
Update on the Epidemiology, Diagnosis, and Treatment of Coccidioidomycosis

Abstract
:1. Introduction
2. Epidemiology
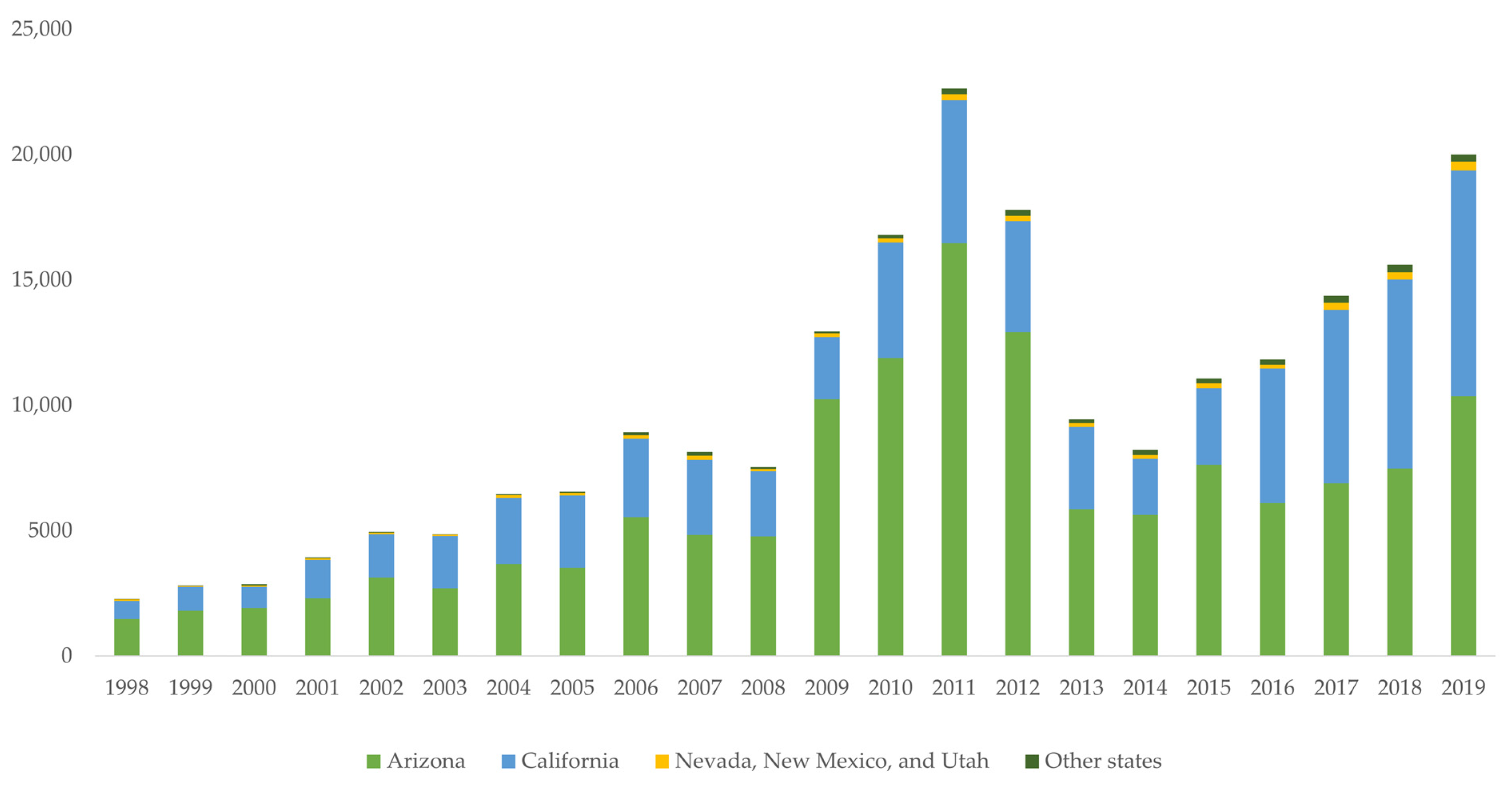
2.1. Increased Number of Reported Cases
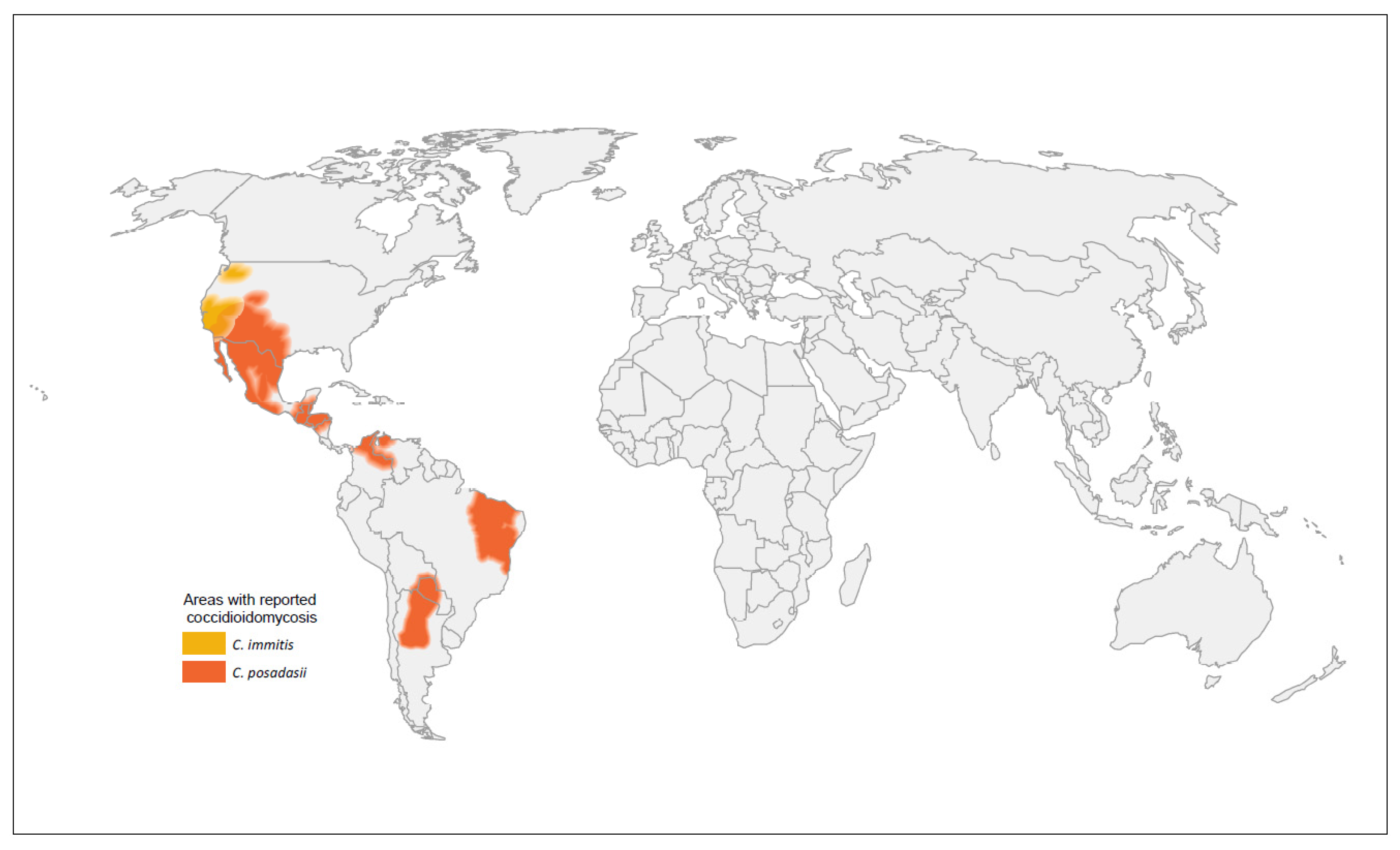
2.2. Geographic Expansion of Coccidioides Species
2.3. Risk Factors
2.4. Coccidioidomycosis and COVID-19
3. Diagnosis
3.1. Diagnostic Challenges
3.2. Serology
3.3. Antigen Detection
3.4. Microscopy and Culture
3.5. Additional Laboratory Diagnostic Methods

{kind=link}
{kind=link}
| Test | Sensitivity | Specificity ‡ | Considerations |
|---|---|---|---|
| Serology | |||
| Antibody | Antibody production may lag behind symptom onset. Sensitivity is often lower in immunosuppressed patients. | ||
| EIA IgG or IgM [103,104,105] | 59–88% | 68–96% | Rapid performance time within hours. Often used as a screening test, later confirmed by ID or CF. IgM only may lead to more false positives than IgG only. |
| EIA IgG [103,104,105] | 47–87% | 89–97% | |
| EIA IgM [103,104,105] | 22–61% | 70–99% | |
| ID § [103,118] | 60–91% | 99–100% | Results may take several days to receive. Some specialized training is required. Methods are not standardized across laboratories. |
| CF § [103,108,109,118] | 65–98% | 80–98% | Titers may offer prognostic value of disease progression. Measurement of IgG only. Highly specialized training is required. Methods are not standardized across laboratories. |
| LFA § [117,118] | 31–99% | 92–98% | Rapid 1-h performance time. |
| Antigen | |||
| Urine and serum [113] | 57% | 99% | May detect Coccidioides in the early stages of the disease [112]. May be preferred to antibody tests for immunocompromised patients. Substantial cross-reactivity with other dimorphic fungi. |
| Urine [111,113] | 37–71% | 99% | |
| Serum [119] | 73% | 100% | |
| Microscopy and culture | |||
| Culture [114] | 23–93% | High | Considered the gold standard of coccidioidomycosis diagnosis. Biosafety level 3 lab needed for safe isolation of Coccidioides. Culture growth may take up to a week. Sensitivity is heavily dependent on specimen quality. |
| Histopathology [114] | 23–84% | High | |
| Cytology [114] | 15–75% | High | |
| Additional laboratory methods | |||
| PCR [115,116] | 56–75% | 99–100% | Rapid 4-h performance time. Site of specimen collection may influence results. |
| (1→3) β-d-glucan [117] | 44% | 91% | Lower sensitivity among patients with acute pulmonary coccidioidomycosis. Values correlate poorly with CF titers. Test cannot detect specific pathogens. |
4. Treatment
4.1. Azoles
4.2. Polyenes
4.3. Treatment Duration and Follow-Up
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Smith, C.E.; Whiting, E.G.; Baker, E.E.; Rosenberger, H.G.; Beard, R.R.; Saito, M.T. The Use of Coccidioidin1, 2. Am. Rev. Tuberc. 1948, 57, 330–360. [Google Scholar] [CrossRef] [PubMed]
- Donovan, F.M.; Wightman, P.; Zong, Y.; Gabe, L.; Majeed, A.; Ynosencio, T.; Bedrick, E.J.; Galgiani, J.N. Delays in Coccidioidomycosis Diagnosis and Associated Healthcare Utilization, Tucson, Arizona, USA. Emerg. Infect. Dis. 2019, 25, 1745–1747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, C.E.; Beard, R.R. Varieties of Coccidioidal Infection in Relation to the Epidemiology and Control of the Diseases. Am. J. Public Health Nations Health 1946, 36, 1394–1402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galgiani, J.N.; Ampel, N.M.; Blair, J.E.; Catanzaro, A.; Geertsma, F.; Hoover, S.E.; Johnson, R.H.; Kusne, S.; Lisse, J.; MacDonald, J.D.; et al. 2016 Infectious Diseases Society of America (IDSA) Clinical Practice Guideline for the Treatment of Coccidioidomycosis. Clin. Infect. Dis. 2016, 63, e112–e146. [Google Scholar] [CrossRef]
- Benedict, K.; Jackson, B.R.; Chiller, T.; Beer, K.D. Estimation of direct healthcare costs of fungal diseases in the United States. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2019, 68, 1791–1797. [Google Scholar] [CrossRef] [Green Version]
- Benedict, K.; Whitham, H.K.; Jackson, B.R. Economic Burden of Fungal Diseases in the United States. Open Forum Infect. Dis. 2022, 9, ofac097. [Google Scholar] [CrossRef]
- Wilson, L.; Ting, J.; Lin, H.; MacLean, M.; Peterson, M.W.; Stockamp, N.; Libke, R.; Brown, P. The Rise of Valley Fever: Prevalence and Cost Burden of Coccidioidomycosis Infection in California. Int. J. Environ. Res. Public Health 2019, 16, 1113. [Google Scholar] [CrossRef] [Green Version]
- Grizzle, A.J.; Wilson, L.; Nix, D.E.; Galgiani, J.N. Clinical and Economic Burden of Valley Fever in Arizona: An Incidence-Based Cost-of-Illness Analysis. Open Forum Infect. Dis. 2020, 8, ofaa623. [Google Scholar] [CrossRef]
- Edwards, P.Q.; Palmer, C.E. Prevalence of Sensitivity to Coccidioidin, With Special Reference to Specific and Nonspecific Reactions to Coccidioidin and to Histoplasmin. Dis. Chest. 1957, 31, 35–60. [Google Scholar] [CrossRef]
- Marsden-Haug, N.; Goldoft, M.; Ralston, C.; Limaye, A.P.; Chua, J.; Hill, H.; Jecha, L.; Thompson, G.R.; Chiller, T. Coccidioidomycosis Acquired in Washington State. Clin. Infect. Dis. 2013, 56, 847–850. [Google Scholar] [CrossRef] [Green Version]
- Benedict, K.; Thompson, G.R.; Deresinski, S.; Chiller, T. Mycotic Infections Acquired outside Areas of Known Endemicity, United States. Emerg. Infect. Dis. 2015, 21, 1935–1941. [Google Scholar] [CrossRef]
- Laniado-Laborín, R.; Arathoon, E.G.; Canteros, C.; Muñiz-Salazar, R.; Rendon, A. Coccidioidomycosis in Latin America. Med. Mycol. 2019, 57 (Suppl. 1), S46–S55. [Google Scholar] [CrossRef]
- Ashraf, N.; Kubat, R.C.; Poplin, V.; Adenis, A.A.; Denning, D.W.; Wright, L.; McCotter, O.; Schwartz, I.S.; Jackson, B.R.; Chiller, T.; et al. Re-drawing the Maps for Endemic Mycoses. Mycopathologia 2020, 185, 843–865. [Google Scholar] [CrossRef]
- Benedict, K.; Ireland, M.; Weinberg, M.P.; Gruninger, R.J.; Weigand, J.; Chen, L.; Perez-Lockett, K.; Bledsoe, C.; Denny, L.; Cibulskas, K.; et al. Enhanced Surveillance for Coccidioidomycosis, 14 US States, 2016. Emerg. Infect. Dis. 2018, 24, 1444–1452. [Google Scholar] [CrossRef] [Green Version]
- Benedict, K.; Li, Y.; Molinari, N.A.M.; Jackson, B.R. Health Care Providers’ Testing Practices for Coccidioidomycosis and Histoplasmosis in Patients With Community-Acquired Pneumonia—United States, 2020. Open Forum Infect. Dis. 2021, 8, ofab020. [Google Scholar] [CrossRef]
- Reportable Fungal Diseases by State Fungal Diseases CDC. Published 19 November 2021. Available online: https://www.cdc.gov/fungal/fungal-disease-reporting-table.html (accessed on 1 April 2022).
- Valley Fever Statistics Coccidioidomycosis Types of Fungal Diseases Fungal CDC. Published 15 October 2021. Available online: https://www.cdc.gov/fungal/diseases/coccidioidomycosis/statistics.html (accessed on 26 March 2022).
- Epidemiologic Summary of Valley Fever (Coccidioidomycosis) in California, 2019; California Department of Public Health: Sacramento, CA, USA, 2019. Available online: https://www.cdph.ca.gov/Programs/CID/DCDC/CDPH%20Document%20Library/CocciEpiSummary2019.pdf (accessed on 12 April 2022).
- Valley Fever 2019 Annual Report; Arizona Department of Health Services. Available online: https://www.azdhs.gov/documents/preparedness/epidemiology-disease-control/valley-fever/reports/valley-fever-2019.pdf (accessed on 12 April 2022).
- Coccidioidomycosis in California Provisional Monthly Report, January–February 2022; California Department of Public Health. Available online: https://www.cdph.ca.gov/Programs/CID/DCDC/CDPH%20Document%20Library/CocciinCAProvisionalMonthlyReport.pdf (accessed on 12 April 2022).
- Year-to-Date Communicable Disease Summary; Arizona Department of Health Services: 2022. Available online: https://www.azdhs.gov/documents/preparedness/epidemiology-disease-control/disease-data-statistics-reports/data-statistics-archive/2021/2021-ytd-communicable-disease-summary.pdf (accessed on 12 April 2022).
- Gorris, M.E.; Cat, L.A.; Zender, C.S.; Treseder, K.K.; Randerson, J.T. Coccidioidomycosis Dynamics in Relation to Climate in the Southwestern United States. GeoHealth 2018, 2, 6–24. [Google Scholar] [CrossRef]
- Head, J.R.; Sondermeyer-Cooksey, G.; Heaney, A.K.; Yu, A.T.; Jones, I.; Bhattachan, A.; Campo, S.; Wagner, R.; Mgbara, W.; Phillips, S.; et al. Influence of Meteorological Factors and Drought on Coccidioidomycosis Incidence in California, 2000–2020. Epidemiology 2022. [Google Scholar] [CrossRef]
- Gorris, M.E.; Treseder, K.K.; Zender, C.S.; Randerson, J.T. Expansion of Coccidioidomycosis Endemic Regions in the United States in Response to Climate Change. GeoHealth 2019, 3, 308–327. [Google Scholar] [CrossRef] [Green Version]
- Baptista-Rosas, R.C.; Hinojosa, A.; Riquelme, M. Ecological Niche Modeling of Coccidioides spp. in Western North American Deserts. Ann. N. Y. Acad. Sci. 2007, 1111, 35–46. [Google Scholar] [CrossRef]
- Kolivras, K.N.; Comrie, A.C. Modeling valley fever (coccidioidomycosis) incidence on the basis of climate conditions. Int. J. Biometeorol. 2003, 47, 87–101. [Google Scholar] [CrossRef]
- Tamerius, J.D.; Comrie, A.C. Coccidioidomycosis Incidence in Arizona Predicted by Seasonal Precipitation. PLoS ONE 2011, 6, e21009. [Google Scholar] [CrossRef] [Green Version]
- Talamantes, J.; Behseta, S.; Zender, C.S. Fluctuations in Climate and Incidence of Coccidioidomycosis in Kern County, California. Ann. N. Y. Acad. Sci. 2007, 1111, 73–82. [Google Scholar] [CrossRef]
- Zender, C.S.; Talamantes, J. Climate controls on valley fever incidence in Kern County, California. Int. J. Biometeorol. 2006, 50, 174–182. [Google Scholar] [CrossRef] [Green Version]
- Comrie, A.C. Climate Factors Influencing Coccidioidomycosis Seasonality and Outbreaks. Environ. Health Perspect. 2005, 113, 688–692. [Google Scholar] [CrossRef]
- Park, B.J.; Sigel, K.; Vaz, V.; Komatsu, K.; McRill, C.; Phelan, M.; Colman, T.; Comrie, A.C.; Warnock, D.W.; Galgiani, J.N.; et al. An Epidemic of Coccidioidomycosis in Arizona Associated with Climatic Changes, 1998–2001. J. Infect. Dis. 2005, 191, 1981–1987. [Google Scholar] [CrossRef] [Green Version]
- US EPA, O. Particulate Matter (PM10) Trends. Published 19 July 2016. Available online: https://www.epa.gov/air-trends/particulate-matter-pm10-trends (accessed on 1 April 2022).
- Kollath, D.R.; Mihaljevic, J.R.; Barker, B.M. PM10 and Other Climatic Variables Are Important Predictors of Seasonal Variability of Coccidioidomycosis in Arizona. Microbiol. Spectr. 2022, 10, e0148321. [Google Scholar] [CrossRef]
- U.S. Census Bureau QuickFacts. Available online: https://www.census.gov/quickfacts/fact/table/maricopacountyarizona,CA,AZ,US/AGE775220 (accessed on 26 March 2022).
- Colson, A.J.; Vredenburgh, L.; Guevara, R.E.; Rangel, N.P.; Kloock, C.T.; Lauer, A. Large-Scale Land Development, Fugitive Dust, and Increased Coccidioidomycosis Incidence in the Antelope Valley of California, 1999–2014. Mycopathologia 2017, 182, 439–458. [Google Scholar] [CrossRef]
- Guevara, R.E.; Motala, T.; Terashita, D. The Changing Epidemiology of Coccidioidomycosis in Los Angeles (LA) County, California, 1973–2011. PLoS ONE 2015, 10, e0136753. [Google Scholar] [CrossRef] [Green Version]
- Leake, J.A.D.; Mosley, D.G.; England, B.; Graham, J.V.; Plikaytis, B.D.; Ampel, N.M.; Perkins, B.A.; Hajjeh, R.A. Risk Factors for Acute Symptomatic Coccidioidomycosis among Elderly Persons in Arizona, 1996–1997. J. Infect. Dis. 2000, 181, 1435–1440. [Google Scholar] [CrossRef]
- Center for International Blood and Marrow Transplant Research Transplant Activity Report Covering 2009–2013. Available online: https://bloodstemcell.hrsa.gov/data/donation-and-transplantation-statistics/transplant-activity-report (accessed on 26 March 2022).
- Organ Procurement and Transplantation Network: View Data Reports. Available online: https://optn.transplant.hrsa.gov/data/view-data-reports/ (accessed on 26 March 2022).
- Casadevall, A. Fungal Diseases in the 21st Century: The Near and Far Horizons. Pathog. Immun. 2018, 3, 183–196. [Google Scholar] [CrossRef]
- Brown, J.; Benedict, K.; Park, B.J.; Thompson, G.R. Coccidioidomycosis: Epidemiology. Clin. Epidemiol. 2013, 5, 185–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odio, C.D.; Marciano, B.E.; Galgiani, J.N.; Holland, S.M. Risk Factors for Disseminated Coccidioidomycosis, United States. Emerg. Infect. Dis. 2017, 23, 308–311. [Google Scholar] [CrossRef] [PubMed]
- Tsang, C.A.; Anderson, S.M.; Imholte, S.B.; Erhart, L.M.; Chen, S.; Park, B.J.; Christ, C.; Komatsu, K.K.; Chiller, T.; Sunenshine, R.H. Enhanced Surveillance of Coccidioidomycosis, Arizona, USA, 2007–2008. Emerg. Infect. Dis. 2010, 16, 1738–1744. [Google Scholar] [CrossRef] [PubMed]
- Benedict, K.; Molinari, N.A.M.; Jackson, B.R. Public Awareness of Invasive Fungal Diseases—United States, 2019. Morb. Mortal. Wkly. Rep. 2020, 69, 1343–1346. [Google Scholar] [CrossRef]
- Hurd-Kundeti, G.; Sondermeyer Cooksey, G.L.; Jain, S.; Vugia, D.J. Valley Fever (Coccidioidomycosis) Awareness—California, 2016–2017. Morb. Mortal. Wkly. Rep. 2020, 69, 1512–1516. [Google Scholar] [CrossRef]
- Werner, S.B.; Pappagianis, D. Coccidioidomycosis in Northern California—An Outbreak among Archeology Students near Red Bluff. Calif. Med. 1973, 119, 16–20. [Google Scholar]
- Petersen, L.R.; Marshall, S.L.; Barton, C.; Hajjeh, R.A.; Lindsley, M.D.; Warnock, D.W.; Panackal, A.A.; Shaffer, J.B.; Haddad, M.B.; Fisher, F.S.; et al. Coccidioidomycosis among Workers at an Archeological Site, Northeastern Utah. Emerg. Infect. Dis. 2004, 10, 637–642. [Google Scholar] [CrossRef]
- Werner, S.B.; Pappagianis, D.; Heindl, I.; Mickel, A. An Epidemic of Coccidioidomycosis among Archeology Students in Northern California. N. Engl. J. Med. 1972, 286, 507–512. [Google Scholar] [CrossRef]
- Factors Influencing Distribution of Coccidioides Immitis in Soil, Washington State, 2016-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/34730378/ (accessed on 23 March 2022).
- Kobziar, L.N.; Thompson, G.R. Wildfire smoke, a potential infectious agent. Science 2020, 370, 1408–1410. [Google Scholar] [CrossRef]
- Laws, R.L.; Jain, S.; Cooksey, G.S.; Mohle-Boetani, J.; McNary, J.; Wilken, J.; Harrison, R.; Leistikow, B.; Vugia, D.J.; Windham, G.C.; et al. Coccidioidomycosis outbreak among inmate wildland firefighters: California, 2017. Am. J. Ind. Med. 2021, 64, 266–273. [Google Scholar] [CrossRef]
- Tong, D.Q.; Wang, J.X.L.; Gill, T.E.; Lei, H.; Wang, B. Intensified dust storm activity and Valley fever infection in the southwestern United States. Geophys. Res. Lett. 2017, 44, 4304–4312. [Google Scholar] [CrossRef] [Green Version]
- Comrie, A.C. No Consistent Link Between Dust Storms and Valley Fever (Coccidioidomycosis). GeoHealth 2021, 5, e2021GH000504. [Google Scholar] [CrossRef]
- Gade, L.; McCotter, O.Z.; Bowers, J.R.; Waddell, V.; Brady, S.; Carvajal, J.A.; Sunenshine, R.; Komatsu, K.K.; Engelthaler, D.M.; Chiller, T.; et al. The detection of Coccidioides from ambient air in Phoenix, Arizona: Evidence of uneven distribution and seasonality. Med. Mycol. 2020, 58, 552–559. [Google Scholar] [CrossRef]
- Emmons, C.W. Coccidioidomycosis in Wild Rodents. A Method of Determining the Extent of Endemic Areas. Public Health Rep. (1896–1970) 1943, 58, 1–5. [Google Scholar] [CrossRef]
- Health ASD of Proceedings of Symposium on Coccidioidomycosis: Held at Phoenix, Ariz.-Feb. 11–13, 1957; U.S. Department of Health, Education, and Welfare Public Health Service, Bureau of State Services, Communicable Disease Center: Washington, DC, USA, 1957.
- Kollath, D.R.; Miller, K.J.; Barker, B.M. The mysterious desert dwellers: Coccidioides immitis and Coccidioides posadasii, causative fungal agents of coccidioidomycosis. Virulence 2019, 10, 222–233. [Google Scholar] [CrossRef] [Green Version]
- Soil Ecology of Coccidioides Immitis at Amerindian Middens in California Applied Microbiology. Available online: https://journals.asm.org/doi/abs/10.1128/am.27.2.379-388.1974 (accessed on 23 March 2022).
- Cordeiro, R.A.; Brilhante, R.S.N.; Rocha, M.F.G.; Fechine, M.A.B.; Camara, L.M.C.; Camargo, Z.P.; Sidrim, J.J.C. Phenotypic characterization and ecological features of Coccidioides spp. from Northeast Brazil. Med. Mycol. 2006, 44, 631–639. [Google Scholar] [CrossRef] [Green Version]
- Sharpton, T.J.; Stajich, J.E.; Rounsley, S.D.; Gardner, M.J.; Wortman, J.R.; Jordar, V.S.; Maiti, R.; Kodira, C.D.; Neafsey, D.E.; Zeng, Q.; et al. Comparative genomic analyses of the human fungal pathogens Coccidioides and their relatives. Genome Res. 2009, 19, 1722–1731. [Google Scholar] [CrossRef] [Green Version]
- Ampel, N.M.; Dols, C.L.; Galgiani, J.N. Coccidioidomycosis during human immunodeficiency virus infection: Results of a prospective study in a coccidioidal endemic area. Am. J. Med. 1993, 94, 235–240. [Google Scholar] [CrossRef]
- Woods, C.W.; McRill, C.; Plikaytis, B.D.; Rosenstein, N.E.; Mosley, D.; Boyd, D.; England, B.; Perkins, B.A.; Ampel, N.M.; Hajjeh, R.A. Coccidioidomycosis in Human Immunodeficiency Virus–Infected Persons in Arizona, 1994–1997: Incidence, Risk Factors, and Prevention. J. Infect. Dis. 2000, 181, 1428–1434. [Google Scholar] [CrossRef]
- Masannat, F.Y.; Ampel, N.M. Coccidioidomycosis in Patients with HIV-1 Infection in the Era of Potent Antiretroviral Therapy. Clin. Infect. Dis. 2010, 50, 1–7. [Google Scholar] [CrossRef]
- Blair, J.E.; Logan, J.L. Coccidioidomycosis in Solid Organ Transplantation. Clin. Infect. Dis. 2001, 33, 1536–1544. [Google Scholar] [CrossRef]
- Bergstrom, L.; Yocum, D.E.; Ampel, N.M.; Villanueva, I.; Lisse, J.; Gluck, O.; Tesser, J.; Posever, J.P.; Miller, M.; Araujo, J.; et al. Increased risk of coccidioidomycosis in patients treated with tumor necrosis factor α antagonists. Arthritis Rheum. 2004, 50, 1959–1966. [Google Scholar] [CrossRef]
- Blair, J.E.; Douglas, D.D.; Mulligan, D.C. Early results of targeted prophylaxis for coccidioidomycosis in patients undergoing orthotopic liver transplantation within an endemic area. Transpl. Infect. Dis. 2003, 5, 3–8. [Google Scholar] [CrossRef]
- Kahn, A.; Carey, E.J.; Blair, J.E. Universal fungal prophylaxis and risk of coccidioidomycosis in liver transplant recipients living in an endemic area. Liver Transpl. 2015, 21, 353–361. [Google Scholar] [CrossRef]
- Keckich, D.W.; Blair, J.E.; Vikram, H.R.; Seville, M.T.; Kusne, S. Reactivation of Coccidioidomycosis Despite Antifungal Prophylaxis in Solid Organ Transplant Recipients. Transplantation 2011, 92, 88–93. [Google Scholar] [CrossRef]
- Truong, C.N.; Nailor, M.D.; Walia, R.; Cherrier, L.; Nasar, A.; Goodlet, K.J. Universal lifelong fungal prophylaxis and risk of coccidioidomycosis in lung transplant recipients living in an endemic area. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 74, ciab752. [Google Scholar] [CrossRef]
- Al-Obaidi, M.M.; Nematollahi, S.; Nix, D.E.; Zangeneh, T.T. Remarks on the universal lifelong coccidioidomycosis prophylaxis in lung transplant recipients. Clin. Infect. Dis. 2021, 74, ciab878. [Google Scholar] [CrossRef]
- Bercovitch, R.S.; Catanzaro, A.; Schwartz, B.S.; Pappagianis, D.; Watts, D.H.; Ampel, N.M. Coccidioidomycosis During Pregnancy: A Review and Recommendations for Management. Clin. Infect. Dis. 2011, 53, 363–368. [Google Scholar] [CrossRef] [Green Version]
- Crum, N.F.; Ballon-Landa, G. Coccidioidomycosis in Pregnancy: Case Report and Review of the Literature. Am. J. Med. 2006, 119, e11–e993. [Google Scholar] [CrossRef]
- Crum, N.F.; Lederman, E.R.; Stafford, C.M.; Parrish, J.S.; Wallace, M.R. Coccidioidomycosis: A Descriptive Survey of a Reemerging Disease. Clinical Characteristics and Current Controversies. Medicine 2004, 83, 149–175. [Google Scholar] [CrossRef]
- Sondermeyer Cooksey, G.L.; Nguyen, A.; Vugia, D.; Jain, S. Regional Analysis of Coccidioidomycosis Incidence—California, 2000–2018. Morb. Mortal. Wkly. Rep. 2020, 69, 1817–1821. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.C.; Anderson, S.; Wannemuehler, K.; Engelthaler, D.M.; Erhart, L.; Sunenshine, R.H.; Burwell, L.A.; Park, B.J. Testing for Coccidioidomycosis among Patients with Community-Acquired Pneumonia. Emerg. Infect. Dis. 2008, 14, 1053–1059. [Google Scholar] [CrossRef] [PubMed]
- Valley Fever (Coccidioidomycosis), Jobs at Risk NIOSH CDC. Published 11 March 2022. Available online: https://www.cdc.gov/niosh/topics/valleyfever/risk.html (accessed on 26 March 2022).
- de Perio, M.A.; Niemeier, R.T.; Burr, G.A. Coccidioides Exposure and Coccidioidomycosis among Prison Employees, California, United States. Emerg. Infect. Dis. 2015, 21, 1031–1033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilken, J.A.; Marquez, P.; Terashita, D.; McNary, J.; Windham, G.; Materna, B. Coccidioidomycosis Among Cast and Crew Members at an Outdoor Television Filming Event—California, 2012. MMWR Morb. Mortal Wkly Rep. 2014, 63, 20. [Google Scholar]
- Durry, E.; Pappagianis, D.; Werner, S.B.; Hutwagner, L.; Sun, R.K.; Maurer, M.; McNeil, M.M.; Pinner, R.W. Coccidioidomycosis in Tulare County, California, 1991: Reemergence of an endemic disease. J. Med. Vet. Mycol. 1997, 35, 321–326. [Google Scholar] [CrossRef] [Green Version]
- Sondermeyer, G.; Lee, L.; Gilliss, D.; Tabnak, F.; Vugia, D. Coccidioidomycosis-associated Hospitalizations, California, USA, 2000–2011. Emerg. Infect. Dis. 2013, 19, 1590–1597. [Google Scholar] [CrossRef]
- Einstein, H.E.; Johnson, R.H. Coccidioidomycosis: New Aspects of Epidemiology and Therapy. Clin. Infect. Dis. 1993, 16, 349–356. [Google Scholar] [CrossRef]
- McHardy, I.; Reagan, K.L.; Sebastian, J.F.; Barker, B.; Bays, D.J.; Dandekar, S.; Cohen, S.H.; Jennings, K.E.; Sykes, J.; Thompson, G.R. Sex Differences in Susceptibility to Coccidioidomycosis. Open Forum Infect. Dis. 2022, 9, ofab543. [Google Scholar] [CrossRef]
- Shah, A.S.; Heidari, A.; Civelli, V.F.; Sharma, R.; Clark, C.S.; Munoz, A.D.; Ragland, A.S.; Johnson, R.H. The Coincidence of 2 Epidemics, Coccidioidomycosis and SARS-CoV-2: A Case Report. J. Investig. Med. High Impact Case Rep. 2020, 8, 2324709620930540. [Google Scholar] [CrossRef]
- Chang, C.C.; Senining, R.; Kim, J.; Goyal, R. An Acute Pulmonary Coccidioidomycosis Coinfection in a Patient Presenting With Multifocal Pneumonia With COVID-19. J. Investig. Med. High Impact Case Rep. 2020, 8, 2324709620972244. [Google Scholar] [CrossRef]
- Chen, J.C.; Wong, D.; Rabi, S.; Worswick, S.; DeClerck, B.; Gibb, J. All That Coughs Is Not COVID-19: A Delayed Diagnosis of Disseminated Coccidioidomycosis Following Severe Acute Respiratory Syndrome Coronavirus 2 Infection. Open Forum Infect. Dis. 2021, 8, ofab246. [Google Scholar] [CrossRef]
- Nielsen, M.C.; Reynoso, D.; Ren, P. The Brief Case: A Fatal Case of SARS-CoV-2 Coinfection with Coccidioides in Texas—Another Challenge We Face. Burnham, C.A.D., Ed. J. Clin. Microbiol. 2021, 59, e00163-21. [Google Scholar] [CrossRef]
- Ko, J.; Lee, M.M. A Case of Disseminated Coccidioidomycosis in a Patient with a Prolonged Course of COVID-19 Pneumonia. In TP98. TP098 FUNGUS AMONG-US-RARE FUNGAL CASE REPORTS; American Thoracic Society International Conference Abstracts; American Thoracic Society: New York, NY, USA, 2021; p. A3997. [Google Scholar] [CrossRef]
- Mathew, J.; Cherukuri, S.V.; Dihowm, F. SARS-CoV-2 with concurrent coccidioidomycosis complicated by refractory pneumothorax in a Hispanic male: A case report and literature review. World J. Respirol. 2021, 11, 1–11. [Google Scholar] [CrossRef]
- Patel, B.; Jarrett, B.; Bixby, B. Diagnostic Error and Cognitive Bias in the Era of COVID-19: Don’t Forget About Endemic Diseases. Chest 2020, 158, A541–A542. [Google Scholar] [CrossRef]
- Krauth, D.S.; Jamros, C.M.; Rivard, S.C.; Olson, N.H.; Maves, R.C. Accelerated Progression of Disseminated Coccidioidomycosis Following SARS-CoV-2 Infection: A Case Report. Mil. Med. 2021, 186, usab132. [Google Scholar] [CrossRef]
- Heaney, A.K.; Head, J.R.; Broen, K.; Click, K.; Taylor, J.; Balmes, J.R.; Zelner, J.; Remais, J.V. Coccidioidomycosis and COVID-19 Co-Infection, United States, 2020. Emerg. Infect. Dis. 2021, 27, 1266–1273. [Google Scholar] [CrossRef]
- Shi, Y.; Yu, X.; Zhao, H.; Wang, H.; Zhao, R.; Sheng, J. Host susceptibility to severe COVID-19 and establishment of a host risk score: Findings of 487 cases outside Wuhan. Crit. Care. 2020, 24, 108. [Google Scholar] [CrossRef] [Green Version]
- CDC COVID-19 Response Team. Preliminary Estimates of the Prevalence of Selected Underlying Health Conditions Among Patients with Coronavirus Disease 2019—United States, 12 February–28 March 2020. Morb. Mortal. Wkly. Rep. 2020, 69. [Google Scholar] [CrossRef]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of immune response in patients with COVID-19 in Wuhan, China. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 71, ciaa248. [Google Scholar] [CrossRef]
- Beaman, L.; Benjamini, E.; Pappagianis, D. Activation of macrophages by lymphokines: Enhancement of phagosome-lysosome fusion and killing of Coccidioides immitis. Infect. Immun. 1983, 39, 1201–1207. [Google Scholar] [CrossRef] [Green Version]
- Benedict, K.; Williams, S.; Beekmann, S.E.; Polgreen, P.M.; Jackson, B.R.; Toda, M. Testing Practices for Fungal Respiratory Infections and SARS-CoV-2 among Infectious Disease Specialists, United States. J. Fungi. 2021, 7, 605. [Google Scholar] [CrossRef]
- Olson, G.; Davis, A.M. Diagnosis and Treatment of Adults With Community-Acquired Pneumonia. JAMA 2020, 323, 885. [Google Scholar] [CrossRef]
- Valdivia, L.; Nix, D.; Wright, M.; Lindberg, E.; Fagan, T.; Lieberman, D.; Stoffer, T.; Ampel, N.M.; Galgiani, J.N. Coccidioidomycosis as a Common Cause of Community-acquired Pneumonia. Emerg. Infect. Dis. 2006, 12, 958–962. [Google Scholar] [CrossRef]
- Chi, G.C.; Benedict, K.; Beer, K.D.; Jackson, B.R.; McCotter, O.; Xie, F.; Lawrence, J.M.; Tartof, S.Y. Antibiotic and antifungal treatment among persons with confirmed coccidioidomycosis—Southern California, 2011. Med. Mycol. 2020, 58, 411–413. [Google Scholar] [CrossRef]
- Chen, S.; Erhart, L.M.; Anderson, S.; Komatsu, K.; Park, B.; Chiller, T.; Sunenshine, R. Coccidioidomycosis: Knowledge, attitudes, and practices among healthcare providers—Arizona, 2007. Med. Mycol. 2011, 49, 649–656. [Google Scholar] [CrossRef]
- Pu, J.; Donovan, F.M.; Ellingson, K.; Leroy, G.; Stone, J.; Bedrick, E.; Galgiani, J.N. Clinician Practice Patterns That Result in the Diagnosis of Coccidioidomycosis Before or During Hospitalization. Clin. Infect. Dis. 2021, 73, e1587–e1593. [Google Scholar] [CrossRef]
- Malo, J.; Holbrook, E.; Zangeneh, T.; Strawter, C.; Oren, E.; Robey, I.; Erickson, H.; Chahal, R.; Durkin, M.; Thompson, C.; et al. Enhanced Antibody Detection and Diagnosis of Coccidioidomycosis with the MiraVista IgG and IgM Detection Enzyme Immunoassay. J. Clin. Microbiol. 2017, 55, 893–901. [Google Scholar] [CrossRef] [Green Version]
- Malo, J.; Holbrook, E.; Zangeneh, T.; Strawter, C.; Oren, E.; Robey, I.; Erickson, H.; Carranza-Chahal, R.; Durkin, M.; Thompson, C.; et al. Comparison of three anti-coccidioides antibody enzyme immunoassay kits for the diagnosis of coccidioidomycosis. Med. Mycol. 2020, 58, 774–778. [Google Scholar] [CrossRef]
- Grys, T.E.; Brighton, A.; Chang, Y.H.; Liesman, R.; Bolster LaSalle, C.; Blair, J.E. Comparison of two FDA-cleared EIA assays for the detection of Coccidioides antibodies against a composite clinical standard. Med. Mycol. 2019, 57, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Kuberski, T.; Herrig, J.; Pappagianis, D. False-Positive IgM Serology in Coccidioidomycosis. J. Clin. Microbiol. 2010, 48, 2047–2049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donovan, F.M.; Ramadan, F.A.; Khan, S.A.; Bhaskara, A.; Lainhart, W.D.; Narang, A.T.; Mosier, J.M.; Ellingson, K.D.; Bedrick, E.J.; Saubolle, M.A.; et al. Comparison of a Novel Rapid Lateral Flow Assay to Enzyme Immunoassay Results for Early Diagnosis of Coccidioidomycosis. Clin. Infect. Dis. 2021, 73, e2746–e2753. [Google Scholar] [CrossRef] [PubMed]
- Huppert, M. Serology of coccidioidomycosis. Mycopathol. Mycol. Appl. 1970, 41, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Blair, J.E.; Coakley, B.; Santelli, A.C.; Hentz, J.G.; Wengenack, N.L. Serologic testing for symptomatic coccidioidomycosis in immunocompetent and immunosuppressed hosts. Mycopathologia 2006, 162, 317–324. [Google Scholar] [CrossRef] [Green Version]
- Mendoza, N.; Blair, J.E. The Utility of Diagnostic Testing for Active Coccidioidomycosis in Solid Organ Transplant Recipients. Am. J. Transplant. 2013, 13, 1034–1039. [Google Scholar] [CrossRef]
- Durkin, M.; Connolly, P.; Kuberski, T.; Myers, R.; Kubak, B.M.; Bruckner, D.; Pegues, D.; Wheat, L.J. Diagnosis of Coccidioidomycosis with Use of the Coccidioides Antigen Enzyme Immunoassay. Clin. Infect. Dis. 2008, 47, e69–e73. [Google Scholar] [CrossRef] [Green Version]
- Galgiani, J.N.; Grace, G.M.; Lundergan, L.L. New Serologic Tests for Early Detection of Coccidioidomycosis. J. Infect. Dis. 1991, 163, 671–674. [Google Scholar] [CrossRef]
- Kassis, C.; Durkin, M.; Holbrook, E.; Myers, R.; Wheat, L. Advances in Diagnosis of Progressive Pulmonary and Disseminated Coccidioidomycosis. Clin. Infect. Dis. 2021, 72, 968–975. [Google Scholar] [CrossRef] [Green Version]
- Wheat, L.J.; Knox, K.S.; Hage, C.A. Approach to the Diagnosis of Histoplasmosis, Blastomycosis and Coccidioidomycosis. Curr Curr. Treat. Options Infect. Dis. 2014, 6, 337–351. [Google Scholar] [CrossRef]
- Dizon, D.; Mitchell, M.; Dizon, B.; Libke, R.; Peterson, M.W. The utility of real-time polymerase chain reaction in detecting Coccidioides immitis among clinical specimens in the Central California San Joaquin Valley. Med. Mycol. 2019, 57, 688–693. [Google Scholar] [CrossRef]
- Vucicevic, D.; Blair, J.E.; Binnicker, M.J.; McCullough, A.E.; Kusne, S.; Vikram, H.R.; Parish, J.M.; Wengenack, N.L. The utility of Coccidioides polymerase chain reaction testing in the clinical setting. Mycopathologia 2010, 170, 345–351. [Google Scholar] [CrossRef]
- Thompson, G.R.; Bays, D.J.; Johnson, S.M.; Cohen, S.H.; Pappagianis, D.; Finkelman, M.A. Serum (1→3)-β-d-Glucan Measurement in Coccidioidomycosis. J. Clin. Microbiol. 2012, 50, 3060–3062. [Google Scholar] [CrossRef] [Green Version]
- Caceres, D.H.; Chiller, T.; Lindsley, M.D. Immunodiagnostic Assays for the Investigation of Fungal Outbreaks. Mycopathologia 2020, 185, 867–880. [Google Scholar] [CrossRef]
- Durkin, M.; Estok, L.; Hospenthal, D.; Crum-Cianflone, N.; Swartzentruber, S.; Hackett, E.; Wheat, L.J. Detection of Coccidioides Antigenemia following Dissociation of Immune Complexes. Clin. Vaccine Immunol. 2009, 16, 1453–1456. [Google Scholar] [CrossRef] [Green Version]
- Messina, J.A.; Maziarz, E.K.; Galgiani, J.; Truong, J.T.; Htoo, A.K.; Heidari, A.; Johnson, R.H.; Narang, A.T.; Donovan, F.M.; Ewell, M.; et al. A randomized, double-blind, placebo-controlled clinical trial of fluconazole as early empiric treatment of coccidioidomycosis pneumonia (Valley Fever) in adults presenting with community-acquired pneumonia in endemic areas (FLEET-Valley Fever). Contemp. Clin. Trials. Commun. 2021, 24, 100851. [Google Scholar] [CrossRef]
- Sugar, A.M.; Alsip, S.G.; Galgiani, J.N.; Graybill, J.R.; Dismukes, W.E.; Cloud, G.A.; Craven, P.C.; Stevens, D.A. Pharmacology and toxicity of high-dose ketoconazole. Antimicrob. Agents Chemother. 1987, 31, 1874–1878. [Google Scholar] [CrossRef] [Green Version]
- Pont, A.; Graybill, J.R.; Craven, P.C.; Galgiani, J.N.; Dismukes, W.E.; Reitz, R.E.; Stevens, D.A. High-Dose Ketoconazole Therapy and Adrenal and Testicular Function in Humans. Arch. Intern. Med. 1984, 144, 2150–2153. [Google Scholar] [CrossRef]
- Arndt, C.A.S.; Walsh, T.J.; McCully, C.L.; Balis, F.M.; Pizzo, P.A.; Poplack, D.G. Fluconazole Penetration into Cerebrospinal Fluid: Implications for Treating Fungal Infections of the Central Nervous System. J. Infect. Dis. 1988, 157, 178–180. [Google Scholar] [CrossRef]
- Brewer, A.C.; Huber, J.T.; Girardo, M.E.; Kosiorek, H.E.; Burns, M.W.; Stewart, T.D.; Blair, J.E. Cutaneous effects associated with fluconazole in patients treated for coccidioidomycosis. Int. J. Dermatol. 2019, 58, 250–253. [Google Scholar] [CrossRef]
- Thompson, G.R.; Barker, B.M.; Wiederhold, N.P. Large-Scale Evaluation of In Vitro Amphotericin B, Triazole, and Echinocandin Activity against Coccidioides Species from U.S. Institutions. Antimicrob. Agents Chemother. 2017, 61, e02634-16. [Google Scholar] [CrossRef] [Green Version]
- Galgiani, J.N. Comparison of Oral Fluconazole and Itraconazole for Progressive, Nonmeningeal Coccidioidomycosis: A Randomized, Double-Blind Trial. Ann. Intern. Med. 2000, 133, 676. [Google Scholar] [CrossRef]
- Hoffmann, W.J.; McHardy, I.; Thompson, G.R., III. Itraconazole induced hypertension and hypokalemia: Mechanistic evaluation. Mycoses 2018, 61, 337–339. [Google Scholar] [CrossRef]
- Lestner, J.M.; Roberts, S.A.; Moore, C.B.; Howard, S.J.; Denning, D.W.; Hope, W.W. Toxicodynamics of Itraconazole: Implications for Therapeutic Drug Monitoring. Clin. Infect. Dis. 2009, 49, 928–930. [Google Scholar] [CrossRef]
- Sharkey, P.K.; Rinaldi, M.G.; Dunn, J.F.; Hardin, T.C.; Fetchick, R.J.; Graybill, J.R. High-dose itraconazole in the treatment of severe mycoses. Antimicrob. Agents Chemother. 1991, 35, 707–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.M.; Vikram, H.R.; Kusne, S.; Seville, M.T.; Blair, J.E. Treatment of Refractory Coccidioidomycosis With Voriconazole or Posaconazole. Clin. Infect. Dis. 2011, 53, 1060–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortez, K.J.; Walsh, T.J.; Bennett, J.E. Successful Treatment of Coccidioidal Meningitis with Voriconazole. Clin. Infect. Dis. 2003, 36, 1619–1622. [Google Scholar] [CrossRef] [PubMed]
- Freifeld, A.; Proia, L.; Andes, D.; Baddour, L.M.; Blair, J.; Spellberg, B.; Arnold, S.; Lentnek, A.; Wheat, L.J. Voriconazole Use for Endemic Fungal Infections. Antimicrob. Agents Chemother. 2009, 53, 1648–1651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epaulard, O.; Villier, C.; Ravaud, P.; Chosidow, O.; Blanche, S.; Mamzer-Bruneel, M.; Thiebaut, A.; Leccia, M.; Lortholary, O. A Multistep Voriconazole-Related Phototoxic Pathway May Lead to Skin Carcinoma: Results From a French Nationwide Study. Clin. Infect. Dis. 2013, 57, e182–e188. [Google Scholar] [CrossRef]
- Haylett, A.K.; Felton, S.; Denning, D.W.; Rhodes, L.E. Voriconazole-induced photosensitivity: Photobiological assessment of a case series of 12 patients. Br. J. Dermatol. 2013, 168, 179–185. [Google Scholar] [CrossRef]
- Williams, K.; Mansh, M.; Chin-Hong, P.; Singer, J.; Arron, S.T. Voriconazole-Associated Cutaneous Malignancy: A Literature Review on Photocarcinogenesis in Organ Transplant Recipients. Clin. Infect. Dis. 2014, 58, 997–1002. [Google Scholar] [CrossRef] [Green Version]
- Pham, A.N.; Bubalo, J.S.; Lewis, J.S., II. Comparison of posaconazole serum concentrations from haematological cancer patients on posaconazole tablet and oral suspension for treatment and prevention of invasive fungal infections. Mycoses 2016, 59, 226–233. [Google Scholar] [CrossRef]
- Anstead, G.M.; Corcoran, G.; Lewis, J.; Berg, D.; Graybill, J.R. Refractory Coccidioidomycosis Treated with Posaconazole. Clin. Infect. Dis. 2005, 40, 1770–1776. [Google Scholar] [CrossRef]
- Catanzaro, A.; Cloud, G.A.; Stevens, D.A.; Levine, B.E.; Williams, B.L.; Johnson, R.H.; Rendon, A.; Mirels, L.F.; Lutz, J.E.; Holloway, M.; et al. Safety, Tolerance, and Efficacy of Posaconazole Therapy in Patients with Nonmeningeal Disseminated or Chronic Pulmonary Coccidioidomycosis. Clin. Infect. Dis. 2007, 45, 562–568. [Google Scholar] [CrossRef] [Green Version]
- Ruping, M.J.G.T.; Albermann, N.; Ebinger, F.; Burckhardt, I.; Beisel, C.; Muller, C.; Vehreschild, J.J.; Kochanek, M.; Fatkenheuer, G.; Bangard, C.; et al. Posaconazole concentrations in the central nervous system. J. Antimicrob. Chemother. 2008, 62, 1468–1470. [Google Scholar] [CrossRef] [Green Version]
- Schein, R.; Homans, J.; Larsen, R.A.; Neely, M. Posaconazole for Chronic Refractory Coccidioidal Meningitis. Clin. Infect. Dis. 2011, 53, 1252–1254. [Google Scholar] [CrossRef] [Green Version]
- González, G.M.; Tijerina, R.; Najvar, L.K.; Bocanegra, R.; Rinaldi, M.; Loebenberg, D.; Graybill, J.R. In Vitro and In Vivo Activities of Posaconazole against Coccidioides immitis. Antimicrob. Agents Chemother. 2002, 46, 1352–1356. [Google Scholar] [CrossRef] [Green Version]
- Donnelley, M.A.; Zhu, E.S.; Thompson, G.R. Isavuconazole in the treatment of invasive aspergillosis and mucormycosis infections. Infect. Drug Resist. 2016, 9, 79–86. [Google Scholar] [CrossRef] [Green Version]
- Thompson, G.R.; Rendon, A.; Ribeiro dos Santos, R.; Queiroz-Telles, F.; Ostrosky-Zeichner, L.; Azie, N.; Maher, R.; Lee, M.; Kovanda, L.; Engelhardt, M.; et al. Isavuconazole Treatment of Cryptococcosis and Dimorphic Mycoses. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2016, 63, 356–362. [Google Scholar] [CrossRef] [Green Version]
- Isavuconazole versus voriconazole for primary treatment of invasive mould disease caused by Aspergillus and other filamentous fungi (SECURE): A phase 3, randomised-controlled, non-inferiority trial Elsevier Enhanced Reader. Lancet 2015, 387, 760–769. [CrossRef]
- Hamill, R.J. Amphotericin B Formulations: A Comparative Review of Efficacy and Toxicity. Drugs 2013, 73, 919–934. [Google Scholar] [CrossRef]
- Saravolatz, L.D.; Ostrosky-Zeichner, L.; Marr, K.A.; Rex, J.H.; Cohen, S.H. Amphotericin B: Time for a New “Gold Standard”. Clin. Infect. Dis. 2003, 37, 415–425. [Google Scholar] [CrossRef] [Green Version]
- Stevens, D.A.; Shatsky, S.A. Intrathecal amphotericin in the management of coccidioidal meningitis. Semin. Respir. Infect. 2001, 16, 263–269. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Williams, S.L.; Chiller, T. Update on the Epidemiology, Diagnosis, and Treatment of Coccidioidomycosis. J. Fungi 2022, 8, 666. https://doi.org/10.3390/jof8070666
Williams SL, Chiller T. Update on the Epidemiology, Diagnosis, and Treatment of Coccidioidomycosis. Journal of Fungi. 2022; 8(7):666. https://doi.org/10.3390/jof8070666
Chicago/Turabian StyleWilliams, Samantha L., and Tom Chiller. 2022. "Update on the Epidemiology, Diagnosis, and Treatment of Coccidioidomycosis" Journal of Fungi 8, no. 7: 666. https://doi.org/10.3390/jof8070666