
Occupational Dermatitis Treated with Alitretinoin

 ,
, {kind=link}
{kind=link}
Abstract
:1. Introduction
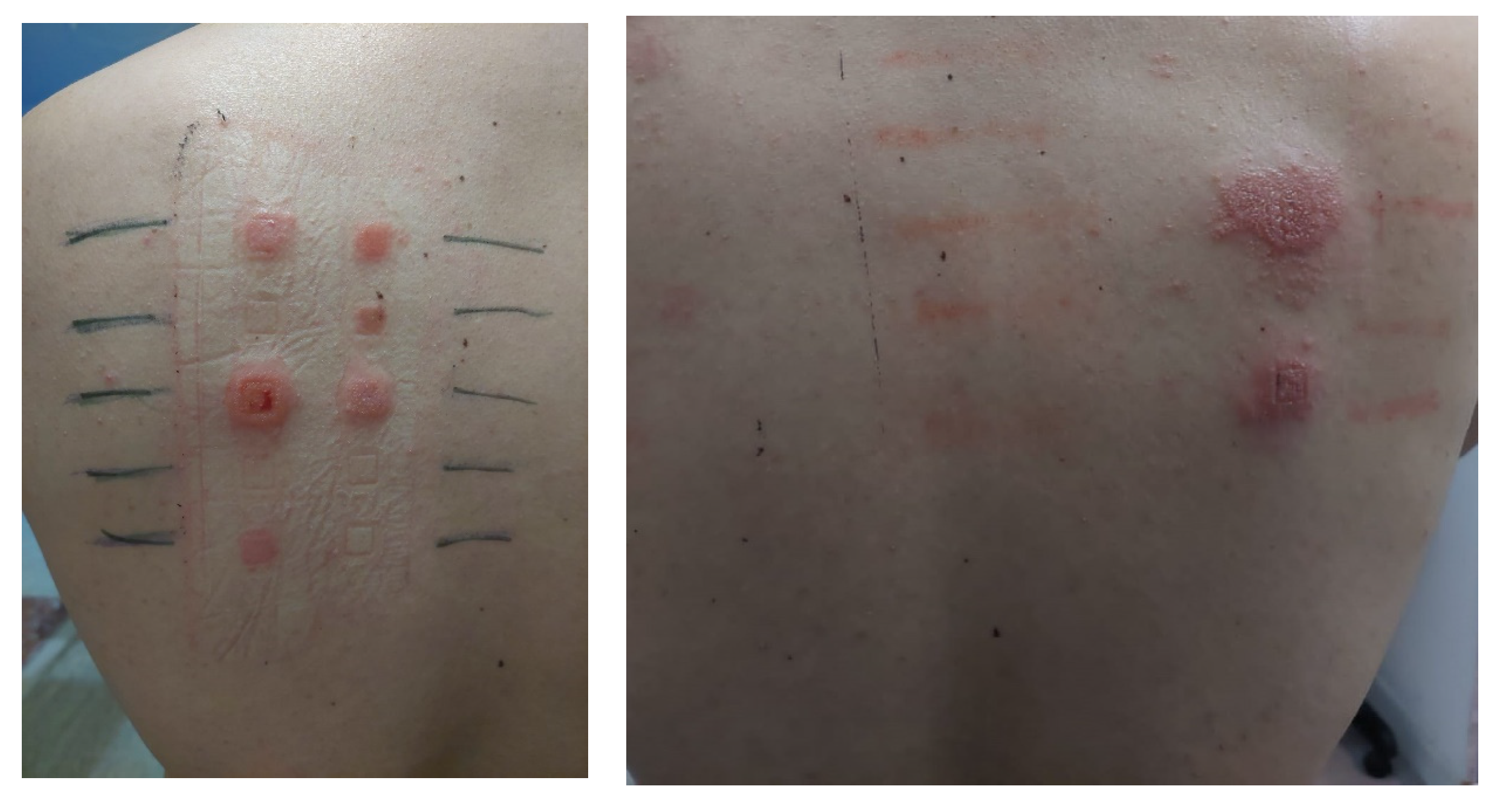
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Piapan, L.; Mauro, M.; Martinuzzo, C.; Larese Filon, F. Characteristics and incidence of contact dermatitis among hairdressers in north-eastern Italy. Contact Dermat. 2020, 83, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Lyons, G.; Roberts, H.; Palmer, A.; Matheson, M.; Nixon, R. Hairdressers presenting to an occupational dermatology clinic in Melbourne, Australia. Contact Dermat. 2013, 68, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.; Marks, J.G.; Flamm, A. Occupational Contact Dermatitis: Common Occupational Allergens. Derm. Clin. 2020, 38, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Warshaw, E.M.; Ruggiero, J.L.; DeKoven, J.G.; Maibach, H.I.; Atwater, A.R.; Taylor, J.S.; Zug, K.A.; Reeder, M.J.; Silverberg, J.I.; Sasseville, D.; et al. Contact Dermatitis Associated With Hair Care Products: A Retrospective Analysis of the North American Contact Dermatitis Group Data, 2001–2016. Dermat. Contact Atopic. Occup. Drug. 2022, 33, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Holness, D.L. Occupational Dermatitis and Urticaria. Immunol. Allergy Clin. North Am. 2021, 41, 439–453. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Nixon, R. Occupational skin disease in hairdressers. Australas J. Dermatol. 2001, 42, 1–6, quiz 7–8. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, R.L.; White, I.R.; Mc Fadden, J.P.; White, J.M.L. Hairdressers with dermatitis should always be patch tested regardless of atopy status. Contact Dermat. 2010, 62, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Thyssen, J.P.; Schuttelaar, M.L.A.; Alfonso, J.H.; Andersen, K.E.; Angelova-Fischer, I.; Arents, B.W.M.; Bauer, A.; Brans, R.; Cannavo, A.; Christoffers, W.A.; et al. Guidelines for diagnosis, prevention, and treatment of hand eczema. Contact Dermat. 2022, 86, 357–378. [Google Scholar] [CrossRef] [PubMed]
- Bubna, A.K. Alitretinoin in Dermatology—An Update. Indian J. Dermatol. 2015, 60, 520. [Google Scholar] [CrossRef] [PubMed]
- Dubin, C.; Del Duca, E.; Guttman-Yassky, E. Drugs for the Treatment of Chronic Hand Eczema: Successes and Key Challenges. Ther. Clin. Risk Manag. 2020, 16, 1319–1332. [Google Scholar] [CrossRef] [PubMed]
- Kislat, A.; Meller, S.; Mota, R.; Gerber, P.A.; Buhren, B.A.; Bünemann, E.; Wiesner, U.; Ruzicka, T.; Homey, B. Alitretinoin—molecular and cellular mechanisms of action. J. Transl. Med. 2011, 9 (Suppl. 2), 16. [Google Scholar] [CrossRef] [Green Version]
- Christoffers, W.A.; Coenraads, P.; Svensson, Å.; Diepgen, T.L.; Dickinson-Blok, J.L.; Xia, J.; Williams, H.C. Interventions for hand eczema. Cochrane. Database Syst. Rev. 2019, 2019, CD004055. [Google Scholar] [CrossRef] [PubMed]
- King, T.; McKenna, J.; Alexandroff, A.B. Alitretinoin for the treatment of severe chronic hand eczema. Patient Prefer. Adherence 2014, 8, 1629–1634. [Google Scholar] [PubMed] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tammaro, A.; Chello, C.; Parisella, F.R.; Adebanjo, G.A.R. Occupational Dermatitis Treated with Alitretinoin. Allergies 2022, 2, 75-79. https://doi.org/10.3390/allergies2030007
Tammaro A, Chello C, Parisella FR, Adebanjo GAR. Occupational Dermatitis Treated with Alitretinoin. Allergies. 2022; 2(3):75-79. https://doi.org/10.3390/allergies2030007
Chicago/Turabian StyleTammaro, Antonella, Camilla Chello, Francesca Romana Parisella, and Ganiyat Adenike Ralitsa Adebanjo. 2022. "Occupational Dermatitis Treated with Alitretinoin" Allergies 2, no. 3: 75-79. https://doi.org/10.3390/allergies2030007