
Epidemiology of Mucormycosis in Greece; Results from a Nationwide Prospective Survey and Published Case Reports
 , , , ,
, , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Case Lists
2.1.1. Prospective Study
2.1.2. Published Case Reports
2.2. Incidence
2.3. Laboratory Diagnosis
2.4. Statistical Analysis
3. Results
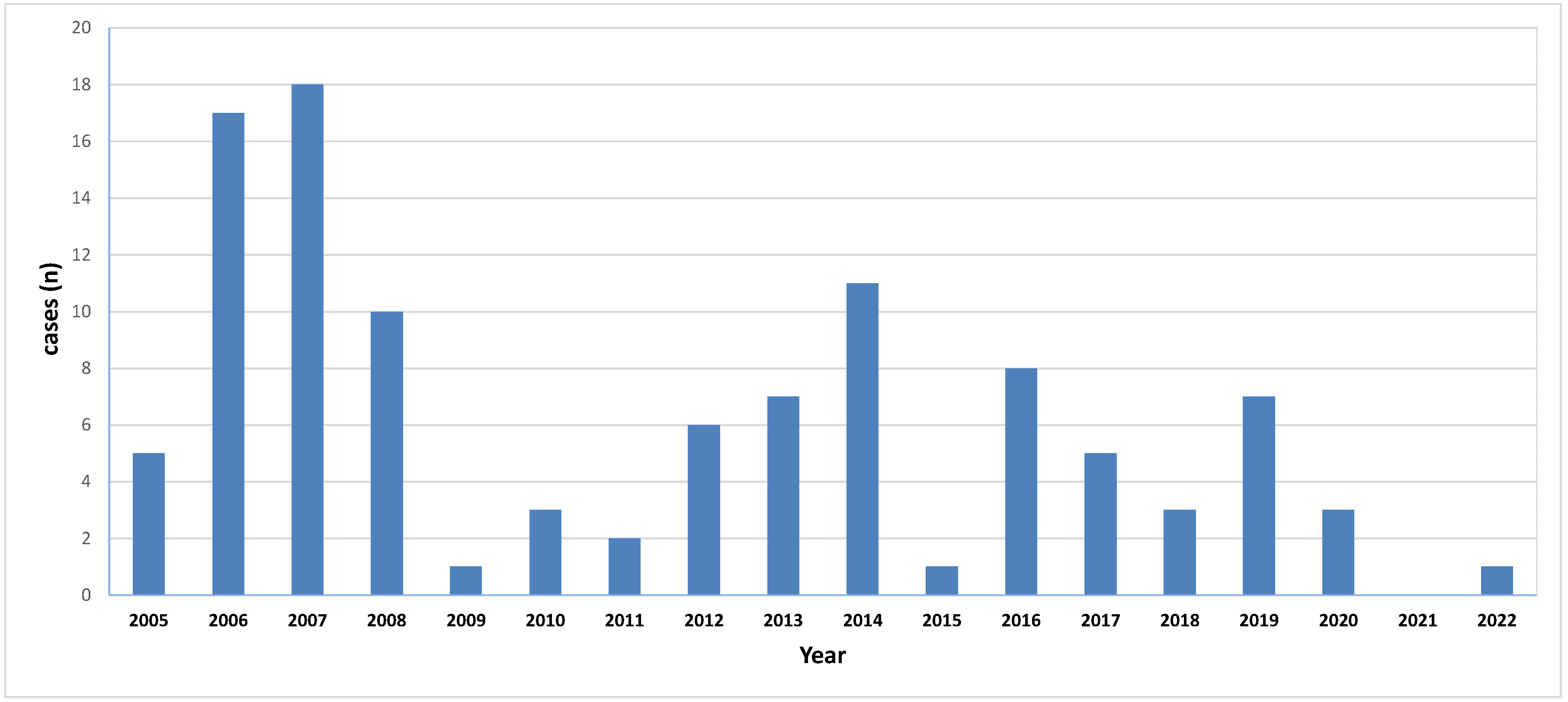
3.1. Demographic Data, Incidence
3.2. Prospective Study
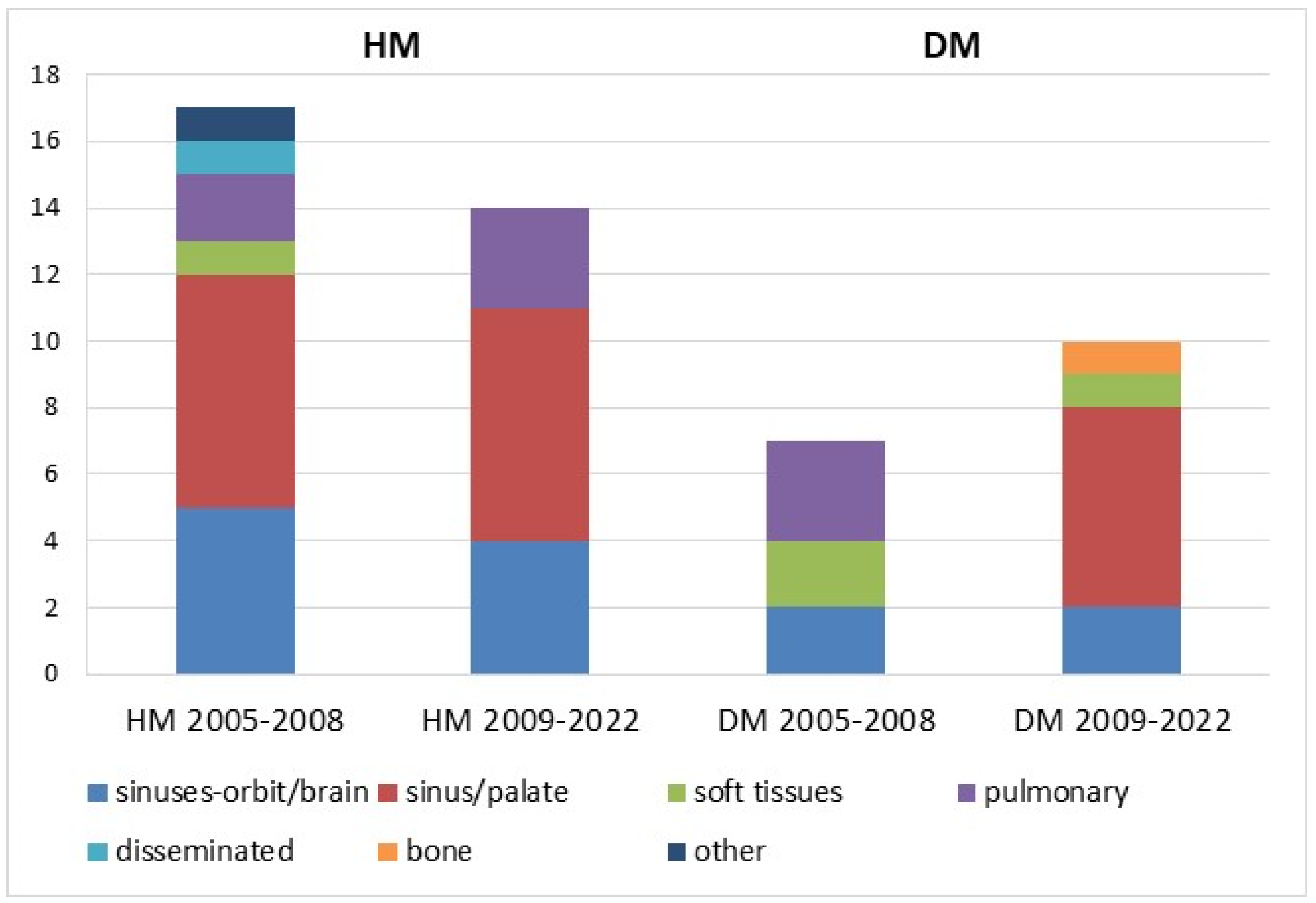
3.2.1. Localisation/Clinical Forms
3.2.2. Underlying Conditions
3.2.3. Laboratory Diagnosis
3.2.4. Infectious Agents
3.2.5. Therapy
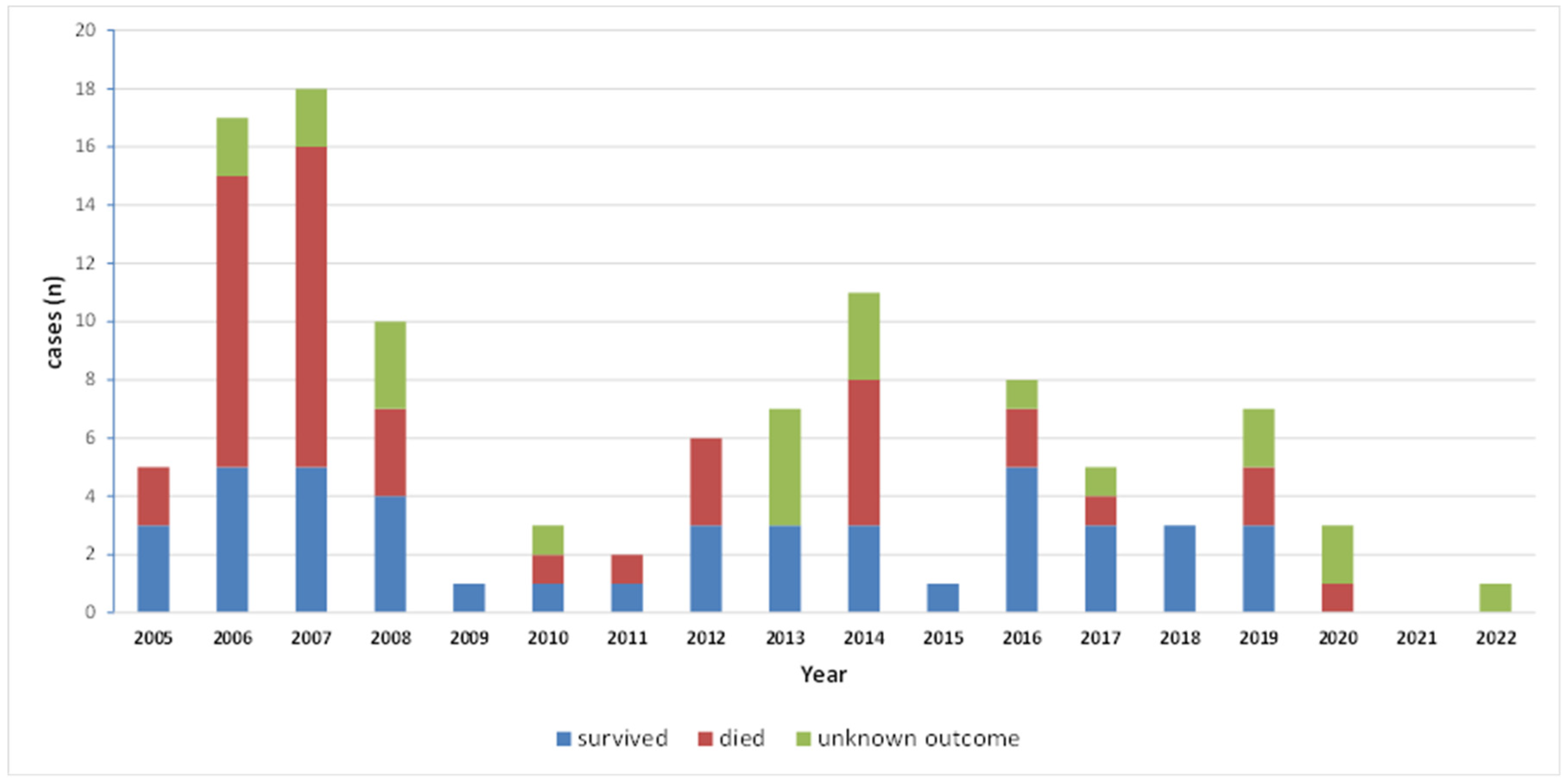
3.2.6. Outcome
3.3. Published Case Reports
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ibrahim, A.S.; Spellberg, B.; Walsh, T.J.; Kontoyiannis, D.P. Pathogenesis of Mucormycosis. Clin. Infect. Dis. 2012, 54 (Suppl. S1), S16–S22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoenigl, M.; Seidel, D.; Sprute, R.; Cunha, C.; Oliverio, M.; Goldman, G.H.; Ibrahim, A.S.; Carvalho, A. COVID-19-associated fungal infections. Nat. Microbiol. 2022, 7, 1127–1140. [Google Scholar] [CrossRef] [PubMed]
- Skiada, A.; Pavleas, I.; Drogari-Apiranthitou, M. Epidemiology and Diagnosis of Mucormycosis: An Update. J. Fungi 2020, 6, 265. [Google Scholar] [CrossRef] [PubMed]
- Skiada, A.; Drogari-Apiranthitou, M.; Pavleas, I.; Daikou, E.; Petrikkos, G. Global Cutaneous Mucormycosis: A Systematic Review. J. Fungi 2022, 8, 194. [Google Scholar] [CrossRef]
- Petrikkos, G.; Skiada, A.; Sambatakou, H.; Toskas, A.; Vaiopoulos, G.; Giannopoulou, M.; Katsilambros, N. Mucormycosis: Ten-Year Experience at a Tertiary-Care Center in Greece. Eur. J. Clin. Microbiol. Infect. Dis. 2003, 22, 753–756. [Google Scholar] [CrossRef]
- Zygomyco.Net, the Official Site of the ECMM/ISHAM Working Group on Zygomycosis. Available online: https://www.zygomyco.net (accessed on 30 January 2023).
- Cornely, O.A.; Alastruey-Izquierdo, A.; Arenz, D.; Chen, S.C.A.; Dannaoui, E.; Hochhegger, B.; Hoenigl, M.; Jensen, H.E.; Lagrou, K.; Lewis, R.E.; et al. Global guideline for the diagnosis and management of mucormycosis: An initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect. Dis. 2019, 19, e405–e421. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.; Verweij, P.; Clancy, C.; Wingard, J.; Lockhart, S.; Groll, A.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Kefala-Agoropoulou, K.; Farmaki, E.; Tsiouris, J.; Roilides, E.; Velegraki, A. Cutaneous zygomycosis in an infant with Pearson syndrome. Pediatr. Blood Cancer 2008, 50, 939–940. [Google Scholar] [CrossRef]
- Vyzantiadis, T.A.; Kioumi, A.; Papadakis, E.; Braimi, M.; Dermitzakis, E.; Tsitouridis, I.; Antoniadis, A. Rhino-cerebral zygomycosis resistant to antimycotic treatment: A case report. Mycoses 2009, 52, 87–90. [Google Scholar] [CrossRef]
- Nicolatou-Galitis, O.; Sachanas, S.; Drogari-Apiranthitou, M.; Moschogiannis, M.; Galiti, D.; Yiakoumis, X.; Rontogianni, D.; Yiotakis, I.E.; Petrikkos, G.L.; Pangalis, G.A. Mucormycosis presenting with dental pain and palatal ulcer in a patient with chronic myelomonocytic leukaemia: Case report and literature review. JMM Case Rep. 2015, 2, e000014. [Google Scholar] [CrossRef]
- Gkegkes, I.D.; Kotrogiannis, I.; Konstantara, F.; Karetsou, A.; Tsiplakou, S.; Fotiou, E.; Stamopoulou, S.; Papazacharias, C.; Paraskevopoulos, I.A. Cutaneous Mucormycosis by Saksenaea vasiformis: An Unusual Case Report and Review of Literature. Mycopathologia 2019, 184, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Mamali, V.; Koutserimpas, C.; Zarkotou, O.; Vrioni, G.; Samonis, G. Isolated Cerebral Mucormycosis Caused by Lichtheimia Species in a Polytrauma Patient. Diagnostics 2022, 12, 358. [Google Scholar] [CrossRef] [PubMed]
- Mamali, V.; Koutserimpas, C.; Manoloudaki, K.; Zarkotou, O.; Samonis, G.; Vrioni, G. Necrotizing Skin and Soft Tissue Infection Due to Syncephalastrum Species and Fusarium solani Species Complex Following Open Tibia Fracture. Diagnostics 2022, 12, 1163. [Google Scholar] [CrossRef]
- Hellenic Statistical Authority. Available online: https://www.statistics.gr/en/statistics/-/publication/SPO18/ (accessed on 30 January 2023).
- Bialek, R.; Konrad, F.; Kern, J.; Aepinus, C.; Cecenas, L.; Gonzalez, G.M.; Just-Nübling, G.; Willinger, B.; Presterl, E.; Lass-Flörl, C.; et al. PCR based identification and discrimination of agents of mucormycosis and aspergillosis in paraffin wax embedded tissue. J. Clin. Pathol. 2005, 58, 1180–1184. [Google Scholar] [CrossRef]
- Drogari-Apiranthitou, M.; Panayiotides, I.; Galani, I.; Konstantoudakis, S.; Arvanitidis, G.; Spathis, A.; Gouloumi, A.R.; Tsakiraki, Z.; Tsiodras, S.; Petrikkos, G. Diagnostic value of a semi-nested PCR for the diagnosis of mucormycosis and aspergillosis from paraffin-embedded tissue: A single center experience. Pathol. Res. Pract. 2016, 212, 393–397. [Google Scholar] [CrossRef]
- Walther, G.; Pawłowska, J.; Alastruey-Izquierdo, A.; Wrzosek, M.; Rodriguez-Tudela, J.L.; Dolatabadi, S.; Chakrabarti, A.; de Hoog, G.S. DNA barcoding in Mucorales: An inventory of biodiversity. Persoonia 2013, 30, 11–47. [Google Scholar] [CrossRef] [Green Version]
- Irinyi, L.; Lackner, M.; de Hoog, G.S.; Meyer, W. DNA barcoding of fungi causing infections in humans and animals. Fungal Biol. 2016, 120, 125–136. [Google Scholar] [CrossRef]
- Rassias, K.; Tamvakis, N.; Anastasiou, E.; Bartsokas, S. Rhinocerebral mucormycosis. Iatriki 1984, 46, 245–249. (In Greek) [Google Scholar]
- Filippidis, T.; Kouri, E.; Agapitos, M.; Papacharalampous, N.X. Lethal phycomycosis. Necrotomy findings and histological investigation. Iatriki 1985, 47, 251–254. (In Greek) [Google Scholar]
- Kalafrentzos, F.; Chatzimichail, A.; Tzanakakis, G.; Tsolakis, I.; Basiaris, C. Cutaneous and subcutaneous phycomycosis without predisposing factors. Hell. J. Surg. 1987, 59, 491–495. (In Greek) [Google Scholar]
- Kotzamanoglou, K.; Tzanakakis, G.; Michalopoulos, E.; Stathopoulou, M. Orbital cellulitis due to mucormycosis. A case report. Graefes Arch. Clin. Exp. Ophthalmol. 1988, 226, 539–541. [Google Scholar] [CrossRef]
- Economopoulou, P.; Laskaris, G.; Ferekidis, E.; Kanelis, N. Rhinocerebral mucormycosis with severe oral lesions: A case report. J. Oral Maxillofac. Surg. 1995, 53, 215–217. [Google Scholar] [CrossRef] [PubMed]
- Athanasiou, E.; Barbanis, S.; Kostopoulos, L.; Kaloutsi, V.; Zois, E.; Ageloudi, M.; Malaka, A.; Papadimitriou, C. Opportunistic infections in immunosuppressed/ immunodeficient patients: A histological and immunohistochemical study in three cases. Arch. Hellenic Pathol. 1998, 12, 116–121. (In Greek) [Google Scholar]
- Papadogeorgakis, N.; Logothetis, I.; Marti-Zografou, K.; Rondogianni, D.; Foundas, A.; Chalevelakis, G.; Raptis, S.A. Late surgical intervention in a diabetic patient with mucormycosis of the head and neck, after prolonged treatment with liposomal amphotericin B. Arch. Hellenic Med. 1999, 16, 496–500. (In Greek) [Google Scholar]
- Kanellopoulou, M.; Velegraki, A.; Mylona, E.; Papaefstathiou, K.; Legakis, N.; Papafrangas, E. Cutaneous Rhizopus oryzae mucormycosis. Arch. Hellenic Med. 1999, 16, 383–385. (In Greek) [Google Scholar]
- Alexopoulou, A.; Sevastianos, B.; Kalotairakis, A.; Petrikkos, G.; Petraki, K.; Hatzigiannis, S.I. Rhinoorbital mucormycosis in a patient with lymphocytic leukemia and iatrogenic diabetes mellitus. Iatriki 2000, 77, 563–568. (In Greek) [Google Scholar]
- Tsaousis, G.; Koutsouri, A.; Gatsiou, C.; Paniara, O.; Peppas, C.; Chalevelakis, G. Liver and brain mucormycosis in a diabetic patient type II successfully treated with liposomal amphotericin B. Scand. J. Infect. Dis. 2000, 32, 335–337. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, T.H.; Mastrodimos, V.; Tsilimbaris, M.; Pallikaris, J. Orbital mucormycosis. Iatriki 2001, 79, 74–78. (In Greek) [Google Scholar]
- Tsoutsos, D.; Tsati, E.; Metaxotos, N.; Keramidas, E.; Rodopoulou, S.; Ioannovich, J. Extensive burn injury complicated by mucormycosis: A case report. Ann. Burn. Fire Disasters 2001, 16, 1–2. [Google Scholar]
- Tryfon, S.; Stanopoulos, I.; Kakavelas, E.; Nikolaidou, A.; Kioumis, I. Rhinocerebral mucormycosis in a patient with latent diabetes mellitus: A case report. J. Oral Maxillofac. Surg. 2002, 60, 328–330. [Google Scholar] [CrossRef]
- Kyrmizakis, D.E.; Doxas, P.G.; Hajiioannou, J.K.; Papadakis, C.E. Palate ulcer due to mucormycosis. J. Laryngol. Otol. 2002, 116, 146–147. [Google Scholar] [CrossRef]
- Akritidis, N.; Papaioannides, D.; Kitsiou, E.; Korantzopoulos, P. Necrotizing cutaneous mucormycosis. Hosp. Med. 2002, 63, 308–309. [Google Scholar] [CrossRef]
- Georgopoulou, S.; Kounougeri, E.; Katsenos, C.; Rizos, M.; Michalopoulos, A. Rhinocerebral mucormycosis in a patient with cirrhosis and chronic renal failure. Hepatogastroenterology 2003, 50, 843–845. [Google Scholar] [PubMed]
- Kofteridis, D.P.; Karabekios, S.; Panagiotides, J.G.; Bizakis, J.; Kyrmizakis, D.; Saridaki, Z.; Gikas, A. Successful treatment of rhinocerebral mucormycosis with liposomal amphotericin B and surgery in two diabetic patients with renal dysfunction. J. Chemother. 2003, 15, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Economopoulos, N.; Kelekis, D.; Papadopoulos, A.; Kontopoulou, C.; Brountzos, E.N. Subclavian artery occlusion and pseudoaneurysm caused by lung apex mucormycosis: Successful treatment with transcatheter embolization. Cardiovasc. Intervent. Radiol. 2007, 30, 143–145. [Google Scholar] [CrossRef] [PubMed]
- Kotoulas, C.; Psathakis, K.; Tsintiris, K.; Sampaziotis, D.; Karnesis, L.; Laoutidis, G. Pulmonary mucormycosis presenting as Horner’s syndrome. Asian Cardiovasc. Thorac. Ann. 2006, 14, 86–87. [Google Scholar] [CrossRef]
- Liapis, C.D.; Petrikkos, G.L.; Paraskevas, K.I.; Skiada, A.; Nikolaou, A.C.; Tzortzis, G.; Kostakis, A. External Iliac artery stent mucormycosis in a renal transplant patient. Ann. Vasc. Surg. 2006, 20, 253–257. [Google Scholar] [CrossRef]
- Kontogiorgi, M.; Floros, I.; Koroneos, A.; Vamvouka, C.; Paniara, O.; Roussos, C.; Routsi, C. Fatal post-traumatic zygomycosis in an immunocompetent young patient. J. Med. Microbiol. 2007, 56, 1243–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mourkas, D.; Zacharioudaki, E.; Aggeletos, D.; Koltsidopoulos, P.; Kaisas, C.; Papapetropoulos, N.; Pappas, Z. Mucormycosis of the nose–paranasal sinuses. Case report and literature review. Hell. Otorhinolaryngol. Head Neck Surg. 2008, 34, 36–40. (In Greek) [Google Scholar]
- Bibashi, E.; Sidi, V.; Kotsiou, M.; Makrigiannaki, E.; Koliouskas, D. Pulmonary Zygomycosis caused by Cunninghamella bertholletiae in a child with acute lymphoblastic leukemia. Hippokratia 2008, 12, 43–45. [Google Scholar]
- Papadogeorgakis, N.; Parara, E.; Petsinis, V.; Vourlakou, C. A case of successfully treated rhinocerebral mucormycosis: Dental implications. Int. J. Dent. 2010, 2010, 273127. [Google Scholar] [CrossRef] [Green Version]
- Kompoti, M.; Michalia, M.; Kallitsi, G.; Giannopoulou, P.; Arabatzis, M.; Liapi, G.; Velegraki, A.; Trikka-Graphakos, E.; Clouva-Molyvdas, P.M. Fatal cutaneous Saksenaea vasiformis infection in a critically ill trauma patient. Mycoses. 2011, 54, e599–e601. [Google Scholar] [CrossRef] [PubMed]
- Lalayanni, C.; Baliakas, P.; Xochelli, A.; Apostolou, C.; Arabatzis, M.; Velegraki, A.; Anagnostopoulos, A. Outbreak of cutaneous zygomycosis associated with the use of adhesive tape in haematology patients. J. Hosp. Infect. 2012, 81, 213–215. [Google Scholar] [CrossRef] [PubMed]
- Bibashi, E.; de Hoog, G.S.; Pavlidis, T.E.; Symeonidis, N.; Sakantamis, A.; Walther, G. Wound infection caused by Lichtheimia ramosa due to a car accident. Med. Mycol. Case Rep. 2012, 2, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Dimaka, K.; Mallis, A.; Naxakis, S.S.; Marangos, M.; Papadas, T.A.; Stathas, T.; Mastronikolis, N.S. Chronic rhinocerebral mucormycosis: A rare case report and review of the literature. Mycoses 2014, 57, 699–702. [Google Scholar] [CrossRef]
- Kyriopoulos, E.J.; Kyriakopoulos, A.; Karonidis, A.; Gravvanis, A.; Gamatsi, I.; Tsironis, C.; Tsoutsos, D. Burn injuries and soft tissue traumas complicated by mucormycosis infection: A report of six cases and review of the literature. Ann. Burn. Fire Disasters 2015, 28, 280–287. [Google Scholar]
- Kalogerakos, P.D.; Kiparakis, M.; Pavlaki, K.; Pontikoglou, C.; Lazopoulos, G.; Chalkiadakis, G. Thoracoabdominal Resection of Mucormycosis Lesions in a Leukemic Patient. Ann. Thorac. Surg. 2018, 106, e239–e241. [Google Scholar] [CrossRef]
- Samaras, K.; Markantonatou, A.M.; Karapiperis, D.; Digonis, P.; Kartalis, N.; Kostogloudis, N.; Vyzantiadis, T.A. Saksenaea vasiformis infections: A case of an immunocompetent adult after mild injury and a literature review. J. Mycol. Med. 2019, 29, 260–264. [Google Scholar] [CrossRef]
- Dotis, J.; Printza, N.; Stabouli, S.; Karava, V.; Gkogka, C.; Vyzantiadis, T.A.; Roilides, E.; Papachristou, F. Disseminated mucormycosis in an adolescent kidney transplant recipient. Kidney Int. 2019, 95, 236. [Google Scholar] [CrossRef]
- Athanasiadou, K.I.; Athanasiadis, D.I.; Constantinidis, J.; Anastasiou, A.; Roilides, E.; Papakonstantinou, E. Successful treatment of rhinoorbital mucormycosis due to Rhizopus arrhizus with liposomal amphotericin B, posaconazole and surgical debridement in a child with neuroblastoma. Med. Mycol. Case Rep. 2019, 25, 10–14. [Google Scholar] [CrossRef]
- Antoniadi, K.; Iosifidis, E.; Vasileiou, E.; Tsipou, C.; Lialias, I.; Papakonstantinou, E.; Kattamis, A.; Polychronopoulou, S.; Roilides, E.; Tragiannidis, A. Invasive mucormycosis in children with malignancies: Report from the infection working group of the Hellenic Society of Pediatric Hematology-Oncology. J. Pediatr. Hematol. Oncol. 2021, 43, 176–179. [Google Scholar] [CrossRef] [PubMed]
- Stavrakas, M.; Koskinas, I.; Constantinidis, J.; Karkos, P.D. A “Terrible” Headache in a HIV Patient. Ear Nose Throat J. 2021, 28, 1455613211014106. [Google Scholar] [CrossRef] [PubMed]
- Ziaka, M.; Papakonstantinou, E.; Vasileiou, E.; Chorafa, E.; Antachopoulos, C.; Roilides, E. Paediatric cutaneous mucormycosis: A case report and review of the literature. Mycoses 2022, 65, 674–682. [Google Scholar] [CrossRef]
- Bitar, D.; Van Cauteren, D.; Lanternier, F.; Dannaoui, E.; Che, D.; Dromer, F.; Desenclos, J.C.; Lortholary, O. Increasing incidence of zygomycosis (mucormycosis), France, 1997–2006. Emerg. Infect. Dis. 2009, 15, 1395–1401. [Google Scholar] [CrossRef]
- Rees, J.R.; Pinner, R.W.; Hajjeh, R.A.; Brandt, M.E.; Reingold, A.L. The Epidemiological Features of Invasive Mycotic Infections in the San Francisco Bay Area, 1992–1993: Results of Population-Based Laboratory Active Surveillance. Clin. Infect. Dis. 1998, 27, 1138–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kontoyiannis, D.P.; Yang, H.; Song, J.; Kelkar, S.S.; Yang, X.; Azie, N.; Harrington, R.; Fan, A.; Lee, E.; Spalding, J.R. Prevalence, clinical and economic burden of mucormycosis-related hospitalizations in the United States: A retrospective study. BMC Infect. Dis. 2016, 16, 730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parra Fariñas, R.; Alonso-Sardón, M.; Velasco-Tirado, V.; Pérez, I.G.; Carbonell, C.; Álvarez Artero, E.; Romero-Alegría, Á.; Pardo-Lledías, J.; Belhassen-García, M. Increasing incidence of mucormycosis in Spanish inpatients from 1997 to 2018. Mycoses 2022, 65, 344–353. [Google Scholar] [CrossRef]
- Saegeman, V.; Maertens, J.; Meersseman, W.; Spriet, I.; Verbeken, E.; Lagrou, K. Increasing incidence of mucormycosis in University Hospital, Belgium. Emerg. Infect. Dis. 2010, 16, 1456–1458. [Google Scholar] [CrossRef]
- Mareș, M.; Moroti-Constantinescu, V.R.; Denning, D.W. The Burden of Fungal Diseases in Romania. J. Fungi 2018, 4, 31. [Google Scholar] [CrossRef] [Green Version]
- Mortensen, K.L.; Denning, D.W.; Arendrup, M.C. The burden of fungal disease in Denmark. Mycoses 2015, 58 (Suppl. S5), 15–21. [Google Scholar] [CrossRef]
- Buil, J.B.; Meijer, E.F.J.; Denning, D.W.; Verweij, P.E.; Meis, J.F. Burden of serious fungal infections in the Netherlands. Mycoses 2020, 63, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Prakash, H.; Chakrabarti, A. Epidemiology of Mucormycosis in India. Microorganisms 2021, 9, 523. [Google Scholar] [CrossRef] [PubMed]
- Lanternier, F.; Dannaoui, E.; Morizot, G.; Elie, C.; Garcia-Hermoso, D.; Huerre, M.; Bitar, D.; Dromer, F.; Lortholary, O.; The French Mycosis Study Group. A Global Analysis of Mucormycosis in France: The RetroZygo Study (2005–2007). Clin. Infect. Dis. 2012, 54, S35–S43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skiada, A.; Pagano, L.; Groll, A.; Zimmerli, S.; Dupont, B.; Lagrou, K.; Lass-Florl, C.; Bouza, E.; Klimko, N.; Gaustad, P.; et al. Zygomycosis in Europe: Analysis of 230 cases accrued by the registry of the European Confederation of Medical Mycology (ECMM) Working Group on Zygomycosis between 2005 and 2007. Clin. Microbiol. Infect. 2011, 17, 1859–1867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagano, L.; Valentini, C.G.; Posteraro, B.; Girmenia, C.; Ossi, C.; Pan, A.; Candoni, A.; Nosari, A.; Riva, M.; Cattaneo, C.; et al. Zygomycosis in Italy: A Survey of FIMUA-ECMM (Federazione Italiana Di Micopatologia Umana ed Animale and European Confederation of Medical Mycology). J. Chemother. 2009, 21, 322–329. [Google Scholar] [CrossRef]
- Kömür, S.; İnal, A.S.; Kurtaran, B.; Ulu, A.; Uğuz, A.; Aksu, H.S.; Taşova, Y. Mucormycosis: A 10-year experience at a tertiary care center in Turkey. Turk. J. Med. Sci. 2016, 46, 58–62. [Google Scholar] [CrossRef]
- Kennedy, K.; Daveson, K.; Slavin, M.; Van Hal, S.; Sorrell, T.; Lee, A.; Marriott, D.; Chapman, B.; Halliday, C.; Hajkowicz, K.; et al. Mucormycosis in Australia: Contemporary epidemiology and outcomes. Clin. Microbiol. Infect. 2016, 22, 775–781. [Google Scholar] [CrossRef] [Green Version]
- Dolatabadi, S.; Ahmadi, B.; Rezaei-Matehkolaei, A.; Zarrinfar, H.; Skiada, A.; Mirhendi, H.; Nashibi, R.; Niknejad, F.; Nazeri, M.; Rafiei, A.; et al. Mucormycosis in Iran: A six-year retrospective experience. J. Mycol. Med. 2018, 28, 269–273. [Google Scholar] [CrossRef]
- Patel, A.; Kaur, H.; Xess, I.; Michael, J.S.; Savio, J.; Rudramurthy, S.; Singh, R.; Shastri, P.; Umabala, P.; Sardana, R.; et al. A multicentre observational study on the epidemiology, risk factors, management and outcomes of mucormycosis in India. Clin. Microbiol. Infect. 2020, 26, e9–e944. [Google Scholar] [CrossRef]
- Corzo-León, D.E.; Chora-Hernández, L.D.; Rodríguez-Zulueta, A.P.; Walsh, T.J. Diabetes mellitus as the major risk factor for mucormycosis in Mexico: Epidemiology, diagnosis, and outcomes of reported cases. Med. Mycol. 2018, 56, 29–43. [Google Scholar] [CrossRef] [Green Version]
- Makrilakis, K.; Kalpourtzi, N.; Ioannidis, I.; Iraklianou, S.; Raptis, A.; Sotiropoulos, A.; Gavana, M.; Vantarakis, A.; Kantzanou, M.; Hadjichristodoulou, C.; et al. Prevalence of diabetes and pre-diabetes in Greece. Results of the First National Survey of Morbidity and Risk Factors (EMENO) study. Diabetes Res. Clin. Pract. 2021, 172, 108646. [Google Scholar] [CrossRef]
- Chevreul, K.; Berg Brigham, K.; Bouché, C. The burden and treatment of diabetes in France. Global. Health 2014, 10, 6. [Google Scholar] [CrossRef] [Green Version]
- Giampaoli, S.; Palmieri, L.; Donfrancesco, C.; Lo Noce, C.; Pilotto, L.; Vanuzzo, D. Osservatorio Epidemiologico Cardiovascolare/Health Examination Survey Research Group. Cardiovascular health in Italy. Ten-year surveillance of cardiovascular diseases and risk factors: Osservatorio Epidemiologico Cardiovascolare/Health Examination Survey 1998–2012. Eur. J. Prev. Cardiol. 2015, 22, 9–37. [Google Scholar] [CrossRef]
- Heidemann, C.; Scheidt-Nave, C.; Koch-Institut, R. Prevalence, incidence and mortality of diabetes mellitus in adults in Germany-A review in the framework of the Diabetes Surveillance. J. Health Monit. 2017, 2, 98–121. [Google Scholar] [CrossRef]
- Soriguer, F.; Goday, A.; Bosch-Comas, A.; Bordiú, E.; Calle-Pascual, A.; Carmena, R. Prevalence of diabetes mellitus and impaired glucose regulation in Spain: The Di@bet.es study. Diabetologia 2012, 55, 88–93. [Google Scholar] [CrossRef] [Green Version]
- Kaveeshwar, S.A.; Cornwall, J. The current state of diabetes mellitus in India. Australas. Med. J. 2014, 7, 45–48. [Google Scholar] [CrossRef]
- Mathur, P.; Leburu, S.; Kulothungan, V. Prevalence, Awareness, Treatment and Control of Diabetes in India From the Countrywide National NCD Monitoring Survey. Front. Public Health 2022, 10, 748157. [Google Scholar] [CrossRef]
- Arora, U.; Priyadarshi, M.; Katiyar, V.; Soneja, M.; Garg, P.; Gupta, I. Risk factors for Coronavirus disease-associated mucormycosis. J. Infect. 2022, 84, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Cornely, O.A.; Maertens, J.; Winston, D.J.; Perfect, J.; Ullmann, A.J.; Walsh, T.J. Posaconazole vs fluconazole or itraconazole prophylaxis in patients with neutropenia. N. Engl. J. Med. 2007, 356, 348–359. [Google Scholar] [CrossRef] [Green Version]
- Walsh, T.J.; Anaissie, E.J.; Denning, D.W.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Segal, B.H.; Steinbach, W.J.; Stevens, D.A.; et al. Treatment of aspergillosis: Clinical practice guidelines of the Infectious Diseases Society of America. Clin. Infect. Dis. 2008, 46, 327–360. [Google Scholar] [CrossRef]
- Leventakos, K.; Lewis, R.E.; Kontoyiannis, D.P. Fungal infections in leukemia patients: How do we prevent and treat them? Clin. Infect. Dis. 2010, 50, 405–415. [Google Scholar] [CrossRef]
- Kung, H.C.; Johnson, M.D.; Drew, R.H.; Saha-Chaudhuri, P.; Perfect, J.R. Clinical effectiveness of posaconazole versus fluconazole as antifungal prophylaxis in hematology-oncology patients: A retrospective cohort study. Cancer Med. 2014, 3, 667–673. [Google Scholar] [CrossRef]
- Cornely, O.A.; Robertson, M.N.; Haider, S.; Grigg, A.; Geddes, M.; Aoun, M.; Heinz, W.J.; Raad, I.; Schanz, U.; Meyer, R.G.; et al. Pharmacokinetics and safety results from the Phase 3 randomized, open-label, study of intravenous posaconazole in patients at risk of invasive fungal disease. J. Antimicrob. Chemother. 2017, 72, 3406–3413. [Google Scholar] [CrossRef] [Green Version]
- Pana, Z.D.; Seidel, D.; Skiada, A.; Groll, A.H.; Petrikkos, G.; Cornely, O.A.; Roilides, E.; Collaborators of Zygomyco.net and/or FungiScope™ Registries*. Invasive mucormycosis in children: An epidemiologic study in European and non-European countries based on two registries. BMC Infect. Dis. 2016, 16, 667. [Google Scholar] [CrossRef] [Green Version]
- Jeong, W.; Keighley, C.; Wolfe, R.; Lee, W.L.; Slavin, M.A.; Kong, D.C.M.; Chen, S.C.A. The epidemiology and clinical manifestations of mucormycosis: A systematic review and meta-analysis of case reports. Clin. Microbiol. Infect. 2019, 25, 26–34. [Google Scholar] [CrossRef] [Green Version]
- Prakash, H.; Ghosh, A.K.; Rudramurthy, S.M.; Singh, P.; Xess, I.; Savio, J.; Pamidimukkala, U.; Jillwin, J.; Varma, S.; Das, A.; et al. A prospective multicenter study on mucormycosis in India: Epidemiology, diagnosis, and treatment. Med. Mycol. 2019, 57, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.; Sun, X. Characteristics of pulmonary mucormycosis and predictive risk factors for the outcome. Infection 2018, 46, 503–512. [Google Scholar] [CrossRef]
- Antoniadou, A. Outbreaks of zygomycosis in hospitals. Clin. Microbiol. Infect. 2009, 15, 55–59. [Google Scholar] [CrossRef] [Green Version]
- Prakash, H.; Chakrabarti, A. Global Epidemiology of Mucormycosis. J. Fungi 2019, 5, 26. [Google Scholar] [CrossRef] [Green Version]
- Benedict, K.; Park, B.J. Invasive Fungal Infections after Natural Disasters. Emerg. Infect. Dis. 2014, 20, 349–355. [Google Scholar] [CrossRef]
- Huppert, H.E.; Sparks, R.S.J. Extreme natural hazards: Population growth, globalization and environmental change. Philos. Trans. R. Soc. Lond. Ser. A Math. Phys. Eng. Sci. 2006, 364, 1875–1888. [Google Scholar] [CrossRef]
- Vitale, R.G.; de Hoog, G.S.; Schwarz, P.; Dannaoui, E.; Deng, S.; Machouart, M.; Voigt, K.; van de Sande, W.W.; Dolata Badi, S.; Meis, J.F.; et al. Antifungal susceptibility and phylogeny of opportunistic members of the order mucorales. J. Clin. Microbiol. 2012, 50, 66–75. [Google Scholar] [CrossRef] [Green Version]
- Chowdhary, A.; Singh, P.K.; Kathuria, S.; Hagen, F.; Meis, J.F. Comparison of the EUCAST and CLSI Broth Microdilution Methods for Testing Isavuconazole, Posaconazole, and Amphotericin B against Molecularly Identified Mucorales Species. Antimicrob. Agents Chemother. 2015, 59, 7882–7887. [Google Scholar] [CrossRef] [Green Version]
- Badali, H.; Cañete-Gibas, C.; McCarthy, D.; Patterson, H.; Sanders, C.; David, M.P.; Mele, J.; Fan, H.; Wiederhold, N.P. Epidemiology and Antifungal Susceptibilities of Mucoralean Fungi in Clinical Samples from the United States. J. Clin. Microbiol. 2021, 59, e0123021. [Google Scholar] [CrossRef]
- Drogari-Apiranthitou, M.; Mantopoulou, F.D.; Skiada, A.; Kanioura, L.; Grammatikou, M.; Vrioni, G.; Mitroussia-Ziouva, A.; Tsakris, A.; Petrikkos, G. In vitro antifungal susceptibility of filamentous fungi causing rare infections: Synergy testing of amphotericin B, posaconazole and anidulafungin in pairs. J. Antimicrob. Chemother. 2012, 67, 1937–1940. [Google Scholar] [CrossRef]
- Spellberg, B.; Walsh, T.; Kontoyiannis, D.P.; Edwards, J., Jr.; Ibrahim, A.S. Recent advances in the management of mucormycosis: From bench to bedside. Clin. Infect. Dis. 2009, 48, 1743–1751. [Google Scholar] [CrossRef]
- Lewis, R.E.; Cahyame-Zuniga, L.; Leventakos, K.; Chamilos, G.; Ben-Ami, R.; Tamboli, P.; Tarrand, J.; Bodey, G.P.; Luna, M.; Kontoyiannis, D.P. Epidemiology and sites of involvement of invasive fungal infections in patients with haematological malignancies: A 20-year autopsy study. Mycoses 2013, 56, 638–645. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Reference | Age | Gender | Localization/Clinical Form | Organism | Underlying Condition | Time to Antifungal (days) | Therapy (mg/kg/d) | Surgery | Outcome 60 d |
|---|---|---|---|---|---|---|---|---|---|
| 1984 Rassias et al. [20] | x | x | Rhinocerebral | x | DM | x | |||
| 1985 Filippidis et al. [21] | 24 | Μ | Disseminated | x | d (post mortem diagnosis) | ||||
| 1987 Kalafrenzos et al. [22] | x | Soft tissues | Absidia | none | AmB | yes | s | ||
| 1988 Kotzamanoglou et al. [23] | 76 | F | Orbital | x | DM after cortico | 10 | AmB | no | d |
| 1995 Economopoulou et al. [24] | 55 | F | Sinus | x | DM, cortico, pericarditis | 21 | AmB | no | s |
| 1998 Athanasiou et al. [25] | x | Soft tissues | x | ALL | AmB | s | |||
| 1999 Papadogeorgakis et al. [26] | 65 | Μ | Rhino- orbital | x | DM, COPD | 60 | AmB | yes | s |
| 1999 Kanellopoulou et al. [27] | 60 | F | Cutaneous abdomen LE | Rhizopus arrhizus | none | 1 | AmB3 | yes | s |
| 2000 Alexopoulou et al. [28] | 60 | M | Rhino- orbital | Rhizopus arrhizus | ALL, DM | 1 | AmB | yes | s |
| 2000 Tsaousis et al. [29] | 73 | F | Liver-Brain | Rhizopus | DM | 20 | AmB1.5, itr | no | s |
| 2001 Papadaki. et al. [30] | 73 | F | Orbital | x | immunosuppression | >14 | AmB, pos | yes | d |
| 2001 Tsoutsos et al. [31] | 38 | M | Cutaneous | x | Burns | x | AmB | yes | d |
| 2002 Tryfon et al. [32] | 57 | F | Rhinocerebral | x | DM, periodontitis | 4 | AmB0.25 | no | d (10 days) |
| 2002 Kyrmizakis et al. [33] | 79 | M | Palate | Absidia corymbifera | DM, chronic kidney failure | AmB | yes | s | |
| 2002 Akritidis et al. [34] | 75 | F | Cutaneous | Rhizopus arrhizus | DM, MDS, neutropenia | 4 | AmB | yes | d (14 days) |
| 2003 Georgopoulou et al. [35] | 58 | F | Rhinocerebral | x | cirrhosis, renal failure, anaemia, thrombocytopenia, DM | 4 | AmB5 | no | d (5 days) |
| 2003 Kofteridis et al. [36] | 66, 79 | 2M | Rhino-orbito-cerebral | x | 1DM, ARF, 1DM, cortico | 3, 7 | AmB3 | yes | s 2 |
| 2003 Petrikkos et al. [5] | 37–80 | 15M, 9F | 12 Soft tissues, 11 Rhinocerebral, 1 lung | 8 Rhizopus spp., 16 Mucor spp.* | 7DM, 1 kidney transplantation, 3 car accidents, 1 burns, 2 scratch, 1thorn (skin), 9 (F) haem (6 AML, 1CLL, 2MDS) | 24 AmB3-5 | 11 | s 11, d 13 | |
| 2006 Economopoulos et al. [37] | 33 | F | Pulmonary. | x | DM ketoacidosis | 1 | AmB, +pos | yes | s |
| 2006 Kotoulas et al. [38] | 33 | F | Pulmonary | x | DM coma | 1 | AmB, +pos | yes | lost to followup |
| 2006 Liapis et al. [39] | 38 | M | Iliac artery stent | x | previous kidney graft rejection, hemodialysis, stents rec thrombosis | 60 | AmB3-5 | yes | s |
| 2007 Kontogiorgi et al. [40] | 25 | M | Pulmonary- Cutaneous | Rhizopus spp. | farmer tractor accident | 3 | AmB4-7 | yes | d |
| 2008 Mourkas et al. [41] | 36 | Μ | Sinus-palate | x | Hodgkin’s lymphoma | 7 | AmB, pos, hyperb | yes | s |
| 2008 Bibashi et al. [42] | 10 | M | Pulmonary | Cunninghamella | ALL, neutropenia | 1 | AmB7 | d | |
| 2010 Papadogeorgakis et al. [43] | 22 | F | Sinus | x | DM | >7 | AmB, pos | s | |
| 2011 Kompoti et al. [44] | 30 | Μ | Cutaneous | Saksenaea | car accident | 0 | AmB, pos, hyperb | yes | d |
| 2012 Lalayanni et al. [45] | 15–58 | 2M, 2F | 4 outbreak cutaneous | Rhizopus arrhizus | 4 haematol | 1AmB3-5, 1pos, AmB + pos2 | yes | s | |
| 2012 Bibashi et al. [46] | 32 | M | Subcutaneous | Lichtheimia ramosa | car accident | no | yes | s | |
| 2014 Dimaka et al. [47] | 87 | M | Sinus | x | DM, coronary, CVA | AmB 5, pos | no | s | |
| 2015 Kyriopoulos et al. [48] | 26–71 | 6M | Cutaneous | 3 Rhizopus, 3 Rhizomucor | 3 fire burns, 1 friction burn car accident, DM, 2 road accidents | 0–21 | AmB0.5 | 5yes | d 2 fire burns |
| 2018 Kalogerakos et al. [49] | 56 | M | Thoracoabdominal | x | AML, neutropenia | AmB + pos | yes | s | |
| 2019 Samaras et al. [50] | 39 | M | Cutaneous | Saksenaea | injury | 63 | AmB 5, pos | s | |
| 2019 Dotis et al. [51] | 16 | F | Disseminated | Rhizopus arrhizus | kidney transplant | AmB 5, pos | yes | s | |
| 2019 Athanasiadou et al. [52] | 11 | M | Rhino-orbital | Rhizopus arrhizus | recurrent neuroblast, neutrop. | 4 | AmB 7, +pos | s | |
| 2020 Antoniadi et al. [53] | 2–15 | 2F 4M | 3 Rhino-orbital, 2 CNS, 1 Soft tissues | 2 Rhizopus, 1 Mucor sp., 1 Lichtheimia sp. | 4 paediatric malignancy (3 ALL, 1 AML,1 neuroblastoma, 1 CNS tumor | 5 to 30 (avg. 13) | 1L-AmB3-10, 1 + pos, 2 + cas, 1 + vor, 1 + cas, vor | 4yes | s 6 |
| 2021 Stavrakas et al. [54] | 52 | M | Sinus | x | HIV | 1 | yes | yes | s |
| 2022 Ziaka et al. [55] | 10 | F | Cutaneous | Rhizopus microsporus | ALL | 1 | AmB8 | yes | s |
| All Cases | 2005–2008 | 2009–2022 | ||||
|---|---|---|---|---|---|---|
| Clinical Form/Localization | n | % | n | % | n | % |
| Rhinocerebral | 56 | 51.8 | 22 | 44 | 34 | 58.6 |
| Cutaneous/soft tissues | 35 | 32.4 | 20 | 40 | 15 | 25.9 |
| Pulmonary | 12 | 11.1 | 6 | 12 | 6 | 10.3 |
| other * | 2 | 1.8 | 1 | 2 | 1 | 1.7 |
| Disseminated | 2 | 1.8 | 1 | 2 | 1 | 1.7 |
| Bone ** | 1 | 0.9 | 2 | 1 | 1.7 | |
| Total | 108 | 50 | 58 |
| Underlying Condition | All Cases | 2005–2008 | 2009–2022 | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Haematologic malignancy/neutropenia | 32 | 29.9 | 17 | 34 | 15 | 26.3 |
| AML | 13 | 5 | 8 | |||
| non-Hodgkin’s lymphoma | 6 | 4 | 2 | |||
| MDS | 4 | 3 | 1 | |||
| Hodgkin lymphoma | 2 | 1 | 1 | |||
| aplastic anemia | 2 | 2 | ||||
| CMML | 2 | 2 | ||||
| ALL | 1 | 1 | ||||
| CLL | 1 | 1 | ||||
| ABL | 1 | 1 | ||||
| HSCT | 5 | 4.7 | 1 | 2 | 4 | 7 |
| Kidney transplantation | 3 | 2.8 | 3 | 5.3 | ||
| Diabetes mellitus | 17 | 15.9 | 7 | 14 | 10 | 17.5 |
| Trauma | 24 | 22.4 | 15 | 30 | 9 | 15.8 |
| Burns | 2 | 2 | ||||
| Surgery/iatrogenic | 15 | 13 | 2 | |||
| Accidents | 7 | 2 | 5 | |||
| SO/or other cancer | 9 | 8.4 | 3 | 6 | 6 | 10.5 |
| Auto-immune | 8 | 7.5 | 6 | 12 | 2 | 3.5 |
| other * | 5 | 4.7 | 1 | 2 | 4 | 7 |
| None/not reported | 4 | 3.7 | 4 | 7 | ||
| Total ** | 107 | 50 | 57 |
| Clinical Form | HM n = 32 | % | DM n = 17 | % |
|---|---|---|---|---|
| Rhinocerebral | 23 | 71.9 | 10 | 58.8 |
| Cutaneous | 3 | 17.6 | ||
| Pulmonary | 5 | 15.6 | 3 | 17.6 |
| Disseminated | 2 | 6.2 | ||
| Other * | 2 | 6.2 | 1 | 5.9 |
| Organisms | Cases | ROC | Pulmonary | Cutaneous | Other | Mortality (%) | |
|---|---|---|---|---|---|---|---|
| n | % | All | |||||
| Rhizopus | 55 | 67.1 | 14/36 | 3/4 | 7/14 | 1/1 disseminated | 26/43 * (60.5) |
| R. arrhizus | 45 | 54.9 | |||||
| R. microsporus | 3 | 3.6 | |||||
| Rizopus spp. | 7 | 8.5 | |||||
| Lichtheimia | 7 | 8.5 | 0/1 | 1/1 | 1/3 | 0/1 brain, 1/1 lung/heart | 3/7 (42.9) |
| L. ramosa | 2 | 2.4 | |||||
| L. corymbifera | 1 | 1.2 | |||||
| Lichtheimia spp. | 4 | 4.9 | |||||
| Mucor | 5 | 6.1 | 0/1 | 0/2 | 0/3 * (0) | ||
| M. circinelloides | 4 | 4.9 | |||||
| Mucor spp. | 1 | 1.2 | |||||
| Saksenaea vasiformis | 3 | 3.6 | 0/2 | 0/1 bone | 0/3 (0) | ||
| Apophysomyses elegans | 1 | 1.2 | 0/1 | 0/1 (0) | |||
| Syncephalastrum racemosum | 1 | 1.2 | 0/1 | 0/1 (0) | |||
| Mucorales ** | 10 | 12.2 | |||||
| Total | 82 |
| 2005–2008 | 2009–2022 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Localisation | Mortality | % | Survival | % | Unknown | Mortality | % | Survival | % | Unknown |
| Sinus/palate | 2/10 | 28.6 * | 5/10 | 71.4 * | 3 | 1/18 | 7.1 * | 13/18 | 92.8 * | 4 |
| Rhino-(orbito)-cerebral | 10/12 | 90.9 * | 1/10 | 9.1 * | 1 | 8/15 | 72.7 * | 2/15 | 27.3 * | 5 |
| Cutaneous | 9/20 | 52.9 * | 8/20 | 47.1 * | 3 | 3/15 | 25 * | 9/15 | 75 * | 3 |
| Pulmonary | 4/6 | 66.7 | 2/6 | 33.3 | 1/6 | 33.3 * | 2/6 | 66.7 * | 3 | |
| Disseminated | 1/1 | 100 | 1/1 | 100 | ||||||
| Lung/heart | 1/1 | |||||||||
| Brain | 1/1 | 100 | ||||||||
| Bone | 1/1 | 100 | ||||||||
| Underlying condition | ||||||||||
| HM/neutropenia | 10/18 | 66.7 * | 5/18 | 33.3 * | 3 | 4/15 | 40 * | 6/10 | 60 * | 5 |
| HSCT | 1 | 2/4 | 50 * | 2 | ||||||
| Diabetes mellitus | 2/7 | 33.3 * | 4/7 | 66.7 * | 1 | 2/10 | 20 | 8/10 | 80 | |
| Trauma | 8/15 | 57.1 * | 6/15 | 42.9 * | 1 | 3/9 | 33.3 | 6/9 | 66.7 | |
| SO/or other cancer | 3/3 | 100 | 3/6 | 50 | 3/6 | 50 | ||||
| Autoimmune | 4/6 | 80 * | 1/6 | 20 * | 1 | 1/2 | 100 * | 1 | ||
| Kidney transplantation | 1/3 | 100 * | 2 | |||||||
| Other ** | 1 | 1/8 | 33.3 * | 2/8 | 66.7 | 5 | ||||
| Published | % | Registered | % | |
|---|---|---|---|---|
| Localisation | ||||
| Rhinocerebral | 8 | 25 | 56 | 51.5 |
| Cutaneous/soft tissues | 17 | 53.1 | 35 | 32 |
| Pulmonary | 4 | 12.5 | 12 | 10.3 |
| CNS | 2 | 6.2 | 1 | 2 |
| Disseminated | 1 | 3 | 2 | 3.1 |
| other a | 2 | 3.1 | ||
| Underlying condition | ||||
| Haematologic malignancy | 12 | 37.5 | 32 | 29.9 |
| Kidney transplantation | 2 | 6.2 | 3 | 2.8 |
| Diabetes mellitus | 4 | 12.5 | 17 | 15.9 |
| Trauma/burn | 10 | 31.2 | 24 | 22.4 |
| SO cancer | 3 | 9.4 | 9 | 8.4 |
| Autoimmune | 8 | 7.5 | ||
| HIV | 1 | 3 | ||
| Organism | ||||
| Rhizopus arrhizus | 6 | 25 | 45 | 54.9 |
| Rhizopus microsporus | 3 | 3.6 | ||
| Rhizopus spp. | 7 | 29.2 | 7 | 8.5 |
| Lichtheimia spp. | 2 | 8.3 | 7 | 8.5 |
| Mucor spp. | 1 | 4.2 | 5 | 6.1 |
| Saksenaea vasiformis | 2 | 8.3 | 3 | 3.6 |
| Apophysomyces elegans | 1 | 1.2 | ||
| Syncephalastrum racemosum | 1 | 1.2 | ||
| Cunninghamella bertholetiae | 1 | 4.2 | ||
| Rhizomucor | 3 | 12.5 | ||
| Mucorales * | 2 | 8.3 | 10 | 13.9 |
| Outcome | ||||
| survival | 26 | 83.9 ** | 44 | 51.2 ** |
| death | 5 | 16.1 ** | 42 | 48.8 ** |
| unknown | 1 | 2.7 | 22 | 20.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drogari-Apiranthitou, M.; Skiada, A.; Panayiotides, I.; Vyzantiadis, T.-A.; Poulopoulou, A.; Christofidou, M.; Antoniadou, A.; Roilides, E.; Iosifidis, E.; Mamali, V.; et al. Epidemiology of Mucormycosis in Greece; Results from a Nationwide Prospective Survey and Published Case Reports. J. Fungi 2023, 9, 425. https://doi.org/10.3390/jof9040425
Drogari-Apiranthitou M, Skiada A, Panayiotides I, Vyzantiadis T-A, Poulopoulou A, Christofidou M, Antoniadou A, Roilides E, Iosifidis E, Mamali V, et al. Epidemiology of Mucormycosis in Greece; Results from a Nationwide Prospective Survey and Published Case Reports. Journal of Fungi. 2023; 9(4):425. https://doi.org/10.3390/jof9040425
Chicago/Turabian StyleDrogari-Apiranthitou, Maria, Anna Skiada, Ioannis Panayiotides, Timoleon-Achilleas Vyzantiadis, Aikaterina Poulopoulou, Myrto Christofidou, Anastasia Antoniadou, Emmanuel Roilides, Elias Iosifidis, Vassiliki Mamali, and et al. 2023. "Epidemiology of Mucormycosis in Greece; Results from a Nationwide Prospective Survey and Published Case Reports" Journal of Fungi 9, no. 4: 425. https://doi.org/10.3390/jof9040425