
Prevalence and Associated Factors of Cryptococcal Antigenemia in HIV-Infected Patients with CD4 < 200 Cells/µL in São Paulo, Brazil: A Bayesian Analysis
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Follow Up
2.2. Lateral Flow Assay
2.3. Ethics
2.4. Statistical Analyses
3. Results
3.1. Prevalence of Positive Antigenemia
3.2. Follow-Up of Patients with Positive LFA
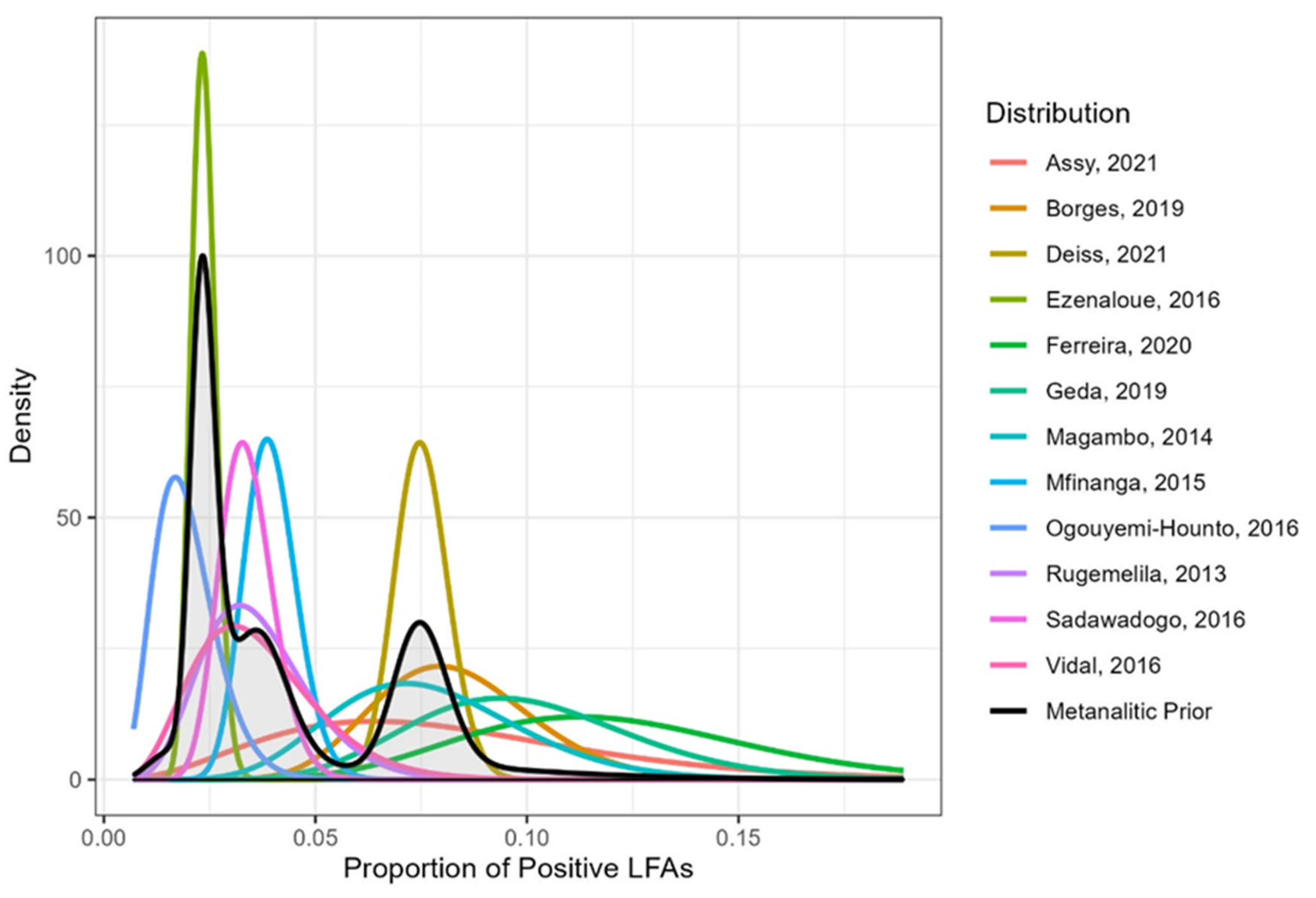
3.3. Prevalence of LFA Positivity by Bayesian Analysis in 13 Studies
3.4. Mortality Rates in Positive LFA and Negative LFA Groups: Bayesian Analysis in Three Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rajasingham, R.; Smith, R.M.; Park, B.J.; Jarvis, J.N.; Govender, N.P.; Chiller, T.M.; Denning, D.W.; Loyse, A.; Boulware, D.R. Global burden of disease of HIV-associated cryptococcal meningitis: An updated analysis. Lancet Infect. Dis. 2017, 17, 873–881. [Google Scholar] [CrossRef] [Green Version]
- Rajasingham, R.; Govender, N.P.; Jordan, A.; Loyse, A.; Shroufi, A.; Denning, D.W.; Meya, D.B.; Chiller, T.M.; Boulware, D.R. The global burden of HIV-associated cryptococcal infection in adults in 2020: A modelling analysis. Lancet Infect. Dis. 2022, 22, 1748–1755. [Google Scholar] [CrossRef] [PubMed]
- N DANGER: UNAIDS Global AIDS Update 2022. Geneva: Joint United Nations Programme on HIV/AIDS. 2022. Licence: CC BY-NC-SA 3.0 IGO. Available online: https://www.unaids.org/sites/default/files/media_asset/2022-global-aids-update_en.pdf (accessed on 1 September 2022).
- Guidelines for Diagnosing, Preventing and Managing Cryptococcal Disease among Adults, Adolescents and Children Living with HIV; World Health Organization: Geneva, Switzerland, 2022; ISBN 978-92-4-005217-8/978-92-4-005218-5.
- Prado, M.; Da Silva, M.B.; Laurenti, R.; Travassos, L.R.; Taborda, C.P. Mortality due to systemic mycoses as a primary cause of death or in association with AIDS in Brazil: A review from 1996 to 2006. Mem. Inst. Oswaldo Cruz. 2009, 104, 513–521. [Google Scholar] [CrossRef] [Green Version]
- Soares, E.A.; Lazera, M.D.S.; Wanke, B.; Ferreira, M.D.F.; Oliveira, R.D.V.C.D.; Oliveira, A.G.; Coutinho, Z.F. Mortality by cryptococcosis in Brazil from 2000 to 2012: A descriptive epidemiological study. PLoS Neglected Trop. Dis. 2019, 13, e0007569. [Google Scholar] [CrossRef] [Green Version]
- Carmona, S.; Bor, J.; Nattey, C.; Maughan-Brown, B.; Maskew, M.; Fox, M.P.; Glencross, D.K.; Ford, N.; MacLeod, W.B. Persistent High Burden of Advanced HIV Disease Among Patients Seeking Care in South Africa’s National HIV Program: Data from a Nationwide Laboratory Cohort. Clin. Infect. Dis. 2018, 66, S111–S117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, B.J.; Wannemuehler, K.A.; Marston, B.J.; Govender, N.; Pappas, P.G.; Chiller, T.M. Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. Aids 2009, 23, 525–530. [Google Scholar] [CrossRef]
- Firacative, C.; Lizarazo, J.; Illnait-Zaragozí, M.T.; Castañeda, E. Latin American Cryptococcal Study Group The status of cryptococcosis in Latin America. Mem. Inst. Oswaldo Cruz. 2018, 113, e170554. [Google Scholar] [CrossRef] [Green Version]
- Lizarazo, J.; Chaves, O.; Peña, Y.; Escandón, P.; Agudelo, C.I.; Castañeda, E. Comparación de los hallazgos clínicos y de supervivencia entre pacientes VIH positivos y VIH negativos con criptococosis meníngea en un hospital del tercer nivel. Acta Médica Colombiana 2012, 37, 49–61. [Google Scholar]
- Leimann, B.C.Q.; Koifman, R.J. Cryptococcal meningitis in Rio de Janeiro State, Brazil, 1994–2004. Cad. Saude Publica 2008, 24, 2582–2592. [Google Scholar] [CrossRef] [Green Version]
- Hasimoto e Souza, L.K.; Costa, C.R.; Fernandes, O.F.; Abrão, F.Y.; Silva, T.C.; Treméa, C.M.; Silva, M.R.R. Clinical and microbiological features of cryptococcal meningitis. Rev. Soc. Bras. Med. Trop. 2013, 46, 343–347. [Google Scholar] [CrossRef]
- Vidal, J.E.; de Oliveira, A.C.P.; Dauar, R.F.; Boulware, D.R. Strategies to reduce mortality and morbidity due to AIDS-related cryptococcal meningitis in Latin America. Braz. J. Infect. Dis. 2013, 17, 353–362. [Google Scholar] [CrossRef]
- Guidelines for Managing Advanced HIV Disease and Rapid Initiation of Antiretroviral Therapy, July 2017. Geneva: World Health Organization. 2017. Licence: CC BY-NC-SA 3.0 IGO. Available online: https://apps.who.int/iris/handle/10665/44786 (accessed on 8 August 2022).
- Guidelines for the Diagnosis, Prevention and Management of Cryptococcal Disease in HIV-Infected Adults, Adolescents and Children Supplement to the 2016 Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV infection March 2018. Available online: https://WHO-CDS-HIV-18.2-eng.pdf (accessed on 15 August 2022).
- Jarvis, J.N.; Harrison, T.S.; Lawn, S.D.; Meintjes, G.; Wood, R.; Cleary, S. Cost Effectiveness of Cryptococcal Antigen Screening as a Strategy to Prevent HIV-Associated Cryptococcal Meningitis in South Africa. PLoS ONE 2013, 8, e69288. [Google Scholar] [CrossRef] [Green Version]
- Rajasingham, R.; Meya, D.B.; Greene, G.S.; Jordan, A.; Nakawuka, M.; Chiller, T.M.; Boulware, D.R.; Larson, B.A. Evaluation of a national cryptococcal antigen screening program for HIV-infected patients in Uganda: A cost-effectiveness modeling analysis. PLoS ONE 2019, 14, e0210105. [Google Scholar] [CrossRef] [Green Version]
- French, N.; Gray, K.; Watera, C.; Nakiyingi, J.; Lugada, E.; Moore, M.; Lalloo, D.; Whitworth, J.A.G.; Gilks, C.F. Cryptococcal infection in a cohort of HIV-1-infected Ugandan adults. Aids 2002, 16, 1031–1038. [Google Scholar] [CrossRef]
- Mfinanga, S.; Chanda, D.; Kivuyo, S.L.; Guinness, L.; Bottomley, C.; Simms, V.; Chijoka, C.; Masasi, A.; Kimaro, G.; Ngowi, B.; et al. Cryptococcal meningitis screening and community-based early adherence support in people with advanced HIV infection starting antiretroviral therapy in Tanzania and Zambia: An open-label, randomised controlled trial. Lancet 2015, 385, 2173–2182. [Google Scholar] [CrossRef]
- Magambo, K.A.; Kalluvya, S.E.; Kapoor, S.W.; Seni, J.; Chofle, A.A.; Fitzgerald, D.W.; Downs, J.A. Utility of urine and serum lateral flow assays to determine the prevalence and predictors of cryptococcal antigenemia in HIV-positive outpatients beginning antiretroviral therapy in Mwanza, Tanzania. J. Int. AIDS Soc. 2014, 17, 19040. [Google Scholar] [CrossRef]
- Rugemalila, J.; Maro, V.P.; Kapanda, G.; Ndaro, A.J.; Jarvis, J.N. Cryptococcal antigen prevalence in HIV-infected Tanzanians: A cross-sectional study and evaluation of a point-of-care lateral flow assay. Trop. Med. Int. Health 2013, 18, 1075–1079. [Google Scholar] [CrossRef]
- Vidal, J.E.; Boulware, D. Lateral flow assay for cryptococcal antigen: An important advance to improve the continuum of HIV care and reduce cryptococcal meningitis-related mortality. Rev. Inst. Med. Trop. Sao Paulo 2015, 57 (Suppl. 19), 38–45. [Google Scholar] [CrossRef]
- Vidal, J.E.; Toniolo, C.; Paulino, A.; Colombo, A.; Martins, M.d.A.; Meira, C.S.; Pereira-Chioccola, V.L.; Figueiredo -Mello, C.; Barros, T.; Duarte, J.; et al. Asymptomatic cryptococcal antigen prevalence detected by lateral flow assay in hospitalised HIV-infected patients in São Paulo, Brazil. Trop. Med. Int. Health 2016, 21, 1539–1544. [Google Scholar] [CrossRef]
- Sawadogo, S.; Makumbi, B.; Purfield, A.; Ndjavera, C.; Mutandi, G.; Maher, A.; Kaindjee-Tjituka, F.; Kaplan, J.E.; Park, B.J.; Lowrance, D.W. Estimated Prevalence of Cryptococcus Antigenemia (CrAg) among HIV-Infected Adults with Advanced Immunosuppression in Namibia Justifies Routine Screening and Preemptive Treatment. PLoS ONE 2016, 11, e0161830. [Google Scholar] [CrossRef] [Green Version]
- Ogouyèmi-Hounto, A.; Zannou, D.M.; Ayihounton, G.; Ahouada, A. Prevalence and factors associated with cryptococcal antigenemia in HIV-infected patients in Cotonou/Benin. J. Mycol. Méd. 2016, 26, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Ezeanolue, E.E.; Nwizu, C.; Greene, G.S.; Amusu, O.; Chukwuka, C.; Ndembi, N.; Smith, R.M.; Chiller, T.; Pharr, J.; Kozel, T.R. Brief Report: Geographical Variation in Prevalence of Cryptococcal Antigenemia Among HIV-Infected, Treatment-Naive Patients in Nigeria: A Multicenter Cross-Sectional Study. Mycoses 2020, 63, 145–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, M.F.; Santos, F.B.; Thrilles, L.; Almeida, M.A.; Wanke, B.; Veloso, V.G.; Nunes, E.P.; Lazera, M.S. Cryptococcal antigenemia prevalence and clinical data in HIV—Infected patients from the reference at INI-FIOCRUZ, Rio de Janeiro, Southeast of Brazil. Mycoses 2020, 63, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Borges, M.A.S.B.; de Araújo Filho, J.A.; Oliveira, B.J.S.; Moreira, I.S.; de Paula, V.V.; de Bastos, A.L.; Soares, R.B.A.; Turchi, M.D. Prospective cohort of AIDS patients screened for cryptococcal antigenaemia, preemptively treated and followed in Brazil. PLoS ONE. 2019, 14, e0219928. [Google Scholar] [CrossRef]
- Assy, J.G.P.L.; Said, R.C.; Pinheiro, O.C.; Brandão, A.S.; Boulware, D.R.; França, F.O.S.; Vidal, J.E. High prevalence of Cryptococcal antigenemia using a finger-prick lateral flow assay in individuals with advanced HIV disease in Santarém Municipality, Brazilian Amazon Basin. Med. Mycol. 2021, 59, 909–915. [Google Scholar] [CrossRef] [PubMed]
- Geda, N.; Beyene, T.; Dabsu, R.; Mengist, H.M. Prevalence of Cryptococcal Antigenemia and associated factors among HIV/AIDS patients on second-line antiretroviral therapy at two hospitals in Western Oromia, Ethiopia. PLoS ONE 2019, 14, e0225691. [Google Scholar] [CrossRef] [Green Version]
- Deiss, R.; Loreti, C.V.; Gutierrez, A.G.; Filipe, E.; Tatia, M.; Issufo, S.; Ciglenecki, I.; Loarec, A.; Vivaldo, H.; Barra, C.; et al. High burden of cryptococcal antigenemia and meningitis among patients presenting at an emergency department in Maputo, Mozambique. PLoS ONE 2021, 16, e0250195. [Google Scholar] [CrossRef]
- Jarvis, J.N.; Lawn, S.D.; Vogt, M.; Bangani, N.; Wood, R.; Harrison, T.S. Screening for Cryptococcal antigenaemia in patients accessing an antiretroviral treatment program in South Africa. Clin. Infect. Dis. 2009, 48, 856–862. [Google Scholar] [CrossRef]
- Vianna, C.M.D.M.; Mosegui, G.B.G. Cost-effectiveness analysis and budgetary impact of the Cryptococcal Antigen Lateral Flow Assay (CRAG-LFA) implementation for the screening and diagnosis of cryptococcosis in asymptomatic people living with HIV in Brazil. Rev. Inst. Med. Trop. S. Paulo 2021, 63, e57. [Google Scholar] [CrossRef]
- Berry, D.A. Bayesian clinical trials. Nat. Rev. Drug Discov. 2006, 5, 27–36. [Google Scholar] [CrossRef]
- Lee, J.; Chu, C.T. Bayesian clinical trials in action. Stat. Med. 2012, 31, 2955–2972. [Google Scholar]
- Gomes, L.S.; Polpo, A.C.; Pereira, C.B.; Martins, C.A.B. Calculadora Metanalítica: Interface gráfica para metanálise bayesiana de proporções (in portuguese). Revista Brasileira de Biometria 2019, 37, 32–40. [Google Scholar] [CrossRef]
- Martins, C.B.; Pereira, C.A.D.B.; Polpo, A. Bayesian meta-analytic measure. In International Workshop on Bayesian Inference and Maximum Entropy Methods in Science and Engineering; Springer: Cham, Switzerland, 2017; pp. 37–42. [Google Scholar]
- Pereira, C.A.B.; Stern, J.M. Evidence and credibility: Full Bayesian significance test for precise hypotheses. Entropy 1999, 1, 99–110. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 8 August 2022).
- Team, R. Rstudio: Integrated Development Environment for r. Rstudio, pbc, Boston, ma. 2020. Available online: http://www.rstudio.com (accessed on 8 August 2022).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; ISBN 978-3-319-24277-4. Available online: https://ggplot2.tidyverse.org (accessed on 8 August 2022).
- Ford, N.; Shubber, Z.; Jarvis, J.N.; Chiller, T.; Greene, G.; Migone, C.; Vitoria, M.; Doherty, M.; Meintjes, G. CD4 Cell Count Threshold for Cryptococcal Antigen Screening of HIV-Infected Individuals: A Systematic Review and Meta-analysis. Clin. Infect. Dis. 2018, 66, S152–S159. [Google Scholar] [CrossRef]
- Li, Y.; Huang, X.; Chen, H.; Qin, Y.; Hou, J.; Li, A.; Wu, H.; Yan, X.; Chen, Y. The prevalence of cryptococcal antigen (CrAg) and benefits of pre-emptive antifungal treatment among HIV-infected persons with CD4+ T-cell counts < 200 cells/μL: Evidence based on a meta-analysis. BMC Infect. Dis. 2020, 20, 410. [Google Scholar] [CrossRef]
- Da Costa, M.M.; Madeira, L.D.P.; Feitosa, R.N.M.; Ishak, M.D.O.G.; Ishak, R.; Marques-Da-Silva, S.H.; Vallinoto, A.C.R. Detection of Cryptococcus neoformans Capsular Antigen in HIV-Infected Patients in the State of Para in the North of Brazil. Curr. HIV Res. 2014, 11, 647–651. [Google Scholar] [CrossRef]
- Kapoor, S.W.; Magambo, K.A.; Kalluvya, S.E.; Fitzgerald, D.W.; Peck, R.N.; Downs, J.A. Six-month outcomes of HIV-infected patients given short-course fluconazole therapy for asymptomatic cryptococcal antigenemia. AIDS 2015, 29, 2473–2478. [Google Scholar] [CrossRef] [Green Version]
- Micol, R.; Lortholary, O.; Sar, B.; Laureillard, D.; Ngeth, C.; Dousset, J.-P.; Chanroeun, H.; Ferradini, L.; Guerin, P.J.; Dromer, F.; et al. Prevalence, Determinants of Positivity, and Clinical Utility of Cryptococcal Antigenemia in Cambodian HIV-Infected Patients. Am. J. Ther. 2007, 45, 555–559. [Google Scholar] [CrossRef]
- Osazuwa, O.F.; Dirisu, O.; Okuonghae, E. Cryptococcal antigenemia in anti-retroviral naïve AIDS patients: Prevalence and its association with CD4 cell count. Acta Medica Iran. 2012, 50, 344–347. [Google Scholar]
- Tugume, L.; Rhein, J.; Hullsiek, K.H.; Mpoza, E.; Kiggundu, R.; Ssebambulidde, K.; Schutz, C.; Taseera, K.; Williams, D.A.; Abassi, M.; et al. HIV-Associated Cryptococcal Meningitis Occurring at Relatively Higher CD4 Counts. J. Infect. Dis. 2018, 219, 877–883. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, J.N.; Tenforde, M.W.; Lechiile, K.; Milton, T.; Boose, A.; Leeme, T.B.; Tawe, L.; Muthoga, C.; Rukasha, I.; Mulenga, F.; et al. Evaluation of a Novel Semiquantitative Cryptococcal Antigen Lateral Flow Assay in Patients with Advanced HIV Disease. J. Clin. Microbiol. 2020, 58, e00441-20. [Google Scholar] [CrossRef] [PubMed]
- Meya, D.B.; Kiragga, A.N.; Nalintya, E.; Morawski, B.M.; Rajasingham, R.; Park, B.J.; Mubiru, A.; Kaplan, J.E.; Manabe, Y.C.; Boulware, D. Reflexive Laboratory-Based Cryptococcal Antigen Screening and Preemptive Fluconazole Therapy for Cryptococcal Antigenemia in HIV-Infected Individuals with CD4 <100 Cells/µL: A Stepped-Wedge, Cluster-Randomized Trial. JAIDS J. Acquir. Immune Defic. Syndr. 2019, 80, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, A.; Manabe, Y.; Rajasingham, R.; Shah, M. Cost-effectiveness of CRAG-LFA screening for cryptococcal meningitis among people living with HIV in Uganda. BMC Infect. Dis. 2017, 17, 225. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Muthoga, C.; Callaghan, A.; Ponatshego, P.; Ngidi, J.; Mine, M.; Jordan, A.; Chiller, T.; Larson, B.A.; Jarvis, J.N. Cost-effectiveness of reflex laboratory-based cryptococcal antigen screening for the prevention and treatment of cryptococcal meningitis in Botswana. Wellcome Open Res. 2020, 4, 144. [Google Scholar] [CrossRef]
- Brasil. Ministerio da Saude. Secretaria de Ciencia, Tecnologia, Inovacao e Insumos Estrategicos em Saude. Coordenacao de Monitoramento e Avaliacao de Tecnologias em Saude. Teste diagnostico, point of care, de Cryptococcal Antigen Lateral Flow Assay (CRAG-LFA) para deteccao de infeccao por Cryptococcus e diagnostico de meningite criptocócica em pessoas vivendo com o virus da imunodeficiencia humana (PVHIV). Brasilia: Ministerio da Saude. 2021. Available online: http://www.conitec.gov.br/images/Relatorios/2021/20210611_Relatorio_615_CragLFA_meningite-criptococica_Final.pdf (accessed on 22 June 2021).
- MS, Brazil. PORTARIA SCTIE/MS Nº 28, DE 9 DE JUNHO DE 2021. Secretaria de Ciência, Tecnologia, Inovação e Insumos Estratégicos em Saúde. Teste Diagnóstico, Point of Care, de Cryptococcal Antigen Lateral Flow Assay (CRAG-LFA) para Detecção de Infecção por Cryptococcus e Diagnóstico de Meningite Criptocócica em Pessoas Vivendo com o Vírus da Imunodeficiência Humana (PVHIV). Available online: https://bvsms.saude.gov.br/bvs/saudelegis/sctie/2021/prt0028_11_06_2021.html. (accessed on 24 August 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Sex | Age (Years) | Hospitalization | ART | Opportunistic Disease | Viral Load RNA Copies/μL | Time Since Diagnosis | Symptoms | Mortality a n/N (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n/N (%) | n/N (%) | n/N (%) | n/N (%) | n/N (%) | n/N (%) | n/N (%) | n/N (%) | |||||||||||
| F | M | <40 | >40 | No | Yes | Regular Use | Irregular Use | No | Yes | <1,000,000 | ≥100,000 | ≤12 mo | >12 mo | No | Yes | LFA+ | Negative LFA | |
| Rugemalila, 2013 | 5/124 (4.03%) | 2/94 (2.13%) | NA | NA | 7/218 (3.21%) | NA | 1/96 (1.04%) | 6/122 (4.92%) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Magambo, 2014 | 6/81 (7.41%) | 4/59 6.78% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Mfinanga, 2015 | NA | NA | NA | NA | 38/985 (3.86%) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 12/38 (31.6%) | 1120/947 (12.7%) |
| Ezenaloue, 2016 | 33/1570 (2.10%) | 31/1182 (2.62%) | NA | NA | 64/2752 (2.33%) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Ogouyemi-Hounto, 2016 | 3/205 (1.20%) | 3/150 (2.00%) | NA | NA | 6/355 (1.69%) | NA | 4/289 (1.38%) | 2/66 (3.03%) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Sadawadogo, 2016 | 11/374 (2.94%) | 16/440 (3.64%) | NA | NA | 27/825 (3.27%) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Vidal, 2016 | 2/64 (3.13%) | 3/99 (3.03%) | NA | NA | NA | 5/163 (3.07%) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Borges, 2019 | 3/59 (5.08%) | 14/155 (9.03%) | 11/112 (9.82%) | 6/102 (5.88%) | 13/168 (7.74%) | 4/46 (8.70%) | 11/110 (10.00%) | 6/104 (5.77%) | 4/107 (3.74%) | 13/107 (12.15%) | 10/104 (9.62%) | 7/110 (6.36%) | 7/101 (6.93%) | 10/113 (8.85%) | 13/139 (9.35%) | 4/75 (5.33%) | NA | NA |
| Ferreira 2020 | 5/28 (17.86%) | 5/61 (8.20%) | NA | NA | 10/89 (11.24%) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 4/10 (40.0) | 19/71 (26.8%) |
| Group | Subgroup | N (%) | Positive LFA (N) |
|---|---|---|---|
| Region of Birth | Southeast | 205 (74.0) | 6 |
| Northeast | 54 (19.5) | 2 | |
| Others | 18 (6.5) | 0 | |
| Race | White | 187 (67.5) | 4 |
| Afro-American | 81 (29.3) | 3 | |
| Others | 2 (0.7) | 0 | |
| No available | 7 (2.5) | 1 | |
| Age | ≤40 | 94 (34.0) | 3 |
| >40 | 183 (66.0) | 5 | |
| Sex | Female | 98 (35.4) | 5 |
| Male | 179 (64.6) | 3 | |
| Sexual Orientation a | Heterosexual | 166 (66.7) | 7 |
| Homosexual | 83 (33.3) | 1 | |
| Education | ≤8 years | 122 (44.0) | 4 |
| >9 years | 144 (52.0) | 3 | |
| Not available | 11 (4.0) | 1 | |
| Time Since Diagnosis b | ≤12 months | 76 (27.8) | 5 |
| >12 months | 197 (72.2) | 3 | |
| Hospitalization c | No | 106 (38.8) | 3 |
| Yes | 150 (61.2) | 5 | |
| Symptoms | No | 47 (17.0) | 1 |
| Yes | 230 (83.0) | 7 | |
| Opportunist Disease d | No | 104 (39.2) | 3 |
| Yes | 161 (60.8) | 5 | |
| CD4 (cells/μL) | 0–100 | 143 (51.6) | 5 |
| 100–200 | 134 (48.4) | 3 | |
| Viral Load (copies/μL) | <100.000 | 86 (31.0) | 2 |
| ≥100.000 | 191 (69.0) | 6 | |
| ART | Regular Use | 71 (25.6) | 2 |
| Irregular Use | 206 (74.4) | 6 | |
| Antifungal Use e | No | 243 (88.4) | 8 |
| Yes | 32 (11.6) | 0 | |
| Meningoencephalitis | No | 275 (99.3) | 6 |
| Yes | 2 (0.7) | 2 | |
| Mortality f | No Yes | 224 (87.2) 33 (12.8) | 07 01 |
| Patients | Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 | Patient 8 |
|---|---|---|---|---|---|---|---|---|
| Inclusion * | 02/10/2015 | 06/16/2015 | 07/23/2015 | 10/21/2015 | 02/16/2017 | 03/30/2017 | 04/05/2017 | 10/16/2017 |
| Hospitalization | Yes | No | No | Yes | No | Yes | Yes | Yes |
| Age (years)/Sex | 54/Male | 38/Female | 60/Female | 38/Female | 49/Male | 21/female | 40/Female | 54/male |
| Ethnicity | White | White | Afro-American | Afro-American | White | Afro-American | NA | White |
| State of birth | São Paulo | Pernambuco | São Paulo | São Paulo | Minas Gerais | São Paulo | Bahia | Minas Gerais |
| Date of HIV diagnosis | 02/01/2015 | 01/01/1997 | 11/01/2014 | 10/01/15 | 09/30/2003 | 02/01/2017 | 07/01/2005 | 09/02/2017 |
| Sexuality | Hetero | Hetero | Hetero | Hetero | Hetero | Hetero | NA | Bisexual |
| Opportunistic infections | Neurotoxo | Neurotoxo | Cachexia | Myelitis | No | KPC bacteriuria | Neurotoxo | Ocular syphilis |
| Symptoms at inclusion | No | No | No | Yes | No | Yes | Yes | Yes |
| CD4 cells/µL(inclusion) | 121 | 77 | 159 | 95 | 137 | 13 | 38 | 73 |
| RNA viral copies/µL (inclusion) | 8,602,804 | 1116 | <40 | 336 | <40 | 364 | 34,505 | 131,527 |
| LFA+ blood/CSF | POS/NA | POS/NA | POS/NA | POS/POS | POS/NA | POS/POS | POS/NA | POS/NA |
| Cryptococcosis | Pulmonary | No | No | Meningitis | No | Meningitis | No | No |
| Antifungal therapy | Fluconazole | refused LP abandonment | refused LP abandonment | Lipo Amp + fluconazole | refused LP, negative LFA in the blood two months later. | Lipo Amp + Fluconazole | Fluco Candida abandonment | abandonment |
| Outcome(m = months) | † sepsis 2.7 m | † sepsis 21 m | Alive 48 m | Alive 78 m | Alive 48 m | Alive 63.5 m | Alive 60 m | Alive 58 m |
| CD4 cells/µL ** | 04/06/2015 124 | 01/09/2017 20 | 06/07/2022 429 | 04/27/2022 377 | 01/20/2021 270 | 07/07/2022 455 | 05/28/2022 211 | 06/01/22 390 |
| RNA viral copies/µL ** | 860,804 | 165,608 | undetectable | undetectable | undetectable | undetectable | undetectable | undetectable |
| Last ART | 3tc/tdf/efv | NA | 3tc/dol | tdf/3tc/dol | tdf/3tc/efv | NA | NA | NA |
| Author, Year | CD4 < 100 Cells/µL | 100 < CD4 < 200 Cells/µL | e Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Cases | Estimate | HPD Ci | n | Cases | Estimate | HPD Ci | ||
| Borges_2019 [28] | 159 | 12 | 0.075 | [0.041; 0.123] | 55 | 5 | 0.091 | [0.034; 0.185] | |
| Deiss_2021 [31] | 897 | 103 | 0.115 | [0.095; 0.137] | 309 | 14 | 0.045 | [0.026; 0.072] | |
| Ezenaloue_2016 [26] | 1451 | 52 | 0.036 | [0.027; 0.047] | 1301 | 12 | 0.009 | [0.005; 0.016] | |
| Ferreira_2020 [27] | 56 | 7 | 0.125 | [0.056; 0.227] | 29 | 3 | 0.103 | [0.027; 0.245] | |
| Geda_2019 [30] | 85 | 10 | 0.118 | [0.061; 0.197] | 43 | 2 | 0.047 | [0.008; 0.139] | |
| Magambo_2014 [20] | 73 | 6 | 0.082 | [0.033; 0.160] | 67 | 4 | 0.060 | [0.019; 0.134] | |
| Mfinanga_2015 [19] | 717 | 33 | 0.046 | [0.032; 0.063] | 268 | 5 | 0.019 | [0.007; 0.040] | |
| Ogouyemi-Hounto_2016 [25] | 155 | 6 | 0.039 | [0.015; 0.077] | 200 | 0 | 0.000 | [0.000; 0.015] | |
| Rugemalila_2013 [21] | 124 | 6 | 0.048 | [0.019; 0.096] | 94 | 1 | 0.011 | [0.000; 0.049] | |
| Sadawadogo_2016 [24] | 511 | 20 | 0.039 | [0.025; 0.058] | 302 | 7 | 0.023 | [0.010; 0.045] | |
| Vidal_2016 [23] | 128 | 4 | 0.031 | [0.010; 0.072] | 35 | 1 | 0.029 | [0.001; 0.126] | |
| Mimicos_2021 [present study) | 143 | 5 | 0.035 | [0.013; 0.074] | 134 | 3 | 0.022 | [0.005; 0.058] | |
| Bayesian Analysis | - | - | 0.036 | [0.025; 0.057] | - | - | 0.011 | [0.005; 0.043] | 0.307 |
| Group | Subgroup | Estimate | HPD Ci | e-Value |
|---|---|---|---|---|
| CD4 | 0–100 | 0.036 | [0.025; 0.057] | 0.307 |
| 100–200 | 0.011 | [0.005; 0.043] | ||
| Sex | Female | 0.023 | [0.015; 0.069] | 0.975 |
| Male | 0.025 | [0.013; 0.039] | ||
| Hospitalization | No | 0.024 | [0.017; 0.047] | 0.896 |
| Yes | 0.030 | [0.014; 0.056] | ||
| Antiretroviral Therapy | Regular Use | 0.017 | [0.004; 0.047] | 0.418 |
| Irregular Use | 0.035 | [0.017; 0.061] | ||
| Age | ≤40 | 0.067 | [0.038; 0.10] | 0.387 |
| >40 | 0.039 | [0.02; 0.066] | ||
| Opportunist Disease | No | 0.027 | [0.011; 0.054] | 0.064 |
| Yes | 0.073 | [0.045; 0.108] | ||
| Viral Load | <100.000 copies/μL | 0.063 | [0.034; 0.104] | 0.626 |
| ≥100.000 copies/μL | 0.043 | [0.024; 0.070] | ||
| Time Since Diagnosis | ≤12 months | 0.067 | [0.037; 0.111] | 0.499 |
| >12 months | 0.042 | [0.023; 0.069] | ||
| Symptoms | No | 0.075 | [0.043; 0.119] | 0.172 |
| Yes | 0.036 | [0.019; 0.061] | ||
| Antifungal Use | No | 0.033 | [0.015; 0.061] | 0.565 |
| Yes | 0.000 | [0.000; 0.087] |
| Mortality | Groups | Estimate | HPD Ci | e-Value |
|---|---|---|---|---|
| LFA | Negative LFA | 0.127 | [0.109; 0.147] | 0.05013 |
| Positive LFA | 0.282 | [0.157; 0.434] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mimicos, E.V.; Fossaluza, V.; Picone, C.d.M.; de Sena, C.C.; Gomes, H.R.; Lázari, C.d.S.; Silva, F.F.d.; Nakanishi, E.S.; Nisida, I.V.; Freitas, A.C.; et al. Prevalence and Associated Factors of Cryptococcal Antigenemia in HIV-Infected Patients with CD4 < 200 Cells/µL in São Paulo, Brazil: A Bayesian Analysis. J. Fungi 2022, 8, 1284. https://doi.org/10.3390/jof8121284
Mimicos EV, Fossaluza V, Picone CdM, de Sena CC, Gomes HR, Lázari CdS, Silva FFd, Nakanishi ES, Nisida IV, Freitas AC, et al. Prevalence and Associated Factors of Cryptococcal Antigenemia in HIV-Infected Patients with CD4 < 200 Cells/µL in São Paulo, Brazil: A Bayesian Analysis. Journal of Fungi. 2022; 8(12):1284. https://doi.org/10.3390/jof8121284
Chicago/Turabian StyleMimicos, Evanthia Vetos, Victor Fossaluza, Camila de Melo Picone, Camila Caroline de Sena, Hélio Rodrigues Gomes, Carolina dos Santos Lázari, Fernanda Ferreira da Silva, Erika Shimoda Nakanishi, Isabelle Vichr Nisida, Angela Carvalho Freitas, and et al. 2022. "Prevalence and Associated Factors of Cryptococcal Antigenemia in HIV-Infected Patients with CD4 < 200 Cells/µL in São Paulo, Brazil: A Bayesian Analysis" Journal of Fungi 8, no. 12: 1284. https://doi.org/10.3390/jof8121284