

Evaluation of Propolis Hydrogel for the Treatment of Dentinal Sensitivity: A Clinical Study
 and
and
Abstract
:1. Introduction
2. Results and Discussion
3. Conclusions
4. Materials and Methods
4.1. Formulation of the Materials
4.1.1. Preparing 2% Sodium Fluoride and 1.23% Acidulated Phosphate Fluoride
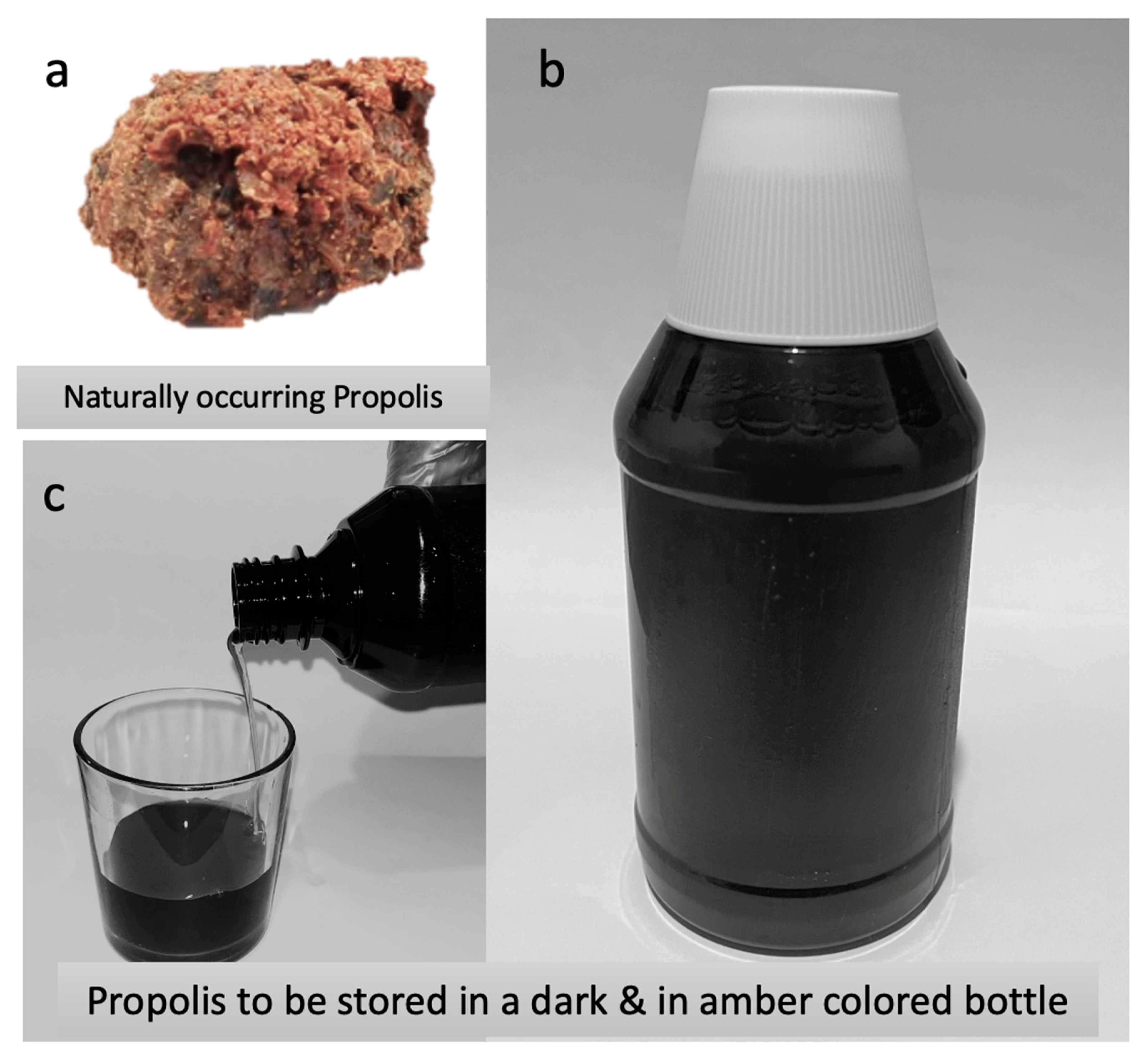
4.1.2. Preparation of 10% Propolis Hydrogel
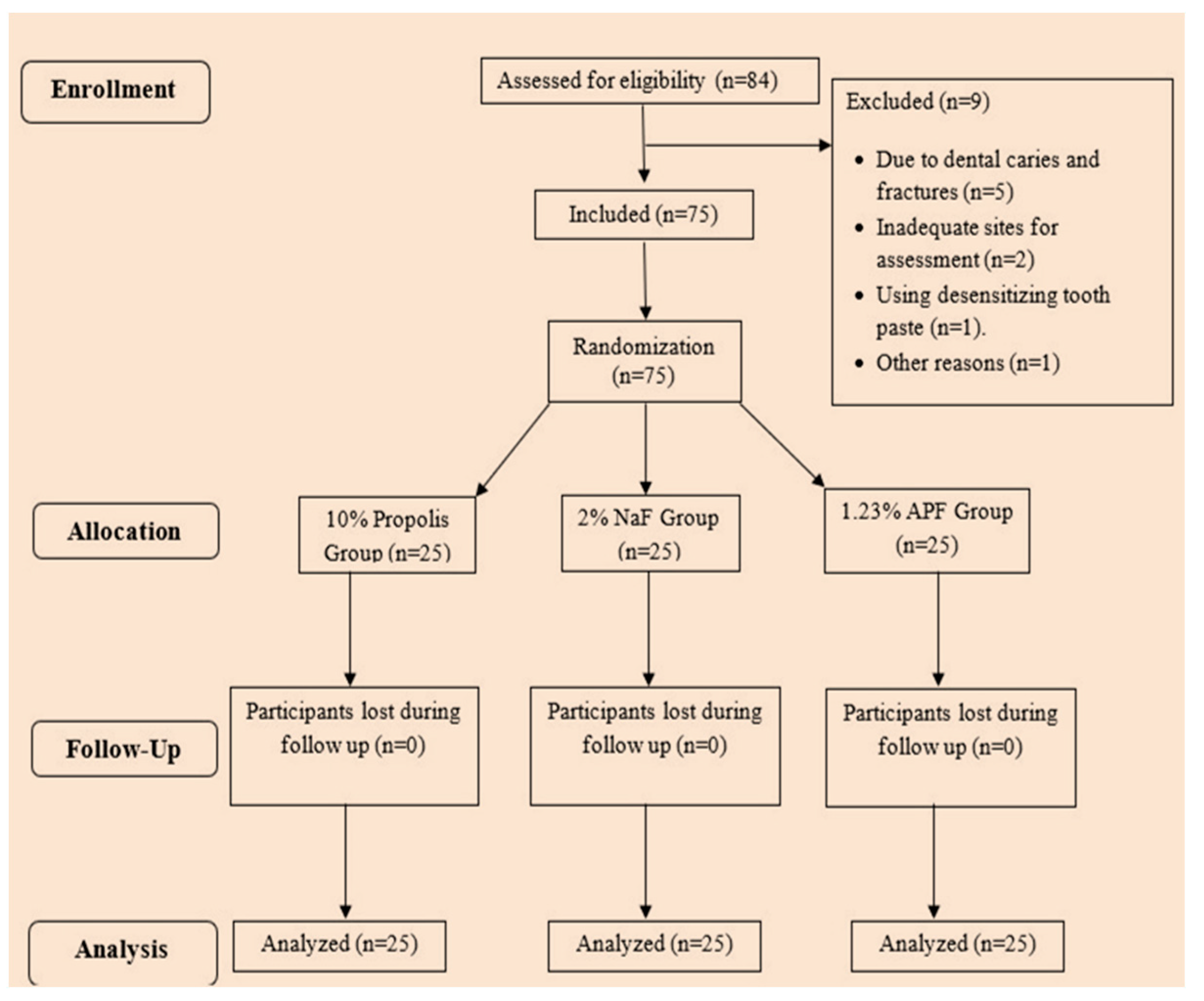
4.2. Study Design
4.3. Study Participants
4.4. Application of Desensitizing Agents
4.5. Application of Iontophoresis
4.6. Assessing Clinical Parameters
4.7. Power Calculation and Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cummins, D. Recent advances in dentin hypersensitivity: Clinically proven treatments for instant and lasting sensitivity relief. Am. J. Dent. 2010, 23, 3A–13A. [Google Scholar] [PubMed]
- Yin, L.; Xu, X.; Chu, C.; Lin, P.; Huang, H.; Luo, B.; Yang, C. In-vitro characterization and evaluation of mesoporous titanium dioxide composite hydroxyapatite and its effectiveness in occluding dentine tubules. BMC Oral Health 2022, 22, 43. [Google Scholar] [CrossRef] [PubMed]
- Kiesow, A.; Menzel, M.; Lippert, F.; Tanzer, J.M.; Milgrom, P. Dentin tubule occlusion by a 38% silver diamine fluoride gel: An in vitro investigation. BDJ Open 2022, 8, 1. [Google Scholar] [CrossRef]
- Tamilselvi, S.; Nagate, R.R.; Al-Ahmari, M.M.M.; Kokila, G.; Tikare, S.; Chaturvedi, S. Comparison of the effect of sodium bicarbonate and glycine air polishing systems on tooth surface roughness: An atomic force microscopic analysis. Technol. Health Care 2021, 29, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Chidchuangchai, W.; Vongsavan, N.; Matthews, B. Sensory transduction mechanisms responsible for pain caused by cold stimulation of dentine in man. Arch. Oral Biol. 2007, 52, 154–160. [Google Scholar] [CrossRef]
- Mittal, P.; Gokhale, S.T.; Manjunath, S.; Al-Qahtani, S.M.; Magbol, M.A.; Nagate, R.R.; Tikare, S.; Chaturvedi, S.; Agarwal, A.; Venkataram, V. Comparative Evaluation of Locally Administered 2% Gel Fabricated from Lemongrass Polymer and 10% Doxycycline Hyclate Gel as an Adjunct to Scaling and Root Planing in the Treatment of Chronic Periodontitis—A Randomized Controlled Trial. Polymers 2022, 14, 2766. [Google Scholar] [CrossRef]
- Koppolu, P.; Qamar, Z.; Abdul, N.S.; Shenoy, M.; Reddy, R.N.; Kakti, A.; Barakat, A.A.; Niazi, F.H. Noncarious cervical lesion pretreated using antimicrobial photodynamic therapy and diode laser in reducing dentin hypersensitivity bonded to different restorative material: Valuation of bond values and invitro dye leakage. Photodiagnosis Photodyn. Ther. 2022, 39, 102885. [Google Scholar] [CrossRef]
- Idon, P.I.; Ikusika, O.F.; Sotunde, O.A.; Ogundare, T.O. Are there associations between the occurrence of dental fluorosis and the experience of dentine hypersensitivity? A cross-sectional study. Niger. Postgrad. Med. J. 2022, 29, 161–166. [Google Scholar] [CrossRef]
- Erkoc, P.; Ulucan-Karnak, F. Nanotechnology-Based Antimicrobial and Antiviral Surface Coating Strategies. Prosthesis 2021, 3, 25–52. [Google Scholar] [CrossRef]
- Bartlett, D.W.; Shah, P. A critical review of non-carious cervical (wear) lesions and the role of abfraction, erosion, and abrasion. J. Dent. Res. 2006, 85, 306–312. [Google Scholar] [CrossRef]
- Que, K.; Guo, B.; Jia, Z.; Chen, Z.; Yang, J.; Gao, P. A cross-sectional study: Non-carious cervical lesions, cervical dentine hypersensitivity and related risk factors. J. Oral Rehabil. 2013, 40, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Rai, J.J.; Chaturvedi, S.; Gokhale, S.T.; Nagate, R.R.; Al-Qahtani, S.M.; Magbol, M.A.; Bavabeedu, S.S.; Elagib, M.F.A.; Venkataram, V.; Chaturvedi, M. Effectiveness of a Single Chair Side Application of NovaMin® [Calcium Sodium Phosphosilicate] in the Treatment of Dentine Hypersensitivity following Ultrasonic Scaling—A Randomized Controlled Trial. Materials 2023, 16, 1329. [Google Scholar] [CrossRef]
- Brännström, M.; Aström, A. The hydrodynamics of the dentine; its possible relationship to dentinal pain. Int. Dent. J. 1972, 22, 219–227. [Google Scholar] [PubMed]
- Hendre, A.D.; Taylor, G.W.; Chávez, E.M.; Hyde, S. A systematic review of silver diamine fluoride: Effectiveness and application in older adults. Gerodontology 2017, 34, 411–419. [Google Scholar] [CrossRef] [PubMed]
- da Rosa, W.L.d.O.; Lund, R.G.; Piva, E.; da Silva, A.F. The effectiveness of current dentin desensitizing agents used to treat dental hypersensitivity: A systematic review. Quintessence Int. 2013, 44, 535–546. [Google Scholar] [CrossRef]
- de CSales-Peres, S.H.; de Carvalho, F.N.; Marsicano, J.A.; Mattos, M.C.; Pereira, J.C.; Forim, M.R.; da Silva, M.F.d.G.F. Effect of propolis gel on the in vitro reduction of dentin permeability. J. Appl. Oral Sci. 2011, 19, 318–323. [Google Scholar] [CrossRef]
- El-Guendouz, S.; Lyoussi, B.; Miguel, M.G. Insight on Propolis from Mediterranean Countries: Chemical Composition, Biological Activities and Application Fields. Chem. Biodivers 2019, 16, e1900094. [Google Scholar] [CrossRef]
- Ezeaku, A.; Okike, B.M.; Ajaegbu, E.E.; Ikuesan, A.J.; Okafor, N.R.; Ezeagwu, P.C.; Ezeagha, C.C. Evaluation of Various Traditional Methods Used in the Treatment of Dental Diseases Using Natural Products Found in Abejukolo Community, Omala Local Government Area, Kogi State. Trop. J. Nat. Prod. Res. 2022, 6, 433–437. [Google Scholar]
- Vazirizadeh, Y.; Azizi, A.; Lawaf, S. Comparison of the efficacy of 940-nm diode laser, Gluma, and 5% sodium fluoride varnish in dentinal tubule occlusion. Lasers Dent. Sci. 2022, 6, 63–70. [Google Scholar] [CrossRef]
- Demirci, M.; Karabay, F.; Berkman, M.; Özcan, I.; Tuncer, S.; Tekçe, N.; Baydemir, C. The prevalence, clinical features, and related factors of dentin hypersensitivity in the Turkish population. Clin. Oral Investig. 2022, 26, 2719–2732. [Google Scholar] [CrossRef]
- Koo, H.; Vacca Smith, A.M.; Bowen, W.H.; Rosalen, P.L.; Cury, J.A.; Park, Y.K. Effects of Apis mellifera propolis on the activities of streptococcal glucosyltransferases in solution and adsorbed onto saliva-coated hydroxyapatite. Caries Res. 2000, 34, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Nair, U.P.; Shivamurthy, R.; Nagate, R.R.; Chaturvedi, S.; Al-Qahtani, S.M.; Al Magbol, M.; Gokhale, S.T.; Tikare, S.; Chaturvedi, M. Effect of Injectable Platelet-Rich Fibrin with a Nano-Hydroxyapatite Bone Graft on the Treatment of a Grade II Furcation Defect. Bioengineering 2022, 9, 602. [Google Scholar] [CrossRef] [PubMed]
- Purra, A.R.; Mushtaq, M.; Acharya, S.R.; Saraswati, V. A comparative evaluation of propolis and 5.0% potassium nitrate as a dentine desensitizer: A clinical study. J. Indian Soc. Periodontol. 2014, 18, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Torwane, N.; Chandrashekar, B.; Goel, P.; Hongal, S. The effect of 30% ethanolic extract of Indian propolis on replica of human dentin compared against commercially available desensitizing agent: A methodological SEM study in vitro. Pharmacogn. Res. 2014, 6, 113. [Google Scholar] [CrossRef]
- Almas, K.; Mahmoud, A.; Dahlan, A. A comparative study of propolis and saline application on human dentin. A SEM study. Indian J. Dent. Res. 2001, 12, 21–27. [Google Scholar]
- Dobrowolski, J.W.; Vohora, S.B.; Sharma, K.; Shah, S.A.; Naqvi, S.A.H.; Dandiya, P.C. Antibacterial, antifungal, antiamoebic, antiinflammatory and antipyretic studies on propolis bee products. J. Ethnopharmacol. 1991, 35, 77–82. [Google Scholar] [CrossRef]
- Tavares, J.A.O.; da Silva, F.A.; Santos, T.M.L.; Caneppele, T.M.F.; Augusto, M.G. The effectiveness of propolis extract in reducing dentin hypersensitivity: A systematic review. Arch. Oral Biol. 2021, 131, 105248. [Google Scholar] [CrossRef]
- Solati, M.; Fekrazad, R.; Vahdatinia, F.; Farmany, A.; Farhadian, M.; Hakimiha, N. Dentinal tubule blockage using nanobioglass in the presence of diode (980 nm) and Nd:YAG lasers: An in vitro study. Clin. Oral Investig. 2022, 26, 2975–2981. [Google Scholar] [CrossRef]
- Barros, A.P.O.; de Melo Alencar, C.; de Melo Pingarilho Carneiro, A.; da Silva Pompeu, D.; Barbosa, G.M.; Araújo, J.L.N.; Silva, C.M. Combination of two desensitizing protocols to control dentin hypersensitivity in non-carious lesions: A randomized, double-blind clinical trial. Clin. Oral Investig. 2022, 26, 1299–1307. [Google Scholar] [CrossRef]
- Ongphichetmetha, N.; Lertpimonchai, A.; Champaiboon, C. Bioactive glass and arginine dentifrices immediately relieved dentine hypersensitivity following non-surgical periodontal therapy: A randomized controlled trial. J. Periodontol. 2022, 93, 246–255. [Google Scholar] [CrossRef]
- Chen, Z.; Duan, Y.; Shan, S.; Sun, K.; Wang, G.; Shao, C.; Tang, Z.; Xu, Z.; Zhou, Y.; Chen, Z.; et al. Deep and compact dentinal tubule occlusion: Via biomimetic mineralization and mineral overgrowth. Nanoscale 2022, 14, 642–652. [Google Scholar] [CrossRef] [PubMed]
- Kijsamanmith, K.; Wallanon, P.; Pitchayasatit, C.; Kittiratanaviwat, P. The effect of fluoride iontophoresis on seal ability of self-etch adhesive in human dentin in vitro. BMC Oral Health 2022, 22, 109. [Google Scholar] [CrossRef] [PubMed]
- Brahmbhatt, N.; Bhavsar, N.; Sahayata, V.; Acharya, A.; Kshatriya, P. A double blind controlled trial comparing three treatment modalities for dentin hypersensitivity. Med. Oral Patol. Oral Cir. Bucal 2012, 17, e483–e490. [Google Scholar] [CrossRef] [PubMed]
- Singal, P.; Gupta, R.; Pandit, N. 2% sodium fluoride-iontophoresis compared to a commercially available desensitizing agent. J. Periodontol. 2005, 76, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Dam, V.V.; Nguyen, T.H.; Trinh, H.A.; Dung, D.T.; Hai, T.D. Advances in the Management of Dentin Hypersensitivity: An Updated Review. Open Dent. J. 2022, 16, e187421062201130. [Google Scholar] [CrossRef]
- Martins, C.C.; Riva, J.J.; Firmino, R.T.; Schünemann, H.J. Formulations of desensitizing toothpastes for dentin hypersensitivity: A scoping review. J. Appl. Oral Sci. 2022, 30, e20210410. [Google Scholar] [CrossRef]
- Nard, G.M.; Sabatin, S.; Acito, G.; Colavito, A.; Chiavistell, L.; Campus, G. The Decision Tree for Clinical Management of Dentin Hypersensitivity. A Consensus Report. Oral Health Prev. Dent. 2022, 20, 27–32. [Google Scholar] [CrossRef]
- Machado, A.C.; Maximiano, V.; Yoshida, M.L.; Freitas, J.G.; Mendes, F.M.; Aranha, A.C.C.; Scaramucci, T. Efficacy of a calcium-phosphate/fluoride varnish and ionomeric sealant on cervical dentin hypersensitivity: A randomized, double-blind, placebo-controlled clinical study. J. Oral Rehabil. 2022, 49, 62–70. [Google Scholar] [CrossRef]
- Tang, H.; Zhu, Y.W.; Zhu, J.X.; Li, Q.L. Occluding dentin tubules with monetite paste in vitro. West China J. Stomatology 2021, 39, 667–674. [Google Scholar] [CrossRef]
- Naseri, S.; Cooke, M.E.; Rosenzweig, D.H.; Tabrizian, M. 3D printed in vitro dentin model to investigate occlusive agents against tooth sensitivity. Materials 2021, 14, 7255. [Google Scholar] [CrossRef]
- Shan, Z.; Ji, J.; McGrath, C.; Gu, M.; Yang, Y. Effects of low-level light therapy on dentin hypersensitivity: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 6571–6595. [Google Scholar] [CrossRef] [PubMed]
- Erdemir, U.; Yildiz, E.; Kilic, I.; Yucel, T.; Ozel, S. The efficacy of three desensitizing agents used to treat dentin hypersensitivity. J. Am. Dent. Assoc. 2010, 141, 285–296. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Liang, B.; Jin, X.; Fu, B.; Hannig, M. Comparative in vivo study on the desensitizing efficacy of dentin desensitizers and one-bottle self-etching adhesives. Oper Dent. 2010, 35, 279–286. [Google Scholar] [CrossRef]
- Wanasathop, A.; Kevin Li, S. Iontophoretic drug delivery in the oral cavity. Pharmaceutics 2018, 10, 121. [Google Scholar] [CrossRef]
- Jalaluddin, M.; Almalki, S.A. Evaluation of the efficacy of three different treatment modalities in the management of dentinal hypersensitivity: A comparative study. World J. Dent. 2019, 10, 202–206. [Google Scholar] [CrossRef]
- Murugesan, S.; Kumar, P.; Reddy, B.N.; Arumugam, K.; Mohankumar, P.; Chandrasekaran, K. Novel Management of Hypersensitive Dentin Using Propolis-based Herbal Desensitizing Agents: An In Vitro Scanning Electron Microscopic Study. J. Contemp. Dent. Pract. 2021, 22, 1030–1034. [Google Scholar] [CrossRef] [PubMed]
- Kripal, K.; Chandrasekaran, K.; Chandrasekaran, S.; Kumar, V.; Chavan, S.; Dileep, A. Treatment of dentinal hypersensitivity using propolis varnish: A scanning electron microscope study. Indian J. Dent. Res. 2019, 30, 249–253. [Google Scholar] [CrossRef]
- Demydova, P.I. Diode laser irradiation combined with propolis application as a treatment for dentine hypersensitivity. J. Stomatol. 2020, 73, 170–175. [Google Scholar] [CrossRef]
- Carvalho, C.D.; Fernandes, W.H.C.; Mouttinho, T.B.F.; Souza, D.M.D.; Marcucci, M.C.; D’Alpino, P.H.P. Evidence-Based Studies and Perspectives of the Use of Brazilian Green and Red Propolis in Dentistry. Eur. J. Dent. 2019, 13, 459–469. [Google Scholar] [CrossRef]
- Kumar, S.; Thomas, B.S.; Gupta, K.; Guddattu, V.; Alexander, M. Iontophoresis and Topical Application of 8% Arginine-calcium Carbonate to Treat Dentinal Hypersensitivity. Niger J. Clin. Pract. 2018, 21, 1029–1033. [Google Scholar] [CrossRef]
- Brink, A.F.T.; Proulx, M.J.; Bultitude, J.H. Validation of the Leiden Visual Sensitivity Scale and Visual Discomfort Scale in Chronic Pain Conditions. Perception 2021, 50, 399–417. [Google Scholar] [CrossRef] [PubMed]
- Kern, D.A.; McQuade, M.J.; Scheidt, M.J.; Hanson, B.; van Dyke, T.E. Effectiveness of sodium fluoride on tooth hypersensitivity with and without iontophoresis. J. Periodontol. 1989, 60, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Olusile, A.O.; Bamise, C.T.; Oginni, A.O.; Dosumu, O.O. Short-term clinical evaluation of four desensitizing agents. J. Contemp. Dent. Pract. 2008, 9, 22–29. [Google Scholar]
- Aranha, A.C.C.; Pimenta, L.A.F.; Marchi, G.M. Clinical evaluation of desensitizing treatments for cervical dentin hypersensitivity. Braz. Oral Res. 2009, 23, 333–339. [Google Scholar] [CrossRef]
- Aparna, S.; Setty, S.; Thakur, S. Comparative efficacy of two treatment modalities for dentinal hypersensitivity: A clinical trial. Indian J. Dent. Res. 2010, 21, 544–548. [Google Scholar] [CrossRef] [PubMed]
- Torwane, N.A.; Hongal, S.; Goel, P.; Chandrashekar, B.R.; Jain, M.; Saxena, E. A clinical efficacy of 30% ethenolic extract of Indian propolis and RecaldentTM in management of dentinal hypersensitivity: A comparative randomized clinical trial. Eur. J. Dent. 2013, 7, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Madhavan, S.; Nayak, M.; Shenoy, A.; Shetty, R.; Prasad, K. Dentinal hypersensitivity: A comparative clinical evaluation of CPP-ACP F, sodium fluoride, propolis, and placebo. J. Conserv. Dent. 2012, 15, 315–318. [Google Scholar] [CrossRef]
- Stadeker, W. Effectively treating dental hypersensitivity. Dent. Today 2011, 30, 182–185. [Google Scholar]
- Ojha, N. Dentinal hypersensitivity: A review on effective treatment with potassium nitrate containing dentifrice. Int. J. Pharma. Bio Sci. 2013, 4, 201–206. [Google Scholar]
- Cartwright, R.B. Dentinal hypersensitivity: A narrative review. Community Dent. Health 2014, 31, 15–20. [Google Scholar] [CrossRef]
- Panda, A.; Satpathy, A.; Mohanty, R.; Nayak, R.; Panda, S. Herbal agents for dentinal hypersensitivity: A review. Indian J. Public Health Res. Dev. 2019, 10, 1002–1003. [Google Scholar] [CrossRef]
- Krell, R. Value-Added Products from Beekeeping; FAO Agricultural Services Bulletin No 124; FAO: Rome, Italy, 1996; Available online: http://www.fao.org/docrep/w0076e/w0076e00.HTM (accessed on 3 May 2023).
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2012, 10, 28–55. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
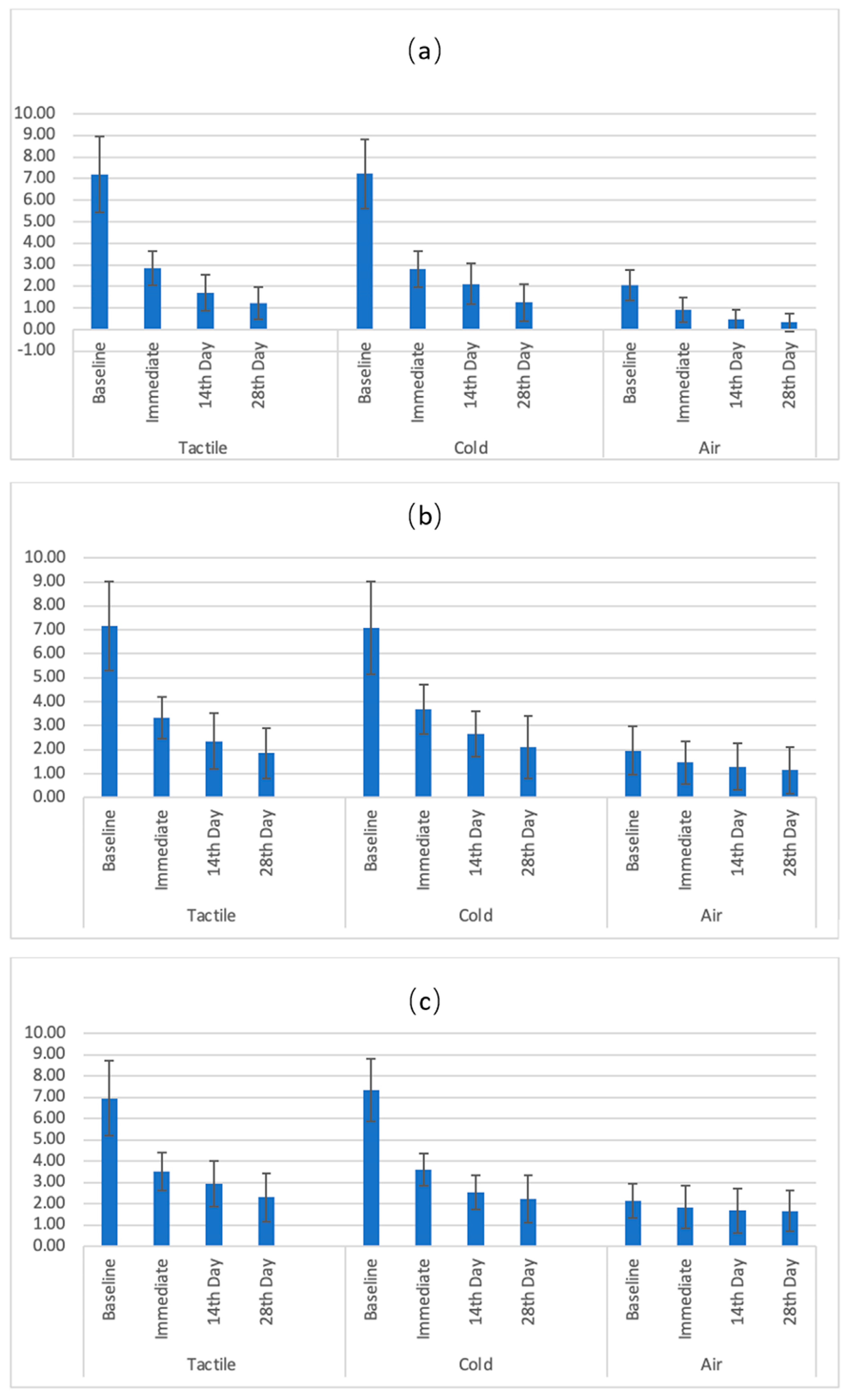
| Assessment Method | Products | Time Points | N | Mean | SD | SE |
|---|---|---|---|---|---|---|
| Tactile test | Sodium fluoride | Baseline | 25 | 7.20 | 1.77 | 0.35 |
| Immediate | 25 | 2.84 | 0.79 | 0.16 | ||
| 14th Day | 25 | 1.70 | 0.83 | 0.17 | ||
| 28th Day | 25 | 1.22 | 0.75 | 0.15 | ||
| Acidulated phosphate fluoride | Baseline | 25 | 7.18 | 1.85 | 0.37 | |
| Immediate | 25 | 3.34 | 0.86 | 0.17 | ||
| 14th Day | 25 | 2.36 | 1.17 | 0.23 | ||
| 28th Day | 25 | 1.86 | 1.06 | 0.21 | ||
| Propolis | Baseline | 25 | 6.96 | 1.77 | 0.35 | |
| Immediate | 25 | 3.52 | 0.88 | 0.18 | ||
| 14th Day | 25 | 2.94 | 1.06 | 0.21 | ||
| 28th Day | 25 | 2.30 | 1.12 | 0.22 | ||
| Cold test | Sodium fluoride | Baseline | 25 | 7.22 | 1.60 | 0.32 |
| Immediate | 25 | 2.80 | 0.83 | 0.17 | ||
| 14th Day | 25 | 2.12 | 0.95 | 0.19 | ||
| 28th Day | 25 | 1.26 | 0.87 | 0.17 | ||
| Acidulated phosphate fluoride | Baseline | 25 | 7.10 | 1.94 | 0.39 | |
| Immediate | 25 | 3.68 | 1.04 | 0.21 | ||
| 14th Day | 25 | 2.66 | 0.94 | 0.19 | ||
| 28th Day | 25 | 2.10 | 1.31 | 0.26 | ||
| Propolis | Baseline | 25 | 7.34 | 1.48 | 0.30 | |
| Immediate | 25 | 3.62 | 0.75 | 0.15 | ||
| 14th Day | 25 | 2.54 | 0.82 | 0.16 | ||
| 28th Day | 25 | 2.22 | 1.12 | 0.22 | ||
| Air Test | Sodium fluoride | Baseline | 25 | 2.08 | 0.70 | 0.14 |
| Immediate | 25 | 0.94 | 0.56 | 0.11 | ||
| 14th Day | 25 | 0.48 | 0.47 | 0.09 | ||
| 28th Day | 25 | 0.34 | 0.43 | 0.09 | ||
| Acidulated phosphate fluoride | Baseline | 25 | 1.96 | 1.01 | 0.20 | |
| Immediate | 25 | 1.46 | 0.90 | 0.18 | ||
| 14th Day | 25 | 1.28 | 0.97 | 0.19 | ||
| 28th Day | 25 | 1.14 | 0.96 | 0.19 | ||
| Propolis | Baseline | 25 | 2.14 | 0.80 | 0.16 | |
| Immediate | 25 | 1.84 | 1.01 | 0.20 | ||
| 14th Day | 25 | 1.68 | 1.03 | 0.21 | ||
| 28th Day | 25 | 1.66 | 0.95 | 0.19 |
| Assessment Method | Source | Type III Sum of Squares | df | Mean Square | F-Value | p-Value | Partial Eta Squared (Effect Size) |
|---|---|---|---|---|---|---|---|
| Tactile test | Groups | 24.47 | 2 | 12.24 | 7.3240 | 0.0001 * | 0.23 |
| Time | 1300.88 | 3 | 433.63 | 363.5090 | 0.0001 * | 0.94 | |
| Groups with Time | 16.62 | 6 | 2.77 | 9.9560 | 0.0001 * | 0.29 | |
| Total | 1341.97 | 11 | 122.00 | ||||
| Cold test | Groups | 20.82 | 2 | 10.41 | 11.5620 | 0.0001 * | 0.33 |
| Time | 1310.46 | 3 | 436.82 | 425.3980 | 0.0001 * | 0.95 | |
| Groups with Time | 9.69 | 6 | 1.61 | 6.7170 | 0.0001 * | 0.22 | |
| Total | 1340.97 | 11 | 121.91 | ||||
| Air test | Groups | 38.13 | 2 | 19.06 | 20.0750 | 0.0001 * | 0.46 |
| Time | 46.78 | 3 | 15.59 | 112.0960 | 0.0001 * | 0.82 | |
| Groups with Time | 13.27 | 6 | 2.21 | 15.4010 | 0.0001 * | 0.39 | |
| Total | 98.18 | 11 | 8.93 |
| Assessment Method | (I) Groups | (J) Groups | Mean Difference (I–J) | Std. Error | p-Value | 95% Confidence Interval for Difference | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| Tactile test | Sodium fluoride | Acidulated phosphate fluoride | −0.45 | 0.14 | 0.0110 * | −0.80 | −0.09 |
| Sodium fluoride | Propolis | −0.69 | 0.18 | 0.0020 * | −1.14 | −0.24 | |
| Acidulated phosphate fluoride | Propolis | −0.25 | 0.22 | 0.8560 | −0.82 | 0.33 | |
| Cold test | Sodium Fluoride | Acidulated phosphate fluoride | −0.54 | 0.12 | 0.0010 * | −0.84 | −0.23 |
| Sodium fluoride | Propolis | −0.58 | 0.12 | 0.0001 * | −0.88 | −0.28 | |
| Acidulated phosphate fluoride | Propolis | −0.05 | 0.16 | 1.0000 | −0.46 | 0.37 | |
| Air test | Sodium fluoride | Acidulated phosphate fluoride | −0.50 | 0.12 | 0.0010 * | −0.82 | −0.18 |
| Sodium fluoride | Propolis | −0.87 | 0.13 | 0.0001 * | −1.20 | −0.54 | |
| Acidulated phosphate fluoride | Propolis | −0.37 | 0.16 | 0.0910 | −0.78 | 0.04 | |
| Groups | Sodium Fluoride_Tactile | Sodium Fluoride_Cold | Sodium Fluoride_Air | Acidulated Phosphate Fluoride_Tactile | Acidulated Phosphate Fluoride_Cold | Acidulated Phosphate Fluoride_Air | Propolis_Tactile | Propolis_Cold | Propolis_Air | |
|---|---|---|---|---|---|---|---|---|---|---|
| Pairs | p-Value | p-Value | p-Value | p-Value | p-Value | p-Value | p-Value | p-Value | p-Value | |
| Baseline | Immediate | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | 0.003 * | <0.001 * | <0.001 * | 0.019 * |
| 14th Day | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | 0.002 * | |
| 28th Day | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | |
| Immediate | 14th Day | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | 1.000 | <0.001 * | <0.001 * | 0.176 |
| 28th Day | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | 0.090 | <0.001 * | <0.001 * | 0.714 | |
| 14th Day | 28th Day | 0.003 * | <0.001 * | 0.033 * | <0.001 * | 0.027 * | 0.097 | <0.001 * | 0.368 | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlQahtani, S.M.; Nagate, R.R.; Al-Ahmari, M.M.M.; Magbol, M.A.; Gokhale, S.T.; Tikare, S.; Chaturvedi, S. Evaluation of Propolis Hydrogel for the Treatment of Dentinal Sensitivity: A Clinical Study. Gels 2023, 9, 483. https://doi.org/10.3390/gels9060483
AlQahtani SM, Nagate RR, Al-Ahmari MMM, Magbol MA, Gokhale ST, Tikare S, Chaturvedi S. Evaluation of Propolis Hydrogel for the Treatment of Dentinal Sensitivity: A Clinical Study. Gels. 2023; 9(6):483. https://doi.org/10.3390/gels9060483
Chicago/Turabian StyleAlQahtani, Saad Mohammed, Raghavendra Reddy Nagate, Manae Musa Musleh Al-Ahmari, Mohammad Al. Magbol, Shankar T. Gokhale, Shreyas Tikare, and Saurabh Chaturvedi. 2023. "Evaluation of Propolis Hydrogel for the Treatment of Dentinal Sensitivity: A Clinical Study" Gels 9, no. 6: 483. https://doi.org/10.3390/gels9060483