
Prognostic Value of Bone Marrow Uptake Using 18F-FDG PET/CT Scans in Solid Neoplasms
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cohort Analysis
2.1.1. Study Design
2.1.2. Eligibility Criteria
2.1.3. Preoperative Workup
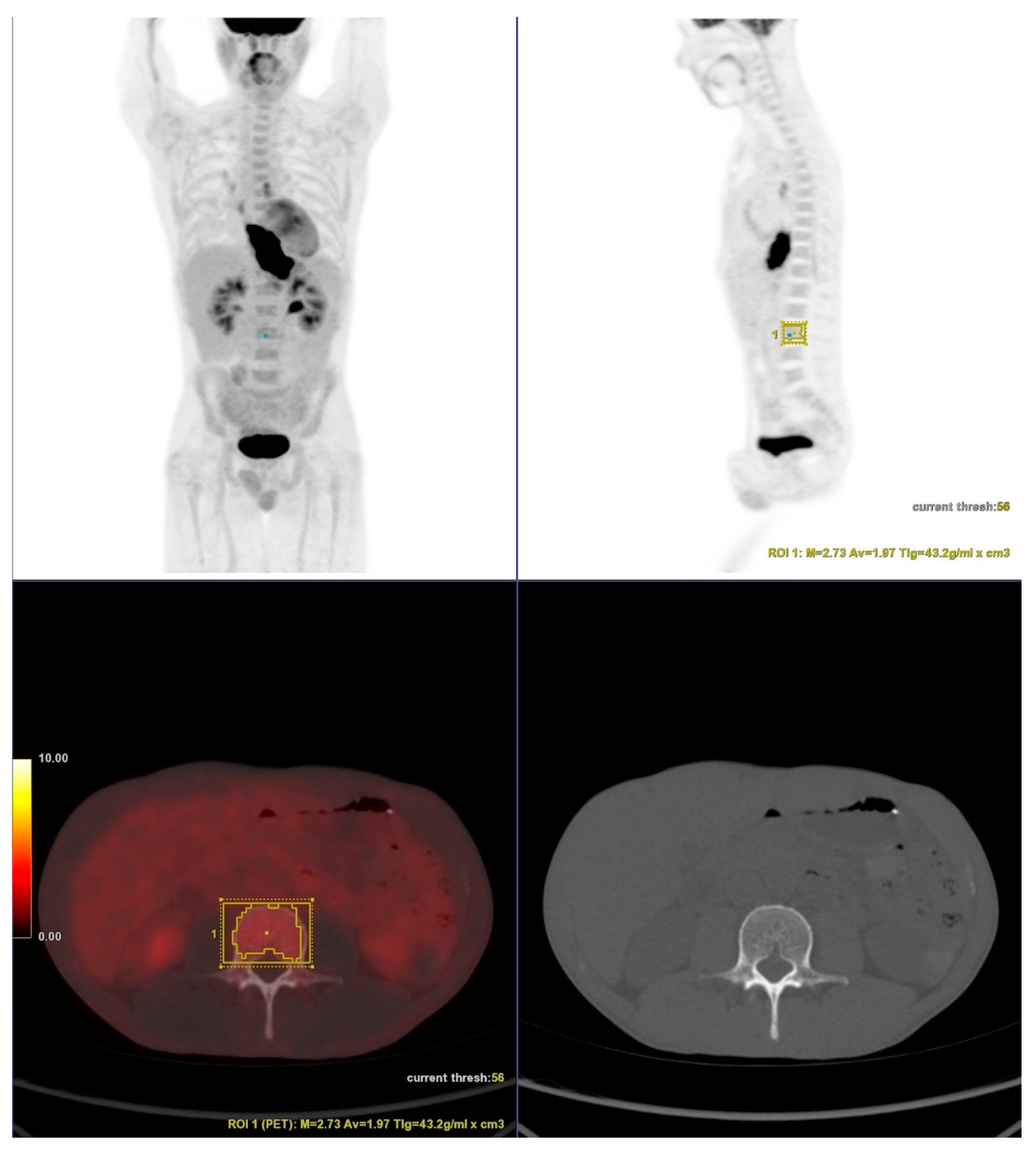
2.1.4. PET/CT
2.1.5. Outcomes
2.1.6. Statistical Analyses
2.2. Systematic Review Analysis
2.2.1. Protocol Register
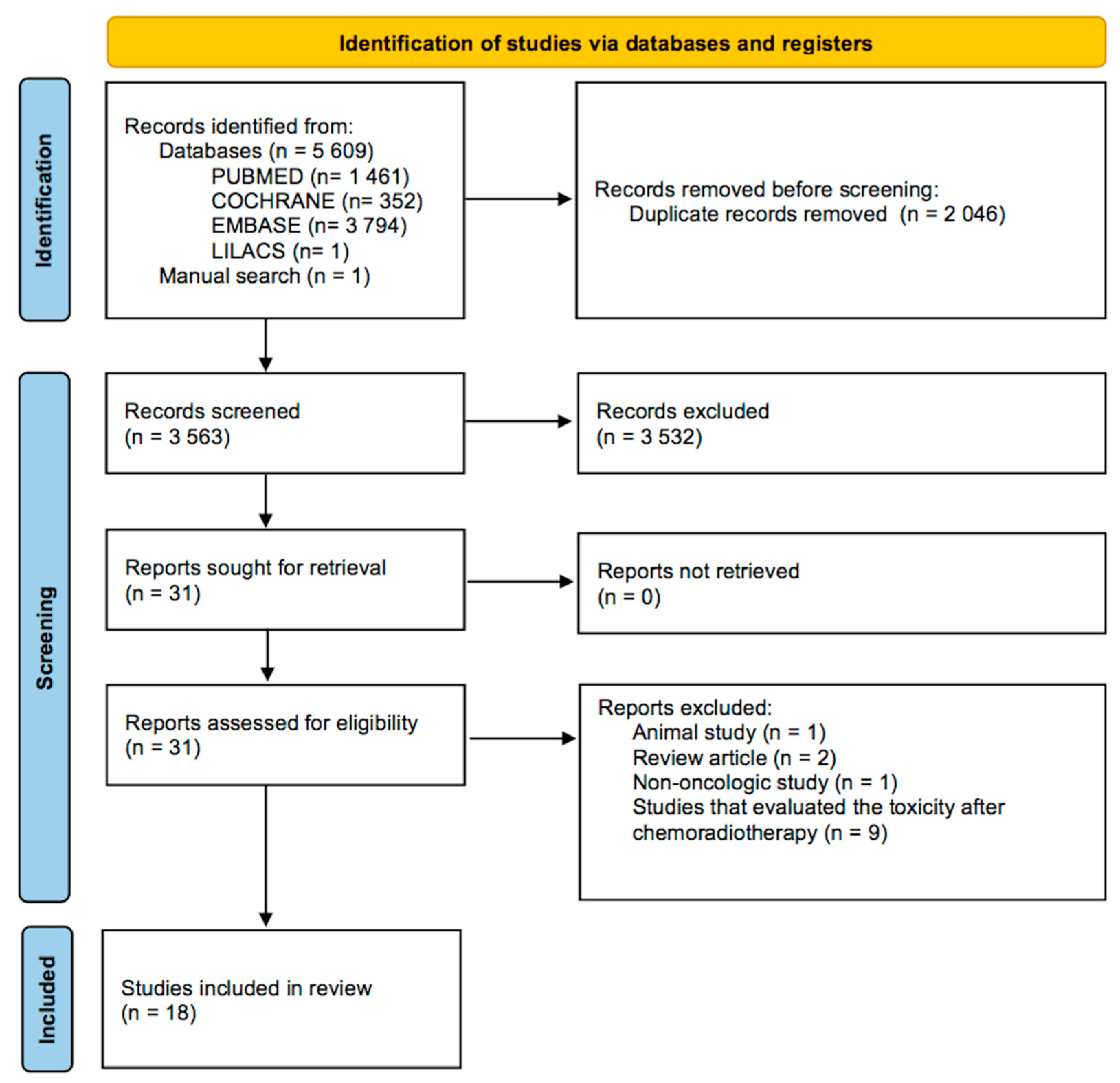
2.2.2. Search and Selection
2.2.3. Eligibility
2.2.4. Data Extraction
2.2.5. Risk of Bias and Certainty Assessment
2.2.6. Synthesis
3. Results
3.1. Cohort
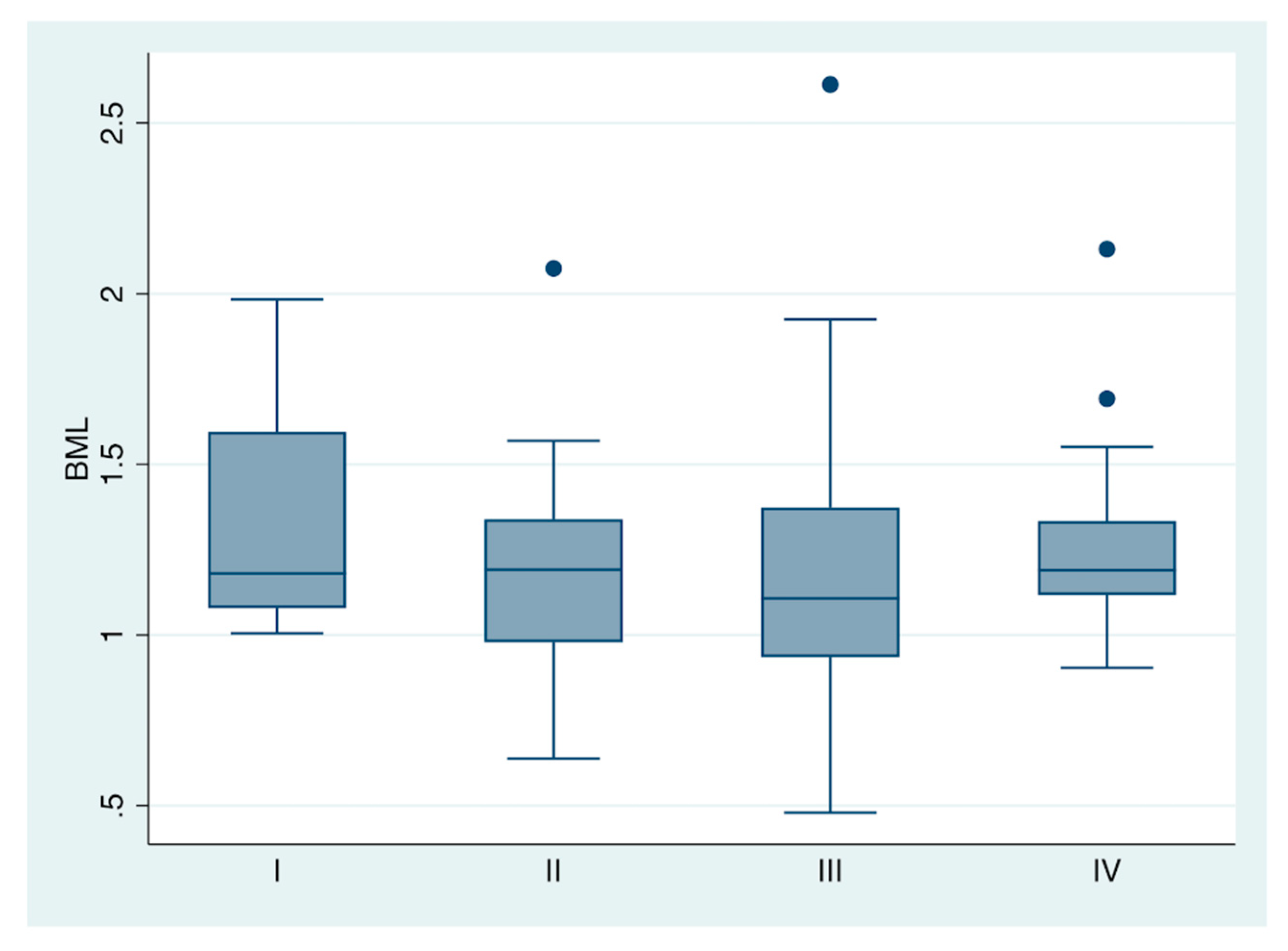
3.1.1. Bone Marrow 18-F-FDG Uptake and Pretreatment Clinical Stage
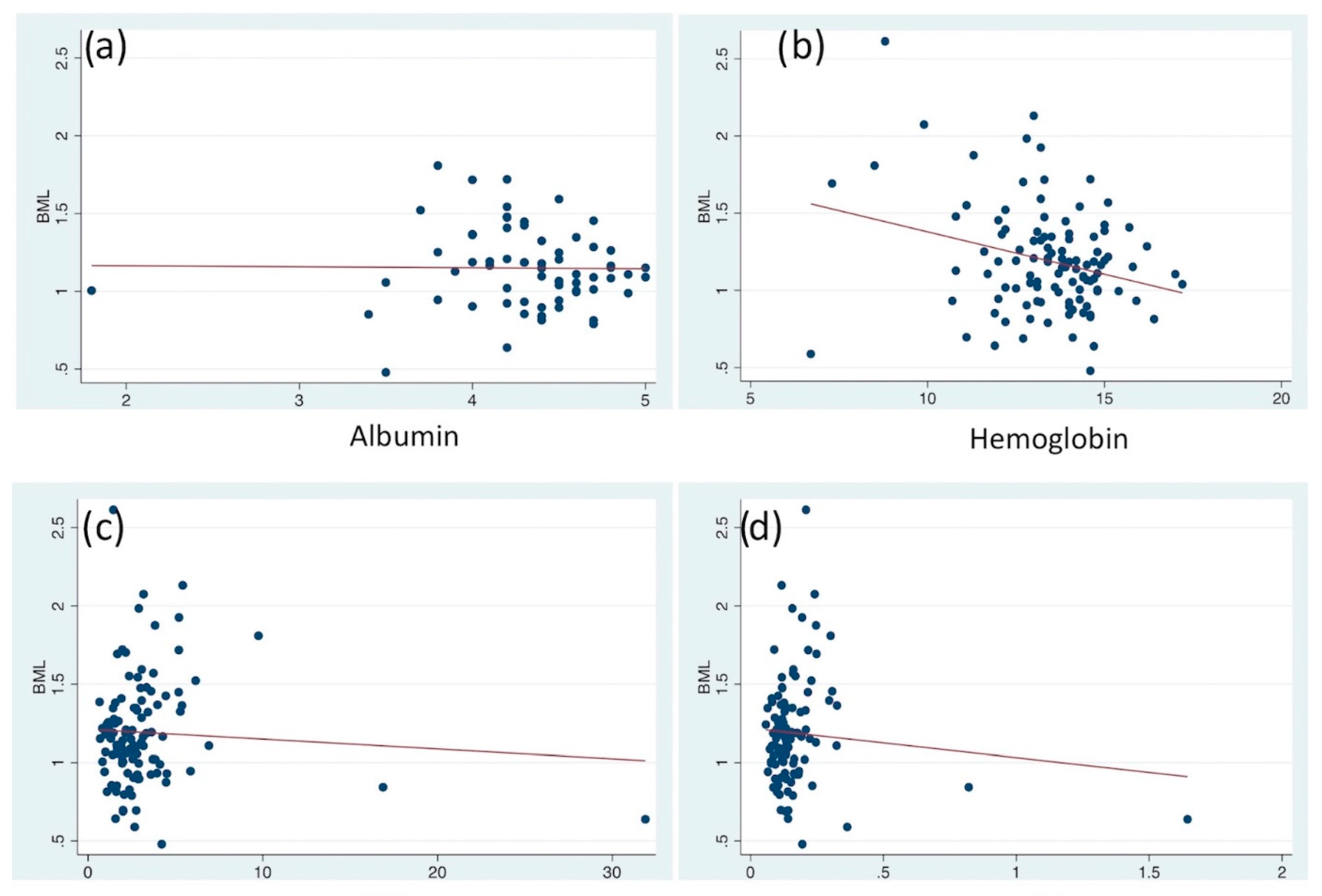
3.1.2. Serum Laboratory Parameters
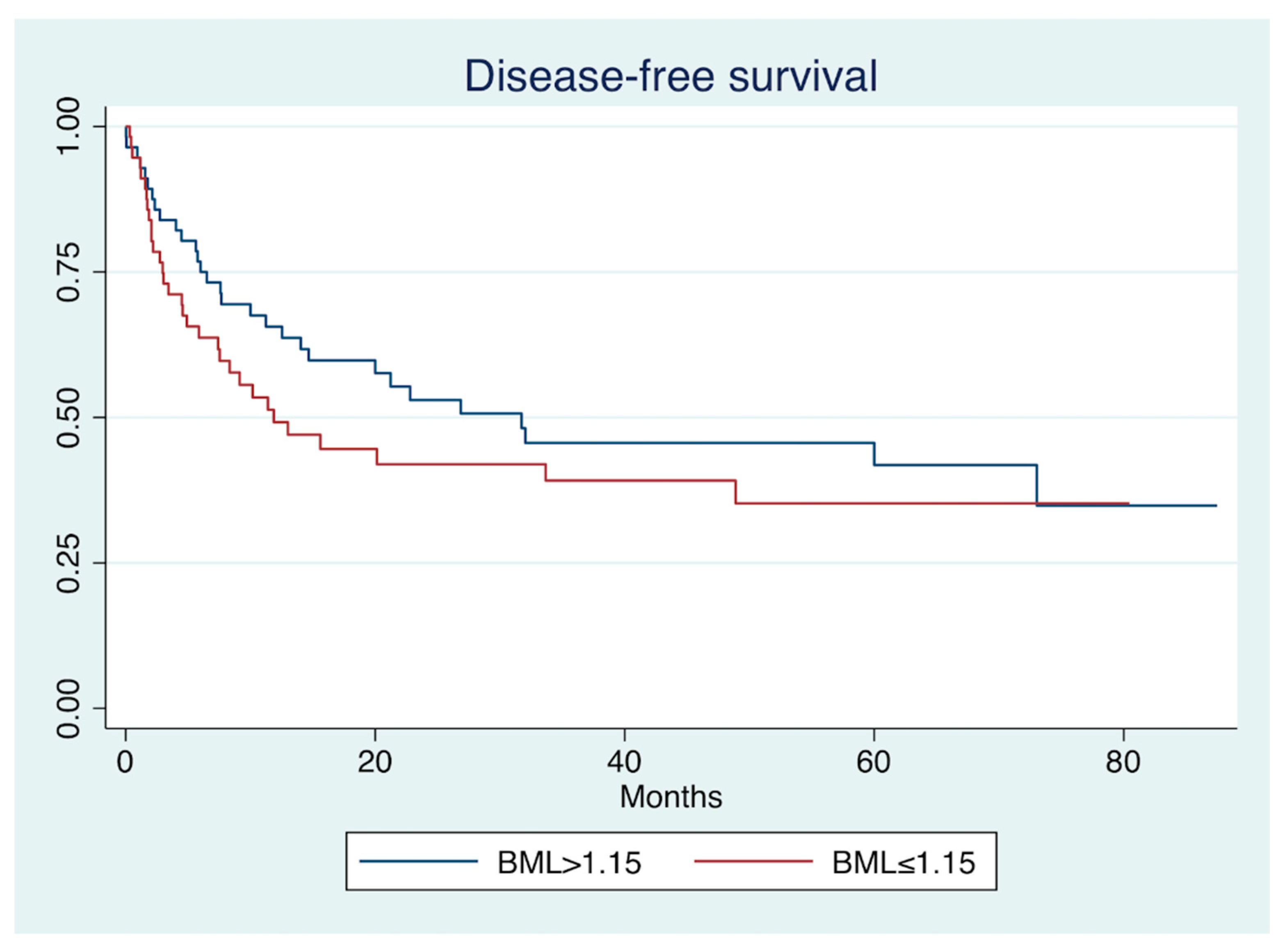
3.1.3. Disease-Free Survival
3.1.4. Pathological Response to Therapy
3.2. Systematic Review
3.2.1. Bone Marrow 18-F-FDG Uptake and Pretreatment Clinical Stage
3.2.2. Serum Laboratory Parameters
3.2.3. Survival Analysis
3.2.4. Other Outcomes
3.3. Risk of Bias and Certainty Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Griffeth, L.K. Use of PET/CT scanning in cancer patients: Technical and practical considerations. Proc. Bayl. Univ. Med. Cent. 2005, 18, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef] [PubMed]
- Valls, L.; Badve, C.; Avril, S.; Herrmann, K.; Faulhaber, P.; O’Donnell, J.; Avril, N. FDG-PET imaging in hematological malignancies. Blood Rev. 2016, 30, 317–331. [Google Scholar] [CrossRef] [Green Version]
- Kung, B.T.; Seraj, S.M.; Zadeh, M.Z.; Rojulpote, C.; Kothekar, E.; Ayubcha, C.; Ng, K.S.; Ng, K.K.; Au-Yong, T.K.; Werner, T.J.; et al. An update on the role of 18F-FDG-PET/CT in major infectious and inflammatory diseases. Am. J. Nucl. Med. Mol. Imaging 2019, 9, 255. [Google Scholar] [PubMed]
- Jamar, F.; Buscombe, J.; Chiti, A.; Christian, P.E.; Delbeke, D.; Donohoe, K.J.; Israel, O.; Martin-Comin, J.; Signore, A. EANM/SNMMI guideline for 18F-FDG use in inflammation and infection. J. Nucl. Med. 2013, 54, 647–658. [Google Scholar] [CrossRef] [Green Version]
- Pijl, J.P.; Kwee, T.C.; Slart, R.H.; Yakar, D.; Wouthuyzen-Bakker, M.; Glaudemans, A.W. Clinical implications of increased uptake in bone marrow and spleen on FDG-PET in patients with bacteremia. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1467–1477. [Google Scholar] [CrossRef] [PubMed]
- Smyth, M.J.; Dunn, G.P.; Schreiber, R.D. Cancer immunosurveillance and immunoediting: The roles of immunity in suppressing tumor development and shaping tumor immunogenicity. Adv. Immunol. 2006, 90, 1–50. [Google Scholar] [PubMed]
- Hu, L.; Li, M.; Ding, Y. Prognostic value of RDW in cancers: A systematic review and meta-analysis. Oncotarget 2017, 8, 16027–16035. [Google Scholar] [CrossRef] [Green Version]
- Kwon, H.C.; Kim, S.H.; Oh, S.Y. Clinical significance of preoperative neutrophil-lymphocyte versus platelet-lymphocyte ratio in patients with operable colorectal cancer. Biomarkers 2012, 17, 216–222. [Google Scholar] [CrossRef]
- Rassouli, A.; Saliba, J.; Castano, R.; Hier, M.; Zeitouni, A.G. Systemic inflammatory markers as independent prognosticators of head and neck squamous cell carcinoma. Head Neck 2015, 37, 103–110. [Google Scholar] [CrossRef]
- Smith, R.A.; Bosonnet, L.; Raraty, M. Preoperative platelet-lymphocyte ratio is an independent significant prognostic marker in resected pancreatic ductal adenocarcinoma. Am. J. Surg. 2009, 197, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.Y.; Hsieh, M.J.; Chiu, Y.C.; Li, S.H.; Huang, H.W.; Fang, F.M.; Huang, Y.J. Higher serum C-reactive protein concentration and hypoalbuminemia are poor prognostic indicators in patients with esophageal cancer undergoing radiotherapy. Radiother. Oncol. 2009, 92, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Szor, D.J.; Dias, A.R.; Pereira, M.A.; Ramos, M.F.K.P.; Zilberstein, B.; Cecconello, I.; Ribeiro-Júnior, U. Prognostic role of neutrophil/ lymphocyte ratio in resected gastric cancer: A systematic review and meta-analysis. Clinics 2018, 73, e360. [Google Scholar] [CrossRef] [PubMed]
- Tustumi, F.; Takeda, F.R.; Viyuela, M.S.; da Cruz Junior, J.B.; Brandão, A.A.; Sallum, R.A.; Ribeiro Junior, U.; Cecconello, I. The value of cellular components of blood in the setting of trimodal therapy for esophageal cancer. J. Surg. Oncol. 2020, 121, 784–794. [Google Scholar] [CrossRef]
- Tustumi, F.; Takeda, F.R.; Brandão, A.A.; Sallum, R.A.; Ribeiro, U.; Cecconello, I. Lymphocyte count and platelet volume predicts postoperative complications in esophagectomy for cancer: A cohort study. Arq. De Gastroenterol. 2019, 56, 377–385. [Google Scholar] [CrossRef]
- Ning, K.; Liu, S.; Yang, B.; Wang, R.; Man, G.; Wang, D.E.; Xu, H. Update on the effects of energy metabolism in bone marrow mesenchymal stem cells differentiation. Mol. Metab. 2022, 58, 101450. [Google Scholar] [CrossRef]
- Devesa, A.; Lobo-González, M.; Martínez-Milla, J.; Oliva, B.; García-Lunar, I.; Mastrangelo, A.; España, S.; Sanz, J.; Mendiguren, J.M.; Bueno, H.; et al. Bone marrow activation in response to metabolic syndrome and early atherosclerosis. Eur. Heart J. 2022, 43, 1809–1828. [Google Scholar] [CrossRef]
- Patel, N.H.; Osborne, M.T.; Teague, H.; Parel, P.; Svirydava, M.; Sorokin, A.V.; Teklu, M.; Manyak, G.; Zhou, W.; Pantoja, C.; et al. Heightened splenic and bone marrow uptake of 18F-FDG PET/CT is associated with systemic inflammation and subclinical atherosclerosis by CCTA in psoriasis: An observational study. Atherosclerosis 2021, 339, 20–26. [Google Scholar] [CrossRef]
- Zhang, L.; Jiang, G.; Zhao, X.; Gong, Y. Dimethyloxalylglycine promotes bone marrow mesenchymal stem cell osteogenesis via Rho/ROCK signaling. Cell. Physiol. Biochem. 2016, 39, 1391–1403. [Google Scholar] [CrossRef]
- Rice, T.W.; Patil, D.T.; Blackstone, E.H. 8th edition AJCC/UICC staging of cancers of the esophagus and esophagogastric junction: Application to clinical practice. Ann. Cardiothorac. Surg. 2017, 6, 119–130. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schünemann, H.; Brożek, J.; Guyatt, G.; Oxman, A. GRADE Handbook for Grading Quality of Evidence and Strength of Recommendations; Updated October 2013. The GRADE Working Group, 2013. Available from Guideline Development. Org/Handbook; Cochrane: London, UK, 2013. [Google Scholar]
- Inoue, K.; Goto, R.; Okada, K.; Kinomura, S.; Fukuda, H. A bone marrow F-18 FDG uptake exceeding the liver uptake may indicate bone marrow hyperactivity. Ann. Nucl. Med. 2009, 23, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Na, J.O.; Kang, D.Y.; Lee, S.Y.; Lee, S.M. Prognostic Significance of FDG Uptake of Bone Marrow on PET/CT in Patients With Non–Small-Cell Lung Cancer After Curative Surgical Resection. Clin. Lung Cancer 2017, 18, 198–206. [Google Scholar] [CrossRef]
- Lee, J.W.; Lee, M.S.; Chung, I.K.; Son, M.W.; Cho, Y.S.; Lee, S.M. Clinical implication of FDG uptake of bone marrow on PET/CT in gastric cancer patients with surgical resection. World J. Gastroenterol. 2017, 23, 2385. [Google Scholar] [CrossRef]
- Lee, J.W.; Jeon, S.; Mun, S.T.; Lee, S.M. Prognostic value of fluorine-18 fluorodeoxyglucose uptake of bone marrow on positron emission tomography/computed tomography for prediction of disease progression in cervical cancer. Int. J. Gynecol. Cancer 2017, 27, 776–783. [Google Scholar] [CrossRef]
- Lee, J.W.; Seo, K.H.; Kim, E.S.; Lee, S.M. The role of 18 F-fluorodeoxyglucose uptake of bone marrow on PET/CT in predicting clinical outcomes in non-small cell lung cancer patients treated with chemoradiotherapy. Eur. Radiol. 2017, 27, 1912–1921. [Google Scholar] [CrossRef]
- Lee, J.W.; Choi, J.S.; Lyu, J.; Lee, S.M. Prognostic significance of 18F-fluorodeoxyglucose uptake of bone marrow measured on positron emission tomography in patients with small cell lung cancer. Lung Cancer 2018, 118, 41–47. [Google Scholar] [CrossRef]
- Lee, J.W.; Baek, M.J.; Ahn, T.S.; Lee, S.M. Fluorine-18-fluorodeoxyglucose uptake of bone marrow on PET/CT can predict prognosis in patients with colorectal cancer after curative surgical resection. Eur. J. Gastroenterol. Hepatol. 2018, 30, 187–194. [Google Scholar] [CrossRef]
- Lee, J.W.; Ban, M.J.; Park, J.H.; Lee, S.M. Effect of F-18 fluorodeoxyglucose uptake by bone marrow on the prognosis of head and neck squamous cell carcinoma. J. Clin. Med. 2019, 8, 1169. [Google Scholar] [CrossRef]
- Lee, J.W.; Kim, S.Y.; Han, S.W.; Lee, J.E.; Lee, H.J.; Heo, N.H.; Lee, S.M. [18 F] FDG uptake of bone marrow on PET/CT for predicting distant recurrence in breast cancer patients after surgical resection. EJNMMI Res. 2020, 10, 72. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Park, S.H.; Ahn, H.; Lee, S.M.; Jang, S.J. Predicting Survival in Patients with Pancreatic Cancer by Integrating Bone Marrow, F.D.G Uptake and Radiomic Features of Primary Tumor in PET/CT. Cancers 2021, 13, 3563. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lee, H.S.; Kim, S.; Park, E.J.; Baik, S.H.; Jeon, T.J.; Lee, K.Y.; Ryu, Y.H.; Kang, J. Prognostic significance of bone marrow and spleen 18F-FDG uptake in patients with colorectal cancer. Sci. Rep. 2021, 11, 12137. [Google Scholar] [CrossRef]
- Li, C.; Zhang, J.; Chen, S.; Huang, S.; Wu, S.; Zhang, L.; Zhang, F.; Wang, H. Prognostic value of metabolic indices and bone marrow uptake pattern on preoperative 18F–FDG PET/CT in pediatric patients with neuroblastoma. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Li, T.C.; Wang, L.L.; Liu, B.L.; Hong, J.J.; Xu, N.N.; Tang, K.; Zheng, X.W. Association between bone marrow fluorodeoxyglucose uptake and recurrence after curative surgical resection in patients with T1–2N0M0 lung adenocarcinoma: A retrospective cohort study. Quant. Imaging Med. Surg. 2020, 10, 2285. [Google Scholar] [CrossRef] [PubMed]
- Mattonen, S.A.; Davidzon, G.A.; Benson, J.; Leung, A.N.; Vasanawala, M.; Horng, G.; Shrager, J.B.; Napel, S.; Nair, V.S. Bone Marrow and Tumor Radiomics at 18F-FDG PET/CT: Impact on Outcome Prediction in Non–Small Cell Lung Cancer. Radiology 2019, 293, 451–459. [Google Scholar] [CrossRef]
- Ozmen, O.; Koyuncu, A.; Koksal, D.; Tatci, E.; Alagoz, E.; Demirag, F.; Gokcek, A.; Arslan, N. The potential value of volume-based quantitative PET parameters and increased bone marrow uptake for the prediction of survival in patients with malignant pleural mesothelioma. Nucl. Med. Commun. 2016, 37, 43–49. [Google Scholar] [CrossRef]
- Prévost, S.; Boucher, L.; Larivée, P.; Boileau, R.; Bénard, F. Bone marrow hypermetabolism on 18F-FDG PET as a survival prognostic factor in non–small cell lung cancer. J. Nucl. Med. 2006, 47, 559–565. [Google Scholar]
- Seban, R.D.; Robert, C.; Dercle, L.; Yeh, R.; Dunant, A.; Reuze, S.; Schernberg, A.; Sun, R.; Mignot, F.; Terroir, M.; et al. Increased bone marrow SUVmax on 18F-FDG PET is associated with higher pelvic treatment failure in patients with cervical cancer treated by chemoradiotherapy and brachytherapy. Oncoimmunology 2019, 8, e1574197. [Google Scholar] [CrossRef] [Green Version]
- Shimura, K.; Mabuchi, S.; Komura, N.; Yokoi, E.; Kozasa, K.; Sasano, T.; Kawano, M.; Matsumoto, Y.; Watabe, T.; Kodama, M.; et al. Prognostic significance of bone marrow FDG uptake in patients with gynecological cancer. Sci. Rep. 2021, 11, 2257. [Google Scholar] [CrossRef]
- Yanagawa, M.; Tatsumi, M.; Miyata, H.; Morii, E.; Tomiyama, N.; Watabe, T.; Isohashi, K.; Kato, H.; Shimosegawa, E.; Yamasaki, M.; et al. Evaluation of response to neoadjuvant chemotherapy for esophageal cancer: PET response criteria in solid tumors versus response evaluation criteria in solid tumors. J. Nucl. Med. 2012, 53, 872–880. [Google Scholar] [CrossRef] [PubMed]
- Tustumi, F.; Duarte, P.S.; Albenda, D.G.; Takeda, F.R.; Sallum, R.A.; Junior, U.R.; Buchpiguel, C.A.; Cecconello, I. Prognostic value of 18F-fluorodeoxyglucose PET/computed tomography metabolic parameters measured in the primary tumor and suspicious lymph nodes before neoadjuvant therapy in patients with esophageal carcinoma. Nucl. Med. Commun. 2021, 42, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Tustumi, F.; Albenda, D.G.; Sallum, R.A.A.; Nahas, S.C.; Ribeiro Junior, U.; Buchpiguel, C.A.; Cecconello, I.; Duarte, P.S. 18F-FDG-PET/CT-measured parameters as potential predictors of residual disease after neoadjuvant chemoradiotherapy in patients with esophageal carcinoma. Radiol. Bras. 2022, 55, 286–292. [Google Scholar] [CrossRef]
- Takeda, F.R.; Tustumi, F.; de Almeida Obregon, C.; Yogolare, G.G.; Navarro, Y.P.; Segatelli, V.; Sallum, R.A.; Junior, U.R.; Cecconello, I. Prognostic value of tumor regression grade based on Ryan score in squamous cell carcinoma and adenocarcinoma of esophagus. Ann. Surg. Oncol. 2020, 27, 1241–1247. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Count | % | ||
|---|---|---|---|
| Sex | Male | 83 | 73 |
| Female | 30 | 27 | |
| Age | >65 years old | 45 | 40 |
| ≤65 years old | 68 | 60 | |
| Histology | SCC | 78 | 69 |
| Adenocarcinoma | 35 | 31 | |
| Pretreatment cStage | I/II | 32 | 28 |
| III/IV | 81 | 62 | |
| BML | >1.152 | 56 | 50 |
| ≤1.152 | 57 | 50 |
| Spearman’s Rho | Prob > |t| | |
|---|---|---|
| Albumin | −0.14 | 0.25 |
| Hemoglobin | −0.17 | 0.08 |
| NLR | 0.13 | 0.19 |
| PLR | 0.11 | 0.26 |
| Disease-Free Survival | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR | SE | p > |z| | HR | SE | p > |z| | |
| Sex (Male) | 0.93 | 0.28 | 0.81 | |||
| Age (>65 years old) | 1.99 | 0.51 | <0.01 | 1.82 | 0.47 | 0.02 |
| Histology (SCC) | 0.42 | 0.11 | <0.01 | 0.67 | 0.21 | 0.21 |
| cStage (I/II) | 1.94 | 0.59 | 0.03 | 1.36 | 0.47 | 0.37 |
| Pathological complete response | 0.44 | 0.12 | <0.01 | 0.54 | 0.16 | 0.04 |
| BML (>1.15) | 1.34 | 0.34 | 0.26 | |||
| Pathological Complete Response | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| OR | SE | p > |z| | OR | SE | p > |z| | |
| Sex (Male) | 1.34 | 0.6 | 0.44 | |||
| Age (>65 years old) | 0.87 | 0.33 | 0.7 | |||
| Histology (SCC) | 18 | 12 | <0.01 | 18 | 12 | <0.01 |
| cStage (I/II) | 0.55 | 0.23 | 0.16 | |||
| BML (>1.15) | 0.81 | 0.31 | 0.58 | |||
| Author Year | Design | Neoplasm | Site of Uptake Measurement | PET/CT Evaluation | N | Mean Age (Years) | Mean Follow-Up (Months) | Therapy | Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Inoue 2009 | Cohort | Lung, esophageal, head and neck, colon, pancreas | Thoracic (T10-12) and lumbar (L2-4) vertebrae | BML SUV | 32 | 62 | at least 6 | Uninformed | Laboratory parameters, comparison malignant vs. benign |
| Lee 2016 | Cohort | Lung cancer | Thoracic (T11-12) and lumbar (L3-5) vertebrae | BML SUV and BM SUV | 110 | 65 | 22 | Surgical resection | OS, PFS/DFS, laboratory parameters |
| Lee 2017.1 | Cohort | Gastric cancer | Thoracic (T10-12) and lumbar (L3-5) vertebrae | BML SUV and BM SUV | 309 | 60 | 34 | Surgical resection | OS, PFS/DFS |
| Lee 2017.2 | Cohort | Cervical cancer | Thoracic (T11-12) and lumbar (L3-5) vertebrae | BML SUV and BM SUV | 145 | 52 | 26 | Chemoradiotherapy or surgical resection | PFS, DRFS, laboratory parameters |
| Lee 2017.3 | Cohort | Lung cancer | Thoracic (T11-12) and lumbar (L3-5) vertebrae | BML SUV and BM SUV | 106 | 74 | 19 | Chemoradiotherapy | OS, PFS/DFS, laboratory parameters |
| Lee 2018.1 | Cohort | Lung cancer | Thoracic and lumbar vertebrae | BM SUV | 70 | 68 | 11 | Chemotherapy, radiotherapy, or surgical resection | OS, PFS/DFS, laboratory parameters |
| Lee 2018.2 | Cohort | Colorectal cancer | Thoracic (T10-12) and lumbar (L3-5) vertebrae | BM SUV | 226 | 66 | 32 | Surgical resection | PFS/DFS, laboratory parameters, cStage |
| Lee 2019 | Cohort | Head and neck | Thoracic and lumbar vertebrae | BML SUV and BM SUV | 157 | 61 | 26 | Chemotherapy, radiotherapy or surgical resection | PFS/DFS, DRRS, cStage, laboratory parameters |
| Lee 2020 | Cohort | Breast cancer | Thoracic and lumbar vertebrae | BML SUV and BM SUV | 345 | 51 | 49 | Surgical resection (with or without neoadjuvant therapy) | PFS/DFS, DRRS, cStage, laboratory parameters |
| Lee 2021.1 | Cohort | Pancreas cancer | Thoracic and lumbar vertebrae | BML SUV and BM SUV | 65 | 66 | Uninformed | Chemotherapy, radiotherapy, or surgical resection | OS |
| Lee 2021.2 | Cohort | Colorectal cancer | Thoracic and lumbar vertebrae | SLR SUV and BML SUV | 411 | Uninformed | 91 | Surgical resection (with or without chemotherapy) | OS, laboratory parameters |
| Li 2018 | Cohort | Neuroblastoma | Uninformed | BM SUV | 47 | 2 | 24 | Surgical resection (with or without chemotherapy or radiotherapy) | OS, PFS/DFS |
| Li 2020 | Cohort | Lung cancer | Thoracic and lumbar vertebrae | BML SUV and BM SUV | 195 | 63 | 4 to 65 | Surgical resection | PFS/DFS, laboratory parameters, cStage |
| Mattonen 2019 | Cohort | Lung cancer | Lumbar vertebrae (L3-L5) | GLCM | 227 | 70 | 41 | Surgical resection | PFS/DFS |
| Ozmen 2016 | Cohort | Pleural mesothelioma | Lumbar vertebrae (L3-L5) | BML SUV and BM SUV | 51 | 56 | 28 to 56 | Surgical resection, chemotherapy, or palliation therapy | OS, laboratory parameters |
| Prévost 2016 | Cohort | Lung cancer | Lumbar vertebrae (L3-L5) | BML SUV and BM SUV | 120 | 68 | 18 | Chemotherapy, radiotherapy, or surgical resection | OS, laboratory parameters, cStage |
| Seban 2019 | Cohort | Cervical cancer | Thoracic (T12) and lumbar (L3-5) vertebrae | BM SUV | 116 | 47 | 75 | Chemoradiotherapy, brachytherapy | OS, PRFS, EPRFS, laboratory parameters |
| Shimura 2021 | Cohort | Gynecological cancer | Thoracic (T8-12) vertebrae | BMAo and BM SUV | 559 | 56 | 48 | Surgical resection | PFS/DFS |
| Current study 2022 | Cohort | Esophageal cancer | Lumbar vertebrae (L3-L5) | BML SUV and BM SUV | 113 | 61 | 25 | Trimodal | PFR/DFS, pCR, cStage, laboratory parameters |
| Author Year | Neoplasm | Survival Analysis * |
|---|---|---|
| Lee 2016 | Lung cancer | DFS: 2.41 |
| OS: 2.15 (n.s.) | ||
| Lee 2017.1 | Gastric cancer | DFS: 8.25 |
| OS: 20.69 | ||
| Lee 2017.2 | Cervical cancer | PFS: 2.32 |
| Lee 2017.3 | Lung cancer | PFS: 14.44 |
| OS: 1.24 (n.s.) | ||
| Lee 2018.1 | Lung cancer | PFS: 2.28 |
| OS: 1.47 (n.s.) | ||
| Lee 2018.2 | Colorectal cancer | DFS: 2.94 |
| Lee 2019 | Head and neck | PFS: 1.96 |
| Lee 2020 | Breast cancer | DFS: 16.38 |
| Lee 2021.1 | Pancreas cancer | OS: 4.3 |
| Lee 2021.2 | Colorectal cancer | OS: 5.28 |
| Li 2018 | Neuroblastoma | RFS: 0.085 (n.s.) |
| OS: 0.032 | ||
| Li 2020 | Lung cancer | RFS: 5.09 (n.s.) |
| Mattonen 2019 | Lung cancer | RFS: 1.62 |
| Ozmen 2016 | Pleural mesothelioma | OS: 3.82 |
| Prévost 2016 | Lung cancer | OS: 1.6 |
| Seban 2019 | Cervical cancer | OS: 2.7 |
| Shimura 2021 | Gynecological cancer | PFS: 3.07 |
| Current study 2022 | Esophageal cancer | DFS: 1.34 (n.s.) |
| Author | 1. Bias due to Confounding | 2. Bias in Selection of Participants into the Study | 3. Bias in Classification of Interventions | 4. Bias due to Deviations from Intended Interventions | 5. Bias due to Missing Data | 6. Bias in Measurement of Outcomes | 7. Bias in Selection of the Reported Results | 8. Overall Bias |
|---|---|---|---|---|---|---|---|---|
| Inoue 2009 | Low | Low | Low | Low | Serious | Low | Moderate | Low |
| Lee 2016 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Lee 2017.1 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Lee 2017.2 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Lee 2017.3 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Lee 2018.1 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Lee 2018.2 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Lee 2019 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Lee 2020 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Lee 2021.1 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Lee 2021.2 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Li 2018 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Li 2020 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Mattonen 2019 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Ozmen 2016 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Prévost 2016 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Seban 2019 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Shimura 2021 | Low | Low | Low | Low | Moderate | Low | Moderate | Low |
| Current study 2022 | Low | Low | Low | Low | Low | Low | Low | Low |
| Certainty Assessment | ||||||
|---|---|---|---|---|---|---|
| Studies | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Overall Certainty of Evidence |
| Clinical stage | ||||||
| 6 observational studies | not serious | very serious a | not serious | not serious | publication bias strongly suspected b | ⨁◯◯◯ Very low |
| Serum laboratory parameters | ||||||
| 16 observational studies | not serious | very serious a | not serious | not serious | publication bias strongly suspected b | ⨁◯◯◯ Very low |
| Survival | ||||||
| 18 observational studies | not serious | very serious a | not serious | not serious | publication bias strongly suspected b | ⨁◯◯◯ Very low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tustumi, F.; Albenda, D.G.; Perrotta, F.S.; Sallum, R.A.A.; Ribeiro Junior, U.; Buchpiguel, C.A.; Duarte, P.S. Prognostic Value of Bone Marrow Uptake Using 18F-FDG PET/CT Scans in Solid Neoplasms. J. Imaging 2022, 8, 297. https://doi.org/10.3390/jimaging8110297
Tustumi F, Albenda DG, Perrotta FS, Sallum RAA, Ribeiro Junior U, Buchpiguel CA, Duarte PS. Prognostic Value of Bone Marrow Uptake Using 18F-FDG PET/CT Scans in Solid Neoplasms. Journal of Imaging. 2022; 8(11):297. https://doi.org/10.3390/jimaging8110297
Chicago/Turabian StyleTustumi, Francisco, David Gutiérrez Albenda, Fernando Simionato Perrotta, Rubens Antonio Aissar Sallum, Ulysses Ribeiro Junior, Carlos Alberto Buchpiguel, and Paulo Schiavom Duarte. 2022. "Prognostic Value of Bone Marrow Uptake Using 18F-FDG PET/CT Scans in Solid Neoplasms" Journal of Imaging 8, no. 11: 297. https://doi.org/10.3390/jimaging8110297