
Identification of Pneumocystis jirovecii with Fluorescence In-Situ Hybridization (FISH) in Patient Samples—A Proof-of-Principle

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Paraffin-Embedded Tissue Samples
2.2. Deep Airway Secretions
2.3. In Silico Evaluation of the FISH Probe
2.4. P. jirovecii FISH-Protocol with Paraffin-Embedded Tissue Samples
2.5. P. jirovecii FISH Protocol with Deep Airway Secretions
2.6. Ethics
3. Results
3.1. In Silico Evaluation
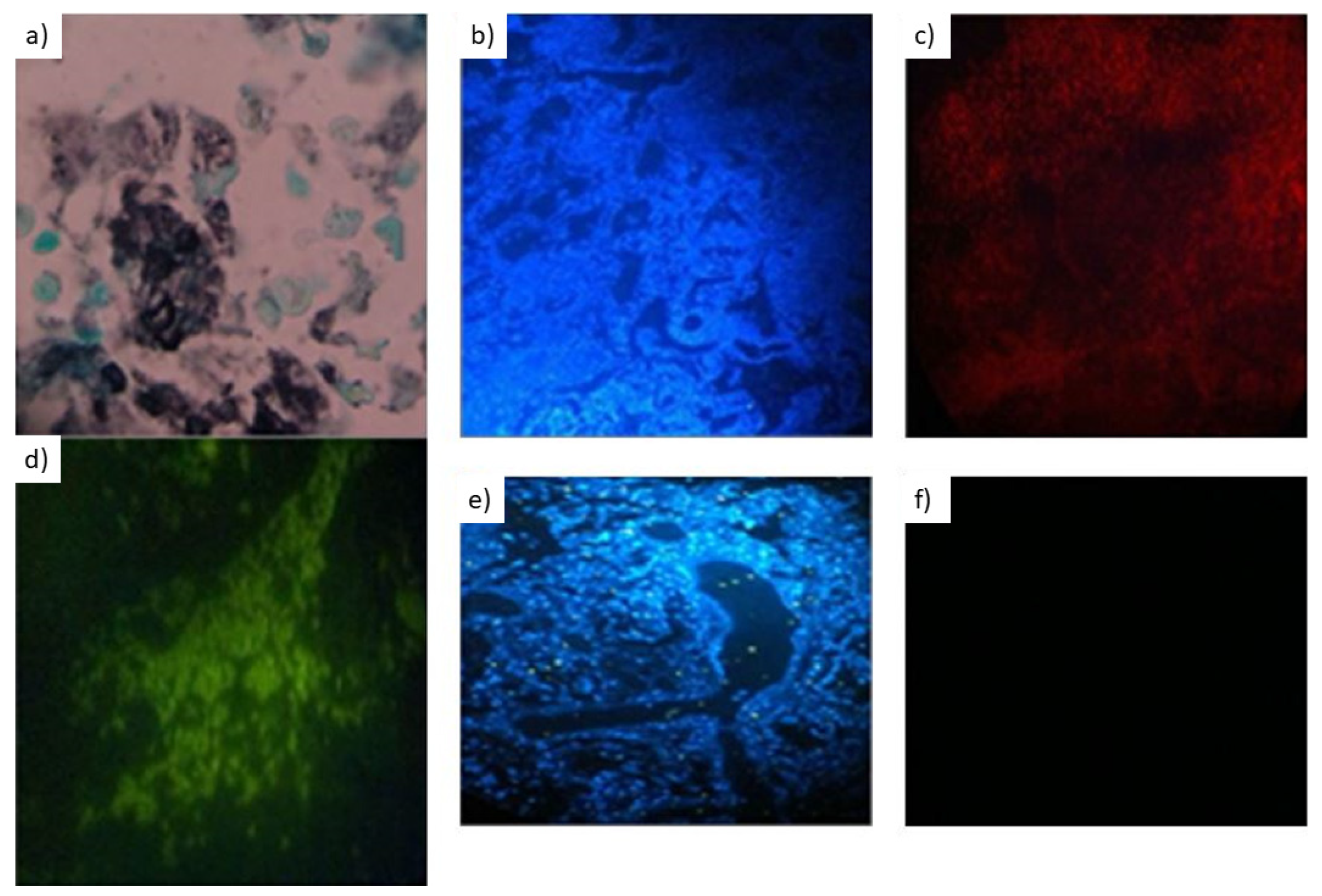
3.2. In Vitro Evaluation with Paraffin-Embedded Tissue Samples
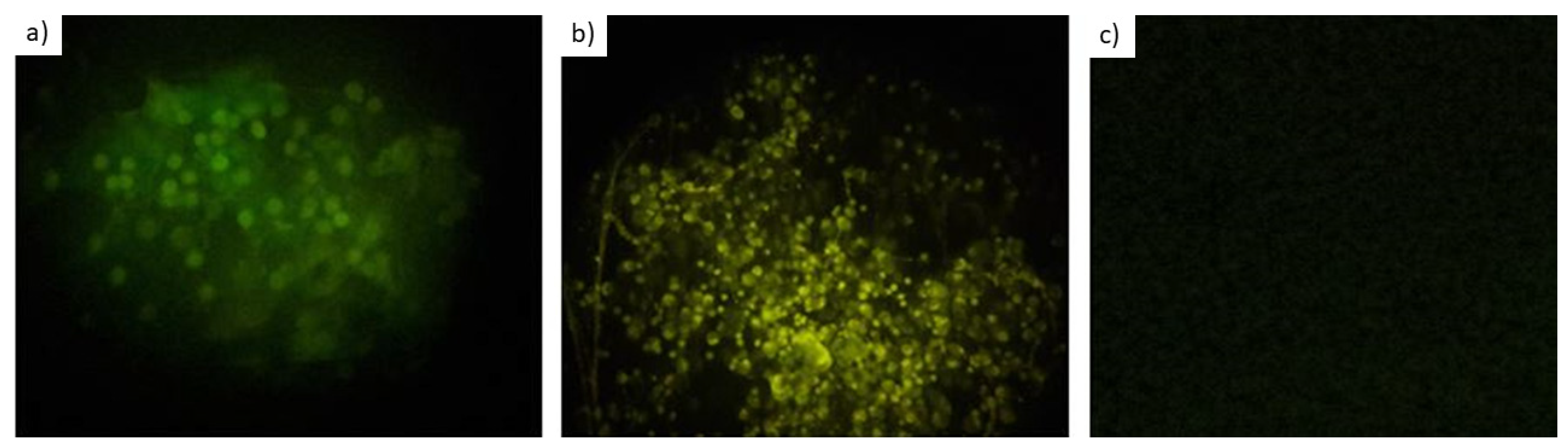
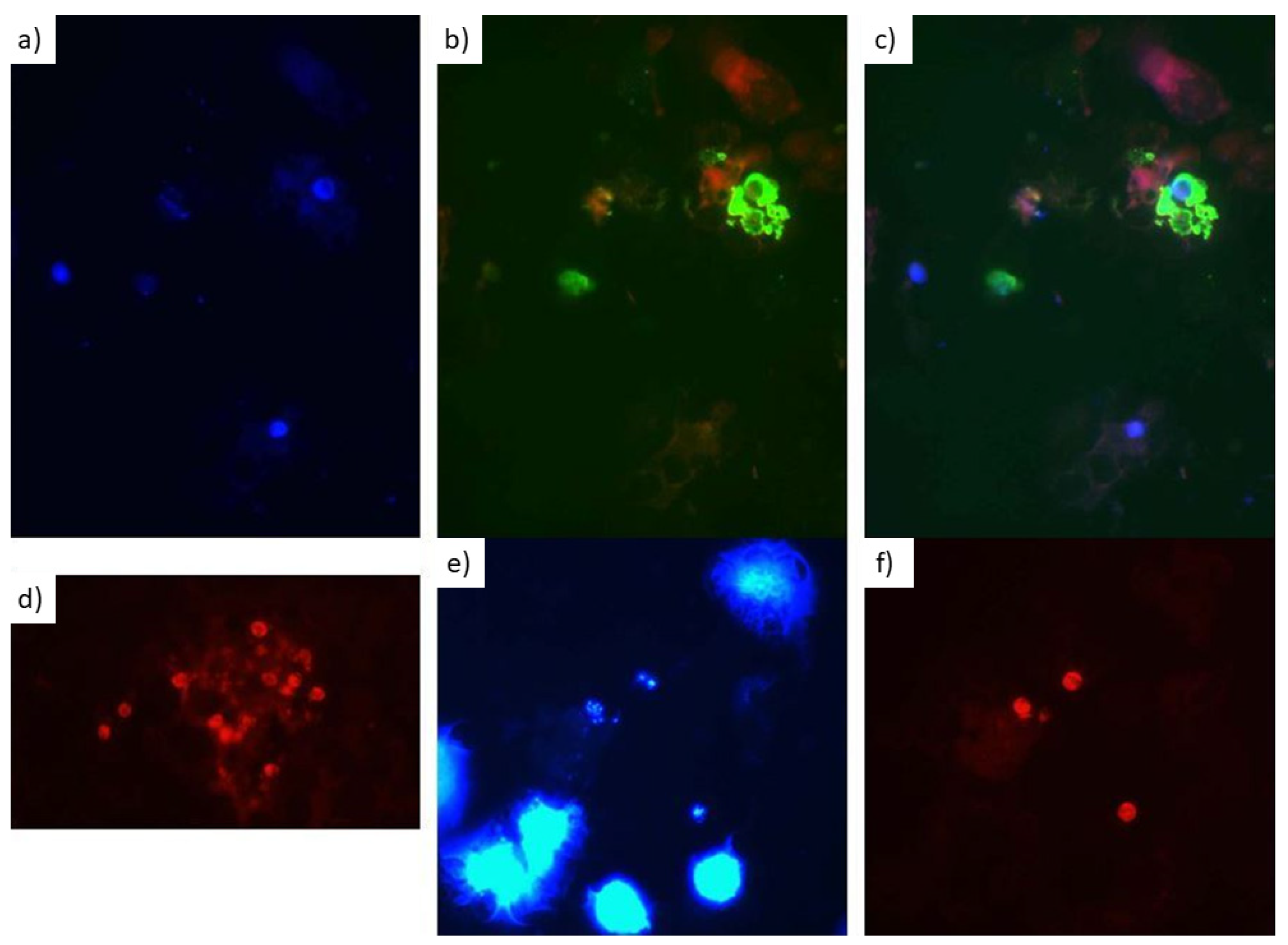
3.3. In Vitro Evaluation with Respiratory Secretions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zalmanovich, A.; Ben-Ami, R.; Rahav, G.; Alon, D.; Moses, A.; Olshtain-Pops, K.; Weinberger, M.; Shitrit, P.; Katzir, M.; Gottesman, B.S.; et al. Healthcare-associated Pneumocystis jirovecii Pneumonia (PJP) Infection in HIV-negative Adults: A Multicenter Study. Isr. Med. Assoc. J. 2021, 23, 312–317. [Google Scholar]
- Salzer, H.J.F.; Schäfer, G.; Hoenigl, M.; Günther, G.; Hoffmann, C.; Kalsdorf, B.; Alanio, A.; Lange, C. Clinical, Diagnostic, and Treatment Disparities between HIV-Infected and Non-HIV-Infected Immunocompromised Patients with Pneumocystis jirovecii Pneumonia. Respiration 2018, 96, 52–65. [Google Scholar] [CrossRef]
- Avino, L.J.; Naylor, S.M.; Roecker, A.M. Pneumocystis jirovecii Pneumonia in the Non–HIV-Infected Population. Ann. Pharmacother. 2016, 50, 673–679. [Google Scholar] [CrossRef]
- Weyant, R.B.; Kabbani, D.; Doucette, K.; Lau, C.; Cervera, C. Pneumocystis jirovecii: A review with a focus on prevention and treatment. Expert Opin. Pharmacother. 2021, 22, 1579–1592. [Google Scholar] [CrossRef]
- Catherinot, E.; Lanternier, F.; Bougnoux, M.E.; Lecuit, M.; Couderc, L.J.; Lortholary, O. Pneumocystis jirovecii Pneumonia. Infect. Dis. Clin. North. Am. 2010, 24, 107–138. [Google Scholar] [CrossRef]
- Sokulska, M.; Kicia, M.; Wesołowska, M.; Hendrich, A.B. Pneumocystis jirovecii—from a commensal to pathogen: Clinical and diagnostic review. Parasitol. Res. 2015, 114, 3577–3585. [Google Scholar] [CrossRef] [Green Version]
- Thomas, C.F., Jr.; Limper, A.H. Pneumocystis pneumonia. N. Engl. J. Med. 2004, 350, 2487–2498. [Google Scholar] [CrossRef]
- Bateman, M.; Oladele, R.; Kolls, J.K. Diagnosing Pneumocystis jirovecii pneumonia: A review of current methods and novel approaches. Med. Mycol. 2020, 58, 1015–1028. [Google Scholar] [CrossRef]
- Del Corpo, O.; Butler-Laporte, G.; Sheppard, D.C.; Cheng, M.P.; McDonald, E.G.; Lee, T.C. Diagnostic accuracy of serum (1-3)-β-D-glucan for Pneumocystis jirovecii pneumonia: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1137–1143. [Google Scholar] [CrossRef]
- Bille, J. New nonculture-based methods for the diagnosis of invasive candidiasis. Curr. Opin. Crit. Care 2010, 16, 460–464. [Google Scholar] [CrossRef]
- Bisha, B.; Kim, H.J.; Brehm-Stecher, B.F. Improved DNA-FISH for cytometric detection of Candida spp. J. Appl. Microbiol. 2011, 110, 881–892. [Google Scholar] [CrossRef] [PubMed]
- Farina, C.; Perin, S.; Andreoni, S.; Conte, M.; Fazii, P.; Lombardi, G.; Manso, E.; Morazzoni, C.; Sanna, S. Evaluation of the peptide nucleic acid fluorescence in situ hybridisation technology for yeast identification directly from positive blood cultures: An Italian experience. Mycoses 2012, 55, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Forrest, G.N.; Mankes, K.; Jabra-Rizk, M.A.; Weekes, E.; Johnson, J.K.; Lincalis, D.P.; Venezia, R.A. Peptide nucleic acid fluorescence in situ hybridization-based identification of Candida albicans and its impact on mortality and antifungal therapy costs. J. Clin. Microbiol. 2006, 44, 3381–3383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frickmann, H.; Zautner, A.E.; Moter, A.; Kikhney, J.; Hagen, R.M.; Stender, H.; Poppert, S. Fluorescence in situ hybridization (FISH) in the microbiological diagnostic routine laboratory: A review. Crit. Rev. Microbiol. 2017, 43, 263–293. [Google Scholar] [CrossRef]
- Frickmann, H.; Lakner, A.; Essig, A.; Poppert, S. Rapid identification of yeast by fluorescence in situ hybridisation from broth and blood cultures. Mycoses 2012, 55, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Gherna, M.; Merz, W.G. Identification of Candida albicans and Candida glabrata within 1.5 hours directly from positive blood culture bottles with a shortened peptide nucleic acid fluorescence in situ hybridization protocol. J. Clin. Microbiol. 2009, 47, 247–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, L.; Le Febre, K.M.; Deml, S.M.; Wohlfiel, S.L.; Wengenack, N.L. Evaluation of the Yeast Traffic Light PNA FISH probes for identification of Candida species from positive blood cultures. J. Clin. Microbiol. 2012, 50, 1446–1448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, D.M.; Hata, D.J. Rapid identification of bacteria and Candida using PNA-FISH from blood and peritoneal fluid cultures: A retrospective clinical study. Ann. Clin. Microbiol. Antimicrob. 2013, 12, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inácio, J.; da Luz Martins, M. Microscopic detection of yeasts using fluorescence in situ hybridization. Methods Mol. Biol. 2013, 968, 71–82. [Google Scholar]
- Kempf, V.A.; Trebesius, K.; Autenrieth, I.B. Fluorescent In situ hybridization allows rapid identification of microorganisms in blood cultures. J. Clin. Microbiol. 2000, 38, 830–838. [Google Scholar] [CrossRef] [Green Version]
- Lakner, A.; Essig, A.; Frickmann, H.; Poppert, S. Evaluation of fluorescence in situ hybridisation (FISH) for the identification of Candida albicans in comparison with three phenotypic methods. Mycoses 2012, 55, e114–e123. [Google Scholar] [CrossRef]
- Martins, M.L.; Ferreira, A.S.; Sampaio, A.; Vieira, R.; Inácio, J. Direct and specific identification of Cryptococcus neoformans in biological samples using fluorescently labelled DNA probes. Eur. J. Clin. Microbiol. Infect. Dis. 2010, 29, 571–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, K.; Haase, G.; Kurtzman, C.; Hyldig-Nielsen, J.J.; Stender, H. Differentiation of Candida albicans and Candida dubliniensis by fluorescent in situ hybridization with peptide nucleic acid probes. J. Clin. Microbiol. 2001, 39, 4138–4141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rickerts, V.; Khot, P.D.; Myerson, D.; Ko, D.L.; Lambrecht, E.; Fredricks, D.N. Comparison of quantitative real time PCR with Sequencing and ribosomal RNA-FISH for the identification of fungi in formalin fixed, paraffin-embedded tissue specimens. BMC Infect. Dis. 2011, 11, 202. [Google Scholar] [CrossRef] [Green Version]
- Rigby, S.; Procop, G.W.; Haase, G.; Wilson, D.; Hall, G.; Kurtzman, C.; Oliveira, K.; Von Oy, S.; Hyldig-Nielsen, J.J.; Coull, J.; et al. Fluorescence in situ hybridization with peptide nucleic acid probes for rapid identification of Candida albicans directly from blood culture bottles. J. Clin. Microbiol. 2002, 40, 2182–2186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shepard, J.R.; Addison, R.M.; Alexander, B.D.; Della-Latta, P.; Gherna, M.; Haase, G.; Hall, G.; Johnson, J.K.; Merz, W.G.; Peltroche-Llacsahuanga, H.; et al. Multicenter evaluation of the Candida albicans/Candida glabrata peptide nucleic acid fluorescent in situ hybridization method for simultaneous dual-color identification of C. albicans and C. glabrata directly from blood culture bottles. J. Clin. Microbiol. 2008, 46, 50–55. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, R.M., Jr.; da Silva Neto, J.R.; Santos, C.S.; Cruz, K.S.; Frickmann, H.; Poppert, S.; Koshikene, D.; de Souza, J.V. Fluorescent in situ hybridization of pre-incubated blood culture material for the rapid diagnosis of histoplasmosis. Med. Mycol. 2015, 53, 160–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Silva, R.M., Jr.; Da Silva Neto, J.R.; Santos, C.S.; Frickmann, H.; Poppert, S.; Cruz, K.S.; Koshikene, D.; De Souza, J.V. Evaluation of fluorescence in situ hybridisation (FISH) for the detection of fungi directly from blood cultures and cerebrospinal fluid from patients with suspected invasive mycoses. Ann. Clin. Microbiol. Antimicrob. 2015, 14, 6. [Google Scholar] [CrossRef] [Green Version]
- Stone, N.R.; Gorton, R.L.; Barker, K.; Ramnarain, P.; Kibbler, C.C. Evaluation of PNA-FISH yeast traffic light for rapid identification of yeast directly from positive blood cultures and assessment of clinical impact. J. Clin. Microbiol. 2013, 51, 1301–1302. [Google Scholar] [CrossRef] [Green Version]
- Trnovsky, J.; Merz, W.; Della-Latta, P.; Wu, F.; Arendrup, M.C.; Stender, H. Rapid and accurate identification of Candida albicans isolates by use of PNA FISHFlow. J. Clin. Microbiol. 2008, 46, 1537–1540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, D.A.; Joyce, M.J.; Hall, L.S.; Reller, L.B.; Roberts, G.D.; Hall, G.S.; Alexander, B.D.; Procop, G.W. Multicenter evaluation of a Candida albicans peptide nucleic acid fluorescent in situ hybridization probe for characterization of yeast isolates from blood cultures. J. Clin. Microbiol. 2005, 43, 2909–2912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Churukian, C.J.; Schenk, E.A. Rapid Grocott’s methenamine—Silver nitrate method for fungi and Pneumocystis carinii. Am. J. Clin. Pathol. 1977, 68, 427–428. [Google Scholar] [CrossRef]
- Shalin, S.C.; Ferringer, T.; Cassarino, D.S. PAS and GMS utility in dermatopathology: Review of the current medical literature. J. Cutan. Pathol. 2020, 47, 1096–1102. [Google Scholar] [CrossRef] [PubMed]
- Gits-Muselli, M.; White, P.L.; Mengoli, C.; Chen, S.; Crowley, B.; Dingemans, G.; Fréalle, E.L.; Gorton, R.; Guiver, M.; Hagen, F.; et al. The Fungal PCR Initiative’s evaluation of in-house and commercial Pneumocystis jirovecii qPCR assays: Toward a standard for a diagnostics assay. Med. Mycol. 2020, 58, 779–788. [Google Scholar] [CrossRef]
- Loy, A.; Arnold, R.; Tischler, P.; Rattei, T.; Wagner, M.; Horn, M. probeCheck—a central resource for evaluating oligonucleotide probe coverage and specificity. Environ. Microbiol. 2008, 10, 2894–2898. [Google Scholar] [CrossRef] [Green Version]
- Pruesse, E.; Quast, C.; Knittel, K.; Fuchs, B.M.; Ludwig, W.; Peplies, J.; Glöckner, F.O. SILVA: A comprehensive online resource for quality checked and aligned ribosomal RNA sequence data compatible with ARB. Nucleic Acids Res. 2007, 35, 7188–7196. [Google Scholar] [CrossRef] [Green Version]
- Amann, R.I.; Ludwig, W.; Schleifer, K.H. Phylogenetic identification and in situ detection of individual microbial cells without cultivation. Microbiol. Rev. 1995, 59, 143–169. [Google Scholar] [CrossRef] [PubMed]
- Woese, C.R. Bacterial evolution. Microbiol. Rev. 1987, 51, 221–271. [Google Scholar] [CrossRef]
- Amann, R.I.; Krumholz, L.; Stahl, D.A. Fluorescent-oligonucleotide probing of whole cells for determinative, phylogenetic, and environmental studies in microbiology. J. Bacteriol. 1990, 172, 762–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frickmann, H.; Loderstaedt, U.; Racz, P.; Tenner-Racz, K.; Eggert, P.; Haeupler, A.; Bialek, R.; Hagen, R.M. Detection of tropical fungi in formalin-fixed, paraffin-embedded tissue: Still an indication for microscopy in times of sequence-based diagnosis? Biomed. Res. Int. 2015, 2015, 938721. [Google Scholar] [CrossRef] [Green Version]
- Frickmann, H.; Tenner-Racz, K.; Eggert, P.; Schwarz, N.G.; Poppert, S.; Tannich, E.; Hagen, R.M. Influence of parasite density and sample storage time on the reliability of Entamoeba histolytica-specific PCR from formalin-fixed and paraffin-embedded tissues. Diagn. Mol. Pathol. 2013, 22, 236–244. [Google Scholar] [CrossRef]
- Frickmann, H.; Künne, C.; Hagen, R.M.; Podbielski, A.; Normann, J.; Poppert, S.; Looso, M.; Kreikemeyer, B. Next-generation sequencing for hypothesis-free genomic detection of invasive tropical infections in poly-microbially contaminated, formalin-fixed, paraffin-embedded tissue samples—A proof-of-principle assessment. BMC Microbiol. 2019, 19, 75. [Google Scholar] [CrossRef]
- McGavin, M.D. Factors affecting visibility of a target tissue in histologic sections. Vet. Pathol. 2014, 51, 9–27. [Google Scholar] [CrossRef] [Green Version]
- Amin, M.B.; Mezger, E.; Zarbo, R.J. Detection of Pneumocystis carinii: Comparative study of monoclonal antibody and silver staining. Am. J. Clin. Pathol. 1992, 98, 13–18. [Google Scholar] [CrossRef]
- Arastéh, K.N.; Simon, V.; Musch, R.; Weiss, R.O.; Przytarski, K.; Futh, U.M.; Pleuger, F.; Huhn, D.; L’age, M.P. Sensitivity and specificity of indirect immunofluorescence and Grocott-technique in comparison with immunocytology (alkaline phosphatase anti alkaline phosphatase = APAAP) for the diagnosis of Pneumocystis carinii in broncho-alveolar lavage (BAL). Eur. J. Med. Res. 1998, 3, 559–563. [Google Scholar] [PubMed]
- Chantziantoniou, N. Differentiating Pneumocystis cysts from Candida sp. yeasts in pulmonary specimens using methenamine silver. Ann. Saudi Med. 1996, 16, 274–279. [Google Scholar] [CrossRef]
- Homer, K.S.; Wiley, E.L.; Smith, A.L.; McCollough, L.; Clark, D.; Nightingale, S.D.; Vuitch, F. Monoclonal antibody to Pneumocystis carinii. Comparison with silver stain in bronchial lavage specimens. Am. J. Clin. Pathol. 1992, 97, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Musto, L.; Flanigan, M.; Elbadawi, A. Ten-minute silver stain for Pneumocystis carinii and fungi in tissue sections. Arch. Pathol. Lab. Med. 1982, 106, 292–294. [Google Scholar] [PubMed]
- Naimey, G.L.; Wuerker, R.B. Comparison of histologic stains in the diagnosis of Pneumocystis carinii. Acta Cytol. 1995, 39, 1124–1127. [Google Scholar]
- Naryshkin, S.; Daniels, J.; Freno, E.; Cunningham, L. Cytology of treated and minimal Pneumocystis carinii pneumonia and a pitfall of the Grocott methenamine silver stain. Diagn. Cytopathol. 1991, 7, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, P.B.; Goyot, P.; Mojon, M. The microscopic diagnosis of Pneumocystis carinii. An evaluation of the gram, the methylene blue, and the Ziehl-Neelsen procedures. Acta Pathol. Microbiol. Immunol. Scand. B. 1986, 94, 19–23. [Google Scholar] [PubMed]
- Roden, A.C.; Schuetz, A.N. Histopathology of fungal diseases of the lung. Semin. Diagn. Pathol. 2017, 34, 530–549. [Google Scholar] [CrossRef] [PubMed]
- Binanti, D.; Mostegl, M.M.; Weissenbacher-Lang, C.; Nedorost, N.; Weissenböck, H. Detection of Pneumocystis infections by in situ hybridization in lung samples of Austrian pigs with interstitial pneumonia. Med. Mycol. 2014, 52, 196–201. [Google Scholar]
- Hahn, A.; Podbielski, A.; Meyer, T.; Zautner, A.E.; Loderstädt, U.; Schwarz, N.G.; Krüger, A.; Cadar, D.; Frickmann, H. On detection thresholds-a review on diagnostic approaches in the infectious disease laboratory and the interpretation of their results. Acta Trop. 2020, 205, 105377. [Google Scholar] [CrossRef]
- Nakashima, K.; Aoshima, M.; Ohkuni, Y.; Hoshino, E.; Hashimoto, K.; Otsuka, Y. Loop-mediated isothermal amplification method for diagnosing Pneumocystis pneumonia in HIV-uninfected immunocompromised patients with pulmonary infiltrates. J. Infect. Chemother. 2014, 20, 757–761. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Yu, Y.; Lv, J.; Yang, S.; Wu, J.; Chen, J.; Peng, W. Application of Metagenomic Next-Generation Sequencing to Diagnose Pneumocystis jirovecii Pneumonia in Kidney Transplantation Recipients. Ann. Transplant. 2021, 26, e931059. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, J.; Bragada, C.; Costa-De-Oliveira, S.; Ricardo, E.; Rodrigues, A.G.; Pina-Vaz, C. A new method for the detection of Pneumocystis jirovecii using flow cytometry. Eur. J. Clin. Microbiol. Infect. Dis. 2010, 29, 1147–1152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietrich, D.; Uhl, B.; Sailer, V.; Holmes, E.E.; Jung, M.; Meller, S.; Kristiansen, G. Improved PCR Performance Using Template DNA from Formalin-Fixed and Paraffin-Embedded Tissues by Overcoming PCR Inhibition. PLoS ONE 2013, 8, e77771. [Google Scholar] [CrossRef] [PubMed]
- Huijsmans, C.J.; Damen, J.; van der Linden, J.C.; Savelkoul, P.H.; Hermans, M.H. Comparative analysis of four methods to extract DNA from paraffin-embedded tissues: Effect on downstream molecular applications. BMC Res. Notes 2010, 3, 239. [Google Scholar] [CrossRef] [Green Version]
- Obersteller, S.; Neubauer, H.; Hagen, R.M.; Frickmann, H. Comparison of Five Commercial Nucleic Acid Extraction Kits for the PCR-based Detection of Burkholderia pseudomallei DNA in Formalin-Fixed, Paraffin-Embedded Tissues. Eur. J. Microbiol. Immunol. 2016, 6, 244–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rickerts, V. Identification of fungal pathogens in Formalin-fixed, Paraffin-embedded tissue samples by molecular methods. Fungal. Biol. 2016, 120, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.O.; Huibers, M.M.H.; de Weger, R.A.; de Leng, W.W.J.; Hinrichs, J.W.J.; Meijers, R.W.J.; Willems, S.M.; Peeters, T.L.M.G. One-fits-all pretreatment protocol facilitating Fluorescence In Situ Hybridization on formalin-fixed paraffin-embedded, fresh frozen and cytological slides. Mol. Cytogenet. 2019, 12, 27. [Google Scholar] [CrossRef]
- Makarovsky, I.; Markel, G.; Hoffman, A.; Schein, O.; Finkelstien, A.; Brosh-Nissimov, T.; Tashma, Z.; Dushnitsky, T.; Eisenkraft, A. Osmium tetroxide: A new kind of weapon. Isr. Med. Assoc. J. 2007, 9, 750–752. [Google Scholar] [PubMed]
- Gescher, D.M.; Kovacevic, D.; Schmiedel, D.; Siemoneit, S.; Mallmann, C.; Halle, E.; Göbel, U.B.; Moter, A. Fluorescence in situ hybridisation (FISH) accelerates identification of Gram-positive cocci in positive blood cultures. Int. J. Antimicrob. Agents 2008, 32 (Suppl. S1), S51–S59. [Google Scholar] [CrossRef] [PubMed]
- Hogardt, M.; Trebesius, K.; Geiger, A.M.; Hornef, M.; Rosenecker, J.; Heesemann, J. Specific and rapid detection by fluorescent in situ hybridization of bacteria in clinical samples obtained from cystic fibrosis patients. J. Clin. Microbiol. 2000, 38, 818–825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Özkoç, S.; Köker, M.; Önder, M.; Delibaş, S.B. Prevalence of Pneumocystis jirovecii colonization in autopsy cases in Turkey. J. Med. Microbiol. 2016, 65, 1152–1157. [Google Scholar] [CrossRef]
- Ponce, C.A.; Gallo, M.; Bustamante, R.; Vargas, S.L. Pneumocystis colonization is highly prevalent in the autopsied lungs of the general population. Clin. Infect. Dis. 2010, 50, 347–353. [Google Scholar] [CrossRef] [Green Version]
- Vargas, S.L.; Ponce, C.; Bustamante, R.; Calderón, E.; Nevez, G.; De Armas, Y.; Matos, O.; Miller, R.F.; Gallo, M.J. Importance of tissue sampling, laboratory methods, and patient characteristics for detection of Pneumocystis in autopsied lungs of non-immunosuppressed individuals. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 1711–1716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansour, N.J.; DeVita, V.T.; Goodell, B.W. Pneumocystis carinii Pneumonia. Ann. Intern. Med. 1970, 73, 342–343. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Grocott’s Staining | ||||
|---|---|---|---|---|
| Positive | Negative | |||
| FISH | Positive | 13 | 10 | 23 |
| Negative | 0 | 7 | 7 | |
| 13 | 17 | 30 | ||
| Concordance | 66.7% | |||
| Sensitivity | 100% | |||
| Specificity | 41% | |||
| In-House Real-Time PCR | ||||
|---|---|---|---|---|
| Positive | Negative | |||
| FISH | Positive | 10 | 0 | 10 |
| Negative | 2 | 18 | 20 | |
| 12 | 18 | 30 | ||
| Concordance | 93.3% | |||
| Sensitivity | 83.3% | |||
| Specificity | 100% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Sousa, D.R.T.; da Silva Neto, J.R.; da Silva, R.M., Jr.; Cruz, K.S.; Poppert, S.; Frickmann, H.; Souza, J.V.B. Identification of Pneumocystis jirovecii with Fluorescence In-Situ Hybridization (FISH) in Patient Samples—A Proof-of-Principle. J. Fungi 2022, 8, 13. https://doi.org/10.3390/jof8010013
de Sousa DRT, da Silva Neto JR, da Silva RM Jr., Cruz KS, Poppert S, Frickmann H, Souza JVB. Identification of Pneumocystis jirovecii with Fluorescence In-Situ Hybridization (FISH) in Patient Samples—A Proof-of-Principle. Journal of Fungi. 2022; 8(1):13. https://doi.org/10.3390/jof8010013
Chicago/Turabian Stylede Sousa, Débora Raysa Teixeira, João Ricardo da Silva Neto, Roberto Moreira da Silva, Jr., Kátia Santana Cruz, Sven Poppert, Hagen Frickmann, and João Vicente Braga Souza. 2022. "Identification of Pneumocystis jirovecii with Fluorescence In-Situ Hybridization (FISH) in Patient Samples—A Proof-of-Principle" Journal of Fungi 8, no. 1: 13. https://doi.org/10.3390/jof8010013