

A Randomized, Double-Blind, Placebo-Controlled Trial to Evaluate the Cholesterol-Lowering Effect of BBR 4401 in Adults with Moderate Hypercholesterolemia
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
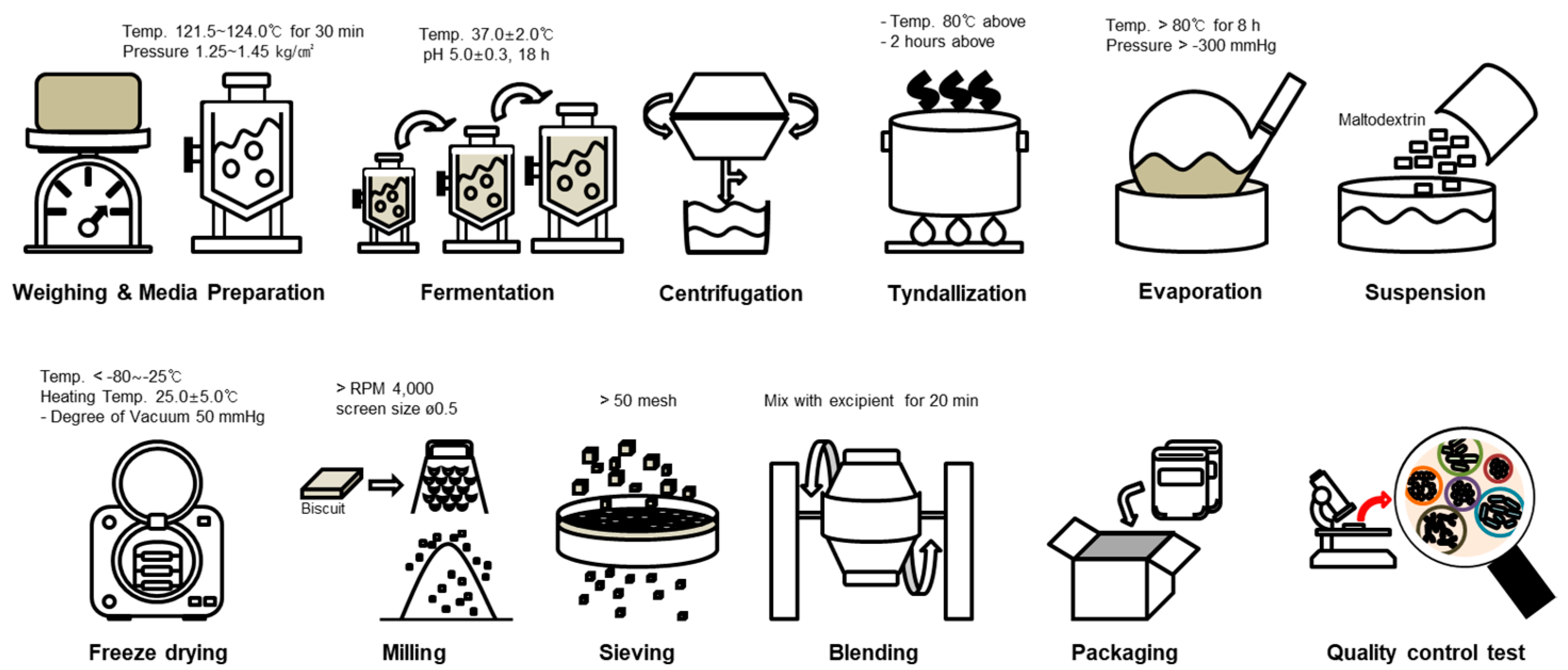
2.1. Process of Manufacturing for Investigation Product
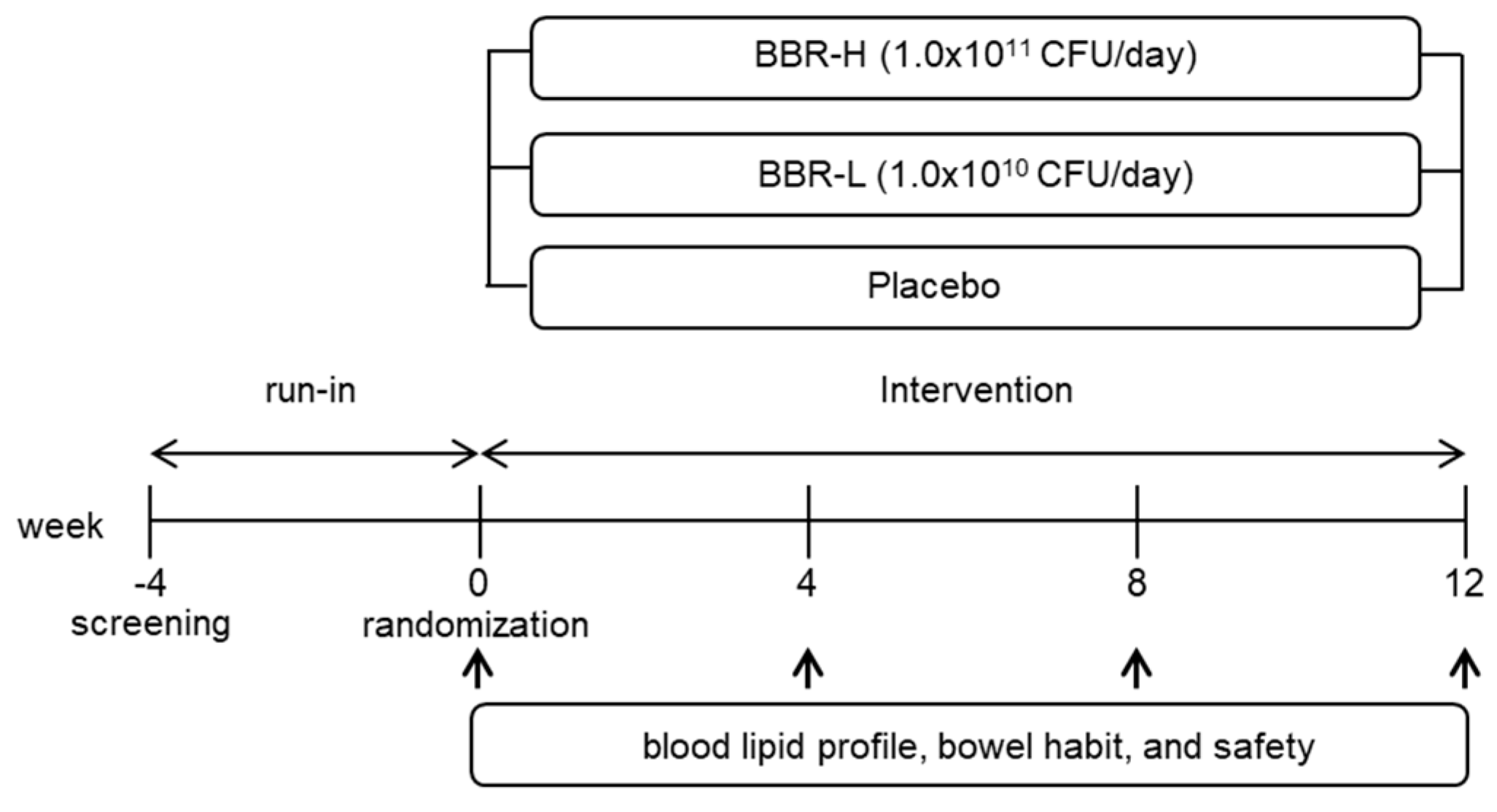
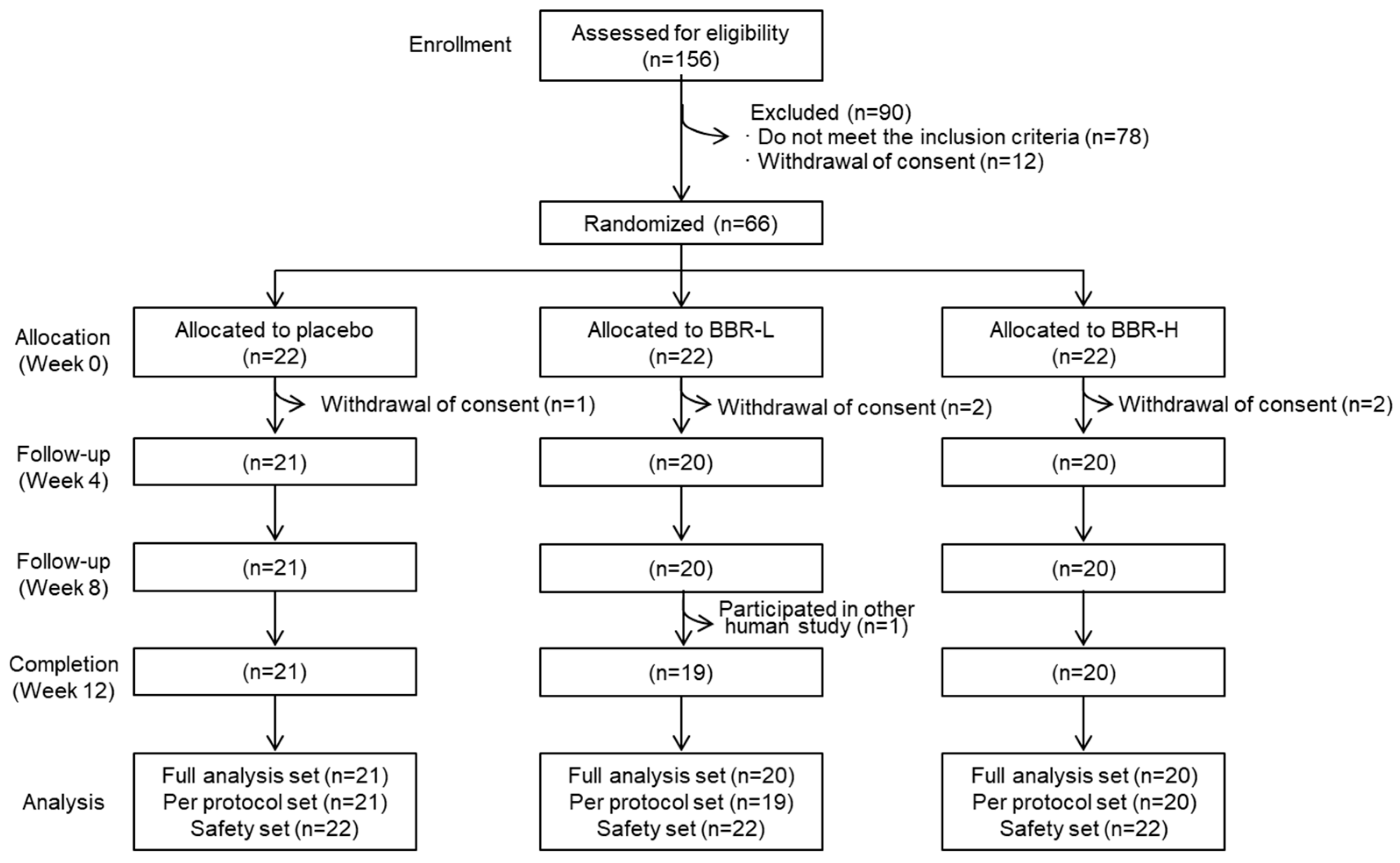
2.2. Subjects and Study Design
2.3. Statistical Analysis
2.4. Metabolites Analysis
3. Results and Discussion
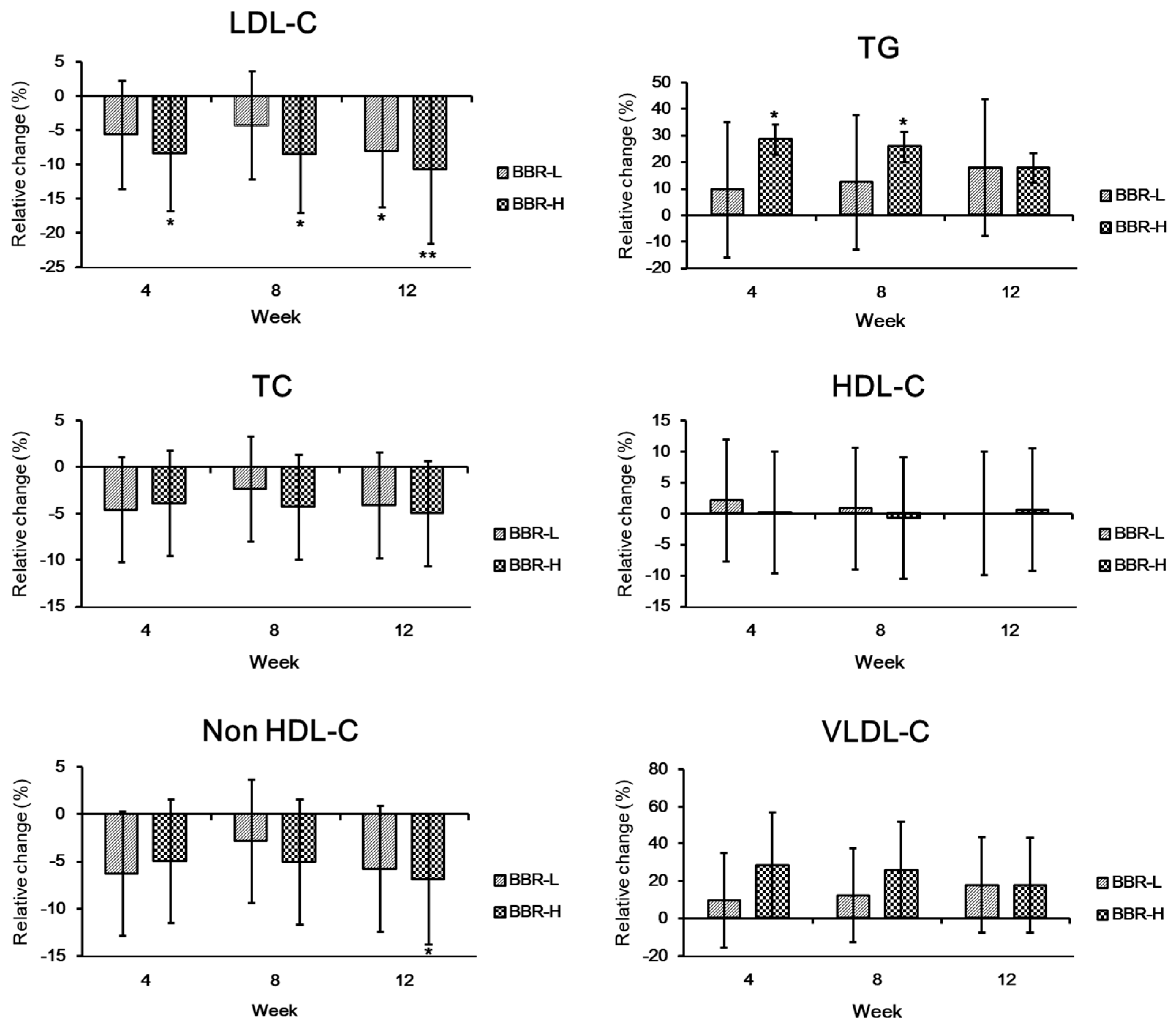
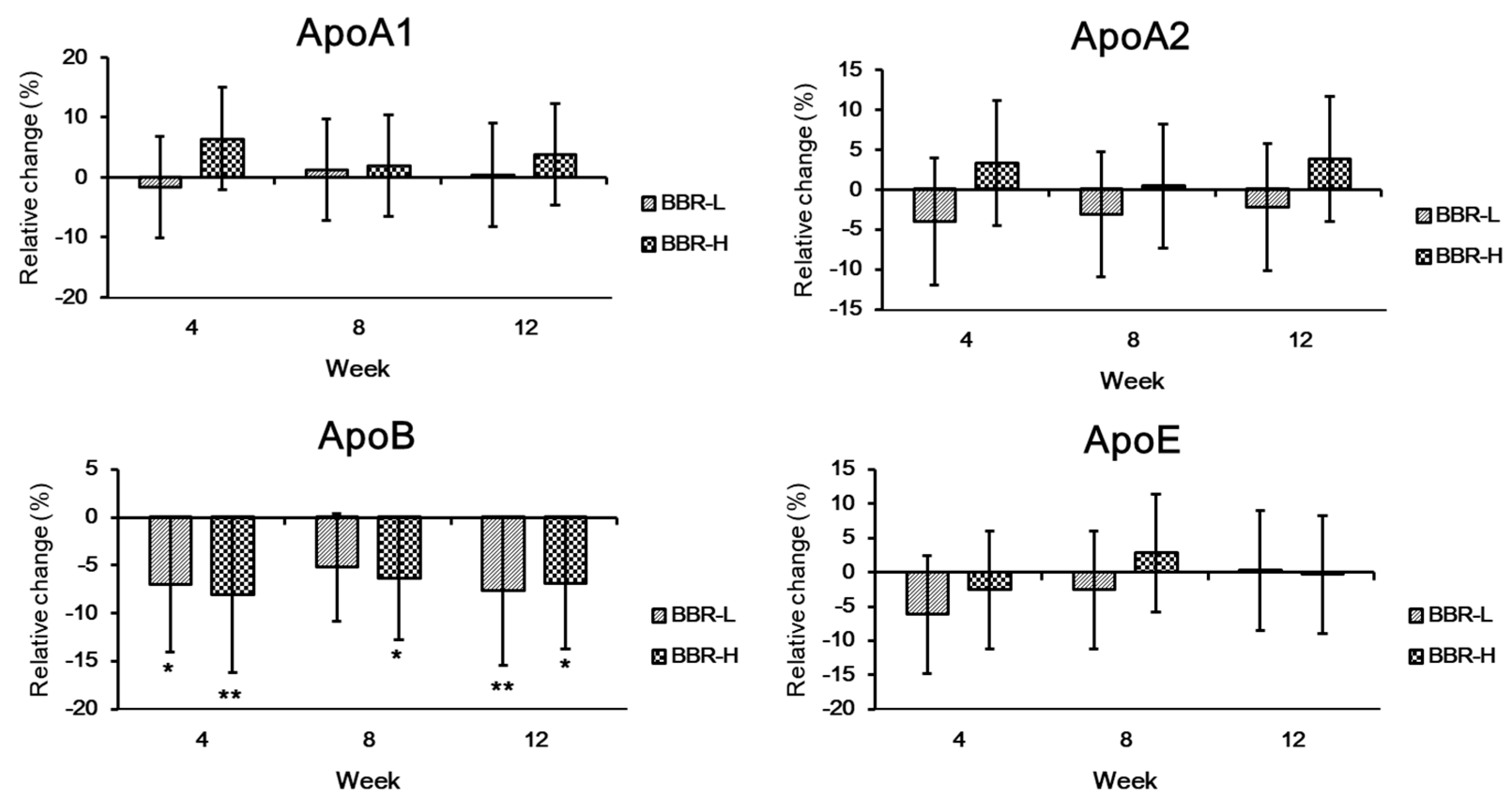
3.1. Lipids and Apolipoprotein Profiles
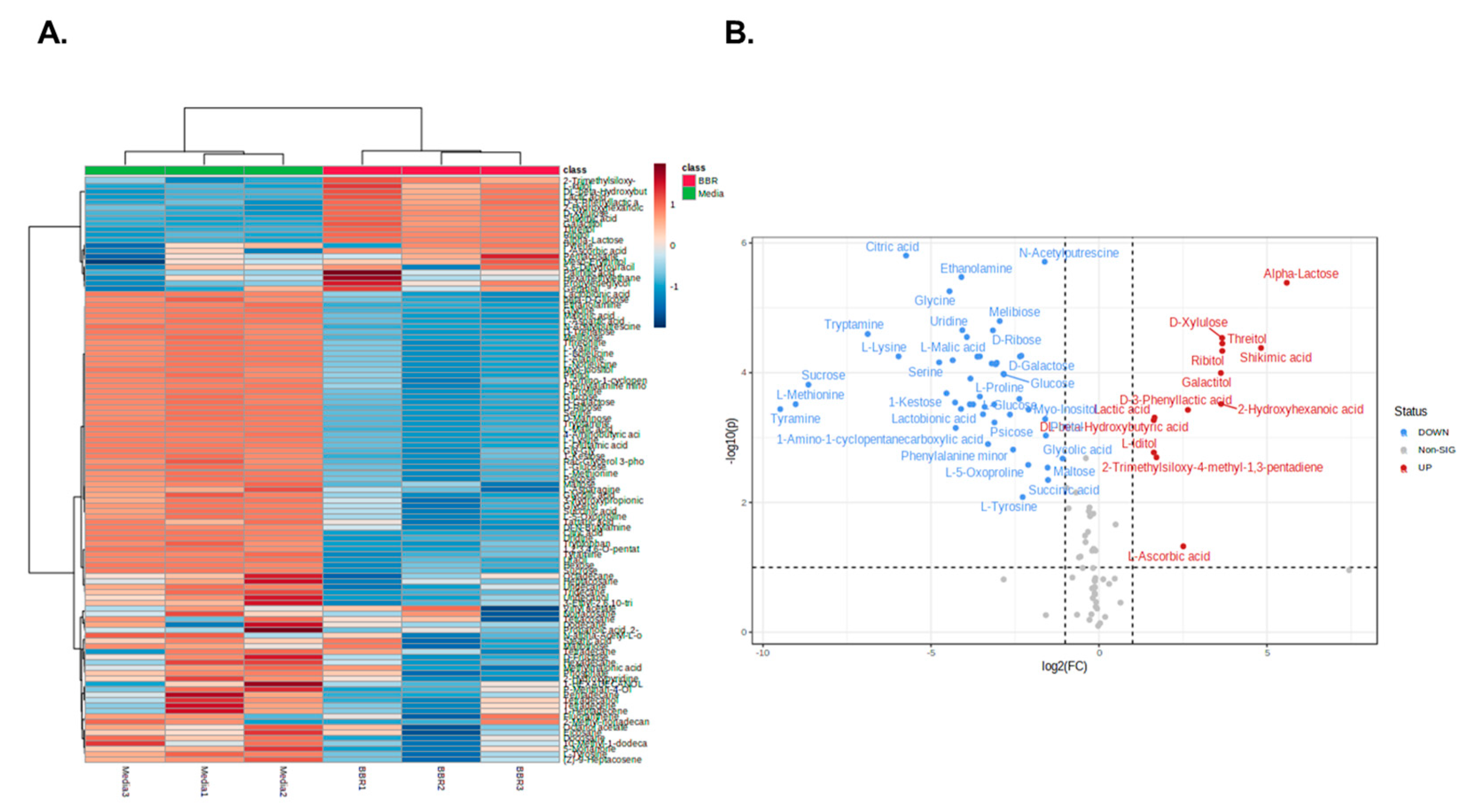
3.2. Metabolites Analysis
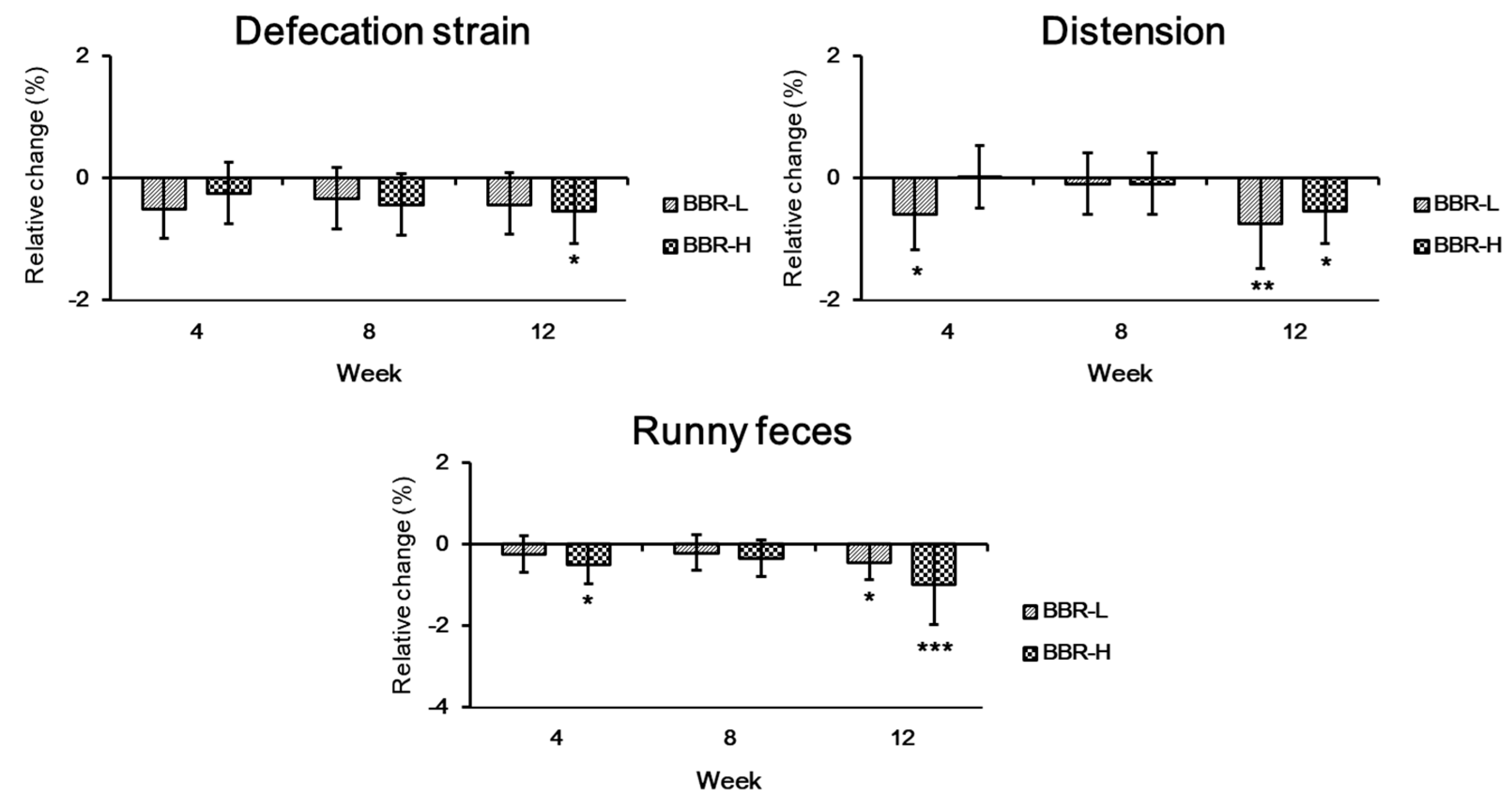
3.3. Changes in Bowel Habits
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Paukner, K.; Králová Lesná, I.; Poledne, R. Cholesterol in the cell membrane-an emerging player in atherogenesis. Int. J. Mol. Sci. 2022, 23, 533. [Google Scholar] [CrossRef] [PubMed]
- Craig, M.; Yarrarapu, S.N.S.; Dimri, M. Biochemistry, Cholesterol. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Elmehdawi, R.R. Hypolipidemia: A word of caution. Libyan J. Med. 2008, 3, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Sahadevan, M.; Kasiske, B.L. Hyperlipidemia in kidney disease: Causes and consequences. Curr. Opin. Nephrol. Hypertens. 2002, 11, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.W.; Zheng, L.; Wang, Q. Regulation of cholesterol homeostasis by liver X receptors. Clin. Chim. Acta 2010, 411, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Musso, G.; Gambino, R.; Cassader, M. Cholesterol metabolism and the pathogenesis of non-alcoholic steatohepatitis. Prog. Lipid Res. 2013, 52, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Nair, P. Brown and Goldstein: The cholesterol chronicles. Proc. Natl Acad. Sci. USA 2013, 110, 14829–14832. [Google Scholar] [CrossRef] [PubMed]
- Feingold, K.R. Cholesterol lowering drugs. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Boyce, A., Blackman, M.R., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Kalra, S., Kaltsas, G., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2020. [Google Scholar]
- Taher, T.H.; Dzavik, V.; Reteff, E.M.; Pearson, G.J.; Woloschuk, B.L.; Francis, G.A. Tolerability of statin-fibrate and statin-niacin combination therapy in dyslipidemic patients at high risk for cardiovascular events. Am. J. Cardiol. 2002, 89, 390–394. [Google Scholar] [CrossRef]
- Jones, M.L.; Tomaro-Duchesneau, C.; Martoni, C.J.; Prakash, S. Cholesterol lowering with bile salt hydrolase-active probiotic bacteria, mechanism of action, clinical evidence, and future direction for heart health applications. Expert Opin. Biol. Ther. 2013, 13, 631–642. [Google Scholar] [CrossRef]
- Williams, N.T. Probiotics. Am. J. Health Syst. Pharm. 2010, 67, 449–458. [Google Scholar] [CrossRef]
- Ishimwe, N.; Daliri, E.B.; Lee, B.H.; Fang, F.; Du, G. The perspective on cholesterol-lowering mechanisms of probiotics. Mol. Nutr. Food Res. 2015, 59, 94–105. [Google Scholar] [CrossRef]
- Ooi, L.G.; Liong, M.T. Cholesterol-lowering effects of probiotics and prebiotics: A review of in vivo and in vitro findings. Int. J. Mol. Sci. 2010, 11, 2499–2522. [Google Scholar] [CrossRef] [PubMed]
- Nataraj, B.H.; Ali, S.A.; Behare, P.V.; Yadav, H. Postbiotics-parabiotics: The new horizons in microbial biotherapy and functional foods. Microb. Cell Fact. 2020, 19, 168. [Google Scholar] [CrossRef]
- Park, D.H.; Kim, J.W.; Park, H.J.; Hahm, D.H. Comparative analysis of the microbiome across the gut–skin axis in atopic dermatitis. Int. J. Mol. Sci. 2021, 22, 4228. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.; Kim, G.; Noh, M.G.; Park, J.H.; Jang, M.; Fang, S.; Park, H. Lactobacillus fermentum promotes adipose tissue oxidative phosphorylation to protect against diet-induced obesity. Exp. Mol. Med. 2020, 52, 1574–1586. [Google Scholar] [CrossRef] [PubMed]
- Salminen, S.; Collado, M.C.; Endo, A.; Hill, C.; Lebeer, S.; Quigley, E.M.M.; Sanders, M.E.; Shamir, R.; Swann, J.R.; Szajewska, H.; et al. The International Scientific Association of Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of postbiotics. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 649–667. [Google Scholar] [CrossRef] [PubMed]
- Siciliano, R.A.; Reale, A.; Mazzeo, M.F.; Morandi, S.; Silvetti, T.; Brasca, M. Paraprobiotics: A new perspective for functional foods and nutraceuticals. Nutrients 2021, 13, 1225. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.C.; Kim, M.G. The mechanism of blood cholesterol-lowering action of parabiotics. Food Suppl. Biomater. Health 2023, 3, e1. [Google Scholar] [CrossRef]
- Kim, M.G.; Lee, D.G.; Kim, T.Y. Development of heat-killed Bifidobacterium breve IDCC 4401 with the potential to improve hypercholesterolemia in rats. Korean J. Microbiol. 2020, 56, 307–314. [Google Scholar]
- Joo, I.-H.; Kim, M.-G.; Park, J.-M.; Min, G.-Y.; Han, S.-H.; Lee, S.-B.; Sim, B.-Y.; Kim, J.-H.; Kim, D.-H. Bifidobacterium breve strain IDCC 4401 improves dyslipidemia in rat model. Int. J. Clin. Exp. Med. 2020, 13, 4137–4144. [Google Scholar]
- Zhuang, X.; Tian, Z.; Li, L.; Zeng, Z.; Chen, M.; Xiong, L. Fecal microbiota alternations associated with diarrhea-predominant irritable bowel syndrome. Front. Microbiol. 2018, 9, 1600. [Google Scholar] [CrossRef]
- O’Donnell, L.J.; Virjee, J.; Heaton, K.W. Detection of pseudodiarrhoea by simple clinical assessment of intestinal transit rate. BMJ 1990, 300, 439–440. [Google Scholar] [CrossRef] [PubMed]
- Park, M.-J.; Na, H.-O.; Kim, Y.-I.; Kim, K.-S. The factors affecting subject’s compliance in a clinical study. Transl. Clin. Pharmacol. 2009, 17, 61–71. [Google Scholar] [CrossRef]
- Jiang, H.; Tan, S.; Ning, K.; Li, H.; Zhao, W.; Zhao, A.; Zhu, H.; Wang, S.; Wang, P.; Zhang, Y. Effects of Lactobacillus paracasei N1115 on dyslipidaemia: A randomized controlled study. J. Funct. Foods 2022, 89, 104956. [Google Scholar] [CrossRef]
- Zhou, Z.; Rahme, E.; Pilote, L. Are statins created equal? Evidence from randomized trials of pravastatin, simvastatin, and atorvastatin for cardiovascular disease prevention. Am. Heart J. 2006, 151, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Weng, T.C.; Yang, Y.H.K.; Lin, S.J.; Tai, S.H. A systematic review and meta-analysis on the therapeutic equivalence of statins. J. Clin. Pharm. Ther. 2010, 35, 139–151. [Google Scholar] [CrossRef]
- Kelly, M.S.; Beavers, C.; Bucheit, J.D.; Sisson, E.M.; Dixon, D.L. Pharmacologic approaches for the management of patients with moderately elevated triglycerides (150–499 mg/dl). J. Clin. Lipidol. 2017, 11, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Capuzzi, D.M.; Morgan, J.M.; Weiss, R.J.; Chitra, R.R.; Hutchinson, H.G.; Cressman, M.D. Beneficial effects of rosuvastatin alone and in combination with extended-release niacin in patients with a combined hyperlipidemia and low high-density lipoprotein cholesterol levels. Am. J. Cardiol. 2003, 91, 1304–1310. [Google Scholar] [CrossRef]
- Feingold, K.R.; Grunfeld, C. Introduction to lipids and lipoproteins. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Boyce, A., Blackman, M.R., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Kalra, S., Kaltsas, G., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2018. [Google Scholar]
- Chen, W.; Guo, J.X.; Chang, P. The effect of taurine on cholesterol metabolism. Mol. Nutr. Food Res. 2012, 56, 681–690. [Google Scholar] [CrossRef]
- McRae, M.P. Vitamin C supplementation lowers serum low-density lipoprotein cholesterol and triglycerides: A meta-analysis of 13 randomized controlled trials. J. Chiropr. Med. 2008, 7, 48–58. [Google Scholar] [CrossRef]
- Dludla, P.V.; Nkambule, B.B.; Nyambuya, T.M.; Ziqubu, K.; Mabhida, S.E.; Mxinwa, V.; Mokgalaboni, K.; Ndevahoma, F.; Hanser, S.; Mazibuko-Mbeje, S.E.; et al. Vitamin C intake potentially lowers total cholesterol to improve endothelial function in diabetic patients at increased risk of cardiovascular disease: A systematic review of randomized controlled trials. Front. Nutr. 2022, 9, 1011002. [Google Scholar] [CrossRef]
- Trupp, M.; Zhu, H.; Wikoff, W.R.; Baillie, R.A.; Zeng, Z.B.; Karp, P.D.; Fiehn, O.; Krauss, R.M.; Kaddurah-Daouk, R. Metabolomics reveals amino acids contribute to variation in response to simvastatin treatment. PLoS ONE 2012, 7, e38386. [Google Scholar] [CrossRef] [PubMed]
- Catalina, D.; Quiroz, D.; Carmona, B.; Bolívar, F.; Escalante, A. Current perspectives on applications of shikimic and aminoshikimic acids in pharmaceutical chemistry. Res. Rep. Med. Chem. 2014, 4, 35–46. [Google Scholar]
- Kim, M.J.; Sim, D.Y.; Lee, H.M.; Lee, H.J.; Kim, S.H. Hypolipogenic effect of shikimic acid via inhibition of MID1IP1 and phosphorylation of AMPK/ACC. Int. J. Mol. Sci. 2019, 20, 582. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Rust, B.; Picklo, M.J. Plasma metabolomics changes in mice with time restricted feeding-attenuated pulmonary metastasis of Lewis lung carcinoma. Anticancer Res. 2020, 40, 1833–1841. [Google Scholar] [CrossRef] [PubMed]
- Aldridge, M.A.; Ito, M.K. Colesevelam hydrochloride: A novel bile acid-binding resin. Ann. Pharmacother. 2001, 35, 898–907. [Google Scholar] [CrossRef] [PubMed]
- Ueno, N.; Fujiya, M.; Segawa, S.; Nata, T.; Moriichi, K.; Tanabe, H.; Mizukami, Y.; Kobayashi, N.; Ito, K.; Kohgo, Y. Heat-killed body of Lactobacillus brevis SBC8803 ameliorates intestinal injury in a murine model of colitis by enhancing the intestinal barrier function. Inflamm. Bowel Dis. 2011, 17, 2235–2250. [Google Scholar] [CrossRef] [PubMed]
- Ramiah, K.; van Reenen, C.A.; Dicks, L.M. Surface-bound proteins of Lactobacillus plantarum 423 that contribute to adhesion of Caco-2 cells and their role in competitive exclusion and displacement of Clostridium sporogenes and Enterococcus faecalis. Res. Microbiol. 2008, 159, 470–475. [Google Scholar] [CrossRef]
- Li, N.; Russell, W.M.; Douglas-Escobar, M.; Hauser, N.; Lopez, M.; Neu, J. Live and heat-killed Lactobacillus rhamnosus GG: Effects on proinflammatory and anti-inflammatory cytokines/chemokines in gastrostomy-fed infant rats. Pediatr. Res. 2009, 66, 203–207. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Visit | ||||
|---|---|---|---|---|---|
| 1(−4 week) | 2(0 week) | 3(4 week) | 4(8 week) | 5(12 week) | |
| Informed consent | √ | ||||
| Demographic information | √ | ||||
| Anthropometric measurement | √ | √ | √ | √ | |
| Vital signs | √ | √ | √ | √ | √ |
| Medical and operational history | √ | ||||
| Medication and dietary supplement use | √ | √ | √ | √ | √ |
| Blood and urine test | √ | ||||
| Eligibility assessment | √ | √ | |||
| Random allocation | √ | ||||
| MEDFICTS and recommended food score | √ | √ | √ | ||
| Physical activity survey | √ | √ | √ | ||
| Drinking and smoking history survey | √ | √ | √ | ||
| Guidelines for diet and lifestyle habits | √ | √ | √ | √ | |
| Dietary record and lifestyle | √ | √ | √ | ||
| Supply with test/placebo food | √ | √ | √ | ||
| Compliance | √ | √ | √ | ||
| Lipid profile and analysis (TG, TC, LDL-C, HDL-C, VLDL-C, non HDL-C, ApoAI, Apo AII, ApoB, ApoE) | √ | √ | √ | √ | |
| Bowel habit satisfaction | √ | √ | √ | √ | |
| Hematologic tests | √ | √ | |||
| Urine analysis | √ | √ | |||
| Electrocardiogram | √ | √ | |||
| Adverse events | √ | √ | √ | √ | √ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.; Lee, M.; Kim, M.-G.; Kim, H.; Choi, B.; Kim, S.; Bang, W.-Y.; Kim, Y.-J.; Yang, J.; Kang, H.-J. A Randomized, Double-Blind, Placebo-Controlled Trial to Evaluate the Cholesterol-Lowering Effect of BBR 4401 in Adults with Moderate Hypercholesterolemia. Fermentation 2023, 9, 766. https://doi.org/10.3390/fermentation9080766
Kim M, Lee M, Kim M-G, Kim H, Choi B, Kim S, Bang W-Y, Kim Y-J, Yang J, Kang H-J. A Randomized, Double-Blind, Placebo-Controlled Trial to Evaluate the Cholesterol-Lowering Effect of BBR 4401 in Adults with Moderate Hypercholesterolemia. Fermentation. 2023; 9(8):766. https://doi.org/10.3390/fermentation9080766
Chicago/Turabian StyleKim, Mincheol, Minjee Lee, Min-Goo Kim, Hayoung Kim, Boyoung Choi, Seongsik Kim, Won-Yeong Bang, Yong-Jin Kim, Jungwoo Yang, and Hyun-Jae Kang. 2023. "A Randomized, Double-Blind, Placebo-Controlled Trial to Evaluate the Cholesterol-Lowering Effect of BBR 4401 in Adults with Moderate Hypercholesterolemia" Fermentation 9, no. 8: 766. https://doi.org/10.3390/fermentation9080766