
The Effects of Intrusion of Anterior Teeth by Skeletal Anchorage in Deep Bite Patients; A Systematic Review and Meta-Analysis
 ,
,
Abstract
:1. Introduction
- -
- P: Deep bite patients needing intrusion of anterior teeth with permanent dentition (14–50 years of age);
- -
- I: Patients undergoing intrusion through the use of mini-implants (directly or indirectly),
- -
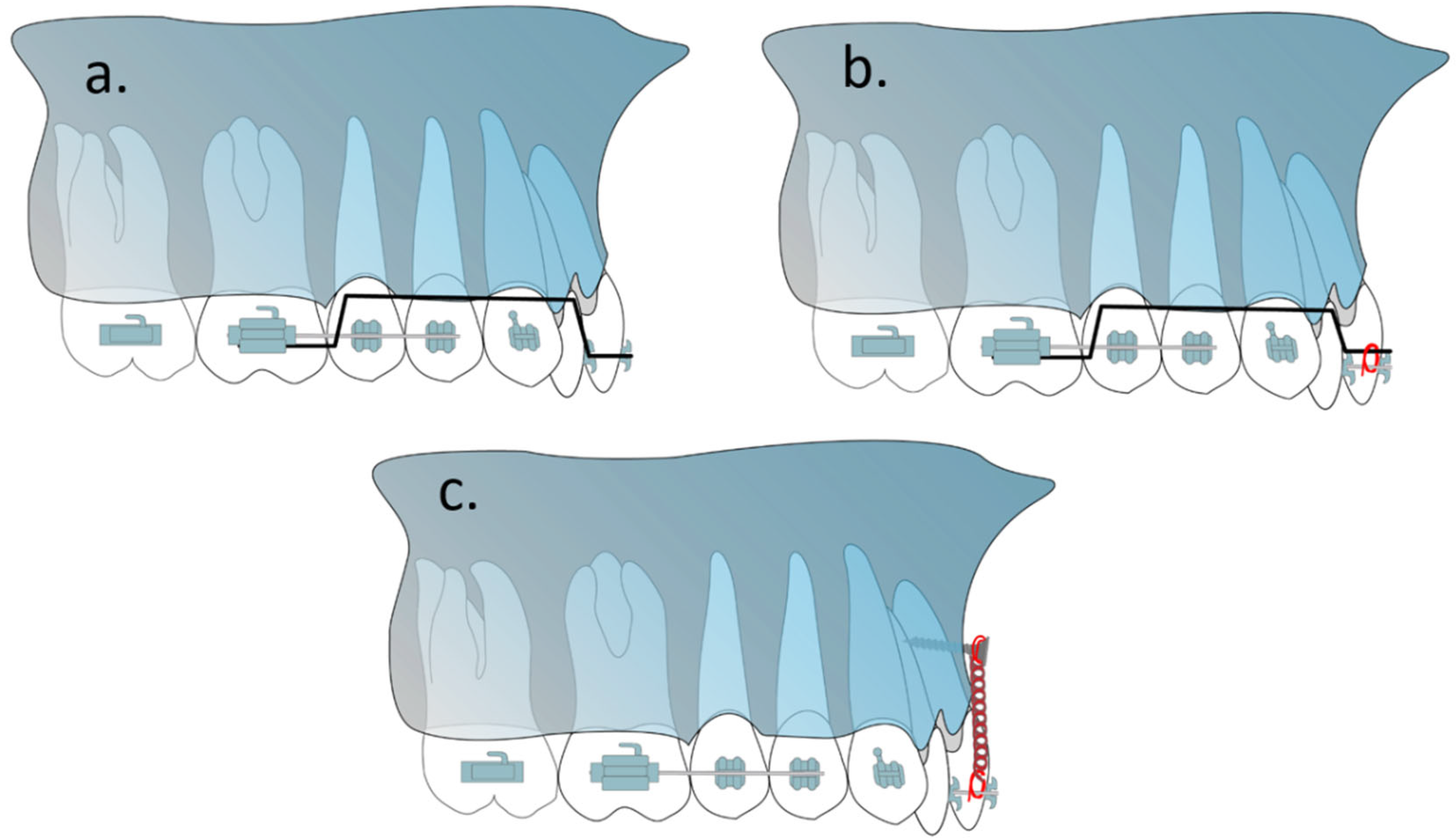
- C: Using other orthodontic methods of anterior tooth intrusion (i.e., utility arch, Connecticut intrusion arch);
- -
- O: Overjet, overbite, cephalometric indicators (dental and skeletal), intrusion duration, intrusion rate and intrusion speed, root resorption;
- -
- S: Clinical studies (cohort studies, RCTs and CCTs).
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Review of Literature
2.3. Study Screening and Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
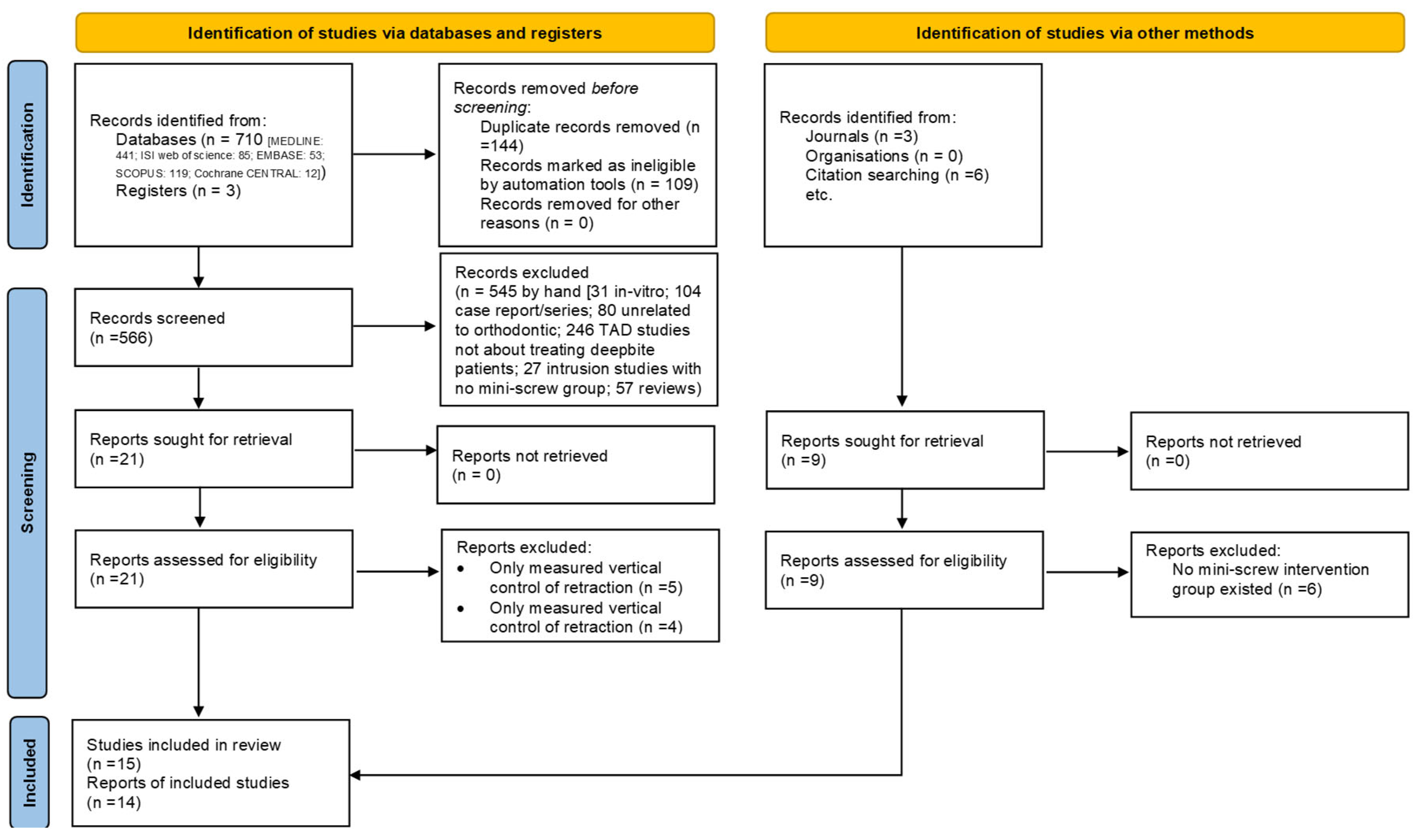
3.1. Study Selection and Characteristics
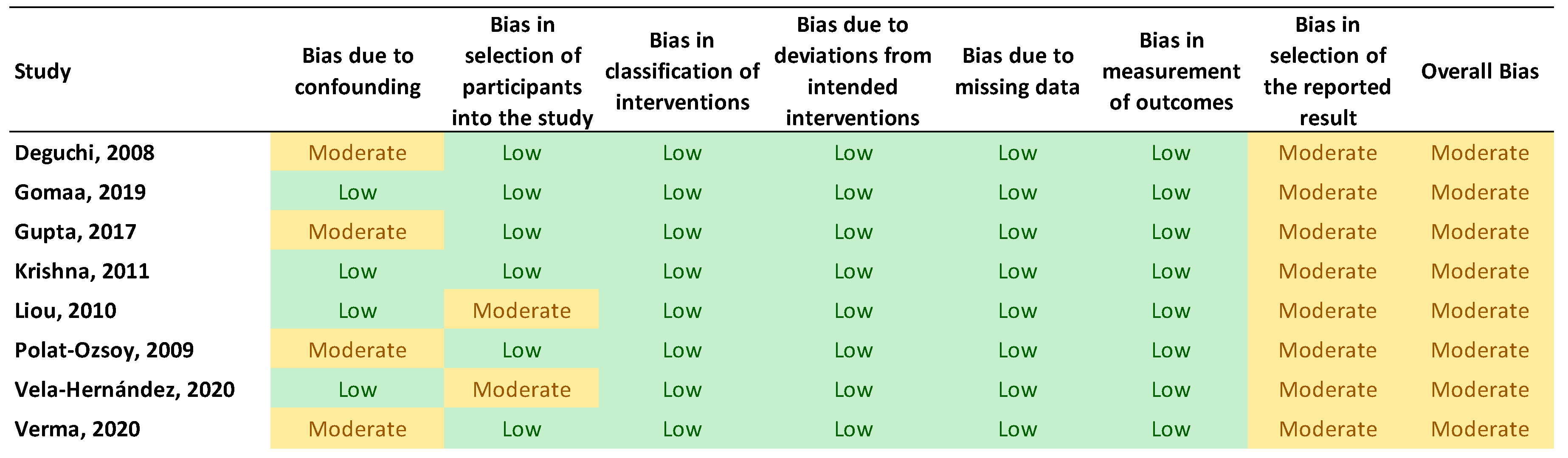
3.2. Risk of Bias
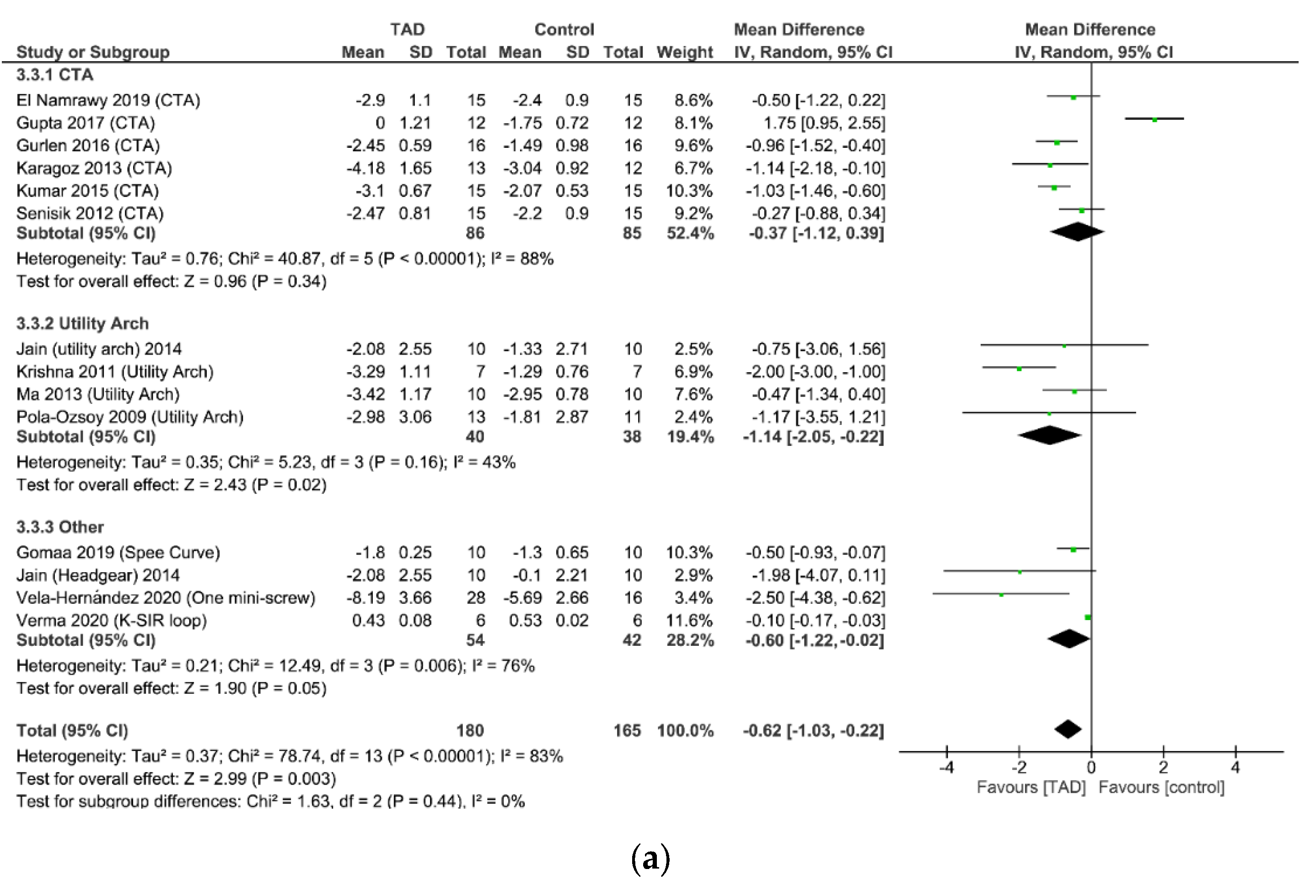
3.3. Data Synthesis
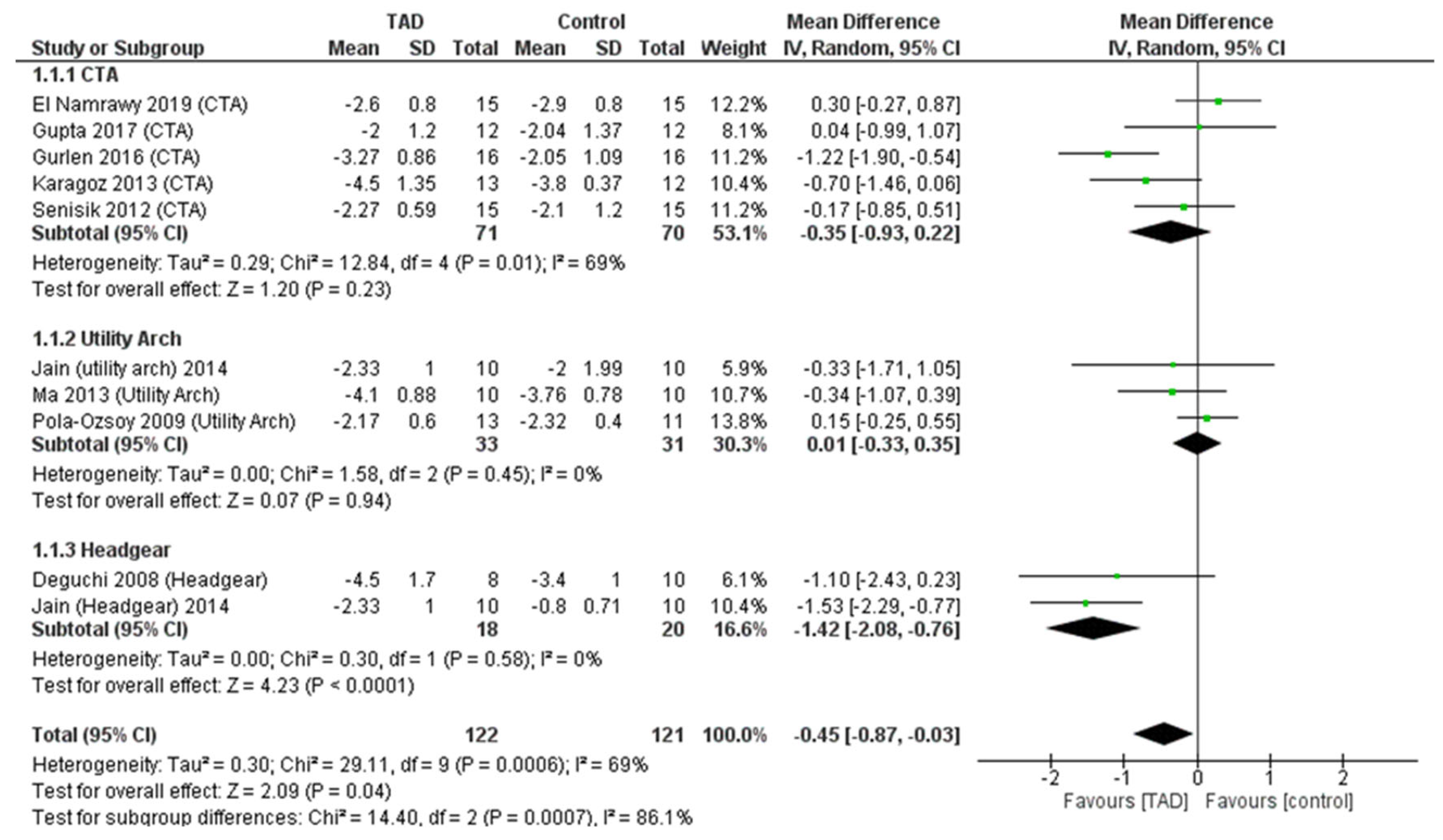
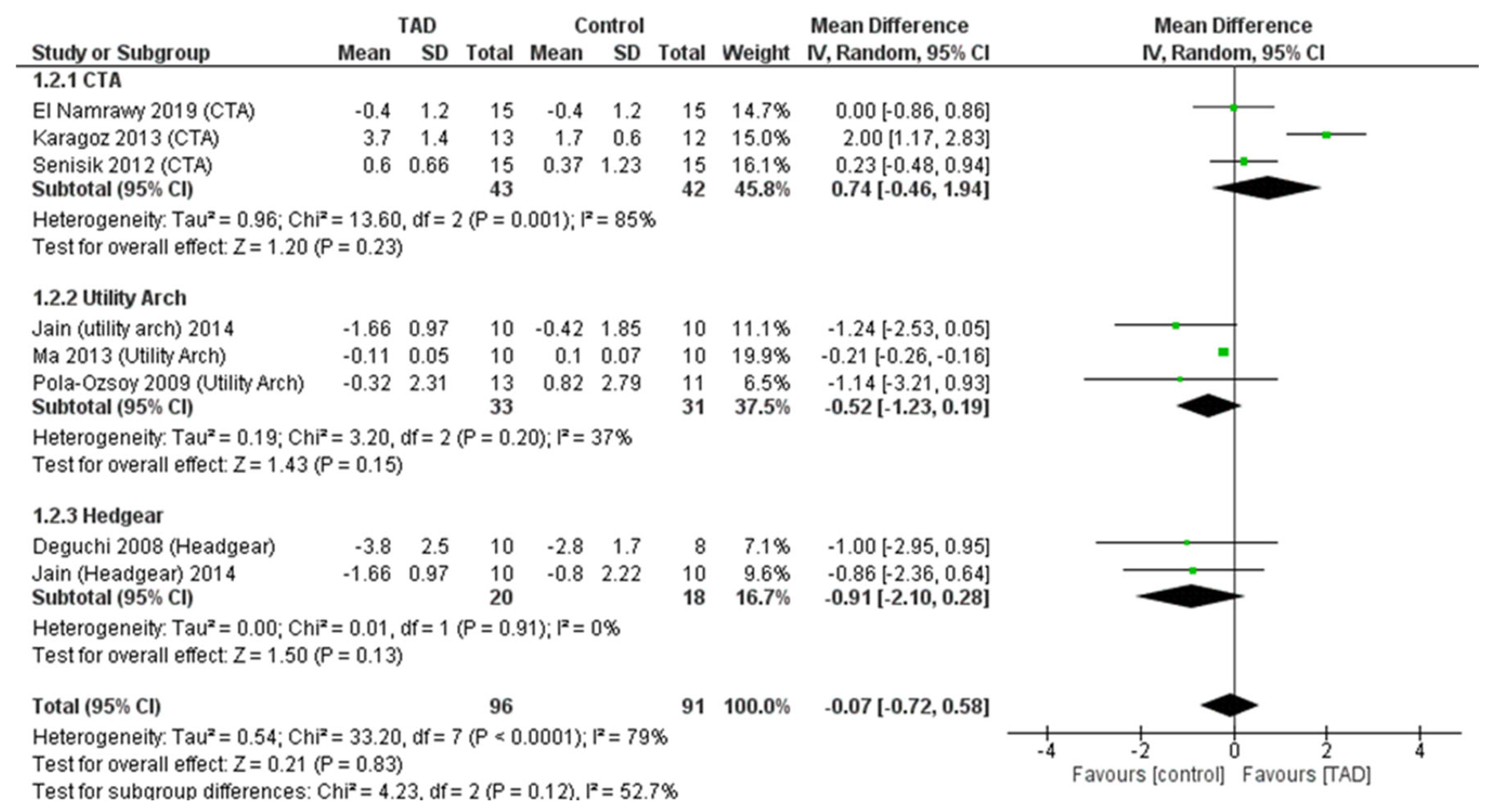
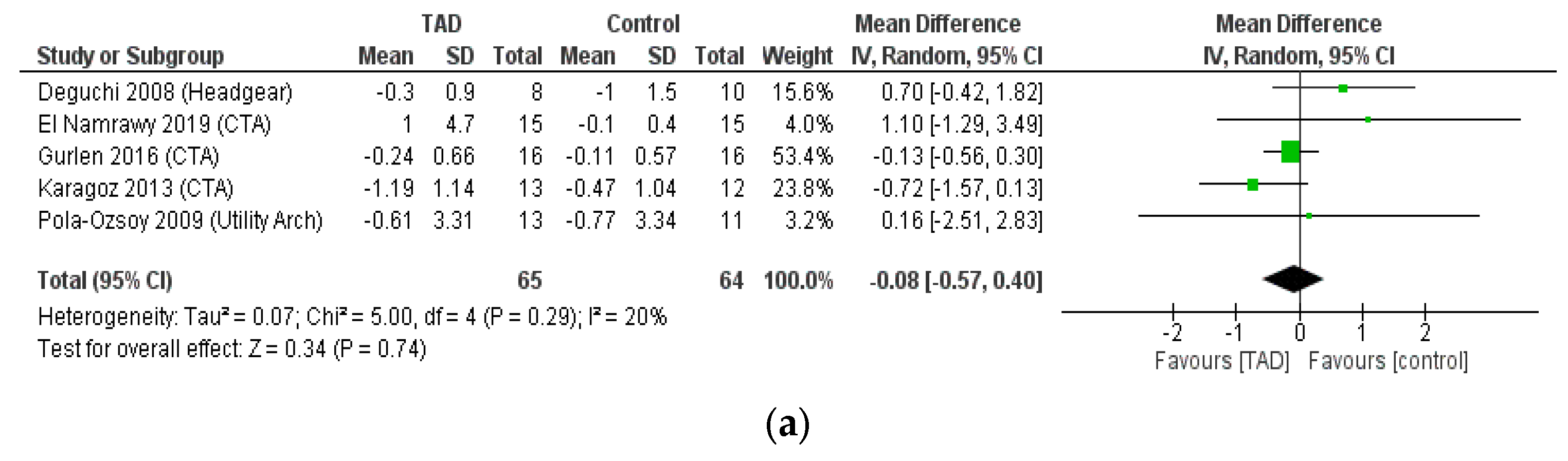
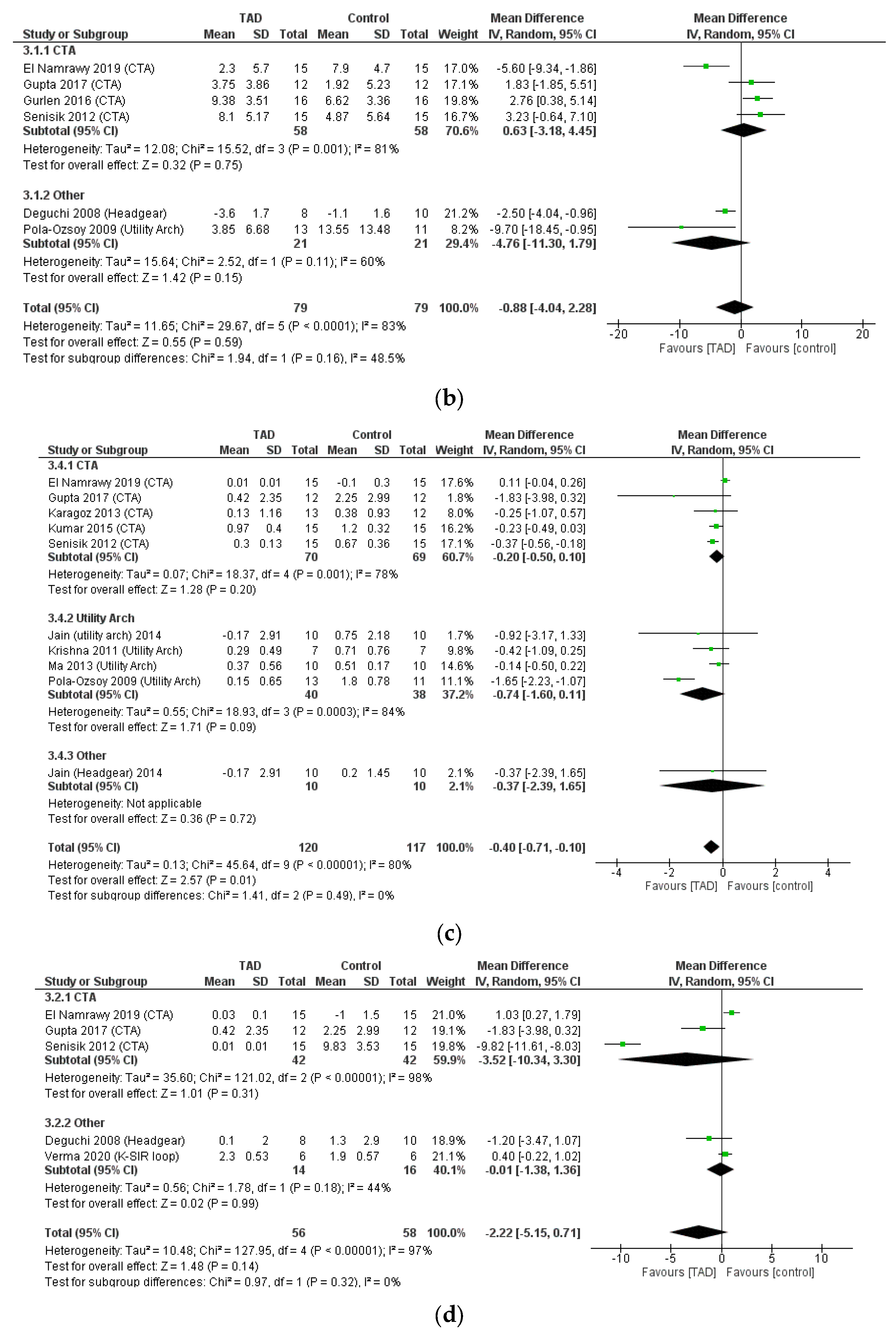
3.4. A Meta-Analysis of Dental Indices
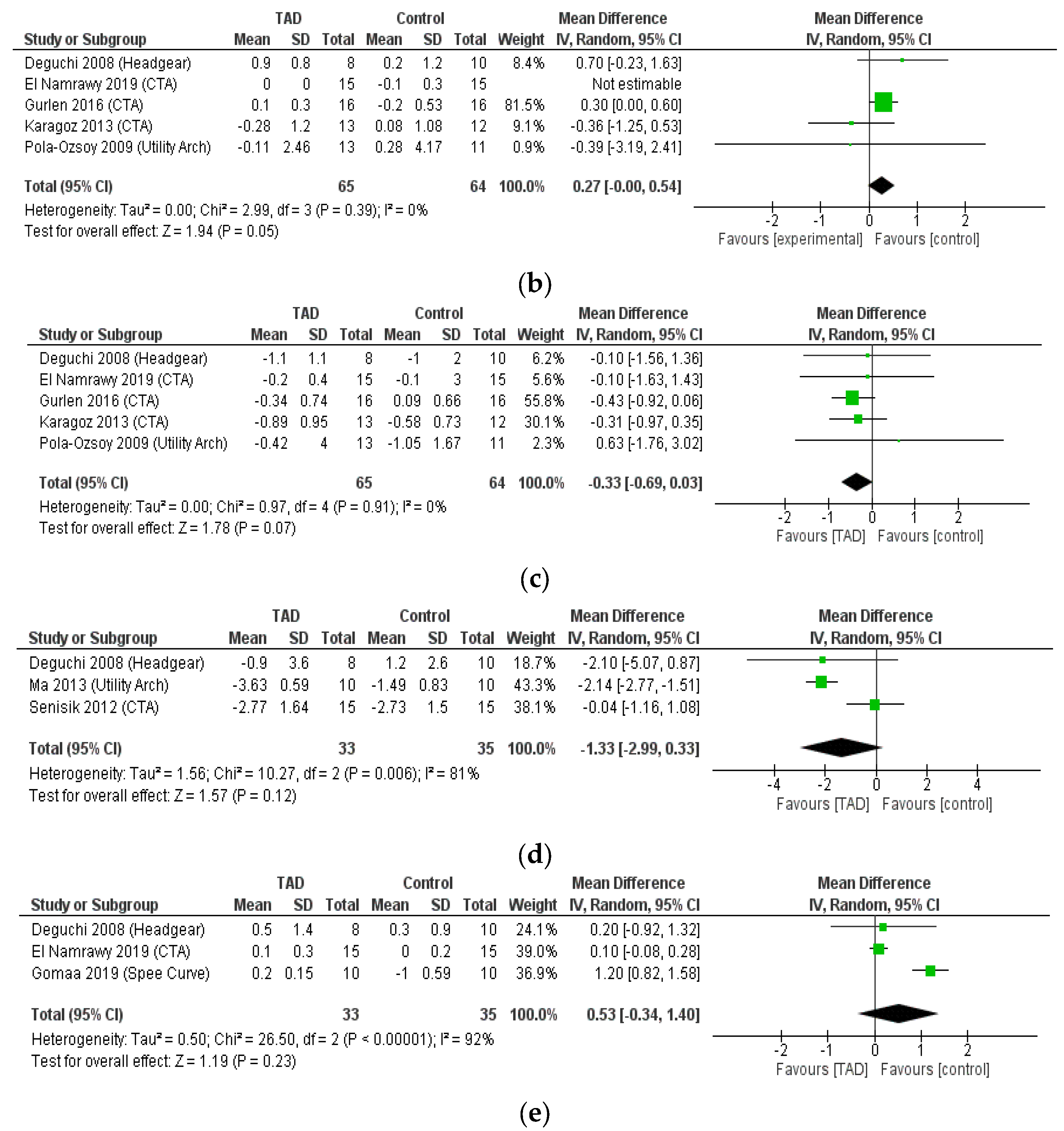
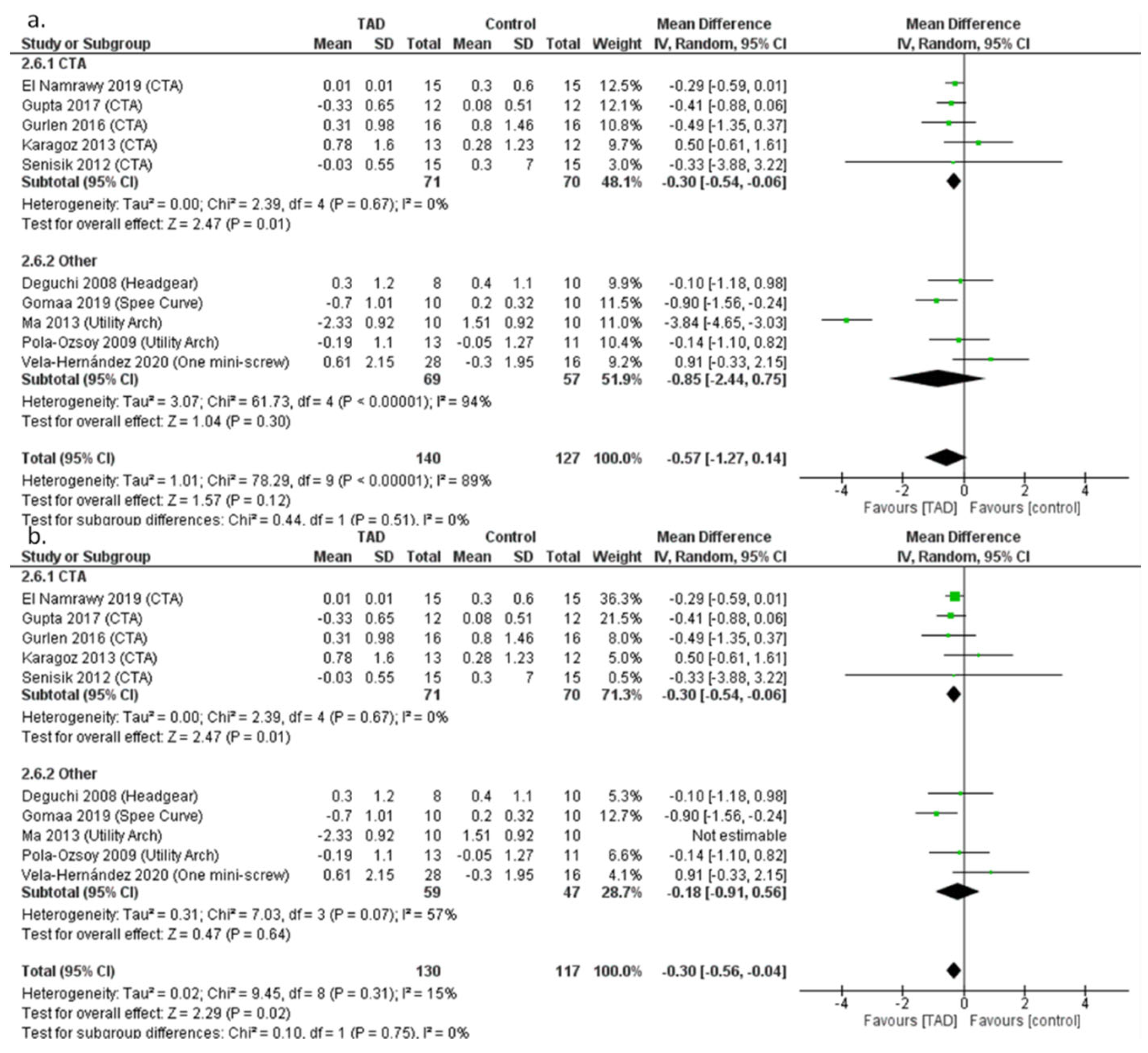
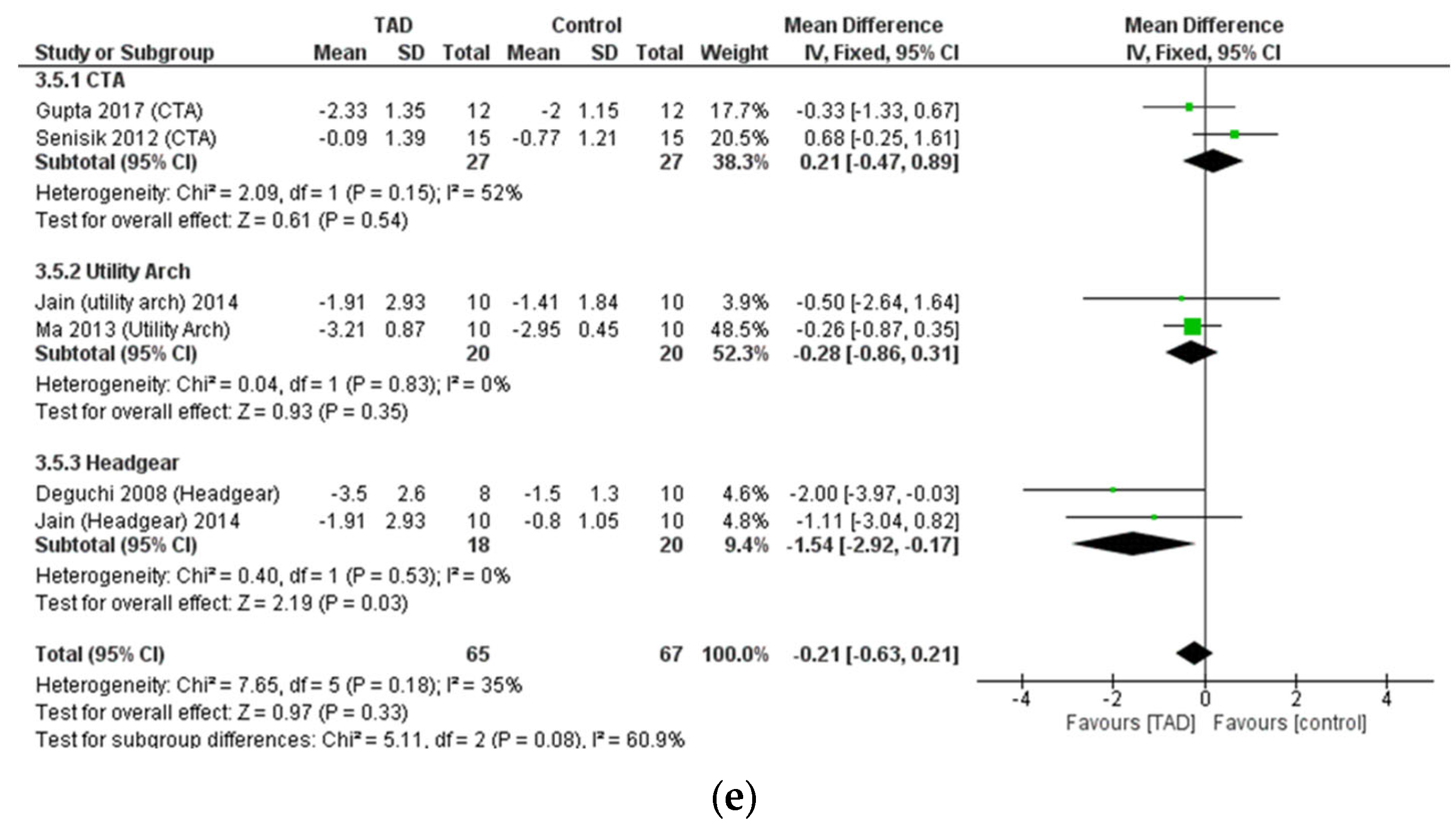
3.5. Meta-Analysis of Skeletal Cephalometric Indices
3.6. Meta-Analysis of Dental Cephalometric Indices
4. Discussion
4.1. Summary of Evidence
4.2. Other Considerations
4.3. Comparison with Other Systematic Reviews
4.4. Implications for Clinical Setting
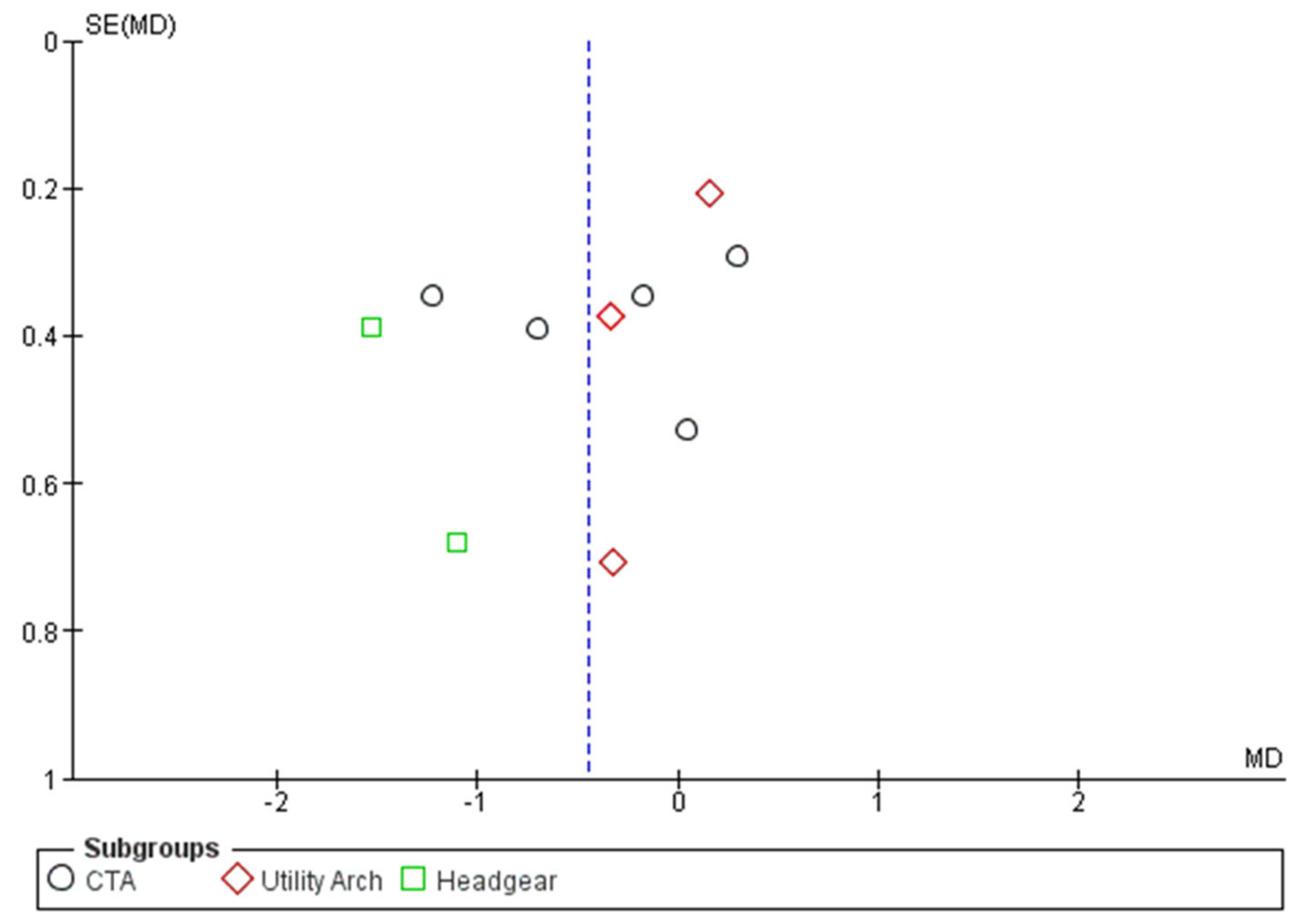
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Quintao, C.C.A.; Miguel, J.A.M.; Brunharo, I.P.; Zanardi, G.; Feu, D. Is traditional treatment a good option for an adult with a Class II deepbite malocclusion? Am. J. Orthod. Dentofac. Orthop. 2012, 141, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.J.; Bates, S.B.; Ehlert, A.A.; Whiting, D.P.; Chen, S.S.-H.; Bollen, A.-M. Stability of deep-bite correction: A systematic review. J. World Fed. Orthod. 2012, 1, e89–e96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhammadi, M.S.; Halboub, E.; Fayed, M.S.; Labib, A.; El-Saaidi, C. Global distribution of malocclusion traits: A systematic review. Dent. Press J. Orthod. 2018, 23, 40.e1–40.e10. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, G. Deep bite its etiology, diagnosis and management: A review. J. Orthod. 2016, 2, 12. [Google Scholar]
- Naini, F.B.; Gill, D.S.; Sharma, A.; Tredwin, C. The aetiology, diagnosis and management of deep overbite. Dent. Update 2006, 33, 326–336. [Google Scholar] [CrossRef]
- Solano-Hernández, B.; Antonarakis, G.S.; Scolozzi, P.; Kiliaridis, S. Combined orthodontic and orthognathic surgical treatment for the correction of skeletal anterior open-bite malocclusion: A systematic review on vertical stability. J. Oral Maxillofac. Surg. 2013, 71, 98–109. [Google Scholar] [CrossRef] [Green Version]
- Hanisch, M.; Hanisch, L.; Kleinheinz, J.; Jung, S. Primary failure of eruption (PFE): A systematic review. Head Face Med. 2018, 14, 5. [Google Scholar] [CrossRef] [Green Version]
- Freitas, K.M.S.; Massaro, C.; Miranda, F.; de Freitas, M.R.; Janson, G.; Garib, D. Occlusal changes in orthodontically treated subjects 40 years after treatment and comparison with untreated control subjects. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 671–685. [Google Scholar] [CrossRef]
- Millett, D.T.; Cunningham, S.J.; D O’Brien, K.; Benson, P.E.; de Oliveira, C.M. Orthodontic treatment for deep bite and retroclined upper front teeth in children. Cochrane Database Syst. Rev. 2018, 2, CD005972. [Google Scholar] [CrossRef] [Green Version]
- Piancino, M.G.; Tortarolo, A.; Di Benedetto, L.; Crincoli, V.; Falla, D. Chewing patterns and muscular activation in deep bite malocclusion. J. Clin. Med. 2022, 11, 1702. [Google Scholar] [CrossRef]
- Khayat, N.; Winocur, E.; Kedem, R.; Winocur Arias, O.; Zaghal, A.; Shpack, N. The prevalence of temporomandibular disorders and dental attrition levels in patients with posterior crossbite and/or deep bite: A preliminary prospective study. Pain Res. Manag. 2021, 2021, 8827895. [Google Scholar] [CrossRef]
- Bhateja, N.K.; Fida, M.; Shaikh, A. Deep Bite Malocclusion: Exploration Of The Skeletal And Dental Factors. J. Ayub Med. Coll. Abbottabad 2016, 28, 449–454. [Google Scholar]
- Al-Zoubi, E.M.; Al-Nimri, K.S. A comparative study between the effect of reverse curve of Spee archwires and anterior bite turbos in the treatment of deep overbite cases: A randomized clinical trial. Angle Orthod. 2022, 92, 36–44. [Google Scholar] [CrossRef]
- Wang, Q.; Chen, W.; Smales, R.J.; Peng, H.; Hu, X.; Yin, L. Apical root resorption in maxillary incisors when employing micro-implant and J-hook headgear anchorage: A 4-month radiographic study. J. Huazhong Univ. Sci. Technol. (Med. Sci.) 2012, 32, 767–773. [Google Scholar] [CrossRef]
- Deguchi, T.; Murakami, T.; Kuroda, S.; Yabuuchi, T.; Kamioka, H.; Takano-Yamamoto, T. Comparison of the intrusion effects on the maxillary incisors between implant anchorage and J-hook headgear. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 654–660. [Google Scholar] [CrossRef]
- Kalra, S.; Tripathi, T. Miniscrew supported Burstone intrusion arch. Int. J. Orthod. (Milwaukee Wis.) 2015, 26, 25–26. [Google Scholar]
- Dahiya, A.; Singh, G. Incisor Intrusion with a Miniscrew-Anchored Segmental Utility Arch. J. Clin. Orthod. JCO 2016, 50, 375–376. [Google Scholar]
- Schwertner, A.; de Almeida, R.R.; de Almeida-Pedrin, R.R.; Fernandes, T.M.F.; Oltramari, P.; de Almeida, M.R. A prospective clinical trial of the effects produced by the Connecticut intrusion arch on the maxillary dental arch. Angle Orthod. 2020, 90, 500–506. [Google Scholar] [CrossRef] [Green Version]
- Davidovitch, M.; Rebellato, J. Two-couple orthodontic appliance systems utility arches: A two-couple intrusion arch. In Proceedings of Seminars in Orthodontics; WB Saunders: Philadelphia, PA, USA, 1995; pp. 25–30. [Google Scholar]
- Sifakakis, I.; Pandis, N.; Makou, M.; Eliades, T.; Bourauel, C. Forces and moments on posterior teeth generated by incisor intrusion biomechanics. Orthod. Craniofacial Res. 2009, 12, 305–311. [Google Scholar] [CrossRef]
- Sharma, S.; Vora, S.; Pandey, V. Clinical evaluation of efficacy of CIA and CNA intrusion arches. J. Clin. Diagn. Res. JCDR 2015, 9, ZC29. [Google Scholar] [CrossRef]
- Al-Sibaie, S.; Hajeer, M.Y. Assessment of changes following en-masse retraction with mini-implants anchorage compared to two-step retraction with conventional anchorage in patients with class II division 1 malocclusion: A randomized controlled trial. Eur. J. Orthod. 2014, 36, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Alteneiji, M.; Liaw, J.J.-L.; Vaid, N.R.; Ferguson, D.J.; Makki, L. Treatment of VME using extra-alveolar TADs: Quantification of treatment effects. In Proceedings of Seminars in Orthodontics; WB Saunders: Philadelphia, PA, USA, 1995; pp. 123–134. [Google Scholar]
- Chang, J.; Mehta, S.; Chen, P.-J.; Upadhyay, M.; Yadav, S. Correction of open bite with temporary anchorage device-supported intrusion. APOS Trends Orthod. 2019, 9, 246–251. [Google Scholar] [CrossRef]
- Hasan, H.S.; Kolemen, A.; Elkolaly, M.; Marya, A.; Gujjar, S.; Venugopal, A. TAD’s for the derotation of 90 rotated maxillary bicuspids. Case Rep. Dent. 2021, 2021, 4285330. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.; Pliska, A.; Busch, C.; Wilmes, B.; Wolf, M.; Drescher, D. Efficacy of orthodontic mini implants for en masse retraction in the maxilla: A systematic review and meta-analysis. Int. J. Implant Dent. 2018, 4, 35. [Google Scholar] [CrossRef] [PubMed]
- Raghis, T.R.; Alsulaiman, T.M.A.; Mahmoud, G.; Youssef, M. Efficiency of maxillary total arch distalization using temporary anchorage devices (TADs) for treatment of Class II-malocclusions: A systematic review and meta-analysis. Int. Orthod. 2022, 20, 100666. [Google Scholar] [CrossRef]
- Davoody, A.R.; Posada, L.; Utreja, A.; Janakiraman, N.; Neace, W.P.; Uribe, F.; Nanda, R. A prospective comparative study between differential moments and miniscrews in anchorage control. Eur. J. Orthod. 2013, 35, 568–576. [Google Scholar] [CrossRef] [Green Version]
- Gomaa, N.E.; Fakhry, N.M.; Elmehy, G.A.; Montasser, M.A. Smile changes after intrusion of maxillary incisors with temporary anchorage devices (TADs) or accentuated compensating curve arch wire. Indian J. Dent. Res. 2019, 30, 531. [Google Scholar] [CrossRef]
- Verma, P.; Jain, R.K. Intrusion Effects on Maxillary Anteriors using Mini Implant Anchorage and K-Sir Loop in Subjects with Deep Overbite-A Cohort Study. J. Clin. Diagn. Res. 2020, 14, 21–25. [Google Scholar] [CrossRef]
- El Namrawy, M.M.; El Sharaby, F.; Bushnak, M. Intrusive arch versus miniscrew-supported intrusion for deep bite correction. Open Access Maced. J. Med. Sci. 2019, 7, 1841. [Google Scholar] [CrossRef] [Green Version]
- Kumar, P.; Datana, S.; Londhe, S.; Kadu, A. Rate of intrusion of maxillary incisors in Class II Div 1 malocclusion using skeletal anchorage device and Connecticut intrusion arch. Med. J. Armed Forces India 2017, 73, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Şenışık, N.E.; Türkkahraman, H. Treatment effects of intrusion arches and mini-implant systems in deepbite patients. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 723–733. [Google Scholar] [CrossRef]
- Polat-Özsoy, Ö.; Arman-Özçırpıcı, A.; Veziroğlu, F.; Çetinşahin, A. Comparison of the intrusive effects of miniscrews and utility arches. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 526–532. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Gupta, N.; Tripathi, T.; Rai, P.; Kanase, A. A comparative evaluation of bite opening by temporary anchorage devices and Connecticut intrusion arch: An in vivo study. Int. J. Orthod. Rehabil. 2017, 8, 129. [Google Scholar]
- GÜRlen, S.; Aras, I. Comparison of the treatment effects of two intrusive mechanics: Connecticut intrusion arch and mini-implant. Turk. Klin. J. Dent. Sci. 2016, 22, 195–201. [Google Scholar] [CrossRef] [Green Version]
- Jain, R.K.; Kumar, S.P.; Manjula, W. Comparison of intrusion effects on maxillary incisors among mini implant anchorage, j-hook headgear and utility arch. J. Clin. Diagn. Res. JCDR 2014, 8, ZC21. [Google Scholar] [CrossRef]
- Ma, D.; Wang, X.; Jin, S.; Dong, R.; Liu, W.; Li, J.; Zhang, J. Comparison of two treatment method for maxillary incisors intrusion. Shanghai Kou Qiang Yi Xue (Shanghai J. Stomatol.) 2013, 22, 206–209. [Google Scholar]
- Vela-Hernández, A.; Gutiérrez-Zubeldia, L.; López-García, R.; García-Sanz, V.; Paredes-Gallardo, V.; Gandía-Franco, J.L.; Lasagabaster-Latorre, F. One versus two anterior miniscrews for correcting upper incisor overbite and angulation: A retrospective comparative study. Prog. Orthod. 2020, 21, 1–10. [Google Scholar] [CrossRef]
- Nayak, U.; Goyal, V.; Godhrawala, F.; Saxena, R. Comparison of skeletodental changes occurring during deep overbite correction with mini-implant anchorage system and the utility arches reinforced by a transpalatal arch. J. Indian Orthod. Soc. 2011, 46, 9–14. [Google Scholar] [CrossRef]
- Liou, E.J.; Chang, P.M. Apical root resorption in orthodontic patients with en-masse maxillary anterior retraction and intrusion with miniscrews. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 207–212. [Google Scholar] [CrossRef]
- Albajes-Eizagirre, A.; Solanes, A.; Radua, J. Meta-analysis of non-statistically significant unreported effects. Stat. Methods Med. Res. 2019, 28, 3741–3754. [Google Scholar] [CrossRef]
- Karagöz, A. Derin Örtülü Kapanışlı Olgularda Üst Keser Intrüzyonunun Konik Işınlı Bilgisayarlı Tomografi ile İncelenmesi. 2013. Available online: openaccess.hacettepe.edu.tr (accessed on 1 November 2022).
- St. Martin, J.; Javed, F.; Rossouw, P.; Michelogiannakis, D. Influence of mini-screw implant-assisted intrusion on orthodontically induced inflammatory root resorption: A systematic review. Eur. Arch. Paediatr. Dent. 2021, 22, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Jayaratne, Y.S.N.; Uribe, F.; Janakiraman, N. Maxillary incisors changes during space closure with conventional and skeletal anchorage methods: A systematic review. J. Istanb. Univ. Fac. Dent. 2017, 51, S90. [Google Scholar] [PubMed]
- Van Steenbergen, E.; Burstone, C.; Prahl-Andersen, B.; Aartman, I. The influence of force magnitude on intrusion of the maxillary segment. Angle Orthod. 2005, 75, 723–729. [Google Scholar] [PubMed]
- Liatti, S.J. Effects of Wire Material, Deflection, and Interbracket Distance on Burstone Bracket Geometry Force Systems; Loma Linda University: Loma Linda, CA, USA, 2017. [Google Scholar]
- Lee, S.-Y.; Vang, M.-S.; Yang, H.-S.; Park, S.-W.; Park, H.-O.; Lim, H.-P. Shear bond strength of composite resin to titanium according to various surface treatments. J. Adv. Prosthodont. 2009, 1, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Atalla, A.I.; AboulFotouh, M.H.; Fahim, F.H.; Foda, M.Y. Effectiveness of orthodontic mini-screw implants in adult deep bite patients during incisor intrusion: A systematic review. Contemp. Clin. Dent. 2019, 10, 372. [Google Scholar] [CrossRef]
- Sosly, R.; Mohammed, H.; Rizk, M.Z.; Jamous, E.; Qaisi, A.G.; Bearn, D.R. Effectiveness of miniscrew-supported maxillary incisor intrusion in deep-bite correction: A systematic review and meta-analysis. Angle Orthod. 2020, 90, 291–304. [Google Scholar] [CrossRef] [Green Version]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database of Published Trials, Dissertations, and Conference Proceedings | Search Strategy Used | Hits |
|---|---|---|
| MEDLINE searched via PubMed searched on 12 September 2022, via www.ncbi.nlm.nih.gov/sites | #1 TAD OR temporary anchorage device OR mini?screw OR micro?implant OR mini?plate OR titanium plate OR surgical plate OR skeletal anchorage 58,286 #2 anterior impaction OR incisor intrusion OR incisal intrusion OR deep?bite OR deep overbite OR gummy smile OR short face OR anterior intrusion 18,346 #3 #1 AND #2 434 | 441 |
| Web of Science Core Collection was searched via Web of Knowledge on 12 September 2022, via apps.webofknowledge.com | #1 TS = (TAD OR temporary anchorage device OR mini?screw OR #2 micro implant OR surgical miniplate OR mini?plate) 14,669 TS = (anterior intrusion OR incisal intrusion OR deep?bite OR short face) 37,935 #3 #1 AND #2 85 | 85 |
| EMBASE searched via Ovid on 13 September 2022, via http://ovidsp.dc2.ovid.com | (tad OR ‘temporary anchorage device’/exp OR ‘temporary anchorage device’ OR ‘miniscrew’/exp OR ‘miniscrew’ OR ‘miniplate’/exp OR ‘miniplate’) AND (((‘overbite’/exp OR ‘overbite’ OR ‘incisor’/exp OR incisor) AND (‘intrusion’/exp OR intrusion) OR incisal) AND (‘intrusion’/exp OR intrusion) OR short?face) | 53 |
| Scopus searched via Scopus on 10 September 2022, via https://www.scopus.com | TITLE-ABS-KEY(TAD OR temporary anchorage device OR mini?plate OR mini?screw OR skeletal anchorage) AND ALL(deep?bite OR incis* intrusion OR short?face) | 119 |
| Cochrane Central Register of Controlled Trials searched via the Cochrane Library Searched on 15 September 2022, via www.thecochranelibrary.com | #1→TAD→274 #2→temporary anchorage device→23 #3→mini?plate→121 #4→mini?screw→134 #5→deep?bite→10 #6→anterior intrusion→65 #7→incisal intrusion→6 #8→incisor intrusion→49 #9→(#1 OR #2 OR #3 OR #4) AND (#5 OR #6 OR #7 OR #8)→12 | 12 |
| Total | 710 |
| Author Year | Study Design | Sample Size | Gender | Age | Malocclusion | Number of Mini-Screws | Mini-Screw Placement | Force | Assessment | Group | Subjects |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Deguchi 2008 | Retro Cohort | 18 | 2 M; 16 F | 20.7 ± 2.5 (headgear); 21.5 ± 3.7 (mini-screw) | NR (probably Cl II) | 2, 1.5 × 6 mm | Between central and lateral | 100 gMS and HG | Root resorption; intrusion duration; cephalometric (angular; linear) | Mini-screw | 8 |
| Headgear | 10 | ||||||||||
| El Namrawy, 2019 | RCT | 30 | 9 M; 21 F | 15.3 ± 1 (mini-screw) 14.8 ± 1 (intrusive arch) | Class I or Class II | 2, 1.4 × 6 mm | Between lateral and canine | 100 gr | Pain; cast measurements (overbite; over jet; inter-canine width; inter-molar width); cephalometric (skeletal; dental; soft tissue) | Mini-screw | 15 |
| Intrusive arch (segmental) | 15 | ||||||||||
| Gomaa, 2019 | Retro cohort | 20 | 2 M; 18 F | 18–24 | Class I or II | 2, 1.3–1.6 × 6–8 mm | Between central and lateral | NR | Smile analysis; overbite; overjet; cephalometric | Mini-screw | 10 |
| Curve of spee arch wire, both dentitions | 10 | ||||||||||
| Gupta, 2017 | Prospective cohort | 24 | NR | 17.75 ± 3.49 (mini-screw) 18.75 ± 3.47 (intrusive arch) | NR | 2, 1.3 × 8 mm | Between lateral and canine | 30 gr per side (60 gr) | Overbite; cephalometric (angular; linear) | Mini-screw | 12 |
| Connecticut intrusion arch | 12 | ||||||||||
| Gurlen, 2016 | RCT | 32 | 16 M; 16 F | 14.65 | NR | 2, 1.4 × 7 mm | Between central and lateral | 60 gr for both | Cephalometric (dental; skeletal); root resorption | Mini-screw | 16 |
| Connecticut intrusion arch | 16 | ||||||||||
| Jain, 2014 | RCT | 30 | 11 M; 19 F | 16–22 | NR | 2, 1.4 × 6 mm | Between central and lateral | 1.5 ounces per side (80 gr) for MS, UA; 2 for J hook | Overjet, overbite, cephalometric (dental) | Mini-screw | 10 |
| Headgear | 10 | ||||||||||
| Utility arch | 10 | ||||||||||
| Karagoz, 2013 | RCT | 25 | 11 M; 14 F | 18.2 ± 3.3 | NR | 2, 1.4 × 8 mm | Between central and lateral | 100 gr | Overjet, overbite, cephalometric (dental; skeletal); root resorption | Mini-screw | 13 |
| Segmental + TPA | 12 | ||||||||||
| Nayak, 2011 | Prospective cohort | 14 | NR | NR | NR | 1, 2 × 8 mm | In the midline in the frenum region | 50 gr | Cephalometric (dental) | Mini-implant | 7 |
| Utility arch | 7 | ||||||||||
| Kumar, 2015 | Prospective cohort | 30 | NR | 15–20 | Class II Div 1 | 2, 1.3 × 7 mm | Between central and lateral | 60 gr for both | Cephalometric (dental) | Mini-screw | 15 |
| Connecticut intrusion arch | 15 | ||||||||||
| Liou, 2010 | Retro cohort | 50 | 4 M; 46 F | 25.4 ± 5.6 | NR | 2, 2 × 9 mm | Infrazygomatic | 100 gr intrusive, 250 gr retractive | Root resorption | Mini-screw Anchorage | 30 |
| Control | 20 | ||||||||||
| Ma, 2013 | RCT | 20 | NR | 22.41 ± 2.02 | NR | 2, 1.6 × 8 mm | Between central and lateral | 50 gr | Overjet; overbite; cephalometric (dental; skeletal) | Mini-screw | 10 |
| Utility arch | 10 | ||||||||||
| Polat-Ozsoy, 2009 | Prospective cohort | 24 | 10 M; 14 F | 20.90 ± 7.12 (mini-screw) 15.25 ± 3.93 (utility arch) | NR | 2, 1.2 × 6 mm | Between lateral and canine | 50 gr mini-screw | Overjet; overbite; cephalometric (dental; skeletal) | Mini-screw | 13 |
| Utility arch | 11 | ||||||||||
| Senisik, 2012 | RCT | 45 | 19 M; 26 F) | 20.29 ± 3.12 | Class II Division 2 | 2, 1.3 × 5 mm | Between lateral and canine | 90 gr mini-screw; 60 gr CTA | Overjet; overbite; cephalometric (dental; skeletal) | Mini-screw | 15 |
| Connecticut intrusion arch | 15 | ||||||||||
| Control | 15 | ||||||||||
| Vela-Hernández, 2020 | Retro cohort | 44 | 20 M; 24 F | 36.6 ± 4.9 | Class I | 1/2, both 1.6 × 8 mm | In midline/Between lateral and canine | 90 gr per mini-screw | Overbite; cephalometric (dental; skeletal) | One mini-screw | 16 |
| Two mini-Screws | 28 | ||||||||||
| Verma, 2020 | Prospective cohort | 12 | NR | 29.5 ± 2.1 | Class I or Class II Div 1 | 2, 1.3 × 8 mm | Between central and lateral | 30 gr each side | Cephalometric (dental) | Mini-screw | 6 |
| K-SIR loop | 6 |
| Certainty Assessment | № of Patients | Effect | Certainty | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | TAD | Other Treatment Methods | Relative (95% CI) | Absolute (95% CI) | ||
| Overbite | ||||||||||||
| 10 | Observational studies | Not serious | Serious a | Not serious | Not serious | None | 122 | 121 | - | MD 0.45 lower (0.87 lower to 0.03 lower) | ⨁⨁⨁◯ Moderate | |
| Overjet | ||||||||||||
| 8 | Observational studies | Not serious | Serious a | Not serious | Not serious a | None | 96 | 91 | - | MD 0.07 lower (0.72 lower to 0.58 higher) | ⨁⨁⨁◯ Moderate | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bardideh, E.; Tamizi, G.; Shafaee, H.; Rangrazi, A.; Ghorbani, M.; Kerayechian, N. The Effects of Intrusion of Anterior Teeth by Skeletal Anchorage in Deep Bite Patients; A Systematic Review and Meta-Analysis. Biomimetics 2023, 8, 101. https://doi.org/10.3390/biomimetics8010101
Bardideh E, Tamizi G, Shafaee H, Rangrazi A, Ghorbani M, Kerayechian N. The Effects of Intrusion of Anterior Teeth by Skeletal Anchorage in Deep Bite Patients; A Systematic Review and Meta-Analysis. Biomimetics. 2023; 8(1):101. https://doi.org/10.3390/biomimetics8010101
Chicago/Turabian StyleBardideh, Erfan, Golnaz Tamizi, Hooman Shafaee, Abdolrasoul Rangrazi, Mahsa Ghorbani, and Navid Kerayechian. 2023. "The Effects of Intrusion of Anterior Teeth by Skeletal Anchorage in Deep Bite Patients; A Systematic Review and Meta-Analysis" Biomimetics 8, no. 1: 101. https://doi.org/10.3390/biomimetics8010101