
Meningeal Sporotrichosis Due to Sporothrix brasiliensis: A 21-Year Cohort Study from a Brazilian Reference Center
 , , , , , ,
, , , , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patients with Disseminated Sporotrichosis (Groups 1 and 2)
3.2. Patients with CNS Sporotrichosis (Group 1)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oliveira, M.M.E.; Almeida-Paes, R.; Gutierrez-Galhardo, M.C.; Zancope-Oliveira, R.M. Molecular identification of the Sporothrix schenckii complex. Rev. Iberoam. Micol. 2014, 31, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.M.; de Melo Teixeira, M.; de Hoog, G.S.; Schubach, T.M.; Pereira, S.A.; Fernandes, G.F.; Bezerra, L.M.; Felipe, M.S.; de Camargo, Z.P. Phylogenetic analysis reveals a high prevalence of Sporothrix brasiliensis in feline sporotrichosis outbreaks. PLoS Negl. Trop. Dis. 2013, 7, e2281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arrillaga-Moncrieff, I.; Capilla, J.; Mayayo, E.; Marimon, R.; Mariné, M.; Gené, J.; Cano, J.; Guarro, J. Different virulence levels of the species of Sporothrix in a murine model. Clin. Microbiol. Infect. 2009, 15, 651–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García Carnero, L.C.; Lozoya Pérez, N.E.; González Hernández, S.E.; Martínez Álvarez, J.A. Immunity and treatment of sporotrichosis. J. Fungi 2018, 4, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shoemaker, E.H.; Bennett, H.D.; Fields, W.S.; Whitcomb, F.C.; Halpert, B. Leptomeningitis due to Sporotrichum schenckii. AMA Arch. Pathol. 1957, 64, 222–227. [Google Scholar]
- Scott, E.N.; Kaufman, L.; Brown, A.C.; Muchmore, H.G. Serologic studies in the diagnosis and management of meningitis due to Sporothrix schenckii. N. Engl. J. Med. 1987, 317, 935–940. [Google Scholar] [CrossRef]
- Freitas, D.F.S.; Lima, M.A.; de Almeida-Paes, R.; Lamas, C.C.; do Valle, A.C.; Oliveira, M.M.; Zancopé-Oliveira, R.M.; Gutierrez-Galhardo, M.C. Sporotrichosis in the central nervous system caused by Sporothrix brasiliensis. Clin. Infect. Dis. 2015, 61, 663–664. [Google Scholar] [CrossRef] [Green Version]
- Galhardo, M.C.G.; Silva, M.T.T.; Lima, M.A.; Nunes, E.P.; Schettini, L.E.; de Freitas, R.F.; Paes, R.A.; Neves, E.S.; do Valle, A.C. Sporothrix schenckii meningitis in AIDS during immune reconstitution syndrome. J. Neurol. Neurosurg. Psychiatry 2010, 81, 696–699. [Google Scholar] [CrossRef]
- Amirali, M.H.; Liebenberg, J.; Pillay, S.; Nel, J. Sporotrichosis in renal transplant patients: Two case reports and a review of the literature. J. Med. Case Rep. 2020, 14, 79. [Google Scholar] [CrossRef]
- Hessler, C.; Kauffman, C.A.; Chow, F.C. The upside of bias: A case of chronic meningitis due to Sporothrix Schenckii in an immunocompetent host. Neurohospitalist 2016, 7, 30–34. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, A.M.; de Hoog, G.S.; de Camargo, Z.P. Molecular diagnosis of pathogenic Sporothrix species. PLoS Negl. Trop. Dis. 2015, 9, e0004190. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.M.E.; Muniz, M.M.; Almeida-Paes, R.; Zancope-Oliveira, R.M.; Freitas, A.D.; Lima, M.A.; Gutierrez-Galhardo, M.C.; Freitas, D.F.S. Cerebrospinal fluid PCR: A new approach for the diagnosis of CNS sporotrichosis. PLoS Negl. Trop. Dis. 2020, 14, e0008196. [Google Scholar] [CrossRef] [PubMed]
- Almeida-Paes, R.; de Oliveira, M.M.E.; Freitas, D.F.S.; do Valle, A.C.F.; Zancopé-Oliveira, R.M.; Gutierrez-Galhardo, M.C. Sporotrichosis in Rio de Janeiro, Brazil: Sporothrix brasiliensis is associated with atypical clinical presentations. PLoS Negl. Trop. Dis. 2014, 8, e3094. [Google Scholar] [CrossRef] [Green Version]
- Lima, M.A.; Vallier, R.; Silva, M.M. Sporothrix brasiliensis meningitis in an immunocompetent patient. Pract. Neurol. 2021, 21, 241–242. [Google Scholar] [CrossRef]
- Marra, C.M.; Maxwell, C.L.; Collier, A.C.; Robertson, K.R.; Imrie, A. Interpreting cerebrospinal fluid pleocytosis in HIV in the era of potent antiretroviral therapy. BMC Infect. Dis. 2007, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Aksamit, A.J. Chronic Meningitis. N. Engl. J. Med. 2021, 385, 930–936. [Google Scholar] [CrossRef] [PubMed]
- Kauffman, C.A. Central nervous system infection with other endemic mycoses: Rare manifestation of blastomycosis, paracoccidioidomycosis, talaromycosis, and sporotrichosis. J. Fungi 2019, 5, 64. [Google Scholar] [CrossRef] [Green Version]
- Scott, E.N.; Muchmore, H.G. Immunoblot analysis of antibody responses to Sporothrix schenckii. J. Clin. Microbiol. 1989, 27, 300–304. [Google Scholar] [CrossRef] [Green Version]
- Donabedian, H.; O’Donnell, E.; Olszewski, C.; MacArthur, R.D.; Budd, N. Disseminated cutaneous and meningeal sporotrichosis in an AIDS patient. Diagn. Microbiol. Infect. Dis. 1994, 18, 111–115. [Google Scholar] [CrossRef]
- Duani, H.; Palmerston, M.F.; Rosa Júnior, J.F.; Ribeiro, V.T.; Alcântara Neves, P.L. Meningeal and multiorgan disseminated sporotrichosis: A case report and autopsy study. Med. Mycol. Case Rep. 2019, 26, 47–52. [Google Scholar] [CrossRef]
- Bowen, L.; Nath, A.; Smith, B. CNS immune reconstitution inflammatory syndrome. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2018; pp. 167–176. [Google Scholar] [CrossRef]
- Johnson, T.P.; Nath, A. New insights into immune reconstitution inflammatory syndrome of the central nervous system. Curr. Opin. HIV AIDS 2014, 9, 572–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riveiro-Barciela, M.; Falcó, V.; Burgos, J.; Curran, A.; Van den Eynde, E.; Navarro, J.; Villar del Saz, S.; Ocaña, I.; Ribera, E.; Crespo, M.; et al. Neurological opportunistic infections and neurological immune reconstitution syndrome: Impact of one decade of highly active antiretroviral treatment in a tertiary hospital. HIV Med. 2013, 14, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Dai, L.; Mahajan, S.D.; Guo, C.; Zhang, T.; Wang, W.; Li, T.; Jiang, T.; Wu, H.; Li, N. Spectrum of central nervous system disorders in hospitalized HIV/AIDS patients (2009–2011) at a major HIV/AIDS referral center in Beijing, China. J. Neurol. Sci. 2014, 342, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Kauffman, C.A.; Bustamante, B.; Chapman, S.W.; Pappas, P.G.; Infectious Diseases Society of America. Clinical practice guidelines for the management of sporotrichosis: 2007 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2007, 45, 1255–1265. [Google Scholar] [CrossRef] [Green Version]
- Thompson, G.R.; Le, T.; Chindamporn, A.; Kauffman, C.A.; Alastruey-Izquierdo, A.; Ampel, N.M.; Andes, D.R.; Armstrong-James, D.; Ayanlowo, O.; Baddley, J.W.; et al. Global guideline for the diagnosis and management of the endemic mycoses: An initiative of the European Confederation of Medical Mycology in cooperation with the International Society for Human and Animal Mycology. Lancet Infect. Dis. 2021, 21, e364–e374. [Google Scholar] [CrossRef]
- Yuan, L.; Chen, F.; Sun, Y.; Zhang, Y.; Ji, X.; Jin, B. Candida meningitis in an infant after abdominal surgery successfully treated with intrathecal and intravenous amphotericin B: A case report. Medicine 2021, 100, e27205. [Google Scholar] [CrossRef]
- Jackson, N.R.; Blair, J.E.; Ampel, N.M. Central nervous system infections due to coccidioidomycosis. J. Fungi 2019, 5, 54. [Google Scholar] [CrossRef] [Green Version]
- Gullberg, R.M.; Quintanilla, A.; Levin, M.L.; Williams, J.; Phair, J.P. Sporotrichosis: Recurrent cutaneous, articular, and central nervous system infection in a renal transplant recipient. Rev. Infect. Dis. 1987, 9, 369–375. [Google Scholar] [CrossRef]
- Rodrigues, A.M.; de Hoog, G.S.; de Cássia Pires, D.; Brihante, R.S.; Sidrim, J.J.; Gadelha, M.F.; Colombo, A.L.; de Camargo, Z.P. Genetic diversity and antifungal susceptibility profiles in causative agents of sporotrichosis. BMC Infect. Dis. 2014, 14, 219. [Google Scholar] [CrossRef] [Green Version]
- Ottonelli Stopiglia, C.D.; Magagnin, C.M.; Castrillón, M.R.; Mendes, S.D.; Heidrich, D.; Valente, P.; Scroferneker, M.L. Antifungal susceptibilities and identification of species of the Sporothrix schenckii complex isolated in Brazil. Med. Mycol. 2014, 52, 56–64. [Google Scholar] [CrossRef]
- Wiederhold, N.P.; Pennick, G.J.; Dorsey, S.A.; Furmaga, W.; Lewis, J.S.; Patterson, T.F.; Sutton, D.A.; Fothergill, A.W. A reference laboratory experience of clinically achievable voriconazole, posaconazole, and itraconazole concentrations within the bloodstream and cerebral spinal fluid. Antimicrob. Agents Chemother. 2014, 58, 424–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calcagno, A.; Baietto, L.; De Rosa, F.G.; Tettoni, M.C.; Libanore, V.; Bertucci, R.; D’Avolio, A.; Di Perri, G. Posaconazole cerebrospinal concentrations in an HIV-infected patient with brain mucormycosis. J. Antimicrob. Chemother. 2011, 66, 224–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinwald, M.; Uharek, L.; Lampe, D.; Grobosch, T.; Thiel, E.; Schwartz, S. Limited penetration of posaconazole into cerebrospinal fluid in an allogeneic stem cell recipient with invasive pulmonary aspergillosis. Bone Marrow Transplant. 2009, 44, 269–270. [Google Scholar] [CrossRef] [Green Version]
- Rüping, M.J.G.T.; Albermann, N.; Ebinger, F.; Burckhardt, I.; Beisel, C.; Müller, C.; Vehreschild, J.J.; Kochanek, M.; Fätkenheuer, G.; Bangard, C.; et al. Posaconazole concentrations in the central nervous system. J. Antimicrob. Chemother. 2008, 62, 1468–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paixão, A.G.; Galhardo, M.C.G.; Almeida-Paes, R.; Nunes, E.P.; Gonçalves, M.L.C.; Chequer, G.L.; Lamas, C.D.C. The difficult management of disseminated Sporothrix brasiliensis in a patient with advanced AIDS. AIDS Res. Ther. 2015, 12, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mario, D.N.; Guarro, J.; Santurio, J.M.; Alves, S.H.; Capilla, J. In vitro and in vivo efficacy of amphotericin B combined with posaconazole against experimental disseminated sporotrichosis. Antimicrob. Agents Chemother. 2015, 59, 5018–5021. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group 1 (n = 17) | Group 2 (n = 36) | |
|---|---|---|
| Mean age in years (range) | 35.3 (20–57) | 43 (16–72) |
| Male—n (%) | 15 (88.2%) | 29 (80.6%) |
| Non-white skin color—n (%) | 16 (94.1%) | 24 (66.7%) |
| Close contact with cats—n (%) | 12 (70.6 %) | 28 (77.8%) |
| Immunosuppression—n (%) | ||
| HIV infection | 15 (88.2%) | 27 (75%) |
| Alcoholism | 1 (5.9%) | 2 (5.6%) |
| Chronic steroid use | 1 (5.9%) | 4 (11.1%) |
| None of the above | - | 3 (8.3%) |
| Mean duration of signs/symptoms until lumbar puncture in months (range) | 6.9 (1–20) | 7.4 (1–67) |
| Mean CSF cells/mm3 (range) | 71.5 (3–363) | 2 (0–5) |
| Mean CSF glucose mg/dL (range) | 39.6 (14–65) | 59.1 (27–148) |
| Mean CSF protein mg/dL (range) | 117 (32.3–307) | 50.1 (13–181) |
| Mean duration of first hospital admission in days (range) | 45.1 (10–120) | 28.2 (1–86) |
| ICU admission—n (%) | 6 (35.3%) | 0 |
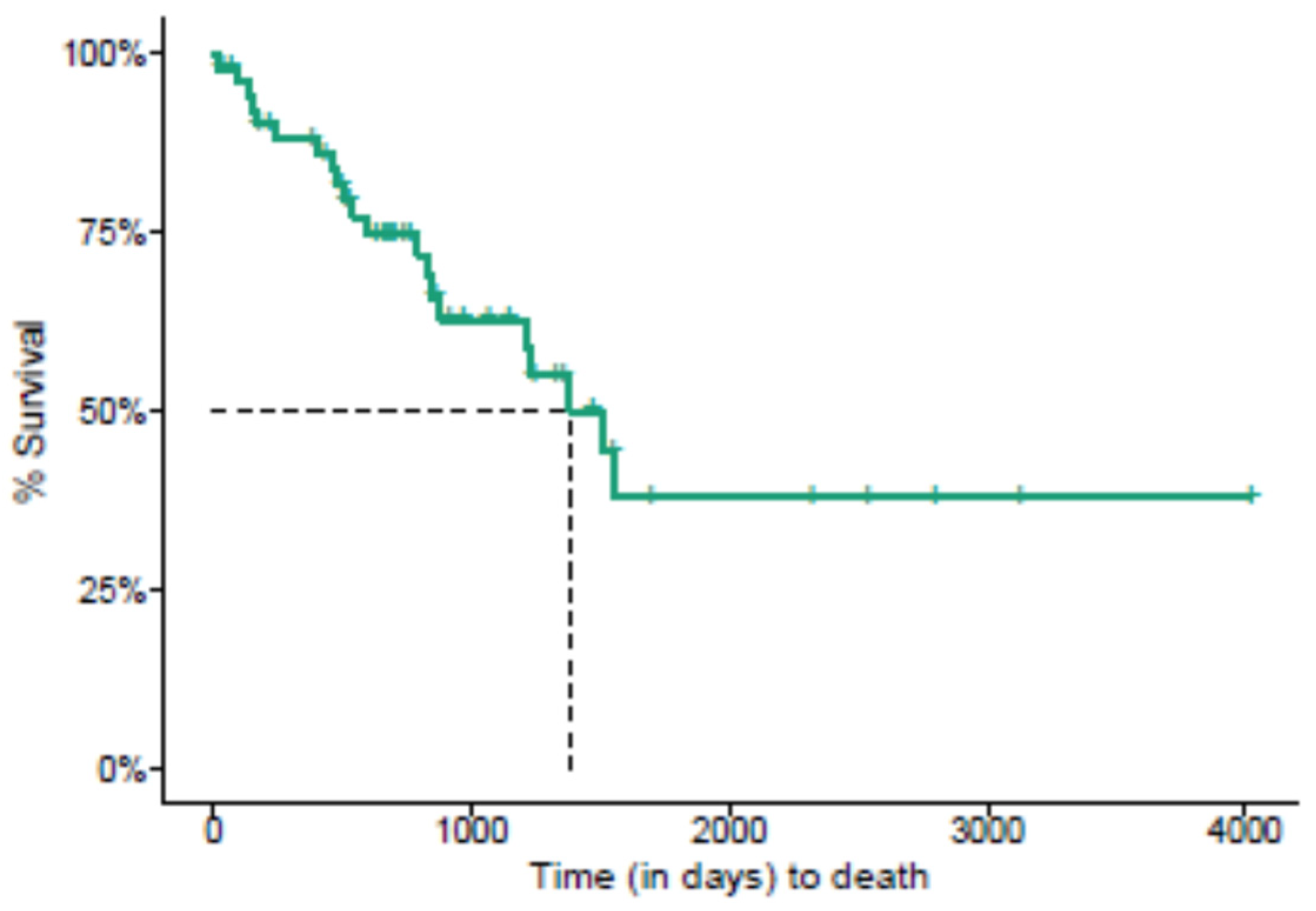
| Death—n (%) | 11 (64.7%) | 10 (27.8%) |
| Levels | n (%) | HR (Crude) | HR (Adjusted) | |
|---|---|---|---|---|
| Sex | Female Male | 9 (17) 44 (83) | 0.72 (0.2–2.58, p = 0.609) | 0.79 (0.21–3, p = 0.733) |
| Skin color | White Non-white | 13 (24.5) 40 (75.5) | 1.7 (0.49–5.98, p = 0.406) | 0.95 (0.23–3.87, p = 0.945) |
| Age | Mean (SD) | 40.5 (12.5) | 1 (0.95–1.04, p = 0.92) | 1.02 (0.96–1.07, p = 0.548) |
| Time of onset | ≤3 months >3 months | 22 (41.5) 31 (58.5) | 1.27 (0.5–3.22, p = 0.608) | 0.72 (0.25–2.11, p = 0.554) |
| Meningitis | No Yes | 36 (67.9) 17 (32.1) | 3 (1.24–7.26, p = 0.015) | 3.87 (1.23–12.17, p = 0.021) |
| HIV infection | No Yes | 11 (20.8) 42 (79.2) | 0.55 (0.17–1.79, p = 0.323) | 0.67 (0.2–2.29, p = 0.521) |
| Patient | Sex/Age a (yo) | Predisposing Condition | Duration of Neurological Symptoms | Clinical Manifestations | Initial CSF Findings | CSF Sporothrix spp. Detection b | Radiological Features | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|
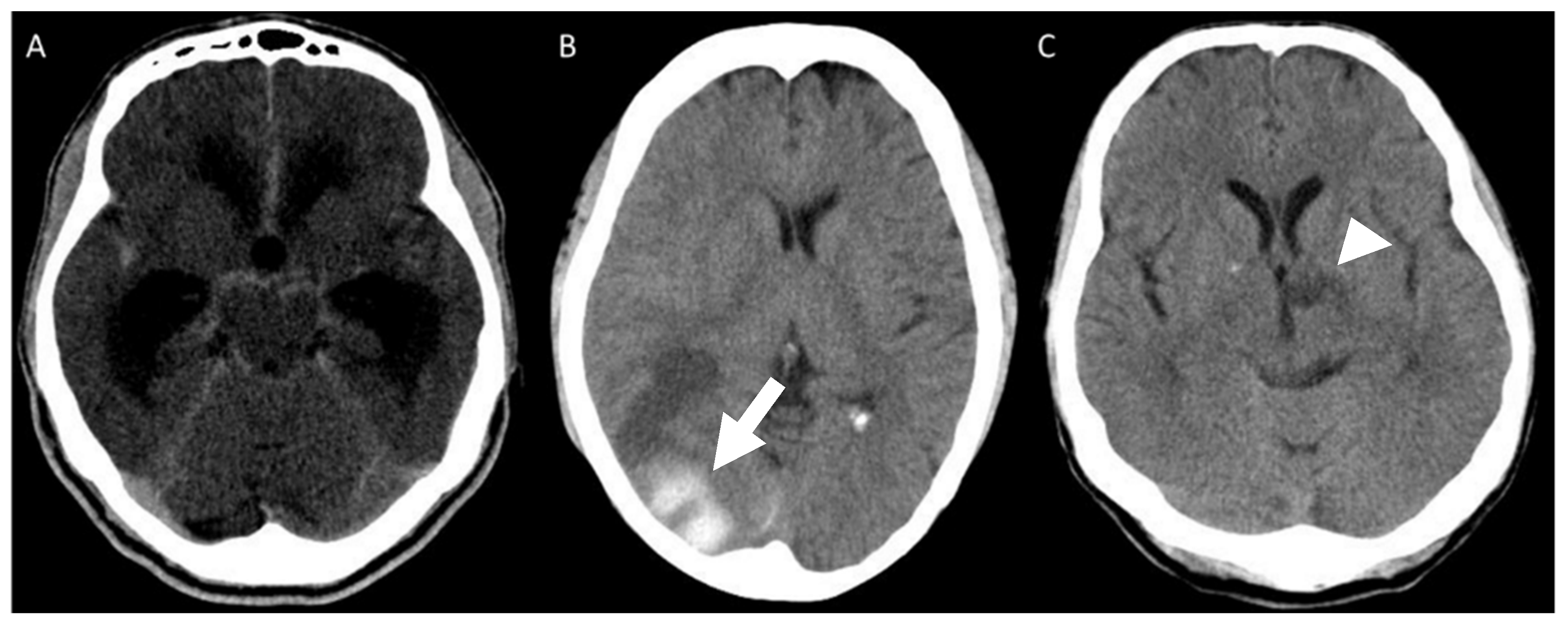
| 1 | M/44 | HIV infection | 15 days | Headache, right III nerve palsy, cognitive complaints | 363 cells/mm3 (91%MN), P: 410 mg/dL; G: 31 mg/dL | Positive Sporothrix spp. PCR | Left thalamus ischemic stroke | AmB + posaconazole | Deceased |
| 2 | M/57 | HIV infection | 1 month | Headache | 90 cells/mm3 (100%MN), P: 63.9 mg/dL; G:48 mg/dL | No | None | AmB + posaconazole | Ongoing treatment (AmB) |
| 3 | M/28 | HIV infection | 2 months | Headache, vomiting, nuchal rigidity | 206 cells/mm3 (90%MN), P: 159 mg/dL; G: 24 mg/dL | No | Meningeal contrast enhancement | AmB | Cured |
| 4 | M/46 | HIV infection | 4 months | Headache, vomiting, nuchal rigidity, cognitive complaints | 12 cells/mm3 (86%MN), P: 293 mg/dL; G: 22 mg/dL | No | Hydrocephalus, right internal capsule ischemic stroke | AmB | Deceased |
| 5 | M/26 | HIV infection | 15 days | Headache, nuchal rigidity, lethargy, seizures | 6 cells/mm3 (100%MN), P: 307 mg/dL; G: 27 mg/dL | Positive culture | Hydrocephalus, meningeal contrast enhancement, and nodular lesion in the right cerebellar hemisphere | AmB | Deceased |
| 6 | M/37 | HIV infection | 1 month | Headache, seizures | 10 cells/mm3 (100%MN), P: 97.5 mg/dL; G: 52 mg/dL | No | None | Itraconazole | Deceased |
| 7 | M/41 | Alcoholism | 1 month | Drowsiness, nuchal rigidity | 79 cells/mm3 (78%MN), P: 162 mg/dL; G: 32 mg/dL | No | None | AmB | Deceased |
| 8 | M/48 | HIV infection | 15 days | Headache, vomiting, seizures | 4 cells/mm3 (98%MN), P: 61.6 mg/dL; G: 35 mg/dL | Positive culture | Hydrocephalus | AmB | Deceased |
| 9 | F/21 | HIV infection | 1 month | Headache, right VI nerve palsy, drowsiness, nuchal rigidity | 3 cells/mm3 (100%MN), P: 33 mg/dL; G: 59 mg/dL | Positive culture | Hydrocephalus, meningeal contrast enhancement | AmB + posaconazole | Deceased |
| 10 | M/40 | HIV infection | 2 months | Headache, vomiting, drowsiness, cognitive complaints | 12 cells/mm3 (97%MN), P: 32 mg/dL; G: 65 mg/dL | No | Hydrocephalus, meningeal contrast enhancement | AmB | Deceased |
| 11 | M/28 | Leprosy and chronic steroid use | 2 months | Headache | 133 cells/mm3 (37%MN), P: 278 mg/dL; G: 58 mg/dL | Positive culture | None | AmB | Asymptomatic but with persistent CSF abnormalities |
| 12 | F/31 | HIV infection | 1 month | Headache, vomiting, motor deficit, seizures, drowsiness | 25 cells/mm3 (90%MN), P: 61 mg/dL; G: 10 mg/dL | Positive Sporothrix spp. PCR | Hydrocephalus, meningeal, contrast enhancement, right parietal hemorrhagic stroke | AmB + posaconazole | Deceased |
| 13 | M/38 | HIV infection | 1 month | Vomiting, cognitive complaints | 86 cells/mm3 (64%MN), P: 74.2 mg/dL; G: 35 mg/dL | Positive culture | Hydrocephalus | AmB | Deceased |
| 14 | M/43 | HIV infection | 8 months | Headache, vomiting, VI nerve palsy, drowsiness | 15 cells/mm3 (100%MN), P: 47.5 mg/dL; G: 53 mg/dL | Positive Sporothrix spp. PCR | Hydrocephalus, meningeal contrast enhancement | AmB | Cured |
| 15 | M/23 | HIV infection | 15 months | Headache, vomiting, nuchal rigidity, drowsiness | 72 cells/mm3 (100%MN), P: 100 mg/dL; G: 34 mg/dL | Positive Sporothrix spp. PCR | Hydrocephalus, meningeal contrast enhancement | AmB + posaconazole | Cured |
| 16 | M/35 | HIV infection | 2 months | Headache, vomiting, drowsiness | 5 cells/mm3 (100%MN), P: 42.5 mg/dL; G: 57 mg/dL | Positive culture | None | AmB | Deceased |
| 17 | M/20 | HIV infection | 3 months | Headache | 86 cells/mm3 (75%MN), P: 68.6 mg/dL; G: 35 mg/dL | Positive culture | Meningeal contrast enhancement | AmB + posaconazole | Ongoing treatment (AmB) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lima, M.A.; Freitas, D.F.S.; Oliveira, R.V.C.; Fichman, V.; Varon, A.G.; Freitas, A.D.; Lamas, C.C.; Andrade, H.B.; Veloso, V.G.; Almeida-Paes, R.; et al. Meningeal Sporotrichosis Due to Sporothrix brasiliensis: A 21-Year Cohort Study from a Brazilian Reference Center. J. Fungi 2023, 9, 17. https://doi.org/10.3390/jof9010017
Lima MA, Freitas DFS, Oliveira RVC, Fichman V, Varon AG, Freitas AD, Lamas CC, Andrade HB, Veloso VG, Almeida-Paes R, et al. Meningeal Sporotrichosis Due to Sporothrix brasiliensis: A 21-Year Cohort Study from a Brazilian Reference Center. Journal of Fungi. 2023; 9(1):17. https://doi.org/10.3390/jof9010017
Chicago/Turabian StyleLima, Marco A., Dayvison F. S. Freitas, Raquel V. C. Oliveira, Vivian Fichman, Andréa G. Varon, Andréa D. Freitas, Cristiane C. Lamas, Hugo B. Andrade, Valdilea G. Veloso, Rodrigo Almeida-Paes, and et al. 2023. "Meningeal Sporotrichosis Due to Sporothrix brasiliensis: A 21-Year Cohort Study from a Brazilian Reference Center" Journal of Fungi 9, no. 1: 17. https://doi.org/10.3390/jof9010017