
Remote Training for Medical Staff in Low-Resource Environments Using Augmented Reality

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Clinical Background
1.2. Related Works
2. Materials & Methods
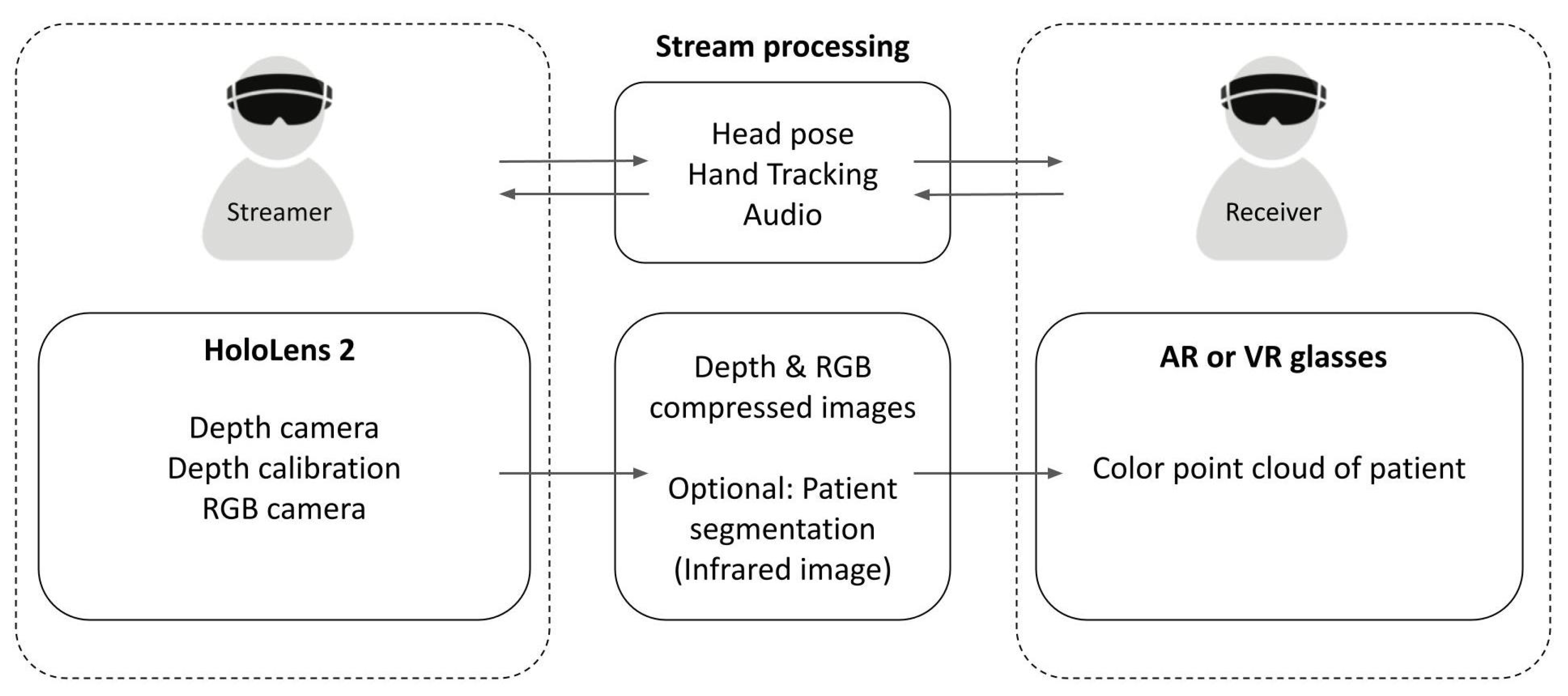
2.1. Streaming Application
2.2. Server
2.3. Receiving Application
2.4. Experimental Design
3. Results & Discussion
3.1. Technical Evaluation
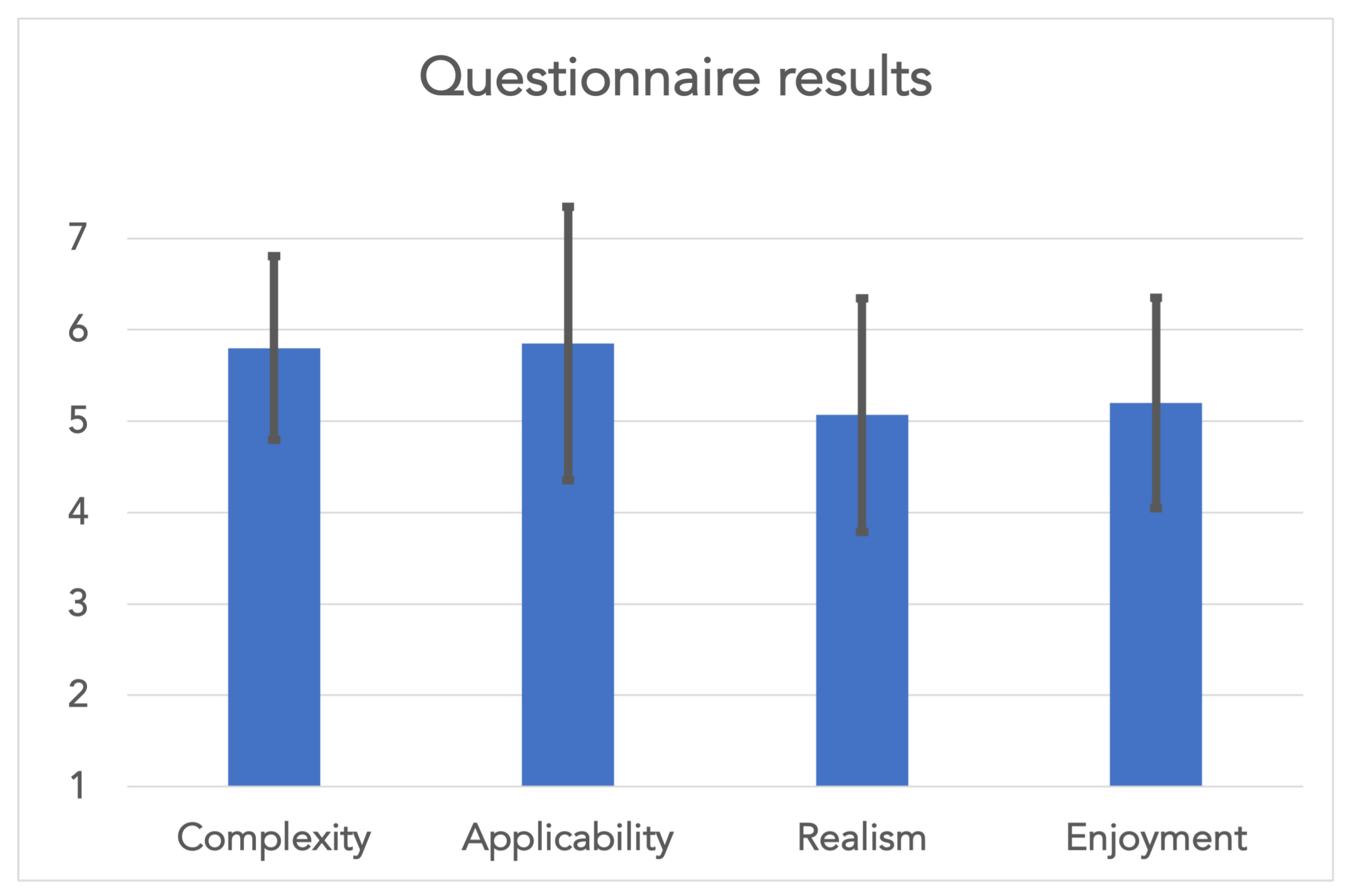
3.2. Pilot Study
3.3. Remote Teaching
3.4. Patching a Remote Specialist
3.5. Limitations
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AR | Augmented reality |
| FPS | Frames per second |
| HMD | Head-mounted display |
| IR | Infrared |
| RGB | Red, green, blue |
| SDK | Software development kit |
| SLAM | Simultaneous localization and mapping |
| VR | Virtual reality |
| WHO | World Health Organization |
References
- Azimi, E.; Winkler, A.; Tucker, E.; Qian, L.; Sharma, M.; Doswell, J.; Navab, N.; Kazanzides, P. Evaluation of Optical See-Through Head-Mounted Displays in Training for Critical Care and Trauma. In Proceedings of the 25th IEEE Conference on Virtual Reality and 3D User Interfaces, Reutlingen, Germany, 18–22 March 2018; pp. 511–512. [Google Scholar] [CrossRef]
- Leuze, C.; Zoellner, A.; Schmidt, A.R.; Cushing, R.E.; Fischer, M.J.; Joltes, K.; Zientara, G.P. Augmented reality visualization tool for the future of tactical combat casualty care. J. Trauma Acute Care Surg. 2021, 91, S40–S45. [Google Scholar] [CrossRef] [PubMed]
- Ellard, D.R.; Shemdoe, A.; Mazuguni, F.; Mbaruku, G.; Davies, D.; Kihaile, P.; Pemba, S.; Bergström, S.; Nyamtema, A.; Mohamed, H.M.; et al. Can training non-physician clinicians/associate clinicians (NPCs/ACs) in emergency obstetric, neonatal care and clinical leadership make a difference to practice and help towards reductions in maternal and neonatal mortality in rural Tanzania? The ETATMBA project. BMJ Open 2016, 6, e008999. [Google Scholar]
- Snowden, J.M.; Muoto, I. Strengthening the health care workforce in Fragile States: Considerations in the Health Care Sector and Beyond. Health Serv. Res. 2018, 53, 1308. [Google Scholar] [CrossRef]
- Silver, L.; Johnson, C. Internet Connectivity Seen as Having Positive Impact on Life in Sub-Saharan Africa. 2018. Available online: https://www.pewresearch.org/global/2018/10/09/internet-connectivity-seen-as-having-positive-impact-on-life-in-sub-saharan-africa/ (accessed on 24 February 2022).
- Kato, H.; Billinghurst, M. Marker tracking and HMD calibration for a video-based augmented reality conferencing system. In Proceedings of the 2nd IEEE and ACM International Workshop on Augmented Reality (IWAR’99), San Francisco, CA, USA, 20–21 October 1999; pp. 85–94. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Parsons, M.; Stone-McLean, J.; Rogers, P.; Boyd, S.; Hoover, K.; Meruvia-Pastor, O.; Gong, M.; Smith, A. Augmented reality as a telemedicine platform for remote procedural training. Sensors 2017, 17, 2294. [Google Scholar] [CrossRef] [PubMed]
- Harris, T.E.; Delellis, S.F.; Heneghan, J.S.; Buckman, R.F.; Miller, G.T.; Magee, J.H.; Vasios, W.N.; Nelson, K.J.; Kane, S.F.; Choi, Y.S. Augmented Reality Forward Damage Control Procedures for Nonsurgeons: A Feasibility Demonstration. Mil. Med. 2020, 185, 521–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rojas-Muñoz, E.; Lin, C.; Sanchez-Tamayo, N.; Cabrera, M.E.; Andersen, D.; Popescu, V.; Barragan, J.A.; Zarzaur, B.; Murphy, P.; Anderson, K.; et al. Evaluation of an augmented reality platform for austere surgical telementoring: A randomized controlled crossover study in cricothyroidotomies. npj Digit. Med. 2020, 3, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, A.W.; Tien, H.; Laporta, A.T.; Lavell, K.; Keillor, J.; Wright Beatty, H.E.; McKee, J.L.; Brien, S.; Roberts, D.J.; Wong, J.; et al. The marriage of surgical simulation and telementoring for damage-control surgical training of operational first responders: A pilot study. J. Trauma Acute Care Surg. 2015, 79, 741–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkpatrick, A.W.; LaPorta, A.; Brien, S.; Leslie, T.; Glassberg, E.; McKee, J.; Ball, C.G.; Wright Beatty, H.E.; Keillor, J.; Roberts, D.J.; et al. Technical innovations that may facilitate real-time telementoring of damage control surgery in austere environments: A proof of concept comparative evaluation of the importance of surgical experience, telepresence, gravity and mentoring in the conduct of damage control laparotomies. Can. J. Surg. 2015, 58, S88–S90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.; Andersen, D.; Popescu, V.; Rojas-Munoz, E.; Cabrera, M.E.; Mullis, B.; Zarzaur, B.; Anderson, K.; Marley, S.; Wachs, J. A first-person mentee second-person mentor AR interface for surgical telementoring. In Proceedings of the 2018 IEEE International Symposium on Mixed and Augmented Reality Adjunct (ISMAR-Adjunct), Munich, Germany, 16–20 October 2018; pp. 3–8. [Google Scholar]
- Gasques, D.; Johnson, J.G.; Sharkey, T.; Feng, Y.; Wang, R.; Xu, Z.R.; Zavala, E.; Zhang, Y.; Xie, W.; Zhang, X.; et al. ARTEMIS: A collaborative mixed-reality system for immersive surgical telementoring. In Proceedings of the 2021 CHI Conference on Human Factors in Computing Systems, Yokohama, Japan, 8–13 May 2021; pp. 1–14. [Google Scholar]
- Roth, D.; Yu, K.; Pankratz, F.; Gorbachev, G.; Keller, A.; Lazarovici, M.; Wilhelm, D.; Weidert, S.; Navab, N.; Eck, U. Real-time mixed reality teleconsultation for intensive care units in pandemic situations. In Proceedings of the 2021 IEEE Conference on Virtual Reality and 3D User Interfaces Abstracts and Workshops (VRW), Lisbon, Portugal, 27 March–1 April 2021; pp. 693–694. [Google Scholar]
- Yu, K.; Gorbachev, G.; Eck, U.; Pankratz, F.; Navab, N.; Roth, D. Avatars for teleconsultation: Effects of avatar embodiment techniques on user perception in 3D asymmetric telepresence. IEEE Trans. Vis. Comput. Graph. 2021, 27, 4129–4139. [Google Scholar] [CrossRef] [PubMed]
- Strak, R.; Yu, K.; Pankratz, F.; Lazarovici, M.; Sandmeyer, B.; Reichling, J.; Weidert, S.; Kraetsch, C.; Roegele, B.; Navab, N.; et al. Comparison Between Video-Mediated and Asymmetric 3D Teleconsultation During a Preclinical Scenario. In Proceedings of the Mensch Und Computer 2021, Ingolstadt, Germany, 4–7 September 2021; Association for Computing Machinery: New York, NY, USA, 2021; pp. 227–235. [Google Scholar]
- Ungureanu, D.; Bogo, F.; Galliani, S.; Sama, P.; Duan, X.; Meekhof, C.; Stühmer, J.; Cashman, T.J.; Tekin, B.; Schönberger, J.L.; et al. Hololens 2 research mode as a tool for computer vision research. arXiv 2020, arXiv:2008.11239. [Google Scholar]
- Microsoft Hololens 2 Research Mode for Unreal Engine. Available online: https://github.com/microsoft/HoloLens-ResearchMode-Unreal (accessed on 24 February 2022).
- Wilson, A. Fast Lossless Depth Image Compression. In Proceedings of the 2017 ACM International Conference on Interactive Surfaces and Spaces (ISS ’17), Brighton, UK, 17–20 October 2017. [Google Scholar]
- 3D Skeletal Tracking on Azure Kinect. Available online: https://www.microsoft.com/en-us/research/uploads/prod/2020/01/AKBTSDK.pdf (accessed on 24 February 2022).



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hale, A.; Fischer, M.; Schütz, L.; Fuchs, H.; Leuze, C. Remote Training for Medical Staff in Low-Resource Environments Using Augmented Reality. J. Imaging 2022, 8, 319. https://doi.org/10.3390/jimaging8120319
Hale A, Fischer M, Schütz L, Fuchs H, Leuze C. Remote Training for Medical Staff in Low-Resource Environments Using Augmented Reality. Journal of Imaging. 2022; 8(12):319. https://doi.org/10.3390/jimaging8120319
Chicago/Turabian StyleHale, Austin, Marc Fischer, Laura Schütz, Henry Fuchs, and Christoph Leuze. 2022. "Remote Training for Medical Staff in Low-Resource Environments Using Augmented Reality" Journal of Imaging 8, no. 12: 319. https://doi.org/10.3390/jimaging8120319