
Hydrogel Encapsulation of Genome-Engineered Stem Cells for Long-Term Self-Regulating Anti-Cytokine Therapy

 , , and
, , and 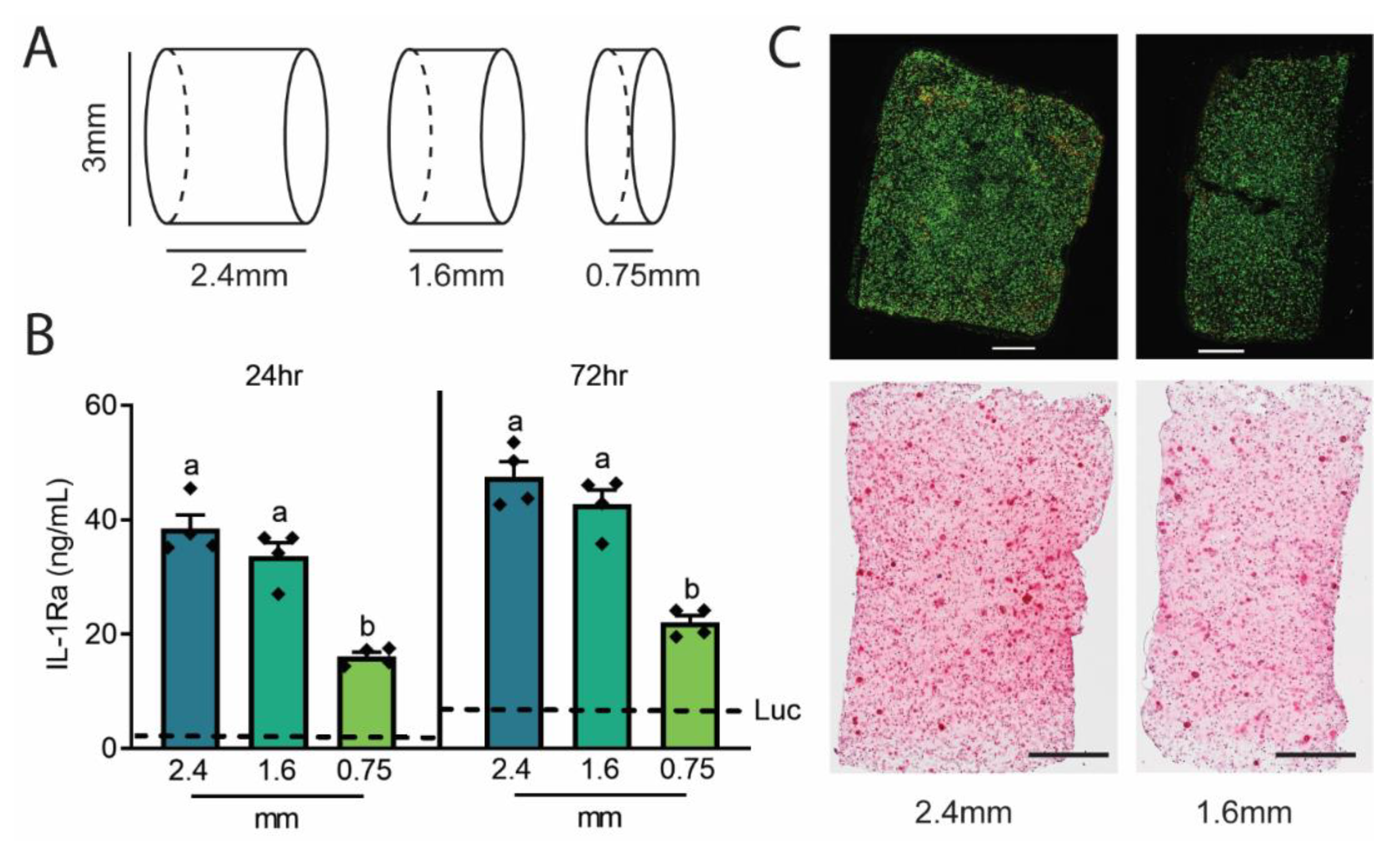{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Initial Agarose Construct Testing
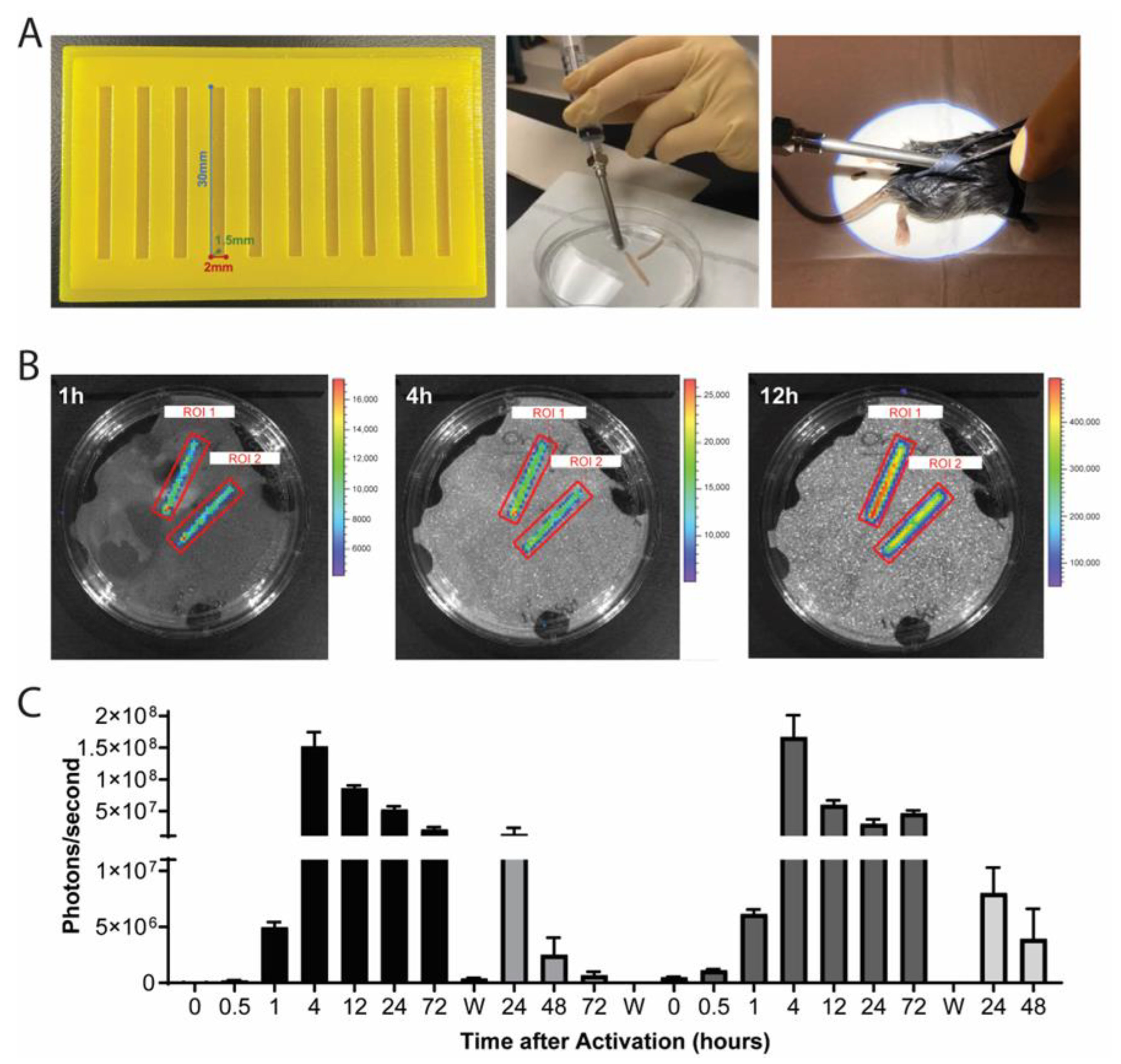
2.2. Translational Delivery Strategy Using 3D-Printed Molds and Wide Bore Needle Delivery
2.3. Agarose Rod Implants Demonstrate Long-Term Viability and Drug Delivery
2.4. Injectable Anti-Cytokine Therapy Mitigates Arthritis Outcomes in Mice Challenged with K/BxN STA
3. Discussion
Limitations and Future Work
4. Conclusions
5. Experimental Section/Methods
5.1. Cell Culture and Agarose Hydrogels
5.2. Quantitative Assessment of IL-1Ra
5.3. Cell Viability and Proteoglycan Staining
5.4. Bioluminescence Imaging
5.5. K/BxN Model of Inflammatory Arthritis
5.6. Pain and Behavioral Testing
5.7. Histology
5.8. Cytokine Bead Array Assay
5.9. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brunger, J.M.; Zutshi, A.; Willard, V.P.; Gersbach, C.A.; Guilak, F. Genome engineering of stem cells for autonomously regulated, closed-loop delivery of biologic drugs. Stem Cell Rep. 2017, 8, 1202–1213. [Google Scholar] [CrossRef] [Green Version]
- Ye, H.; Xie, M.; Xue, S.; Hamri, G.C.-E.; Yin, J.; Zulewski, H.; Fussenegger, M. Self-adjusting synthetic gene circuit for correcting insulin resistance. Nat. Biomed. Eng. 2016, 1, 5. [Google Scholar] [CrossRef] [Green Version]
- Joshi, N.; Yan, J.; Levy, S.; Bhagchandani, S.; Slaughter, K.V.; Sherman, N.E.; Amirault, J.; Wang, Y.; Riegel, L.; He, X.; et al. Towards an arthritis flare-responsive drug delivery system. Nat. Commun. 2018, 9, 1275. [Google Scholar] [CrossRef] [PubMed]
- Brunger, J.M.; Zutshi, A.; Willard, V.P.; Gersbach, C.A.; Guilak, F. CRISPR/Cas9 editing of murine induced pluripotent stem cells for engineering inflammation--resistant tissues. Arthritis Rheumatol. 2017, 69, 1111–1121. [Google Scholar] [CrossRef] [Green Version]
- Singh, N.; Li, C.I. Impact of rheumatoid arthritis and biologic and targeted synthetic disease modifying antirheumatic agents on cancer risk and recurrence. Curr. Opin. Rheumatol. 2021, 33, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.-R.; Collins, K.H.; Springer, L.E.; Pferdehirt, L.; Ross, A.K.; Wu, C.-L.; Moutos, F.T.; Harasymowicz, N.S.; Brunger, J.M.; Pham, C.T.N.; et al. A genome-engineered bioartificial implant for autoregulated anticytokine drug delivery. Sci. Adv. 2021, 7, eabj1414. [Google Scholar] [CrossRef]
- Moutos, F.T.; Glass, K.A.; Compton, S.A.; Ross, A.K.; Gersbach, C.A.; Guilak, F.; Estes, B.T. Anatomically shaped tissue-engineered cartilage with tunable and inducible anticytokine delivery for biological joint resurfacing. Proc. Natl. Acad. Sci. USA 2016, 113, E4513–E4522. [Google Scholar] [CrossRef] [Green Version]
- Brunger, J.M.; Huynh, N.P.T.; Guenther, C.M.; Perez-Pinera, P.; Moutos, F.T.; Sanchez-Adams, J.; Gersbach, C.A.; Guilak, F. Scaffold-mediated lentiviral transduction for functional tissue engineering of cartilage. Proc. Natl. Acad. Sci. USA 2014, 111, E798–E806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yazdi, M.K.; Taghizadeh, A.; Taghizadeh, M.; Stadler, F.J.; Farokhi, M.; Mottaghitalab, F.; Zarrintaj, P.; Ramsey, J.D.; Seidi, F.; Saeb, M.R.; et al. Agarose-based biomaterials for advanced drug delivery. J. Control. Release 2020, 326, 523–543. [Google Scholar] [CrossRef]
- Diekman, B.O.; Christoforou, N.; Willard, V.P.; Sun, H.; Sanchez-Adams, J.; Leong, K.W.; Guilak, F. Cartilage tissue engineering using differentiated and purified induced pluripotent stem cells. Proc. Natl. Acad. Sci. USA 2012, 109, 19172–19177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peppas, N.A.; Hilt, J.Z.; Khademhosseini, A.; Langer, R. Hydrogels in biology and medicine: From molecular principles to bionanotechnology. Adv. Mater. 2006, 18, 1345–1360. [Google Scholar] [CrossRef]
- Stefani, R.M.; Lee, A.; Tan, A.R.; Halder, S.S.; Hu, Y.; Guo, X.E.; Stoker, A.M.; Ateshian, G.A.; Marra, K.G.; Cook, J.; et al. Sustained low-dose dexamethasone delivery via a PLGA microsphere-embedded agarose implant for enhanced osteochondral repair. Acta Biomater. 2019, 102, 326–340. [Google Scholar] [CrossRef] [PubMed]
- Roach, B.L.; Kelmendi-Doko, A.; Balutis, E.C.; Marra, K.G.; Ateshian, G.A.; Hung, C.T. Dexamethasone release from within engineered cartilage as a chondroprotective strategy against interleukin-1α. Tissue Eng. Part A 2016, 22, 621–632. [Google Scholar] [CrossRef] [Green Version]
- Rizzo, F.; Kehr, N.S. Recent advances in injectable hydrogels for controlled and local drug delivery. Adv. Health Mater. 2020, 10, e2001341. [Google Scholar] [CrossRef]
- Kim, T.; Suh, J.; Kim, W.J. Polymeric aggregate--embodied hybrid nitric--oxide--scavenging and sequential drug--releasing hydrogel for combinatorial treatment of rheumatoid arthritis. Adv. Mater. 2021, 33, e2008793. [Google Scholar] [CrossRef] [PubMed]
- Mauck, R.; Yuan, X.; Tuan, R. Chondrogenic differentiation and functional maturation of bovine mesenchymal stem cells in long-term agarose culture. Osteoarthr. Cartil. 2006, 14, 179–189. [Google Scholar] [CrossRef] [Green Version]
- Adkar, S.S.; Brunger, J.M.; Willard, V.P.; Wu, C.-L.; Gersbach, C.A.; Guilak, F. Genome Engineering for personalized arthritis therapeutics. Trends Mol. Med. 2017, 23, 917–931. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-L.; Dicks, A.; Steward, N.; Tang, R.; Katz, D.B.; Choi, Y.-R.; Guilak, F. Single cell transcriptomic analysis of human pluripotent stem cell chondrogenesis. Nat. Commun. 2021, 12, 362. [Google Scholar] [CrossRef]
- Hung, C.T.; Mauck, R.L.; Wang, C.C.-B.; Lima, E.G.; Ateshian, G.A. A paradigm for functional tissue engineering of articular cartilage via applied physiologic deformational loading. Ann. Biomed. Eng. 2004, 32, 35–49. [Google Scholar] [CrossRef] [Green Version]
- Ng, K.W.; Ateshian, G.A.; Hung, C.T. Zonal chondrocytes seeded in a layered agarose hydrogel create engineered cartilage with depth-dependent cellular and mechanical inhomogeneity. Tissue Eng. Part A 2009, 15, 2315–2324. [Google Scholar] [CrossRef]
- Ng, K.; Kugler, L.; Doty, S.; Ateshian, G.; Hung, C. Scaffold degradation elevates the collagen content and dynamic compressive modulus in engineered articular cartilage. Osteoarthr. Cartil. 2009, 17, 220–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nims, R.J.; Cigan, A.D.; Albro, M.B.; Hung, C.T.; Ateshian, G.A. Synthesis rates and binding kinetics of matrix products in engineered cartilage constructs using chondrocyte-seeded agarose gels. J. Biomech. 2013, 47, 2165–2172. [Google Scholar] [CrossRef] [Green Version]
- Tan, A.R.; Hung, C.T. Concise review: Mesenchymal stem cells for functional cartilage tissue engineering: Taking cues from chondrocyte-based constructs. Stem Cells Transl. Med. 2017, 6, 1295–1303. [Google Scholar] [CrossRef]
- Estes, B.; Diekman, B.; Guilak, F. Monolayer cell expansion conditions affect the chondrogenic potential of adipose-derived stem cells. Biotechnol. Bioeng. 2008, 99, 986–995. [Google Scholar] [CrossRef] [Green Version]
- Leach, D.G.; Young, S.; Hartgerink, J.D. Advances in immunotherapy delivery from implantable and injectable biomaterials. Acta Biomater. 2019, 88, 15–31. [Google Scholar] [CrossRef]
- Christensen, A.D.; Haase, C.; Cook, A.; Hamilton, J.A. K/BxN Serum-Transfer Arthritis as a Model for Human Inflammatory Arthritis. Front. Immunol. 2016, 7, 213. [Google Scholar] [CrossRef] [Green Version]
- Nims, R.J.; Pferdehirt, L.; Ho, N.B.; Savadipour, A.; Lorentz, J.; Sohi, S.; Kassab, J.; Ross, A.K.; O’Conor, C.J.; Liedtke, W.B.; et al. A synthetic mechanogenetic gene circuit for autonomous drug delivery in engineered tissues. Sci. Adv. 2021, 7, eabd9858. [Google Scholar] [CrossRef]
- Chen, W.; Yung, B.C.; Qian, Z.; Chen, X. Improving long-term subcutaneous drug delivery by regulating material-bioenvironment interaction. Adv. Drug Deliv. Rev. 2018, 127, 20–34. [Google Scholar] [CrossRef] [PubMed]
- Benhabbour, S.R.; Kovarova, M.; Jones, C.; Copeland, D.J.; Shrivastava, R.; Swanson, M.D.; Sykes, C.; Ho, P.T.; Cottrell, M.L.; Sridharan, A.; et al. Ultra-long-acting tunable biodegradable and removable controlled release implants for drug delivery. Nat. Commun. 2019, 10, 4324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nash, A.M.; Jarvis, M.I.; Aghlara-Fotovat, S.; Mukherjee, S.; Hernandez, A.; Hecht, A.D.; Rios, P.D.; Ghani, S.; Joshi, I.; Isa, D.; et al. Clinically translatable cytokine delivery platform for eradication of intraperitoneal tumors. Sci. Adv. 2022, 8, eabm1032. [Google Scholar] [CrossRef]
- Johnstone, B.; Hering, T.M.; Caplan, A.; Goldberg, V.M.; Yoo, J.U. In vitro chondrogenesis of bone marrow-derived mesenchymal progenitor cells. Exp. Cell Res. 1998, 238, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Korganow, A.-S.; Ji, H.; Mangialaio, S.; Duchatelle, V.; Pelanda, R.; Martin, T.; Degott, C.; Kikutani, H.; Rajewsky, K.; Pasquali, J.-L.; et al. From systemic T cell self-reactivity to organ-specific autoimmune disease via immunoglobulins. Immunity 1999, 10, 451–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kouskoff, V.; Korganow, A.-S.; Duchatelle, V.; Degott, C.; Benoist, C.; Mathis, D. Organ-specific disease provoked by systemic autoimmunity. Cell 1996, 87, 811–822. [Google Scholar] [CrossRef] [Green Version]
- Kyburz, D.; Corr, M. The KRN mouse model of inflammatory arthritis. Springer Semin. Immunopathol. 2003, 25, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.-F.; Chan, H.W.; Wickline, S.A.; Lanza, G.M.; Pham, C.T.N. αvβ3–Targeted nanotherapy suppresses inflammatory arthritis in mice. FASEB J. 2009, 23, 2978–2985. [Google Scholar] [CrossRef] [Green Version]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Collins, K.H.; Pferdehirt, L.; Saleh, L.S.; Savadipour, A.; Springer, L.E.; Lenz, K.L.; Thompson, D.M., Jr.; Oswald, S.J.; Pham, C.T.N.; Guilak, F. Hydrogel Encapsulation of Genome-Engineered Stem Cells for Long-Term Self-Regulating Anti-Cytokine Therapy. Gels 2023, 9, 169. https://doi.org/10.3390/gels9020169
Collins KH, Pferdehirt L, Saleh LS, Savadipour A, Springer LE, Lenz KL, Thompson DM Jr., Oswald SJ, Pham CTN, Guilak F. Hydrogel Encapsulation of Genome-Engineered Stem Cells for Long-Term Self-Regulating Anti-Cytokine Therapy. Gels. 2023; 9(2):169. https://doi.org/10.3390/gels9020169
Chicago/Turabian StyleCollins, Kelsey H., Lara Pferdehirt, Leila S. Saleh, Alireza Savadipour, Luke E. Springer, Kristin L. Lenz, Dominic M. Thompson, Jr., Sara J. Oswald, Christine T. N. Pham, and Farshid Guilak. 2023. "Hydrogel Encapsulation of Genome-Engineered Stem Cells for Long-Term Self-Regulating Anti-Cytokine Therapy" Gels 9, no. 2: 169. https://doi.org/10.3390/gels9020169