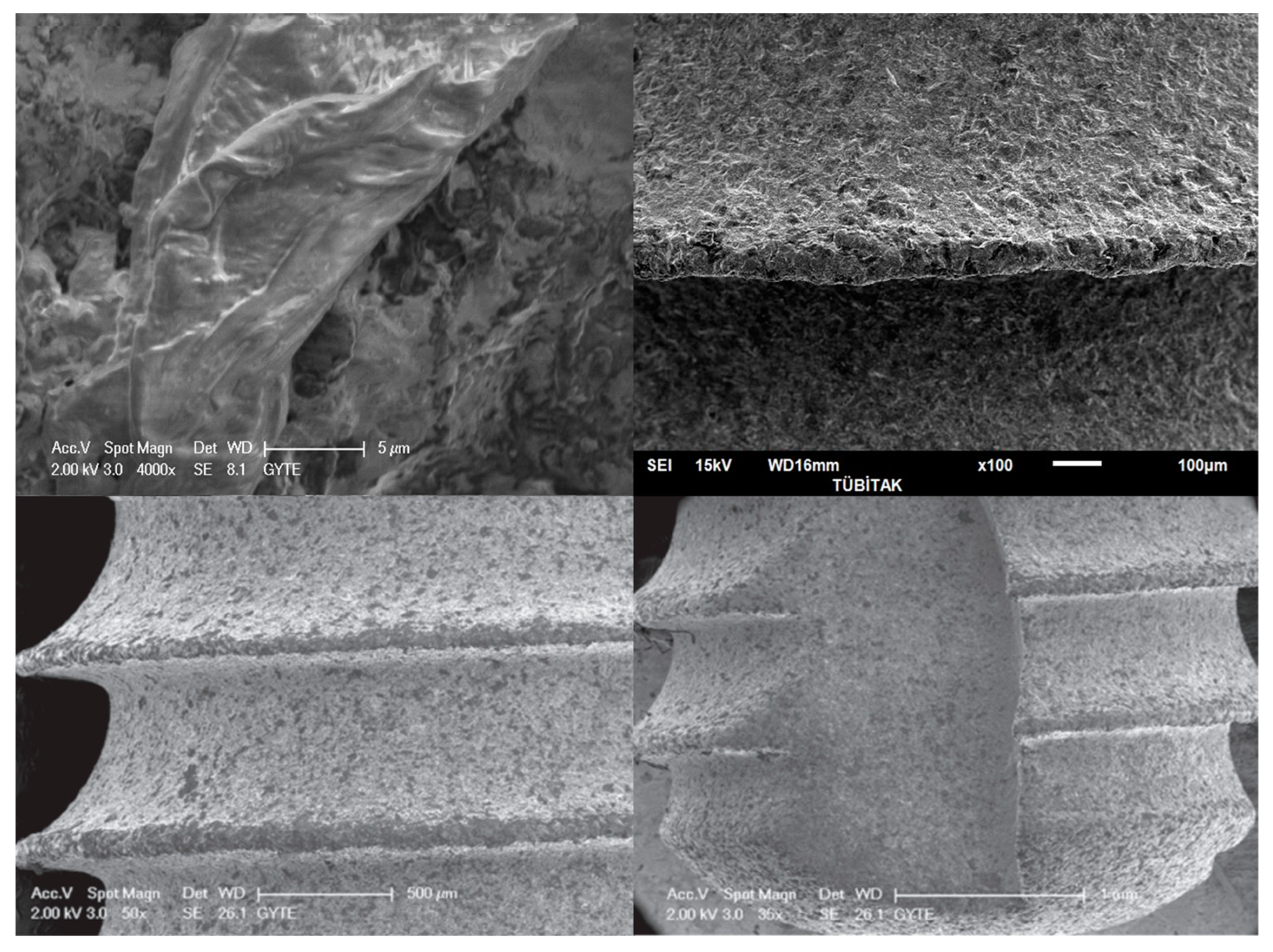
2.3. Features of the Titanium Implant Discs
- Grade 5 titanium discs (Mode Implant) with 10 mm diameter were used for all patients’ blood samples for the contact angle measurements;
- Type: Grade 5 (Ti6Al4V);
- Surface Features: resorbable blast media surface, resorbable blast texturing surface, and soluble blast media surface;
- Brand: Mode Implant;
- Diameter: 10 mm;
- Surface roughness: 1.697 µm;
- Surface sanding materials: tricalcium phosphate and hydroxyapatite. Biphasic calcium phosphate micro-blast with 65% HA content was used to sand the implant surface homogeneously at 1.4–1.8 µm with ROBOT technology.
2.4. Blood Sampling
2.5. Imaging of Blood Samples
2.6. Isotonic and Hypotonic Water
2.7. Contact Angle Measurements
2.8. Statistical Analysis
3. Results
3.1. Patient Demographic Data
3.2. Blood Sample Features of the Participants
3.3. Angular Measurements
3.4. Uncertainty Results
3.5. Statistical Analysis of the Contact Angles
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Origa, R. Beta-Thalassemia, in GeneReviews((R)); Adam, M.P., Everman, D.B., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Needs, T.; Gonzalez-Mosquera, L.F.; Lynch, D.T. Beta Thalassemia, in StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Misch, C.M.; Jolly, R.L.; Williams, D.R.; Chorazy, C.J. Maxillary implant surgery on a patient with thalassemia: A case report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 86, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Chamchoi, A.; Srihirun, S.; Paiboonsukwong, K.; Sriwantana, T.; Kongkaew, P.; Fucharoen, S.; Pattanapanyasat, K.; Sibmooh, N. Hemoglobin-bound platelets correlate with the increased platelet activity in hemoglobin E/β-thalassemia. Int. J. Lab. Hematol. 2020, 42, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Morelli, F.; Lang, N.P.; Bengazi, F.; Baffone, D.; Vila Morales, C.D.; Botticelli, D. Influence of bone marrow on osseointegration in long bones: An experimental study in sheep. Clin. Oral Implant. Res. 2015, 26, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Gittens, R.A.; Scheideler, L.; Rupp, F.; Hyzy, S.L.; Geis-Gerstorfer, J.; Schwartz, Z.; Boyan, B.D. A review on the wettability of dental implant surfaces II: Biological and clinical aspects. Acta Biomater. 2014, 10, 2907–2918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minervini, G.; Fiorillo, L.; Russo, D.; Lanza, A.; D’Amico, C.; Cervino, G.; Meto, A.; Di Fracenco, F. Prosthodontic Treatment in Patients with Temporomandibular Disorders and Orofacial Pain and/or Bruxism: A Review of the Literature. Prosthesis 2022, 4, 253–262. [Google Scholar] [CrossRef]
- Rupp, F.; Gittens, R.A.; Scheideler, L.; Marmur, A.; Boyan, B.D.; Schwartz, Z.; Geis-Gerstrofer, J. A review on the wettability of dental implant surfaces I: Theoretical and experimental aspects. Acta Biomater. 2014, 10, 2894–2906. [Google Scholar] [CrossRef] [Green Version]
- Koca, R.B.; Güven, O.; Çelik, M.S.; Fıratlı, E. Wetting properties of blood lipid fractions on different titanium surfaces. Int. J. Implant Dent. 2020, 6, 16. [Google Scholar] [CrossRef]
- Ozdemir, Z.; Orcun, O.; Bebek, O.; Bahar Basim, G. Development of 3-D Chemical Mechanical Polishing Process for Nanostructuring of Bioimplant Surfaces. ECS Trans. 2014, 61, 21–26. [Google Scholar] [CrossRef]
- Ozdemir, Z.; Ozdemir, A.; Basim, G.B. Application of chemical mechanical polishing process on titanium based implants. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 68, 383–396. [Google Scholar] [CrossRef]
- Blue, D.S.; Griggs, J.A.; Woody, R.D.; Miller, B.H. Effects of bur abrasive particle size and abutment composition on preparation of ceramic implant abutments. J. Prosthet. Dent. 2003, 90, 247–254. [Google Scholar] [CrossRef]
- Ivanoff, C.J.; Hallgren, C.; Widmark, G.; Sennerby, L.; Wennerberg, A. Histologic evaluation of the bone integration of TiO(2) blasted and turned titanium microimplants in humans. Clin. Oral Implant. Res. 2001, 12, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Khang, W.; Feldman, S.; Hawley, C.E.; Gunsolley, J. A multi-center study comparing dual acid-etched and machined-surfaced implants in various bone qualities. J. Periodontol. 2001, 72, 1384–1390. [Google Scholar] [CrossRef] [PubMed]
- Le Guehennec, L.; Soueidan, A.; Layrolle, P.; Amouriq, Y. Surface treatments of titanium dental implants for rapid osseointegration. Dent. Mater. 2007, 23, 844–854. [Google Scholar] [CrossRef] [PubMed]
- Novaes, A.B., Jr.; Souza, S.L.S.; de Oliveira, P.T.; Souza, A.M.M. Histomorphometric analysis of the bone-implant contact obtained with 4 different implant surface treatments placed side by side in the dog mandible. Int. J. Oral Maxillofac. Implant. 2002, 17, 377–383. [Google Scholar]
- Piattelli, A.; Manzon, L.; Scarano, A.; Paolantonio, M.; Piattelli, M. Histologic and histomorphometric analysis of the bone response to machined and sandblasted titanium implants: An experimental study in rabbits. Int. J. Oral Maxillofac. Implant. 1998, 13, 805–810. [Google Scholar]
- Shalabi, M.; Gortemaker, A.; Hof, M.V.; Jansen, J.; Creugers, N. Implant Surface Roughness and Bone Healing: A Systematic Review. J. Dent. Res. 2006, 85, 496–500. [Google Scholar] [CrossRef]
- Wennerberg, A.; Albrektsson, T. Effects of titanium surface topography on bone integration: A systematic review. Clin. Oral Implant. Res. 2009, 20 (Suppl. 4), 172–184. [Google Scholar] [CrossRef]
- Origa, R. Beta-Thalassemia. Genet. Med. 2017, 19, 609–619. [Google Scholar] [CrossRef] [Green Version]
- Shah, F.T.; Sayani, F.; Trompeter, S.; Draser, E.; Piga, A. Challenges of blood transfusions in beta-thalassemia. Blood Rev. 2019, 37, 100588. [Google Scholar] [CrossRef]
- Fagundes, N.C.F.; Minervini, G.; Alonso, B.F.; Nucci, L.; Grassia, V.; d’Apuzzo, F.; Puigdollers, A.; Perillo, L.; Flores-Mir, C. Patient-reported outcomes while managing obstructive sleep apnea with oral appliances: A scoping review. J. Evid. Based Dent. Pr. 2022; In Press. [Google Scholar]
- Walker, M.; Wood, J.; Taher, A. Cardiac Complications in Thalassaemia Major. In Guidelines for the Management of Transfusion Dependent Thalassaemia; Cappellini, M.D., Cohen, A., Porter, J., Eds.; Thalassaemia International Federation: Strovolos, Cyprus, 2014. [Google Scholar]
- Hattab, F.N. Periodontal condition and orofacial changes in patients with thalassemia major: A clinical and radiographic overview. J. Clin. Pediatr. Dent. 2012, 36, 301–307. [Google Scholar]
- Hattab, F.N.; Hazza’a, A.M.; Yassin, O.M.; Al-Rimawi, H.S. Caries risk in patients with thalassaemia major. Int. Dent. J. 2001, 51, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, R.; Verzì, P.; Caltabiano, M. Epidemiological survey of the prevalence of dental caries in young thalassemia major patients. Stomatol. Mediterr. SM 1990, 10, 133–136. [Google Scholar] [PubMed]
- Cervino, G.; Montanari, M.; Santonocito, D.; Nicita, F.; Baldari, R.; de Angelis, C.; Storni, G.; Fiorillo, L. Comparison of Two Low-Profile Prosthetic Retention System Interfaces: Preliminary Data of an In Vitro Study. Prosthesis 2019, 1, 54–60. [Google Scholar] [CrossRef]
- Ferrillo, M.; Nucci, L.; Giudice, A.; Calafiore, D.; Marotta, N.; Minervini, G.; d’Apuzzo, F.; Ammendolia, A.; Perillo, L.; de Sire, A. Efficacy of conservative approaches on pain relief in patients with temporomandibular joint disorders: A systematic review with network meta-analysis. CRANIO 2022, 23, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Spagnuolo, G.; Desiderio, C.; Rivieccio, V.; Amato, M.; Rossetti, D.V.; D’Antò, V.; Schweikl, H.; Lupi, A.; Rengo, S.; Nocca, G. In vitro cellular detoxification of triethylene glycol dimethacrylate by adduct formation with N-acetylcysteine. Dent. Mater. 2013, 29, e153–e160. [Google Scholar] [CrossRef] [PubMed]
- Avishai, E.; Yeghiazaryan, K.; Golubnitschaja, O. Impaired wound healing: Facts and hypotheses for multi-professional considerations in predictive, preventive and personalised medicine. EPMA J. 2017, 8, 23–33. [Google Scholar] [CrossRef] [Green Version]
- Krifka, S.; Hiller, K.-A.; Bolay, C.; Petzel, C.; Spagnuolo, G.; Reichl, F.-X.; Schmalz, G.; Schweikl, H. Function of MAPK and downstream transcription factors in monomer-induced apoptosis. Biomaterials 2012, 33, 740–750. [Google Scholar] [CrossRef] [PubMed]
- Nienhuis, A.W.; Nathan, D.G. Pathophysiology and Clinical Manifestations of the beta-Thalassemias. Cold Spring Harb. Perspect. Med. 2012, 2, a011726. [Google Scholar] [CrossRef] [Green Version]
- Mozos, I. Mechanisms Linking Red Blood Cell Disorders and Cardiovascular Diseases. BioMed Res. Int. 2015, 2015, 682054. [Google Scholar] [CrossRef]
- Rodrigues, M.; Kosaric, N.; Bonham, C.A.; Gurtner, G.C. Wound Healing: A Cellular Perspective. Physiol. Rev. 2019, 99, 665–706. [Google Scholar] [CrossRef]
- Hung, Y.-L.; Chang, Y.-Y.; Wang, M.-J.; Lin, S.-Y. A simple method for measuring the superhydrophobic contact angle with high accuracy. Rev. Sci. Instruments 2010, 81, 65105. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Romano, A.; Petruzzi, M.; Maio, C.; Serpico, R.; Lucchese, A.; Candotto, V.; Di Stasio, D. Telescopic overdenture on natural teeth: Prosthetic rehabilitation on (OFD) syndromic patient and a review on available literature. J. Biol. Regul. Homeost. Agents 2018, 32 (Suppl. 1), 131–134. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29460531 (accessed on 5 November 2022).
- di Stasio, D.; Lauritano, D.; Gritti, P.; Migliozzi, R.; Maio, C.; Minervini, G.; Petruzzi, M.; Serpico, R.; Candotto, V.; Lucchese, A. Psychiatric disorders in oral lichen planus: A preliminary case control study. J. Biol. Regul. Homeost. Agents 2018, 32 (Suppl. 1), 97–100. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29460524 (accessed on 5 November 2022).
- Pektas, Z.O.; Cubuk, S.; Kircelli, B.; Uckan, S. Management of Maxillary Deformity with Segmental Osteotomy followed by Implant Insertion in beta-Thalassemia Major Patient. J. Contemp. Dent. Pract. 2015, 16, 704–707. [Google Scholar] [CrossRef]
- Oren, D.; Dror, A.A.; Bramnik, T.; Sela, E.; Granot, I.; Srouji, S. The power of three-dimensional printing technology in functional restoration of rare maxillomandibular deformity due to genetic disorder: A case report. J. Med Case Rep. 2021, 15, 197. [Google Scholar] [CrossRef]
- Bozkurt, G. Results From The North Cyprus Thalassemia Prevention Program. Hemoglobin 2007, 31, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Modell, B. The Clinical Approaches to Thalassaemia; Grune & Stratton: New York, NY, USA, 1984; p. 453. [Google Scholar]
- Kolnagou, A.; Kontoghiorghes, G.J. Advances in the Prevention and Treatment are Changing Thalassemia from a Fatal to a Chronic Disease. Experience from a Cyprus Model and its Use as a Paradigm for Future Applications. Hemoglobin 2009, 33, 287–295. [Google Scholar] [CrossRef]
- Tillmann, W.; Schroter, W. Rheological properties of erythrocytes in heterozygous and homozygous beta thalassaemia. Br. J. Haematol. 1979, 43, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Dalal, A.; Pawar, V.; McAllister, K.; Weaver, C.; Hallab, N.J. Orthopedic implant cobalt-alloy particles produce greater toxicity and inflammatory cytokines than titanium alloy and zirconium alloy-based particles in vitro, in human osteoblasts, fibroblasts, and macrophages. J. Biomed. Mater. Res. Part A 2012, 100, 2147–2158. [Google Scholar] [CrossRef]
- Zwolak, I. Vanadium carcinogenic, immunotoxic and neurotoxic effects: A review of in vitro studies. Toxicol. Mech. Methods 2014, 24, 1–12. [Google Scholar] [CrossRef]
- Zhang, L.-C.; Chen, L.-Y. A Review on Biomedical Titanium Alloys: Recent Progress and Prospect. Adv. Eng. Mater. 2019, 21, 1801215. [Google Scholar] [CrossRef] [Green Version]
- Willis, J.; Li, S.; Crean, S.J.; Barrak, F.N. Is titanium alloy Ti-6Al-4 V cytotoxic to gingival fibroblasts-A systematic review. Clin. Exp. Dent. Res. 2021, 7, 1037–1044. [Google Scholar] [CrossRef]
- d’Apuzzo, F.; Nucci, L.; Strangio, B.M.; Inchingolo, A.D.; Dipalma, G.; Minervini, G.; Perillo, L.; Grassia, V. Dento-Skeletal Class III Treatment with Mixed Anchored Palatal Expander: A Systematic Review. Appl. Sci. 2022, 12, 4646. [Google Scholar] [CrossRef]
- Gonshor, A.; Goveia, G.; Sotirakis, E. A prospective, multicenter, 4-year study of the ACE Surgical resorbable blast media implant. J. Oral Implantol. 2003, 29, 174–180. [Google Scholar] [CrossRef]
- Koh, M.; Park, J.B.; Jang, Y.J.; Ko, Y. The effect of pretreating resorbable blast media titanium discs with an ultrasonic scaler or toothbrush on the bacterial removal efficiency of brushing. J. Periodontal Implant Sci. 2013, 43, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Piattelli, M.; Scarano, A.; Paolantonio, M.; Iezzi, G.; Petrone, G.; Piattelli, A. Bone Response to Machined and Resorbable Blast Material Titanium Implants: An Experimental Study in Rabbits. J. Oral Implant. 2002, 28, 2–8. [Google Scholar] [CrossRef]
- Fiorillo, L.; De Stefano, R.; Cervino, G.; Crimi, S.; Bianchi, A.; Campagna, P.; Herford, A.S.; Laino, L.; Cicciù, M. Oral and Psychological Alterations in Haemophiliac Patients. Biomedicines 2019, 7, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicciù, M.; Fiorillo, L.; D’Amico, C.; Gambino, D.; Amantia, E.M.; Laino, L.; Crimi, S.; Campagna, P.; Bianchi, A.; Herford, A.S.; et al. 3D Digital Impression Systems Compared with Traditional Techniques in Dentistry: A Recent Data Systematic Review. Materials 2020, 13, 1982. [Google Scholar] [CrossRef] [PubMed]
- Mekayarajjananonth, T.; Winkler, S. Contact Angle Measurement on Dental Implant Biomaterials. J. Oral Implant. 1999, 25, 230–236. [Google Scholar] [CrossRef]
- Spijker, H.T. On the influence of flow conditions and wettability on blood material interactions. Biomaterials 2003, 24, 4717–4727. [Google Scholar] [CrossRef]
- Bagambisa, F.B.; Joos, U. Preliminary studies on the phenomenological behaviour of osteoblasts cultured on hydroxyapatite ceramics. Biomaterials 1990, 11, 50–56. [Google Scholar] [CrossRef]
- Buser, D.; Schenk, R.K.; Steinemann, S.; Fiorellini, J.P.; Fox, C.H.; Stich, H. Influence of surface characteristics on bone integration of titanium implants. A histomorphometric study in miniature pigs. J. Biomed. Mater. Res. 1991, 25, 889–902. [Google Scholar] [CrossRef]
- Bowers, K.T.; Keller, J.C.; Randolph, B.A.; Wick, D.G.; Michaels, C.M. Optimization of surface micromorphology for enhanced osteoblast responses in vitro. Int. J. Oral Maxillofac. Implant. 1992, 7, 302–310. [Google Scholar]
- Scarano, A.; Tari Rexhep, S.; Leo, L.; Lorusso, F. Wettability of implant surfaces: Blood vs autologous platelet liquid (APL). J. Mech. Behav. Biomed. Mater. 2022, 126, 104773. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographic Data of the Participants | Mean Age (Year) | Min Age (Year) | Max Age (Year) | Number of Female Participants | Number of Male Participants |
|---|---|---|---|---|---|
| Healthy participants | 35.85 | 21 | 66 | 22 | 20 |
| BT carriers | 37.3 | 22 | 64 | 23 | 19 |
| BTM patients | 39.7 | 20 | 55 | 22 | 20 |
| RBC | HGB | PLT | |
|---|---|---|---|
| (Million Cells/mcL) | (gr/dL) | (Thousand Platelets/mcL) | |
| Healthy male and BT carrier male | 5.52 (min 4.72/max 6.06) | 15.3 (min 13.45/max 16.41) | 324 (min 174/max 445) |
| BTM male | 3.76 (min 3.19/max 4.34) | 9.91 (min 9.00/max 11.40) | 525 (min 190/max 917) |
| Healthy female and BT carrier female | 4.83 (min 4.23/max 5.26) | 13.53 (min 12.1/max 14.83) | 317 (min 162/max 434) |
| BTM female | 3.79 (min 3.15/max 4.29) | 10.09 (min 8.70/max 11.30) | 470 (min 211/max 754) |
| Parameters | Comparison Groups | p-Value |
|---|---|---|
| BTM male vs. non-BTM male | 0.000 * | |
| BTM female vs. non-BTM female | 0.000 * | |
| RBC | BTM male vs. BTM female | 0.751 ** |
| Non-BTM male vs. non-BTM female | 0.000 * | |
| BTM male vs. non-BTM male | 0.000 * | |
| BTM female vs. non-BTM female | 0.000 * | |
| HGB | BTM male vs. BTM female | 0.416 ** |
| Non-BTM male vs. non-BTM female | 0.000 * | |
| BTM male vs. non-BTM male | 0.002 * | |
| BTM female vs. non-BTM female | 0.010 * | |
| PLT | BTM male vs. BTM female | 0.338 ** |
| Non-BTM male vs. non-BTM female | 0.319 * |
| Theta-Circular | Theta-Ellipse | Theta-Mean | |
|---|---|---|---|
| (Degree) | (Degree) | (Degree) | |
| Healthy participants | 89.89 | 87.6 | 87.59 |
| BT carriers | 88.02 | 85.77 | 85.79 |
| BTM patients | 93.95 | 89.98 | 89.98 |
| Distilled water | 103.8 | 102 | 103.03 |
| Isotonic water | 102.7 | 101.3 | 102.14 |
| Theta-Mean (Degree) | Theta-Circular (Degree) | Theta-Ellipse (Degree) | |
|---|---|---|---|
| Kruskal–Wallis H | 1.227 | 2.926 | 1.226 |
| Degrees of freedom | 2 | 2 | 2 |
| p-value | 0.541 | 0.232 | 0.542 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Temelci, A.; Yılmaz, H.G.; Ünsal, G.; Uyanik, L.O.; Yazman, D.; Ayali, A.; Minervini, G. Investigation of the Wetting Properties of Thalassemia Patients’ Blood Samples on Grade 5 Titanium Implant Surfaces: A Pilot Study. Biomimetics 2023, 8, 25. https://doi.org/10.3390/biomimetics8010025
Temelci A, Yılmaz HG, Ünsal G, Uyanik LO, Yazman D, Ayali A, Minervini G. Investigation of the Wetting Properties of Thalassemia Patients’ Blood Samples on Grade 5 Titanium Implant Surfaces: A Pilot Study. Biomimetics. 2023; 8(1):25. https://doi.org/10.3390/biomimetics8010025
Chicago/Turabian StyleTemelci, Ali, Hasan Güney Yılmaz, Gürkan Ünsal, Lokman Onur Uyanik, Dilek Yazman, Aysa Ayali, and Giuseppe Minervini. 2023. "Investigation of the Wetting Properties of Thalassemia Patients’ Blood Samples on Grade 5 Titanium Implant Surfaces: A Pilot Study" Biomimetics 8, no. 1: 25. https://doi.org/10.3390/biomimetics8010025