
An Overview on Candida auris in Healthcare Settings
 ,
,
Abstract
:1. Introduction
2. Characteristics of the Microorganism
3. Infections and Risk Factors
4. Diagnosis
5. Therapy and Antifungal Resistance
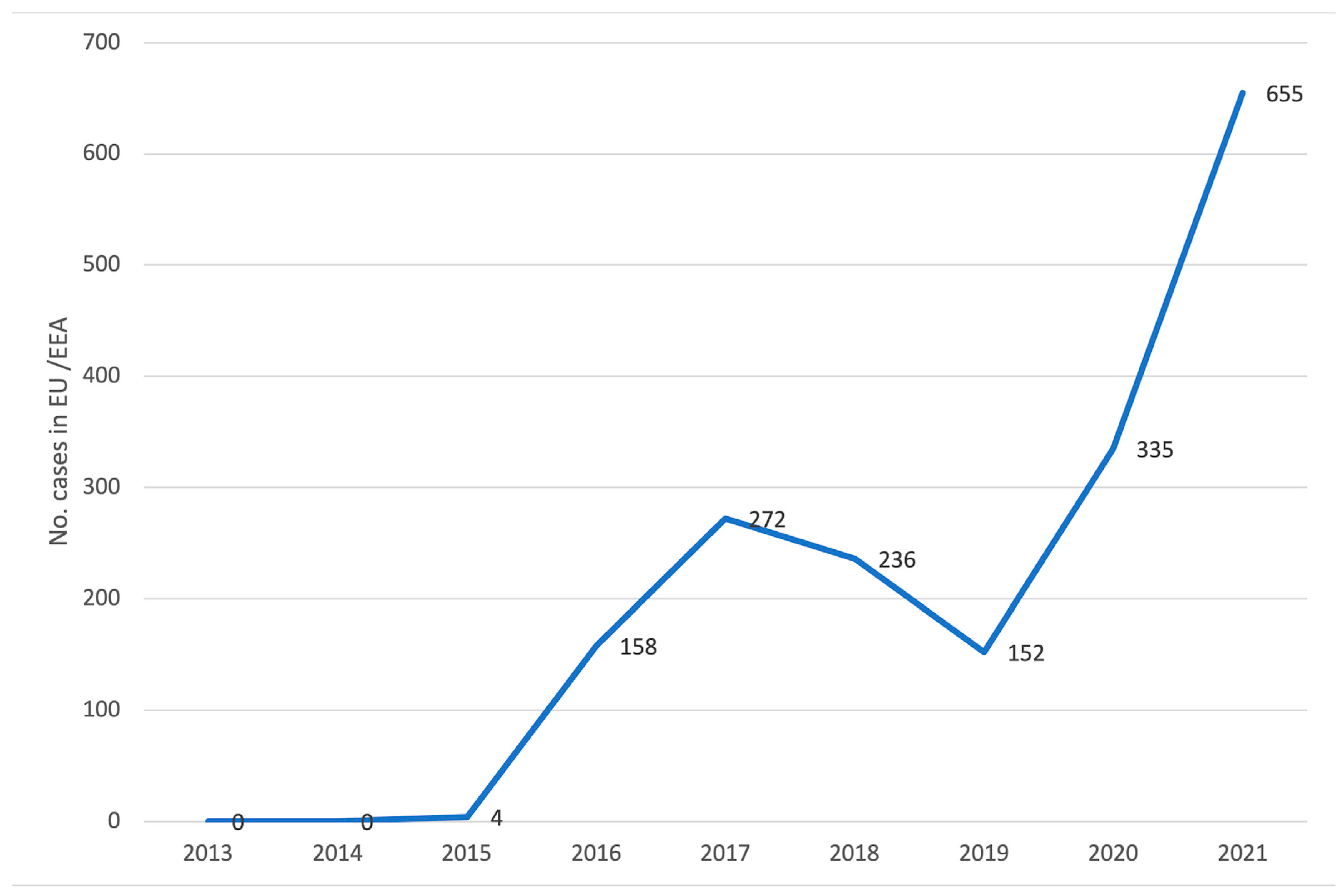
6. Epidemiology
7. Prevention and Control Measures
8. Candida auris Surveillance Measures
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- MSD Manual. Candidiasis Invasive. Available online: https://www.msdmanuals.com/professional/infectious-diseases/fungi/candidiasis-invasive (accessed on 23 February 2023).
- Sabino, R.; Veríssimo, C.; Pereira, Á.A.; Antunes, F. Candida auris, an Agent of Hospital-Associated Outbreaks: Which Challenging Issues Do We Need to Have in Mind? Microorganisms 2020, 8, 181. [Google Scholar] [CrossRef] [PubMed]
- Du, H.; Bing, J.; Hu, T.; Ennis, C.L.; Nobile, C.J.; Huang, G. Candida auris: Epidemiology, biology, antifungal resistance, and virulence. PLoS Pathog. 2020, 16, e1008921. [Google Scholar] [CrossRef]
- Theodoropoulos, N.M.; Bolstorff, B.; Bozorgzadeh, A.; Brandeburg, C.; Cumming, M.; Daly, J.S.; Ellison, R.T., 3rd; Forsberg, K.; Gade, L.; Gibson, L.; et al. Candida auris outbreak involving liver transplant recipients in a surgical intensive care unit. Am. J. Transpl. 2020, 20, 3673–3679. [Google Scholar] [CrossRef] [PubMed]
- Logan, C.; Martin-Loeches, I.; Bicanic, T. Invasive candidiasis in critical care: Challenges and future directions. Intensive Care Med. 2020, 46, 2001–2014. [Google Scholar] [CrossRef]
- Fernandes, L.; Ribeiro, R.; Henriques, M.; Rodrigues, M.E. Candida auris, a singular emergent pathogenic yeast: Its resistance and new therapeutic alternatives. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 1371–1385. [Google Scholar] [CrossRef] [PubMed]
- Mohsin, J.; Weerakoon, S.; Ahmed, S.; Puts, Y.; Al Balushi, Z.; Meis, J.F.; Al-Hatmi, A.M.S. A Cluster of Candida auris Blood Stream Infections in a Tertiary Care Hospital in Oman from 2016 to 2019. Antibiotics 2020, 9, 638. [Google Scholar] [CrossRef]
- Casadevall, A.; Kontoyiannis, D.P.; Robert, V. Environmental Candida auris and the Global Warming Emergence Hypothesis. mBio 2021, 12, e00360-21. [Google Scholar] [CrossRef]
- Watkins, R.R.; Gowen, R.; Lionakis, M.S.; Ghannoum, M. Update on the Pathogenesis, Virulence, and Treatment of Candida auris. Pathog. Immun. 2022, 7, 46–65. [Google Scholar] [CrossRef]
- Escandón, P. Novel Environmental Niches for Candida auris: Isolation from a Coastal Habitat in Colombia. J. Fungi 2022, 8, 748. [Google Scholar] [CrossRef]
- Satoh, K.; Makimura, K.; Hasumi, Y.; Nishiyama, Y.; Uchida, K.; Yamaguchi, H. Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol. Immunol. 2009, 53, 41–44. [Google Scholar] [CrossRef]
- Lockhart, S.R.; Etienne, K.A.; Vallabhanni, S.; Farooqi, J.; Chowdhary, A.; Govender, N.P.; Colombo, A.L.; Calvo, B.; Cuomo, C.A.; Desjardins, C.A.; et al. Simultaneous emergence of multidrug-resistant Candida auris on 3 continents confirmed by whole-genome sequencing and epidemiological analyses. Clin. Infect. Dis. 2017, 64, 134–140. [Google Scholar] [CrossRef]
- Chow, N.A.; de Groot, T.; Badali, H.; Abastabar, M.; Chiller, T.M.; Meis, J.F. Potential Fifth Clade of Candida auris, Iran, 2018. Emerg. Infect. Dis. 2019, 25, 1780–1781. [Google Scholar] [CrossRef]
- Proctor, D.M.; Dangana, T.; Sexton, D.J.; Fukuda, C.; Yelin, R.D.; Stanley, M.; Bell, P.B.; Baskaran, S.; Deming, C.; Chen, Q.; et al. Integrated genomic, epidemiologic investigation of Candida auris skin colonization in a skilled nursing facility. Nat. Med. 2021, 27, 1401–1409. [Google Scholar] [CrossRef] [PubMed]
- Tharp, B.; Zheng, R.; Bryak, G.; Litvintseva, A.P.; Hayden, M.K.; Chowdhary, A.; Thangamani, S. Role of Microbiota in the Skin Colonization of Candida auris. mSphere 2023, 8, e0062322. [Google Scholar] [CrossRef]
- Forsberg, K.; Woodworth, K.; Walters, M.; Berkow, E.L.; Jackson, B.; Chiller, T.; Vallabhaneni, S. Candida auris: The recent emergence of a multidrug-resistant fungal pathogen. Med. Mycol. 2019, 57, 1–12. [Google Scholar] [CrossRef]
- Sears, D.; Schwartz, B.S. Candida auris: An emerging multidrug-resistant pathogen. Int. J. Infect. Dis. 2017, 63, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Vena, A.; Meroi, M.; Cardozo, C.; Cuervo, G.; Giacobbe, D.R.; Salavert, M.; Merino, P.; Gioia, F.; Fernández-Ruiz, P.; et al. Factors associated with the development of septic shock in patients with candidemia: A post hoc analysis from two prospective cohorts. Crit. Care 2020, 24, 117. [Google Scholar] [CrossRef]
- Hu, S.; Zhu, F.; Jiang, W.; Wang, Y.; Quan, Y.; Zhang, G.; Gu, F.; Yang, Y. Retrospective Analysis of the Clinical Characteristics of Candida auris Infection Worldwide From 2009 to 2020. Front. Microbiol. 2021, 12, 658329. [Google Scholar] [CrossRef] [PubMed]
- Ademe, M.; Girma, F. Candida auris: From Multidrug Resistance to Pan-Resistant Strains. Infect. Drug Resist. 2020, 13, 1287–1294. [Google Scholar] [CrossRef] [PubMed]
- Kumar, J.; Eilertson, B.; Cadnum, J.L.; Whitlow, C.S.; Jencson, A.L.; Safdar, N.; Krein, S.L.; Tanner, W.D.; JeanMarie Mayer, J.; Samore, M.H.; et al. Environmental Contamination with Candida Species in Multiple Hospitals Including a Tertiary Care Hospital with a Candida auris Outbreak. Pathog. Immun. 2019, 4, 260–270. [Google Scholar] [CrossRef] [PubMed]
- Cristina, M.L.; Spagnolo, A.M.; Orlando, P.; Perdelli, F. The role of the environment in the spread of emerging pathogens in at-risk hospital wards. Rev. Res. Med. Microbiol. 2013, 24, 104–112. [Google Scholar] [CrossRef]
- Piedrahita, C.T.; Cadnum, J.L.; Jencson, A.L.; Shaikh, A.A.; Ghannoum, M.A.; Donskey, C.J. Environmental Surfaces in Healthcare Facilities are a Potential Source for Transmission of Candida auris and Other Candida Species. Infect. Control Hosp. Epidemiol. 2017, 38, 1107–1109. [Google Scholar] [CrossRef] [PubMed]
- Vallabhaneni, S.; Kallen, A.; Tsay, S.; Chow, N.; Welsh, R.; Kerins, J.; Kemble, S.K.; Pacilli, M.; Black, S.R.; Landon, E.; et al. Investigation of the First Seven Reported Cases of Candida auris, a Globally Emerging Invasive, Multidrug-Resistant Fungus-United States, May 2013–August 2016. Am. J. Transpl. 2017, 17, 296–299. [Google Scholar] [CrossRef] [PubMed]
- Schelenz, S.; Hagen, F.; Rhodes, J.L.; Abdolrasouli, A.; Chowdhary, A.; Hall, A.; Ryan, L.; Shackleton, J.; Trimlett, R.; Meis, J.F.; et al. First hospital outbreak of the globally emerging Candida auris in a European hospital. Antimicrob. Resist. Infect. Control 2016, 5, 35. [Google Scholar] [CrossRef] [PubMed]
- Eyre, D.W.; Sheppard, A.E.; Madder, H.; Moir, I.; Moroney, R.; Quan, T.P.; Griffiths, D.; George, S.; Butcher, L.; Morgan, M.; et al. A Candida auris Outbreak and Its Control in an Intensive Care Setting. N. Engl. J. Med. 2018, 379, 1322–1331. [Google Scholar] [CrossRef] [PubMed]
- Welsh, R.M.; Bentz, M.L.; Shams, A.; Houston, H.; Lyons, A.; Rose, L.J.; Litvintseva, A.P. Survival, Persistence, and Isolation of the Emerging Multidrug-Resistant Pathogenic Yeast Candida auris on a Plastic Health Care Surface. J. Clin. Microbiol. 2017, 55, 2996–3005. [Google Scholar] [CrossRef] [PubMed]
- Ferrer Gómez, C.; Solís Albamonte, P.; Delgado Navarro, C.; Salvador García, C.; Tormo Palop, N.; Andrés Ibáñez, J.A. Analysis of Candida auris candidemia cases in an Intensive Care Unit of a tertiary hospital. Rev. Esp. Anestesiol. Reanim. 2021, 68, 431–436. [Google Scholar] [CrossRef]
- Kean, R.; Sherry, L.; Townsend, E.; McKloud, E.; Short, B.; Akinbobola, A.; Mackay, W.G.; Williams, C.; Jones, B.L.; Ramage, G. Surface disinfection challenges for Candida auris: An in-vitro study. J. Hosp. Infect. 2018, 98, 433–436. [Google Scholar] [CrossRef]
- Sherry, L.; Ramage, G.; Kean, R.; Borman, A.; Johnson, E.M.; Richardson, M.D.; Rautemaa-Richardson, R. Biofilm-Forming Capability of Highly Virulent, Multidrug-Resistant Candida auris. Emerg. Infect. Dis. 2017, 23, 328–331. [Google Scholar] [CrossRef]
- Centers of Diseases Control and Prevention. Available online: https://www.cdc.gov/fungal/candida-auris/candida-auris-qanda.html (accessed on 13 February 2023).
- Centers of Diseases Control and Prevention. Available online: https://www.cdc.gov/fungal/candida-auris/pdf/Testing-algorithm_by-Method_508.pdf (accessed on 20 February 2023).
- Centers of Diseases Control and Prevention. Available online: https://www.cdc.gov/fungal/candida-auris/c-auris-treatment.html (accessed on 13 February 2023).
- European Centre for Disease Prevention and Control. Candida auris Outbreak in Healthcare in Northern Italy, 2019–2021; ECDC: Stockholm, Sweden, 2022.
- Sikora, A.; Hashmi, M.F.; Zahra, F. Candida auris. Available online: https://www.ncbi.nlm.nih.gov/books/NBK563297/ (accessed on 11 July 2023).
- Fakhim, H.; Chowdhary, A.; Prakash, A.; Vaezi, A.; Dannaoui, E.; Meis, J.F.; Badali, H. In Vitro Interactions of Echinocandins with Triazoles against Multidrug-Resistant Candida auris. Antimicrob. Agents Chemother. 2017, 61, e01056-17. [Google Scholar] [CrossRef]
- Centers of Diseases Control and Prevention. Antifungal Susceptibility Testing and Interpretation. Available online: https://www.cdc.gov/fungal/candida-auris/c-auris-antifungal.html (accessed on 11 July 2023).
- Chaabane, F.; Graf, A.; Jequier, L.; Coste, A.T. Review on Antifungal Resistance Mechanisms in the Emerging Pathogen Candida auris. Front. Microbiol. 2019, 10, 2788. [Google Scholar] [CrossRef] [PubMed]
- Raschig, M.; Bernardo Ramírez-Zavala, B.; Wiest, J.; Saedtler, M.; Gutmann, M.; Holzgrabe, U.; Joachim Morschhäuser, J.; Meinel, L. Azobenzene derivatives with activity against drug-resistant Candida albicans and Candida auris. Arch. Pharm. 2023, 356, e2200463. [Google Scholar] [CrossRef]
- Hetta, H.F.; Ramadan, Y.N.; Al-Kadmy, I.M.S.; Ellah, N.H.A.; Shbibe, L.; Battah, B. Nanotechnology-Based Strategies to Combat Multidrug-Resistant Candida auris Infections. Pathogens 2023, 12, 1033. [Google Scholar] [CrossRef] [PubMed]
- Marena, G.D.; Carvalho, G.C.; Dos Santos Ramos, M.A.; Chorilli, M.; Bauab, T.M. Anti-Candida auris activity in vitro and in vivo of micafungin loaded nanoemulsions. Med. Mycol. 2023, 61, myac090. [Google Scholar] [CrossRef] [PubMed]
- Rosato, R.; Napoli, E.; Granata, G.; Di Vito, M.; Garzoli, S.; Geraci, C.; Rizzo, S.; Torelli, R.; Sanguinetti, M.; Bugli, F. Study of the Chemical Profile and Anti-Fungal Activity against Candida auris of Cinnamomum cassia Essential Oil and of Its Nano-Formulations Based on Polycaprolactone. Plants 2023, 12, 358. [Google Scholar] [CrossRef]
- Xin, H.; Rosario-Colon, J.A.; Eberle, K. Novel Intravenous Immunoglobulin Therapy for the Prevention and Treatment of Candida auris and Candida albicans Disseminated Candidiasis. mSphere 2023, 8, e0058422. [Google Scholar] [CrossRef]
- Bongomin, F.; Gago, S.; Oladele, R.O.; Denning, D.W. Global and Multi-National Prevalence of Fungal Diseases-Estimate Precision. J. Fungi 2017, 3, 57. [Google Scholar] [CrossRef]
- Kohlenberg, A.; Monnet, D.L.; Plachouras, D.; Candida auris Survey Collaborative Group. Increasing number of cases and outbreaks caused by Candida auris in the EU/EEA, 2020 to 2021. Eurosurveillance 2022, 27, 2200846. [Google Scholar] [CrossRef]
- Istituto Superiore di Sanità. EpiCentro. Candida auris. Available online: https://www.epicentro.iss.it/candida-auris/ (accessed on 26 February 2023).
- Berrio, I.; Caceres, D.H.; Coronell, R.W.; Salcedo, S.; Mora, L.; Marin, A.; Varón, C.; Lockhart, S.R.; Escandón, P.; Berkow, E.L.; et al. Bloodstream Infections with Candida auris Among Children in Colombia: Clinical Characteristics and Outcomes of 34 Cases. J. Pediatr. Infect. Dis. Soc. 2021, 10, 151–154. [Google Scholar] [CrossRef]
- Ortiz-Roa, C.; Valderrama-Rios, M.C.; Sierra-Umaña, S.F.; Rodríguez, J.Y.; Muñetón-López, G.A.; Solórzano-Ramos, C.A.; Escandón, P.; Alvarez-Moreno, C.A.; Cortés, J.A. Mortality Caused by Candida auris Bloodstream Infections in Comparison with Other Candida Species, a Multicentre Retrospective Cohort. J. Fungi 2023, 9, 715. [Google Scholar] [CrossRef]
- Centers of Diseases Control and Prevention. Available online: http://www.cdc.gov/hicpac/pdf/isolation/Isolation2007.pdf (accessed on 13 February 2023).
- Cadnum, J.L.; Shaikh, A.A.; Piedrahita, C.T.; Sankar, T.; Jencson, A.L.; Larkin, E.L.; Ghannoum, M.A.; Donskey, C.J. Effectiveness of Disinfectants Against Candida auris and Other Candida Species. Infect. Control Hosp. Epidemiol. 2017, 38, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Biswal, M.; Rudramurthy, S.M.; Jain, N.; Shamanth, A.S.; Sharma, D.; Jain, K.; Yaddanapudi, L.N.; Chakrabarti, A. Controlling a possible outbreak of Candida auris infection: Lessons learnt from multiple interventions. J. Hosp. Infect. 2017, 97, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Centers of Diseases Control and Prevention. Available online: https://www.cdc.gov/fungal/candida-auris/c-auris-surveillance.html (accessed on 13 February 2023).
- Centers of Diseases Control and Prevention. Available online: https://www.cdc.gov/fungal/candida-auris/c-auris-screening.html (accessed on 13 February 2023).
- Sticchi, C.; Alberti, M.; Artioli, S.; Assensi, M.; Baldelli, I.; Battistini, A.; Boni, S.; Cassola, G.; Castagnola, E.; Cattaneo, M.; et al. Regional point prevalence study of healthcare-associated infections and antimicrobial use in acute care hospitals in Liguria, Italy. J. Hosp. Infect. 2017, 99, 8–16. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Identification Method | Database/Software, If Applicable | C. auris Is Confirmed If Initial Identification Is C. auris | C. auris Is Possible If the Following Initial Identifications Are Given. Further Work-Up Is Needed to Determine If the Isolate Is C. auris |
|---|---|---|---|
| Bruker Biotyper MALDI-TOF | RUO libraries (v2014 [5627] and more recent) | Yes | n/a |
| CA System library (vClaim 4) | Yes | n/a | |
| bioMérieux VITEK MS MALDI-TOF | RUO library (with Saramis v4.14 database and Saccharomycetaceae update) | Yes | n/a |
| IVD library (v3.2) | Yes | n/a | |
| Earlier than IVD libraries (v3.2) | n/a | C. haemulonii C. lusitaniae No identification | |
| VITEK 2 YST | Software version 8.01 * | Yes | C. haemulonii C. duobushaemulonii Candida spp. not identified |
| Earlier than version 8.01 | n/a | C. haemulonii C. duobushaemulonii Candida spp. not identified | |
| API 20C | n/a | Rhodotorula glutinis (without characteristic red color) C. sake Candida spp. not identified | |
| API ID 32C | n/a | C. intermedia C. sake Saccharomyces kluyveri | |
| BD Phoenix | n/a | C. catenulata C. haemulonii Candida spp. not identified | |
| MicroScan | n/a | C. lusitaniae ** C. guilliermondii ** C. parapsilosis ** C. famata Candida spp. not identified | |
| RapID Yeast Plus | n/a | C. parapsilosis ** Candida spp. not identified | |
| GenMark ePlex BCID-FP Panel | Yes | n/a |
| Year * | No of Cases | Duration (Weeks) | Inter-Facility Transmission | Ongoing at Time of Survey |
|---|---|---|---|---|
| 2019 | 214 | 149 | Yes | Yes |
| 2020 | 50 | 80 | Yes | Yes |
| 2020 | 15 | 44.5 | Yes | No |
| 2020 | 11 | 49 | No | No |
| 2021 | 10 | 5 | Yes | No |
| 2021 | 5 | 28 | Yes | Yes |
| 2021 | 4 | 3.5 | Yes | No |
| 2021 | 4 | 4 | No | No |
| 2021 | 3 | 4 | Yes | No |
| 2021 | 3 | 11 | No | No |
| 2021 | 2 | 8 | No | No |
| 2021 | 2 | 8 | No | No |
| 2021 | 2 | 39 | Yes | No |
| 2021 | 2 | 9 | No | No |
| Total | 327 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cristina, M.L.; Spagnolo, A.M.; Sartini, M.; Carbone, A.; Oliva, M.; Schinca, E.; Boni, S.; Pontali, E. An Overview on Candida auris in Healthcare Settings. J. Fungi 2023, 9, 913. https://doi.org/10.3390/jof9090913
Cristina ML, Spagnolo AM, Sartini M, Carbone A, Oliva M, Schinca E, Boni S, Pontali E. An Overview on Candida auris in Healthcare Settings. Journal of Fungi. 2023; 9(9):913. https://doi.org/10.3390/jof9090913
Chicago/Turabian StyleCristina, Maria Luisa, Anna Maria Spagnolo, Marina Sartini, Alessio Carbone, Martino Oliva, Elisa Schinca, Silvia Boni, and Emanuele Pontali. 2023. "An Overview on Candida auris in Healthcare Settings" Journal of Fungi 9, no. 9: 913. https://doi.org/10.3390/jof9090913