
Invasive Fungal Breakthrough Infections under Targeted Echinocandin Prophylaxis in High-Risk Liver Transplant Recipients

Abstract
:1. Introduction
2. Materials and Methods
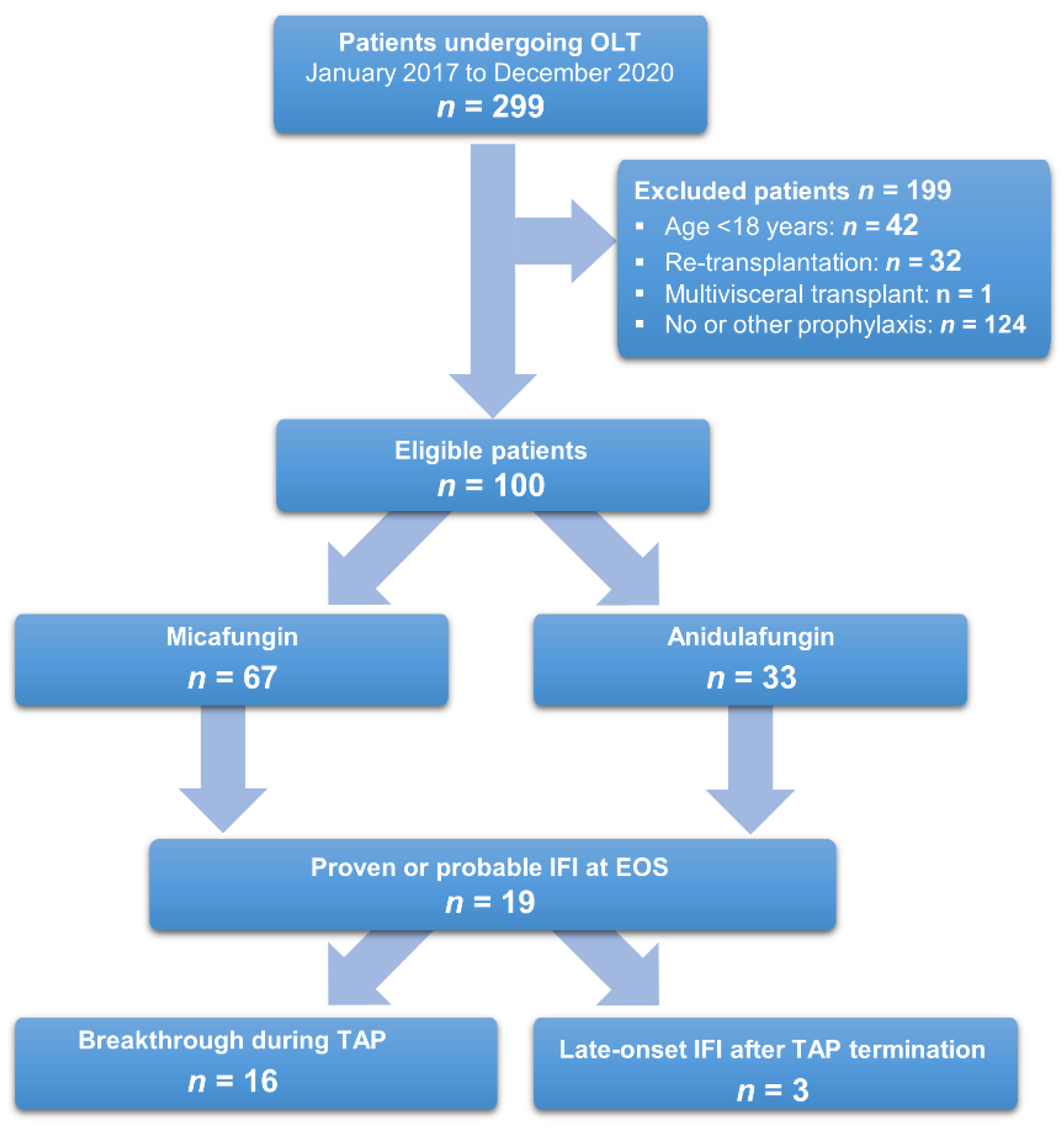
2.1. Study Population and Data Acquisition
2.2. Definition of an Invasive Fungal Infection and Breakthrough Infection
2.3. Immunosuppression and Overall Anti-Infective Prophylaxis
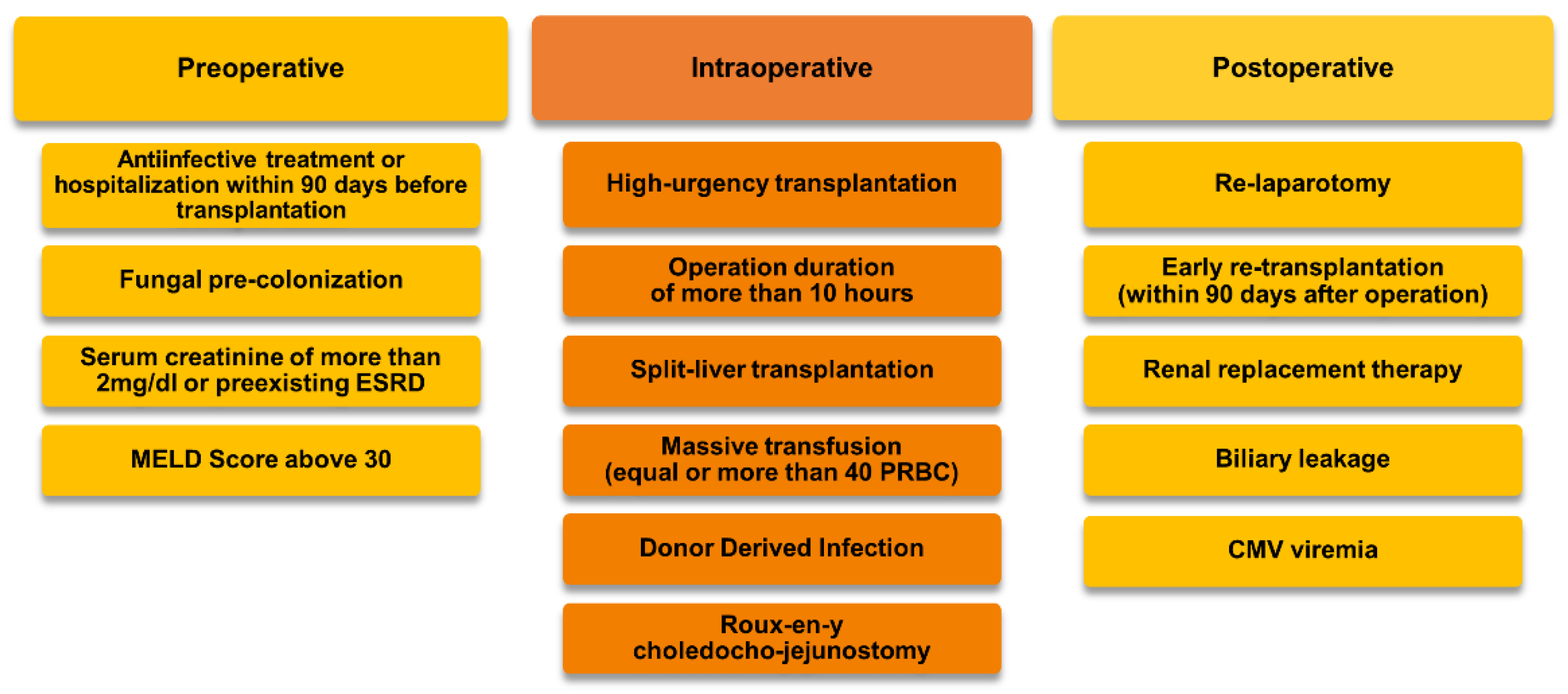
2.4. Antimycotic Prophylaxis and Treatment
2.5. Surgical Technique
2.6. Outcomes
2.7. Statistical Analyses
3. Results
3.1. Patient Population and Risk Factors for b-IFI
3.2. Targeted Antimycotic Prophylaxis
3.3. Characteristics of Invasive Fungal Infections
3.3.1. Incidence
3.3.2. Composition of Pathogens and Infection Sites
3.3.3. Susceptibility and the Therapeutic Regimen
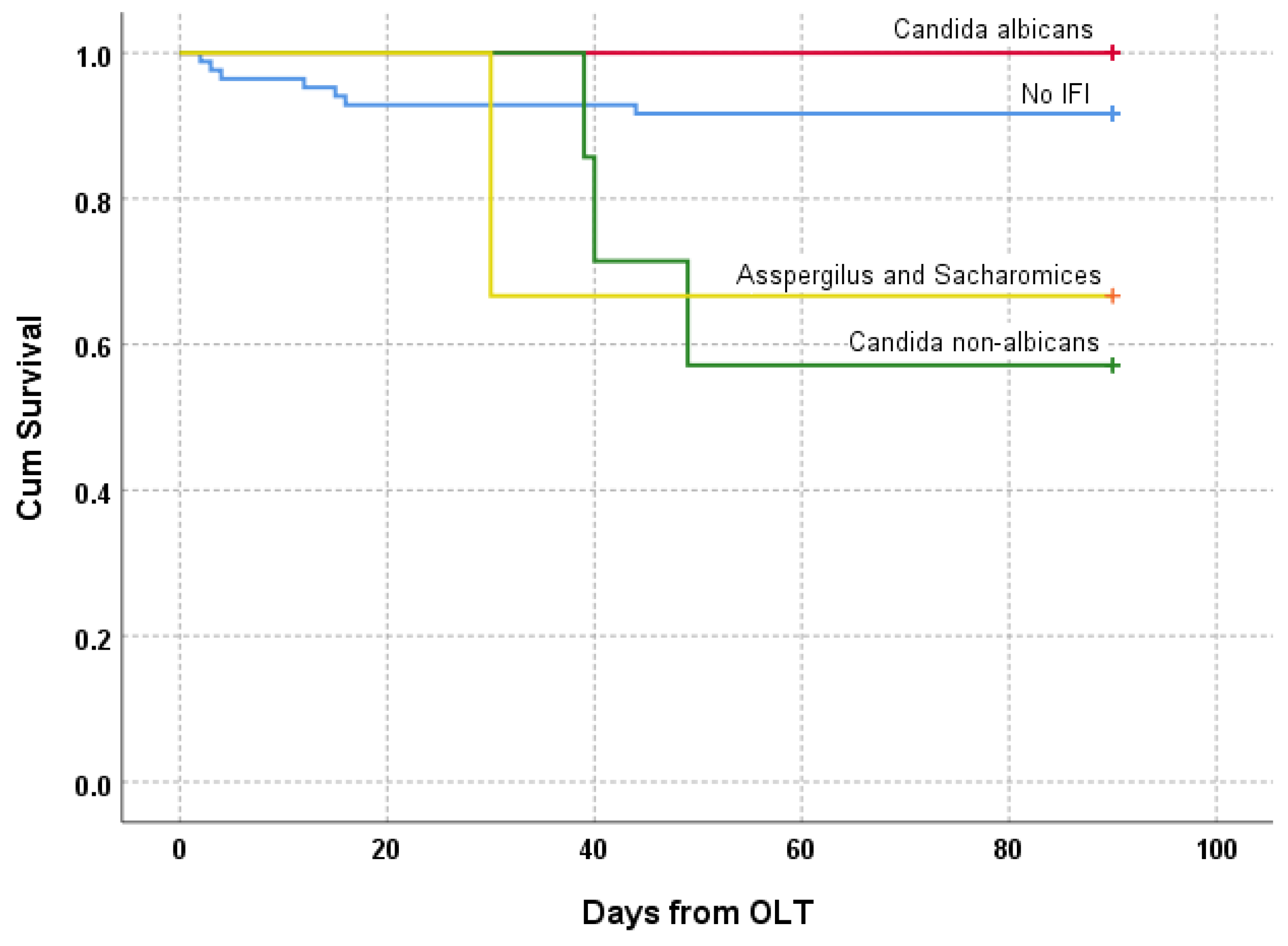
3.4. Outcome
3.4.1. Postoperative Course
3.4.2. Mortality
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scolarici, M.; Jorgenson, M.; Saddler, C.; Smith, J. Fungal Infections in Liver Transplant Recipients. J. Fungi 2021, 7, 524. [Google Scholar] [CrossRef]
- Singh, N.; Wagener, M.M.; Marino, I.R.; Gayowski, T. Trends in Invasive Fungal Infections in Liver Transplant Recipients: Correlation with Evolution in Transplantation Practices. Transplantation 2002, 73, 63–67. [Google Scholar] [CrossRef]
- Silveira, F.P.; Husain, S. Fungal Infections in Solid Organ Transplantation. Med. Mycol. 2007, 45, 305–320. [Google Scholar] [CrossRef]
- Saliba, F.; Delvart, V.; Ichaï, P.; Kassis, N.; Botterel, F.; Mihaila, L.; Azoulay, D.; Adam, R.; Castaing, D.; Bretagne, S.; et al. Fungal Infections after Liver Transplantation: Outcomes and Risk Factors Revisited in the MELD Era. Clin. Transpl. 2013, 27, E454–E461. [Google Scholar] [CrossRef]
- Singh, N. Fungal Infections in the Recipients of Solid Organ Transplantation. Infect. Dis. Clin. N. Am. 2003, 17, 113–134. [Google Scholar] [CrossRef]
- Paya, C.V. Fungal Infections in Solid-Organ Transplantation. Clin. Infect. Dis. 1993, 16, 677–688. [Google Scholar] [CrossRef]
- Gavaldà, J.; Meije, Y.; Fortún, J.; Roilides, E.; Saliba, F.; Lortholary, O.; Muñoz, P.; Grossi, P.; Cuenca-Estrella, M. Invasive Fungal Infections in Solid Organ Transplant Recipients. Clin. Microbiol. Infect. 2014, 20 (Suppl. S7), 27–48. [Google Scholar] [CrossRef] [Green Version]
- Barchiesi, F.; Mazzocato, S.; Mazzanti, S.; Gesuita, R.; Skrami, E.; Fiorentini, A.; Singh, N. Invasive Aspergillosis in Liver Transplant Recipients: Epidemiology, Clinical Characteristics, Treatment, and Outcomes in 116 Cases. Liver Transpl. 2015, 21, 204–212. [Google Scholar] [CrossRef]
- Nagao, M.; Fujimoto, Y.; Yamamoto, M.; Matsumura, Y.; Kaido, T.; Takakura, S.; Uemoto, S.; Ichiyama, S. Epidemiology of Invasive Fungal Infections after Liver Transplantation and the Risk Factors of Late-Onset Invasive Aspergillosis. J. Infect. Chemother. 2016, 22, 84–89. [Google Scholar] [CrossRef]
- Zicker, M.; Colombo, A.L.; Ferraz-Neto, B.H.; Camargo, L.F.A. Epidemiology of Fungal Infections in Liver Transplant Recipients: A Six-Year Study of a Large Brazilian Liver Transplantation Centre. Mem. Inst. Oswaldo Cruz 2011, 106, 339–345. [Google Scholar] [CrossRef] [Green Version]
- Neofytos, D.; Fishman, J.A.; Horn, D.; Anaissie, E.; Chang, C.H.; Olyaei, A.; Pfaller, M.; Steinbach, W.J.; Webster, K.M.; Marr, K.A. Epidemiology and Outcome of Invasive Fungal Infections in Solid Organ Transplant Recipients. Transpl. Infect. Dis. 2010, 12, 220–229. [Google Scholar] [CrossRef]
- Vera, A.; Contreras, F.; Guevara, F. Incidence and Risk Factors for Infections after Liver Transplant: Single-Center Experience at the University Hospital Fundación Santa Fe de Bogotá, Colombia. Transpl. Infect. Dis. 2011, 13, 608–615. [Google Scholar] [CrossRef]
- Raghuram, A.; Restrepo, A.; Safadjou, S.; Cooley, J.; Orloff, M.; Hardy, D.; Butler, S.; Koval, C.E. Invasive Fungal Infections Following Liver Transplantation: Incidence, Risk Factors, Survival, and Impact of Fluconazole-Resistant Candida parapsilosis (2003–2007). Liver Transpl. 2012, 18, 1100–1109. [Google Scholar] [CrossRef]
- Pacholczyk, M.J.; Lagiewska, B.; Lisik, W.; Wasiak, D.; Chmura, A. Invasive Fungal Infections Following Liver Transplantation—Risk Factors, Incidence and Outcome. Ann. Transpl. 2011, 16, 14–16. [Google Scholar] [CrossRef]
- Rogers, J.; Rohal, S.; Carrigan, D.R.; Kusne, S.; Knox, K.K.; Gayowski, T.; Wagener, M.M.; Fung, J.J.; Singh, N. Human Herpesvirus-6 in Liver Transplant Recipients: Role in Pathogenesis of Fungal Infections, Neurologic Complications, and Outcome. Transplantation 2000, 69, 2566–2573. [Google Scholar] [CrossRef]
- Karchmer, A.W.; Samore, M.H.; Hadley, S.; Collins, L.A.; Jenkins, R.L.; Lewis, W.D. Fungal Infections Complicating Orthotopic Liver Transplantation. Trans. Am. Clin. Climatol. Assoc. 1995, 106, 38. [Google Scholar]
- Phoompoung, P.; Herrera, S.; Pérez Cortés Villalobos, A.; Foroutan, F.; Orchanian-Cheff, A.; Husain, S. Risk Factors of Invasive Fungal Infections in Liver Transplant Recipients: A Systematic Review and Meta-Analysis. Am. J. Transpl. 2022, 22, 1213–1229. [Google Scholar] [CrossRef]
- Husain, S.; Tollemar, J.; Dominguez, E.A.; Baumgarten, K.; Humar, A.; Paterson, D.L.; Wagener, M.M.; Kusne, S.; Singh, N. Changes in the Spectrum and Risk Factors for Invasive Candidiasis in Liver Transplant Recipients: Prospective, Multicenter, Case-Controlled Study. Transplantation 2003, 75, 2023–2029. [Google Scholar] [CrossRef]
- Eschenauer, G.A.; Kwak, E.J.; Humar, A.; Potoski, B.A.; Clarke, L.G.; Shields, R.K.; Abdel-Massih, R.; Silveira, F.P.; Vergidis, P.; Clancy, C.J.; et al. Targeted versus Universal Antifungal Prophylaxis Among Liver Transplant Recipients. Am. J. Transpl. 2015, 15, 180–189. [Google Scholar] [CrossRef] [Green Version]
- Cruciani, M.; Mengoli, C.; Malena, M.; Bosco, O.; Serpelloni, G.; Grossi, P. Antifungal Prophylaxis in Liver Transplant Patients: A Systematic Review and Meta-Analysis. Liver Transpl. 2006, 12, 850–858. [Google Scholar] [CrossRef]
- Evans, J.D.W.; Morris, P.J.; Knight, S.R. Antifungal Prophylaxis in Liver Transplantation: A Systematic Review and Network Meta-Analysis. Am. J. Transpl. 2014, 14, 2765–2776. [Google Scholar] [CrossRef]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, e1–e50. [Google Scholar] [CrossRef] [Green Version]
- Husain, S.; Camargo, J.F. Invasive Aspergillosis in Solid-Organ Transplant Recipients: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transpl. 2019, 33, e13544. [Google Scholar] [CrossRef]
- Aslam, S.; Rotstein, C. Candida Infections in Solid Organ Transplantation: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transpl. 2019, 33, e13623. [Google Scholar] [CrossRef]
- Lortholary, O.; Renaudat, C.; Sitbon, K.; Madec, Y.; Denoeud-Ndam, L.; Wolff, M.; Fontanet, A.; Bretagne, S.; Dromer, F.; Bouges-Michel, C.; et al. Worrisome Trends in Incidence and Mortality of Candidemia in Intensive Care Units (Paris Area, 2002–2010). Intensive Care Med. 2014, 40, 1303–1312. [Google Scholar] [CrossRef] [Green Version]
- Gleason, T.G.; May, A.K.; Caparelli, D.; Farr, B.M.; Sawyer, R.G. Emerging Evidence of Selection of Fluconazole-Tolerant Fungi in Surgical Intensive Care Units. Arch. Surg. 1997, 132, 1197–1202. [Google Scholar] [CrossRef]
- Nguyen, M.H.; Peacock, J.E.; Morris, A.J.; Tanner, D.C.; Nguyen, M.L.; Snydman, D.R.; Wagener, M.M.; Rinaldi, M.G.; Yu, V.L. The Changing Face of Candidemia: Emergence of Non-Candida Albicans Species and Antifungal Resistance. Am. J. Med. 1996, 100, 617–623. [Google Scholar] [CrossRef]
- Rocco, T.R.; Reinert, S.E.; Simms, H.H. Effects of Fluconazole Administration in Critically Ill Patients: Analysis of Bacterial and Fungal Resistance. Arch. Surg. 2000, 135, 160–165. [Google Scholar] [CrossRef] [Green Version]
- Singh, N.; Wagener, M.M.; Cacciarelli, T.V.; Levitsky, J. Antifungal Management Practices in Liver Transplant Recipients. Am. J. Transpl. 2008, 8, 426–431. [Google Scholar] [CrossRef]
- Pappas, P.G.; Silveira, F.P. Candida in Solid Organ Transplant Recipients. Am. J. Transpl. 2009, 9 (Suppl. S4), S173–S179. [Google Scholar] [CrossRef]
- Singh, N.; Husain, S. Invasive Aspergillosis in Solid Organ Transplant Recipients. Am. J. Transpl. 2009, 9 (Suppl. S4), S180–S191. [Google Scholar] [CrossRef]
- Saliba, F.; Pascher, A.; Cointault, O.; Laterre, P.-F.; Cervera, C.; Waele, J.J.; de Cillo, U.; Langer, R.M.; Lugano, M.; Göran-Ericzon, B.; et al. Randomized Trial of Micafungin for the Prevention of Invasive Fungal Infection in High-Risk Liver Transplant Recipients. Clin. Infect. Dis. 2015, 60, 997. [Google Scholar] [CrossRef] [PubMed]
- Cornely, O.A.; Bassetti, M.; Calandra, T.; Garbino, J.; Kullberg, B.J.; Lortholary, O.; Meersseman, W.; Akova, M.; Arendrup, M.C.; Arikan-Akdagli, S.; et al. ESCMID* Guideline for the Diagnosis and Management of Candida Diseases 2012: Non-Neutropenic Adult Patients. Clin. Microbiol. Infect. 2012, 18 (Suppl. S7), 19–37. [Google Scholar] [CrossRef] [Green Version]
- Glöckner, A. Treatment and Prophylaxis of Invasive Candidiasis with Anidulafungin, Caspofungin and Micafungin: Review of the Literature. Eur. J. Med. Res. 2011, 16, 167–179. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.C.A.; Slavin, M.A.; Sorrell, T.C. Echinocandin Antifungal Drugs in Fungal Infections: A Comparison. Drugs 2011, 71, 11–41. [Google Scholar] [CrossRef]
- Eschenauer, G.; DePestel, D.D.; Carver, P.L. Comparison of Echinocandin Antifungals. Ther. Clin. Risk Manag. 2007, 3, 71–97. [Google Scholar] [CrossRef] [Green Version]
- Hebert, M.F.; Townsend, R.W.; Austin, S.; Balan, G.; Blough, D.K.; Buell, D.; Keirns, J.; Bekersky, I. Concomitant Cyclosporine and Micafungin Pharmacokinetics in Healthy Volunteers. J. Clin. Pharmacol. 2005, 45, 954–960. [Google Scholar] [CrossRef]
- Fukuoka, N.; Imataki, O.; Ohnishi, H.; Kitanaka, A.; Kubota, Y.; Ishida, T.; Tanaka, T. Micafungin Does Not Influence the Concentration of Tacrolimus in Patients after Allogeneic Hematopoietic Stem Cell Transplantation. Transpl. Proc. 2010, 42, 2725–2730. [Google Scholar] [CrossRef]
- Inoue, Y.; Saito, T.; Ogawa, K.; Nishio, Y.; Kosugi, S.; Suzuki, Y.; Kato, M.; Sakai, T.; Takahashi, M.; Miura, I. Drug Interactions between Micafungin at High Doses and Cyclosporine A in Febrile Neutropenia Patients after Allogeneic Hematopoietic Stem Cell Transplantation. Int. J. Clin. Pharmacol. Ther. 2012, 50, 831–837. [Google Scholar] [CrossRef]
- Hebert, M.F.; Blough, D.K.; Townsend, R.W.; Allison, M.; Buell, D.; Keirns, J.; Bekersky, I. Concomitant Tacrolimus and Micafungin Pharmacokinetics in Healthy Volunteers. J. Clin. Pharmacol. 2005, 45, 1018–1024. [Google Scholar] [CrossRef]
- Muhl, E.; Martens, T.; Iven, H.; Rob, P.; Bruch, H.P. Influence of Continuous Veno-Venous Haemodiafiltration and Continuous Veno-Venous Haemofiltration on the Pharmacokinetics of Fluconazole. Eur. J. Clin. Pharmacol. 2000, 56, 671–678. [Google Scholar] [CrossRef]
- Liu, Y.; Lan, C.; Qin, S.; Qin, Z.; Zhang, Z.; Zhang, P.; Cao, W. Efficacy of Anti-Fungal Agents for Invasive Fungal Infection Prophylaxis in Liver Transplant Recipients: A Network Meta-Analysis. Mycoses 2022, 65, 906–917. [Google Scholar] [CrossRef]
- Peter Donnelly, J.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Bassetti, M.; Azoulay, E.; Kullberg, B.J.; Ruhnke, M.; Shoham, S.; Vazquez, J.; Giacobbe, D.R.; Calandra, T. EORTC/MSGERC Definitions of Invasive Fungal Diseases: Summary of Activities of the Intensive Care Unit Working Group. Clin. Infect. Dis. 2021, 72, S121–S127. [Google Scholar] [CrossRef]
- Blot, S.I.; Vandewoude, K.H.; de Waele, J.J. Candida Peritonitis. Curr. Opin. Crit. Care 2007, 13, 195–199. [Google Scholar] [CrossRef]
- Montravers, P.; Dupont, H.; Eggimann, P. Intra-Abdominal Candidiasis: The Guidelines—Forgotten Non-Candidemic Invasive Candidiasis. Intensive Care Med. 2013, 39, 2226–2230. [Google Scholar] [CrossRef] [Green Version]
- Carneiro, H.A.; Mavrakis, A.; Mylonakis, E. Candida Peritonitis: An Update on the Latest Research and Treatments. World J. Surg. 2011, 35, 2650–2659. [Google Scholar] [CrossRef]
- Cornely, O.A.; Hoenigl, M.; Lass-Flörl, C.; Chen, S.C.A.; Kontoyiannis, D.P.; Morrissey, C.O.; Thompson, G.R. Defining Breakthrough Invasive Fungal Infection-Position Paper of the Mycoses Study Group Education and Research Consortium and the European Confederation of Medical Mycology. Mycoses 2019, 62, 716–729. [Google Scholar] [CrossRef]
- Arendrup, M.C.; Cuenca-Estrella, M.; Lass-Fl€, C.; Hope, W.W. EUCAST Technical Note on Candida and Micafungin, Anidulafungin and Fluconazole. Mycoses 2014, 57, 377–379. [Google Scholar] [CrossRef]
- Sabol, K.; Gumbo, T. Anidulafungin in the Treatment of Invasive Fungal Infections. Ther. Clin. Risk Manag. 2008, 4, 71. [Google Scholar] [CrossRef] [Green Version]
- Aruanno, M.; Glampedakis, E.; Lamoth, F. Echinocandins for the Treatment of Invasive Aspergillosis: From Laboratory to Bedside. Antimicrob. Agents Chemother. 2019, 63, e00399-19. [Google Scholar] [CrossRef] [Green Version]
- Management of Invasive Candidiasis and Aspergillosis in Adults. Conférence de Consensus Commune Organisée Conjointement Par La SFAR, La SPILF et La SRLF Avec La Participation de La Société Française D’Hématologie, de La Société Française de Mycologie Médicale et de La Société Française de Greffe de Mœlle. Rev. Pneumol. Clin. 2004, 60, 289–293. [Google Scholar]
- Boyer, A.; Cadier, G.; Accoceberry, I.; Lhomme, E.; Ricard, C.; Gruson, D.; Blanchard, E. Guidelines for Antifungal Therapies in Intensive Care Unit Patients: Not so Bad! Clin. Microbiol. Infect. 2019, 25, 1291–1292. [Google Scholar] [CrossRef]
- Cardini, B.; Oberhuber, R.; Fodor, M.; Hautz, T.; Margreiter, C.; Resch, T.; Scheidl, S.; Maglione, M.; Bösmüller, C.; Mair, H.; et al. Clinical Implementation of Prolonged Liver Preservation and Monitoring through Normothermic Machine Perfusion in Liver Transplantation. Transplantation 2020, 104, 1917–1928. [Google Scholar] [CrossRef]
- Nemes, B.; Gámán, G.; Polak, W.G.; Gelley, F.; Hara, T.; Ono, S.; Baimakhanov, Z.; Piros, L.; Eguchi, S. Extended Criteria Donors in Liver Transplantation Part I: Reviewing the Impact of Determining Factors. Expert Rev. Gastroenterol. Hepatol. 2016, 10, 827–839. [Google Scholar] [CrossRef] [Green Version]
- Andes, D.R.; Safdar, N.; Baddley, J.W.; Alexander, B.; Brumble, L.; Freifeld, A.; Hadley, S.; Herwaldt, L.; Kauffman, C.; Lyon, G.M.; et al. The Epidemiology and Outcomes of Invasive Candida Infections among Organ Transplant Recipients in the United States: Results of the Transplant-Associated Infection Surveillance Network (TRANSNET). Transpl. Infect. Dis. 2016, 18, 921–931. [Google Scholar] [CrossRef] [Green Version]
- Shields, R.K.; Nguyen, M.H.; Press, E.G.; Clancya, C.J. Abdominal Candidiasis Is a Hidden Reservoir of Echinocandin Resistance. Antimicrob. Agents Chemother. 2014, 58, 7601–7605. [Google Scholar] [CrossRef] [Green Version]
- Kullberg, B.J.; Arendrup, M.C. Invasive Candidiasis. N. Engl. J. Med. 2015, 373, 1445–1456. [Google Scholar] [CrossRef] [Green Version]
- Eschenauer, G.A.; Lam, S.W.; Carver, P.L. Antifungal Prophylaxis in Liver Transplant Recipients. Liver Transplant. 2009, 15, 842–858. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Prideaux, B.; Nagasaki, Y.; Lee, M.H.; Chen, P.Y.; Blanc, L.; Ho, H.; Clancy, C.J.; Nguyen, M.H.; Dartois, V.; et al. Unraveling Drug Penetration of Echinocandin Antifungals at the Site of Infection in an Intra-Abdominal Abscess Model. Antimicrob. Agents Chemother. 2017, 61, e01009-17. [Google Scholar] [CrossRef] [Green Version]
- Rodvold, K.A.; Yoo, L.; George, J.M. Penetration of Anti-Infective Agents into Pulmonaryepithelial Lining Fluid: Focus on Antifungal, Antitubercular and Miscellaneous Anti-Infective Agents. Clin. Pharmacokinet. 2011, 50, 689–704. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients (n = 100) | No b-IFI (n = 84) | b-IFI (n = 16) | p-Value |
|---|---|---|---|---|
| Age (years) | 55.8 ± 12.1 | 57.4 ± 10.8 | 47.7 ± 14.0 | 0.003 |
| Male sex | 75 (75.0) | 66 (78.6) | 9 (56.3) | 0.111 |
| Weight (kg) | 79 ± 18 | 80 ± 17 | 75 ± 21 | 0.290 |
| Height (cm) | 174 ± 9 | 174 ± 9 | 175 ± 9 | 0.759 |
| Body mass index (kg/m2) | 26.2 ± 5.5 | 26.5 ± 5.3 | 24.3 ± 6.0 | 0.150 |
| SAPS III score | 45.6 ± 8.1 | 45.8 ± 8.1 | 44.0 ± 8.4 | 0.458 |
| MELD score | 15 (6–40) | 15 (6–40) | 14.5 (9–40) | 0.777 |
| Charlson Comorbidity Index | 4 (0–10) | 4 (0–10) | 4 (0–8) | 0.980 |
| Underlying disease | ||||
| Cirrhosis—Alcoholic cirrhosis | 26 (26.0) | 21 (25.0) | 5 (31.3) | 0.559 |
| Malignancy and other tumors | 33 (33.0) | 29 (34.5) | 4 (25.0) | |
| Cirrhosis—Virus related | 5 (5.0) | 4 (4.8) | 1 (6.3) | |
| Cirrhosis—Nonalcoholic fatty liver cirrhosis | 5 (5.0) | 5 (6.0) | 0 (0.0) | |
| Acute hepatic failure | 10 (10.0) | 8 (9.5) | 2 (12.5) | |
| Cholestatic diseases | 12 (12.0) | 11 (13.1) | 1 (6.3) | |
| Cirrhosis—Autoimmune cirrhosis | 3 (3.0) | 2 (2.4) | 1 (6.3) | |
| Metabolic diseases | 4 (4.0) | 3 (3.6) | 1 (6.3) | |
| Other | 2 (2.0) | 1 (1.2) | 1 (6.3) | |
| Risk Factors | ||||
| MELD score >30 | 17 (17.0) | 14 (16.7) | 3 (18.8) | 1.000 |
| Fungal precolonization | 13 (13.0) | 10 (11.9) | 3 (18.8) | 0.432 |
| Prehospitalization | 26 (26.0) | 24 (28.6) | 2 (12.5) | 0.227 |
| SCr >2/ESRD | 14 (14.0) | 13 (15.5) | 1 (6.3) | 0.458 |
| Organ donation type | ||||
| Whole organ donation | 95 (95.0) | 82 (97.6) | 13 (81.3) | 0.028 |
| Split-liver donation | 5 (5.0) | 2 (2.4) | 3 (18.8) | |
| High urgency transplantation | 9 (9.0) | 7 (8.3) | 2 (12.5) | 0.633 |
| CMV status | 53 (54.1) | 47 (56.6) | 6 (40.0) | 0.270 |
| High risk (D+/R-) | 32 (34.8) | 28 (36.4) | 4 (26.7) | |
| Intermediate risk (D+/R+, D-/R+) | 33 (35.9) | 27 (35.1) | 6 (40.0) | 0.824 |
| Low risk (D-/R-) | 27 (29.3) | 22 (28.6) | 5 (33.3) | |
| Extended criteria donation | 75 (75.0) | 63 (75.0) | 12 (75.0) | 1.000 |
| Donor age (years) | 47.8 ± 16.1 | 48.6 ± 16.3 | 43.3 ± 15.1 | 0.229 |
| Donation death type | ||||
| DBD | 92 (92.0) | 77 (91.7) | 15 (93.8) | 1.000 |
| DCD | 8 (8.0) | 7 (8.3) | 1 (6.3) | |
| Organ preservation | ||||
| Static cold storage | 68 (68.0) | 55 (65.5) | 13 (81.3) | 0.257 |
| Normothermic machine perfusion | 32 (32.0) | 29 (34.5) | 3 (18.8) | |
| Total operation time (minutes) | 216 (175–754) | 384 (175–754) | 383 (188–614) | 0.840 |
| Cold ischemia time (minutes) | 474 (171–1199) | 470 (185–1199) | 385 (171–724) | 0.021 |
| Prolonged operation (≥10 h) | 2 (2.0) | 2 (2.4) | 0 (0.0) | 1.000 |
| Transfusion of ≥40 units PRBC | 2 (2.0) | 1 (1.2) | 1 (6.3) | 0.296 |
| Venous anastomosis | ||||
| Retrocaval resection | 94 (94.9) | 82 (97.6) | 12 (80.0) | 0.024 |
| Piggyback technique | 5 (5.1) | 2 (2.4) | 3 (20.0) | |
| Biliary anastomosis | ||||
| Duct-to-duct reconstruction | 90 (90.0) | 76 (90.5) | 14 (87.5) | 0.660 |
| Roux-en-Y choledochojejunostomy | 10 (10.0) | 8 (9.5) | 2 (12.5) |
| Patient Number | Sex | Ages (years) | Underlying Disease | Lab MELD Score | MELD Score >30 | Fungal Precolonization | Prehospitalization | Serum Creatinin >2 mg/dL | Split-Liver Transplantation | HU Transplantation | ECD | DCD | NMP | Prolonged Operation | Massive Transfusion | RYC | Dialysis | CMV Viremia | Bile Leak | ERCP | Reconstruction | RYC | Relaparotomy, Other | Early Retransplantation |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 50 | Cancers—Hepatocellular carcinoma and noncirrhotic liver | 7 | ● | ● | ● | ● | ● | |||||||||||||||
| 2 | F | 40 | Acute hepatic failure | 39 | ● | ● | ● | ● | ● | ● | ● | ● | ||||||||||||
| 3 | M | 61 | Cancers—Hepatocellular carcinoma and cirrhosis | 8 | ● | ● | ● | ● | ● | |||||||||||||||
| 4 | M | 60 | Cirrhosis—Alcoholic cirrhosis | 13 | ● | ● | ● | ● | ||||||||||||||||
| 5 | M | 58 | Cancers—Hepatocellular carcinoma and cirrhosis | 13 | ● | ● | ||||||||||||||||||
| 6 | M | 36 | Cholestasis disease-Others: secondary sclerosing cholangitis | 35 | ● | ● | ● | ● | ● | ● | ● | ● | ||||||||||||
| 7 | F | 24 | Metabolic disease-Others: MNGIE | 9 | ● | ● | ● | ● | ● | ● | ||||||||||||||
| 8 | F | 57 | Cirrhosis—Alcoholic cirrhosis | 10 | ● | ● | ● | ● | ||||||||||||||||
| 9 | F | 22 | Metabolic diseases-Wilson disease | 22 | ● | ● | ||||||||||||||||||
| 10 | M | 62 | Cancers—Hepatocellular carcinoma and cirrhosis | 11 | ||||||||||||||||||||
| 11 | F | 57 | Cirrhosis—Virus C-related cirrhosis | 9 | ● | ● | ● | |||||||||||||||||
| 12 | M | 67 | Acute hepatic failure | 40 | ● | ● | ● | ● | ● | ● | ● | ● | ||||||||||||
| 13 | M | 48 | Cirrhosis—Alcoholic cirrhosis | 13 | ● | ● | ● | ● | ● | |||||||||||||||
| 14 | M | 53 | Cirrhosis—Alcoholic cirrhosis | 18 | ● | ● | ● | ● | ● | |||||||||||||||
| 15 | M | 29 | Cholestatic disease-Primary sclerosing cholangitis | 25 | ● | ● | ● | |||||||||||||||||
| 16 | M | 60 | Cirrhosis—Alcoholic cirrhosis | 22 | ● | ● | ● | ● | ● | ● | ||||||||||||||
| 17 | F | 65 | Acute hepatic failure | 37 | ● | ● | ● | ● | ● | ● | ||||||||||||||
| 18 | M | 56 | Cholestasis disease—Others: secondary biliary cirrhosis | 17 | ● | ● | ● | ● | ● | ● | ● | ● | ||||||||||||
| 19 | F | 55 | Cirrhosis—Autoimmune cirrhosis | 16 | ● | ● | ● | ● | ● | ● | ● | ● |
| Nondependent Variable | B-Coefficient | p-Value | HR | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Age (years) | −0.043 | 0.035 | 0.96 | 0.92 | 0.99 |
| Cold ischemia time (minutes) | 0.001 | 0.338 | 1.00 | 1.00 | 1.00 |
| Piggyback operative technique | 1.008 | 0.331 | 2.74 | 0.36 | 20.96 |
| Split-liver transplantation | 1.383 | 0.116 | 3.99 | 0.71 | 22.42 |
| Donor-derived infection | 2.478 | 0.003 | 11.92 | 2.35 | 60.30 |
| Relaparotomy, any reason | 1.016 | 0.127 | 2.76 | 0.75 | 10.19 |
| Patient Number | Prophylaxis (Duration) | Fungal Pathogen | Type of Infection (Diagnosis day) | Definition of IFI | Donor-Derived Infection | Clinical Symptoms | Radiological Abnormalities | Histopathologic Examination | Culture Blood | Culture Catheter | PCR in Blood | Culture Abdominal Specimen | PCR in Abdominal Specimen | Culture BALF | PCR in BALF | Galactomannan in BALF | Fundoscopy | PCR Biopsy | Culture Urine | Therapeutic Regimen | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M (12) | C. albicans | Fungemia, Peritonitis (12) | P | ● | ● | ● | ● | 1. Voriconazol 2. Amphotericin | Survived, graft failure d56, and Re-TX d58 | |||||||||||
| 2 | M (12) | C. krusei | Fungemia, Peritonitis (12) | P | ● | ● | ● | ● | ● | ● | Anidulafungin | Death, sepsis at d39 (ICU) | |||||||||
| 3 | M (3) | C. albicans | Peritonitis (3) | PR | ● | ● | ● | Voriconazol | Survived, graft failure d2, Re-TX d2 | ||||||||||||
| 4 | M (1) | C. albicans | Peritonitis (14) | P | ● | ● | ● | ● | Micafungin | Survived | |||||||||||
| 5 | M (40) | A. fumigatus | Pneumonia (42) | P | ● | ● | ●1 | ● | ● | ● | 1. Voriconazol 2. Amphotericin | Death, sepsis at d110 | |||||||||
| 6 | M (8) | C. dubliniensis | Peritonitis (8) | P | ● | ● | ● | ● | ● | 1. Voriconazol 2. Amphotericin | Death, sepsis at d116 | ||||||||||
| 7 | M (9) | C. krusei | Peritonitis (10) | P | ● | ● | ● | ● | Micafungin | Death, sepsis at d48 (hospital) | |||||||||||
| 8 | M (7) | C. albicans | Peritonitis (26) | P | ● | ● | ● | Micafungin | Survived | ||||||||||||
| 9 | M (1) | C. albicans | Peritonitis (4) | P | ● | ● | ● | ● | Micafungin | Survived | |||||||||||
| 10 | M (1) | C. albicans | Peritonitis (13) | PR | ● | ● | Micafungin | Death, sepsis at d221 (hospital) | |||||||||||||
| 11 | M (1) | Saccharomyces spp. | Peritonitis (55) | P | ● | ● | ● | Micafungin | Survived | ||||||||||||
| 12 | A (14) | C. glabrata | Fungemia, Peritonitis (38) | P | ● | ● | ● | ● | ● | ● | ● | ● | Isovuconazol | Death, sepsis at d43 (ICU) | |||||||
| 13 | A (1) | C. dubliniensis | Peritonitis (37) | PR | ● | ● | Anidulafungin | Survived | |||||||||||||
| 14 | A (21) | C. parapsilosis | Peritonitis (21) | P | ● | ● | ● | Voriconazol | Death, sepsis at d38 (ICU) | ||||||||||||
| 15 | A (20) | C. glabrata | Fungemia, catheter-related (44) | P | ● | ● | ● | Anidulafungin | Graft failure d62, Re-TX d160. Death, sepsis at d329 | ||||||||||||
| 16 | A (13) | C. krusei | Peritonitis (13) | P | ● | ● | ● | Anidulafungin | Survived | ||||||||||||
| 17 | A (8) | C. glabrata | Fungemia, Peritonitis (8) | P | ● | ● | ● | ● | ● | Fluconazol and Amphotericin | Graft failure d10, Re-TX d11. Death, sepsis at d91 (ICU) | ||||||||||
| 18 | A (17) | C. glabrata | Fungemia, catheter-related (77) | P | ● | ● | ● | ● | Anidulafungin | Survived, graft failure d2, Re-TX d4 | |||||||||||
| 19 | A (15) | A. fumigatus | Pneumonia (26) | P | ● | ● | ● | ● | ● | ● | ● | Anidulafungin | Death, sepsis at d26 (ICU) |
| Outcome | All Patients (n = 100) | No b-IFI (n = 84) | b-IFI (n = 16) | p-Value |
|---|---|---|---|---|
| Superficial fungal infections (mucosal) | 11 (11.0) | 11 (13.1) | 0 (0.0) | 0.207 |
| Length of ICU stay (days) | 7.0 (2–117) | 6.5 (2–45) | 18.0 (3–117) | 0.054 |
| Postoperative dialysis | 61 (61.0) | 49 (58.3) | 12 (75.0) | 0.270 |
| Postoperative CMV viremia | 37 (37.0) | 33 (39.3) | 4 (25.0) | 0.399 |
| Reoperations | ||||
| Bile leakage | 30 (30.0) | 19 (22.6) | 11 (68.8) | 0.001 |
| Endoscopic retrograde cholangiopancreatography | 1 (1.0) | 1 (1.2) | 0 (0.0) | 1.000 |
| Reconstruction | 22 (22.0) | 13 (15.5) | 9 (56.3) | 0.001 |
| Secondary Roux-en-Y choledochojejunostomy | 7 (7.0) | 4 (4.8) | 3 (18.8) | 0.079 |
| Early retransplantation (<90 days) | 6 (6.0) | 3 (3.6) | 3 (18.8) | 0.050 |
| Other | 29 (29.0) | 26 (31.0) | 3 (18.8) | 0.385 |
| Mortality within 90 days | 11 (11.0) | 7 (8.3) | 4 (25.0) | 0.073 |
| Mortality during ICU stay | 12 (12.0) | 6 (7.1) | 6 (37.5) | 0.003 |
| 1-year Patient Survival | 81 (81.0) | 73 (86.9) | 8 (50.0) | 0.002 |
| 1-year Death-Censored Graft Survival | 76 (93.8) | 70 (95.9) | 6 (75.0) | 0.074 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Breitkopf, R.; Treml, B.; Senoner, T.; Bukumirić, Z.; Rajsic, S. Invasive Fungal Breakthrough Infections under Targeted Echinocandin Prophylaxis in High-Risk Liver Transplant Recipients. J. Fungi 2023, 9, 272. https://doi.org/10.3390/jof9020272
Breitkopf R, Treml B, Senoner T, Bukumirić Z, Rajsic S. Invasive Fungal Breakthrough Infections under Targeted Echinocandin Prophylaxis in High-Risk Liver Transplant Recipients. Journal of Fungi. 2023; 9(2):272. https://doi.org/10.3390/jof9020272
Chicago/Turabian StyleBreitkopf, Robert, Benedikt Treml, Thomas Senoner, Zoran Bukumirić, and Sasa Rajsic. 2023. "Invasive Fungal Breakthrough Infections under Targeted Echinocandin Prophylaxis in High-Risk Liver Transplant Recipients" Journal of Fungi 9, no. 2: 272. https://doi.org/10.3390/jof9020272