
Transverse Analysis of Maxilla and Mandible in Adults with Normal Occlusion: A Cone Beam Computed Tomography Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Orientation
2.3. Transverse Width Measurements
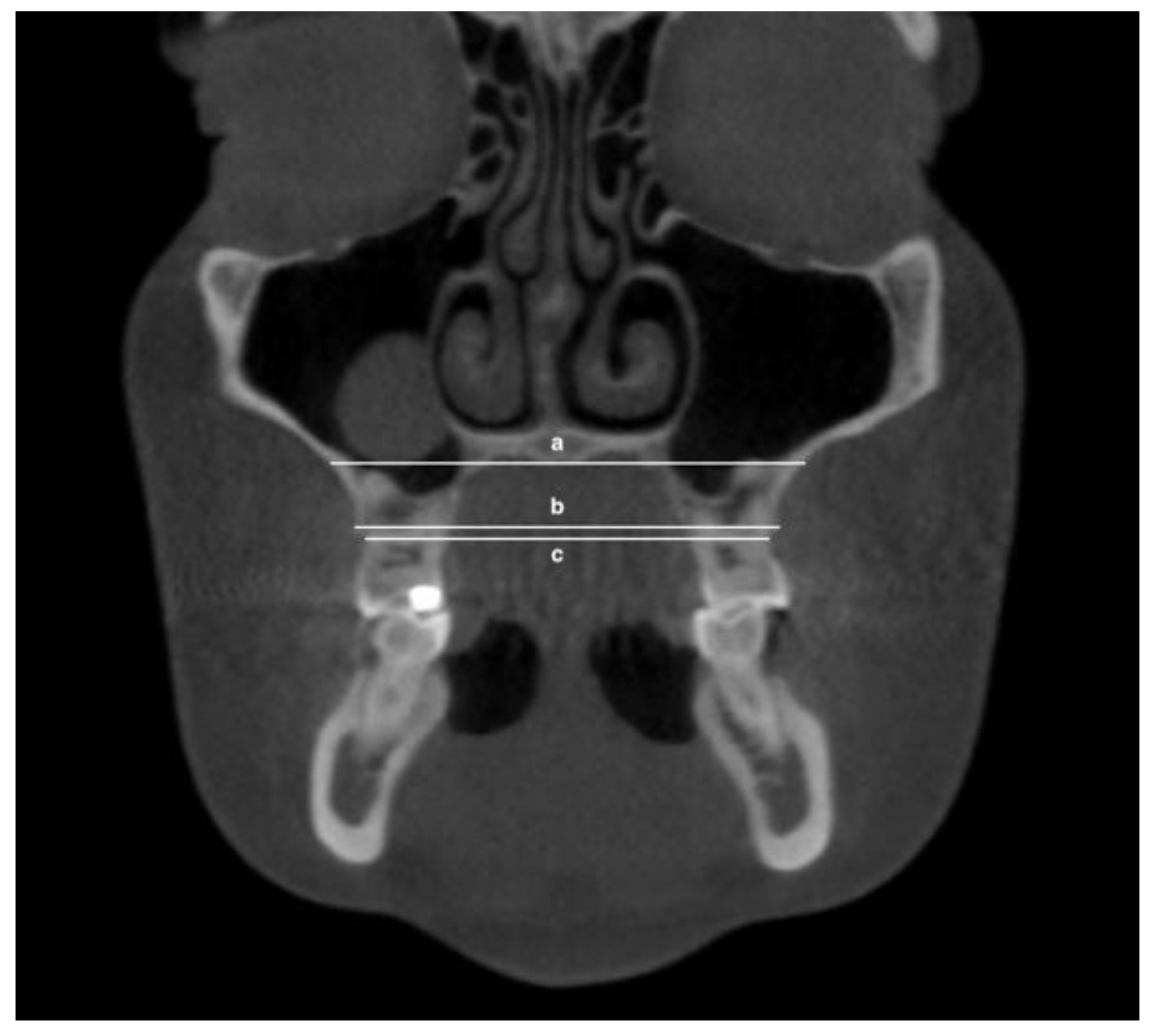
- Maxillary inter-buccal bone widths: from the right to the left points at the level of hard palate, alveolar crest and furcation (Figure 1)
- Maxillary inter-lingual bone widths: from the right to the left points at the level of alveolar crest and furcation (Figure 2)
- Mandibular inter-buccal bone widths: from the right to the left points at the level of alveolar crest and furcation (Figure 3)
- Mandibular inter-lingual bone widths: from the right to the left points at the level of alveolar crest and furcation (Figure 4)
- The differentials of maxillomandibular inter-buccal bone or inter-lingual bone widths were calculated by subtracting mandibular measurements from maxillary measurements at the same level of the first molar.
2.4. Tooth Inclination Measurements
2.5. Statistical Analysis
3. Results
3.1. Transverse Width Measurements
3.2. Differentials of Transverse Width Measurements
3.3. Tooth Inclination Measurements
3.4. Correlation between Differentials of Transverse Width and Tooth Inclination
4. Discussion
5. Conclusions
- Males’ maxillary and mandibular inter-buccal bone and inter-lingual bone widths on the first molars are wider than the corresponding females’ widths.
- At the level of furcation of the first molars, on average, maxillary inter-buccal bone width is slightly wider than mandibular buccal width by 1.1 mm for males and 1.6 mm for females. The maxillary inter-lingual bone width is slightly narrower than mandibular lingual width, by 1.3 mm for males and 0.3 mm for females.
- Maxillary first molars exhibited buccal inclination of 5.3°, whereas the mandibular first molar exhibited lingual inclination of 14.4°.
- A correlation exists between the maxillomandibular differential of inter-buccal and inter-lingual widths and upper and lower first molar inclinations.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ricketts, R.M.; Roth, H.R.; Chaconas, S.P.L.; Schulhof, J.R.; Engle, G.A. Orthodontic Diagnosis and Planning, 1st ed.; Rocky Mountain Communications: Kittredge, CO, USA, 1982. [Google Scholar]
- Ricketts, R.M.; Grummons, D. Frontal cephalometrics: Practical applications, part 1. World J. Orthod. 2003, 4, 297–316. [Google Scholar]
- Wagner, D.M.; Chung, C.H. Transverse growth of the maxilla and mandible in untreated girls with low, average, and high MP-SN angles: A longitudinal study. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Perrotti, G.; Politi, M.; Testori, T. 3D Imaging and Dentistry-From Multiplanar Cephalometry to Guided Navigation in Implantology; Quintessenza Edizione: Milan, Italy, 2014. [Google Scholar]
- Perrotti, G.; Politi, M.; Testori, T. Analisi Cefalometrica 3D: La Ricerca di Valori Norma; Quintessenza Edizioni Srl: Rho, Italy, 2016; Volume 32. [Google Scholar]
- Perrotti, G.; Baccaglione, G.; Clauser, T.; Scaini, R.; Grassi, R.; Testarelli, L.; Reda, R.; Testori, T.; Del Fabbro, M. Total Face Approach (TFA) 3D Cephalometry and Superimposition in Orthognathic Surgery: Evaluation of the Vertical Dimensions in a Consecutive Series. Methods Protoc. 2021, 4, 36. [Google Scholar] [CrossRef] [PubMed]
- McNamara, J.A.; Brudon, W.L. Orthodontic and Orthopedic Treatment in the Mixed Dentition; Needham Press: Ann Arbor, MI, USA, 1993. [Google Scholar]
- Andrews, L.F. The Six Elements of Orofacial Harmony; Andrews, J., Ed.; The Andrews Foundation: Cleverland, OH, USA, 2000; Volume 1. [Google Scholar]
- Major, P.W.; Johnson, D.E.; Hesse, K.L.; Glover, K.E. Landmark identification error in posterior anterior cephalometrics. Angle Orthod. 1994, 64, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Thurow, R.C. Cephalometric methods in research and private practice. Angle Orthod. 1951, 21, 104–116. [Google Scholar] [CrossRef] [PubMed]
- Major, P.W.; Johnson, D.E.; Hesse, K.L.; Glover, K.E. Effect of head orientation on posterior anterior cephalometric landmark identification. Angle Orthod. 1996, 66, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Ghafari, J.; Cater, P.E.; Shofer, F.S. Effect of film-object distance on posteroanterior cephalometric measurements: Suggestions for standardized cephalometric methods. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 30–37. [Google Scholar] [CrossRef]
- Alhammadi, M.S.; Al-Mashraqi, A.A.; Alnami, R.H.; Ashqar, N.M.; Alamir, O.H.; Halboub, E.; Reda, R.; Testarelli, L.; Patil, S. Accuracy and Reproducibility of Facial Measurements of Digital Photographs and Wrapped Cone Beam Computed Tomography (CBCT) Photographs. Diagnostics 2021, 11, 757. [Google Scholar] [CrossRef] [PubMed]
- Alkhatib, R.; Chung, C.H. Buccolingual inclination of first molars in untreated adults: A CBCT study. Angle Orthod. 2017, 87, 598–602. [Google Scholar] [CrossRef] [PubMed]
- Barrera, J.M.; Llamas, J.M.; Espinar, E.; Saenz-Ramirez, C.; Paredes, V.; Perez-Varela, J.C. Wilson maxillary curve analyzed by CBCT. A study on normocclusion and malocclusion individuals. Med. Oral. Patol. Oral. Cir. Bucal. 2013, 18, e547–e552. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Chung, C.H. Buccolingual inclination of molars in untreated children and adults: A cone beam computed tomography study. Angle Orthod. 2019, 89, 87–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yi, L.; Jeon, H.H.; Li, C.; Boucher, N.; Chung, C.H. Transverse Growth of the Maxillo-Mandibular Complex in Untreated Children: A Longitudinal Cone Beam Computed Tomography Study. Sensors 2021, 21, 6378. [Google Scholar] [CrossRef]
- Miner, R.M.; Al Qabandi, S.; Rigali, P.H.; Will, L.A. Cone-beam computed tomography transverse analysis. Part I: Normative data. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 300–307. [Google Scholar] [CrossRef]
- Miner, R.M.; Al Qabandi, S.; Rigali, P.H.; Will, L.A. Cone-beam computed tomography transverse analyses. Part 2: Measures of performance. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Masumoto, T.; Hayashi, I.; Kawamura, A.; Tanaka, K.; Kasai, K. Relationships among facial type, buccolingual molar inclination, and cortical bone thickness of the mandible. Eur. J. Orthod. 2001, 23, 15–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okeson, J.P. Management of Temporomandibular Disorders and Occlusion, 7th ed.; Elsevier: St. Louis, MO, USA, 2012. [Google Scholar]
- Nanda, R. Biomechanics and Esthetic Strategies in Clinical Orthodontics; Elsevier Saunders: St. Louis, MO, USA, 2005. [Google Scholar]
- Dawson, P.E. Functional Occlusion: From TMJ to Smile Design; Mosby: St. Louis, MO, USA, 2007. [Google Scholar]
- Janson, G.; Bombonatti, R.; Cruz, K.S.; Hassunuma, C.Y.; Del Santo, M., Jr. Buccolingual inclinations of posterior teeth in subjects with different facial patterns. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Tsunori, M.; Mashita, M.; Kasai, K. Relationship between facial types and tooth and bone characteristics of the mandible obtained by CT scanning. Angle Orthod. 1998, 68, 557–562. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measurement | n | Mean (mm) | SD a (mm) | Min (mm) | Max (mm) |
|---|---|---|---|---|---|
| Maxillary inter-buccal bone width at hard palate | 12 | 62.4 | 3.9 | 57.0 | 68.1 |
| Maxillary inter-buccal bone width at alveolar crest of first molar | 12 | 54.7 | 3.5 | 47.5 | 62 |
| Maxillary inter-buccal bone width at furcation of first molar | 12 | 58.9 | 3.5 | 52.2 | 66.1 |
| Maxillary inter-lingual bone width at alveolar crest | 12 | 34.8 | 3.4 | 27.6 | 41.4 |
| Maxillary inter-lingual bone width at furcation of first molar | 12 | 30.9 | 2.8 | 24.5 | 33.7 |
| Mandibular inter-buccal bone width at alveolar crest of first molar | 12 | 53.8 | 2.7 | 50.0 | 58.4 |
| Mandibular inter-buccal bone width at furcation of first molar | 12 | 57.8 | 3.0 | 53.3 | 62.8 |
| Mandibular inter-lingual bone width at alveolar crest of first molar | 12 | 35.1 | 2.6 | 30.1 | 40.3 |
| Mandibular inter-lingual bone width at furcation of first molar | 12 | 32.2 | 2.9 | 27.7 | 37.5 |
| Measurement | n | Mean (mm) | SD a (mm) | Min (mm) | Max (mm) |
|---|---|---|---|---|---|
| Maxillary inter-buccal bone width at hard palate | 44 | 58.7 | 3.7 | 51.7 | 68.3 |
| Maxillary inter-buccal bone width at alveolar crest of first molar | 44 | 52.7 | 2.8 | 44.9 | 60.4 |
| Maxillary inter-buccal bone width at furcation of first molar | 44 | 56.5 | 3.5 | 49.1 | 66.8 |
| Maxillary inter-lingual bone width at alveolar crest of first molar | 44 | 32.9 | 2.4 | 26 | 40.1 |
| Maxillary inter-lingual bone width at furcation of first molar | 44 | 29.5 | 2.3 | 24.1 | 34.2 |
| Mandibular inter-buccal bone width at alveolar crest of first molar | 44 | 51.6 | 2.9 | 43.3 | 58.0 |
| Mandibular inter-buccal bone width at furcation of first molar | 44 | 54.9 | 3.2 | 47.2 | 61.1 |
| Mandibular inter-lingual bone width at alveolar crest of first molar | 44 | 33.5 | 2.4 | 28.0 | 38.1 |
| Mandibular inter-lingual bone width at furcation of first molar | 44 | 29.8 | 2.9 | 22.7 | 36.3 |
| Differentials for Male | Mean (mm) | SD a (mm) | Min (mm) | Max (mm) |
| Intrer-buccal bone width at alveolar crest | 0.9 | 3.2 | −4.7 | 6.0 |
| Inter-buccal bone width at furcation | 1.1 | 4.5 | −7.3 | 7.0 |
| Inter-lingual bone width at alveolar crest | −0.4 | 4.1 | −9.4 | 5.7 |
| Inter-lingual bone width at furcation | −1.3 | 3.6 | −10 | 3.1 |
| Differentials for Female | Mean (mm) | SD a (mm) | Min (mm) | Max (mm) |
| Inter-buccal bone width at alveolar crest | 1.1 | 2.2 | −3.3 | 7.8 |
| Inter-buccal bone width at furcation | 1.6 | 2.9 | −4.6 | 8.4 |
| Inter-lingual bone width at alveolar crest | −0.6 | 2.4 | −6.7 | 4.4 |
| Inter-lingual bone width at furcation | −0.3 | 3.2 | −5.9 | 7.8 |
| Measurement | n | Mean (°) | SD a (°) | Min (°) | Max (°) |
|---|---|---|---|---|---|
| Maxillary right first molar | 56 | 4.2 | 5.9 | −10.5 | 16.1 |
| Maxillary left first molar | 56 | 6.5 | 6.3 | −9.2 | 21.6 |
| Average, maxillary first molar | 112 | 5.3 | 6.2 | −10.5 | 21.6 |
| Mandibular right first molar | 56 | −13.9 | 5.1 | −23.4 | −5.5 |
| Mandibular left first molar | 56 | −14.9 | 5.2 | −31.4 | −2.5 |
| Average, mandibular first molar | 112 | −14.4 | 5.2 | −31.4 | −2.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.J.; Jeon, H.H.; Boucher, N.; Chung, C.-H. Transverse Analysis of Maxilla and Mandible in Adults with Normal Occlusion: A Cone Beam Computed Tomography Study. J. Imaging 2022, 8, 100. https://doi.org/10.3390/jimaging8040100
Lee KJ, Jeon HH, Boucher N, Chung C-H. Transverse Analysis of Maxilla and Mandible in Adults with Normal Occlusion: A Cone Beam Computed Tomography Study. Journal of Imaging. 2022; 8(4):100. https://doi.org/10.3390/jimaging8040100
Chicago/Turabian StyleLee, Kyung Jin, Hyeran Helen Jeon, Normand Boucher, and Chun-Hsi Chung. 2022. "Transverse Analysis of Maxilla and Mandible in Adults with Normal Occlusion: A Cone Beam Computed Tomography Study" Journal of Imaging 8, no. 4: 100. https://doi.org/10.3390/jimaging8040100