
Invasive Fungal Rhinosinusitis with and without Orbital Complications: Clinical and Laboratory Differences

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Statistical Analysis
3. Results
3.1. Demographic Data, Lab Data, and Symptoms
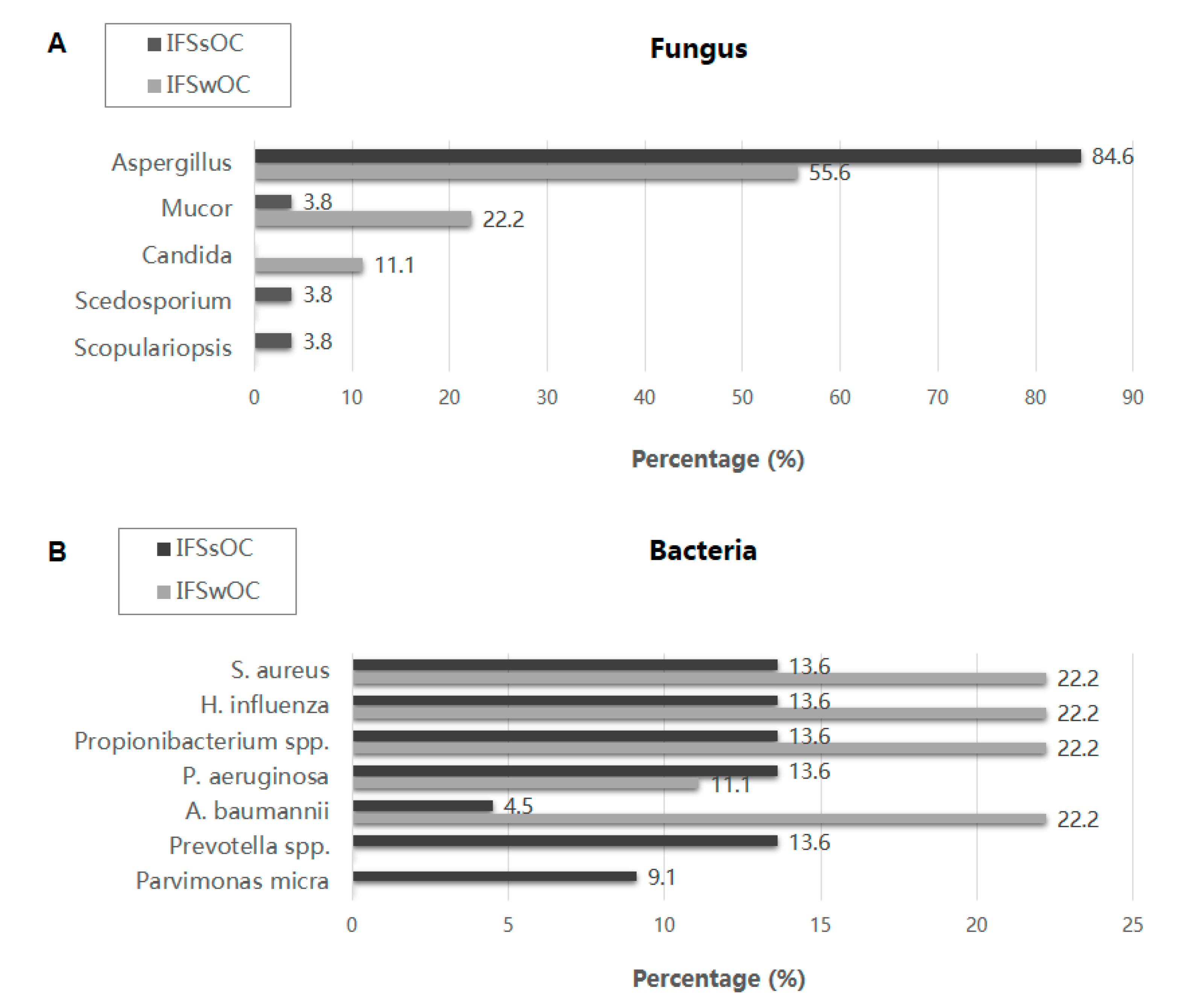
3.2. Microbiology
3.3. Treatment and Outcome
3.4. Clinical Signs Associated with IFSwOC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- DeShazo, R.D.; O’Brien, M.; Chapin, K.; Soto-Aguilar, M.; Gardner, L.; Swain, R. A new classification and diagnostic criteria for invasive fungal sinusitis. Arch. Otolaryngol. Head Neck Surg. 1997, 123, 1181–1188. [Google Scholar] [CrossRef]
- Turner, J.H.; Soudry, E.; Nayak, J.V.; Hwang, P.H. Survival outcomes in acute invasive fungal sinusitis: A systematic review and quantitative synthesis of published evidence. Laryngoscope 2013, 123, 1112–1118. [Google Scholar] [CrossRef] [PubMed]
- Waitzman, A.A.; Birt, B.D. Fungal sinusitis. J. Otolaryngol. 1994, 23, 244–249. [Google Scholar]
- Lueg, E.A.; Ballagh, R.H.; Forte, V. Analysis of the recent cluster of invasive fungal sinusitis at the Toronto Hospital for Sick Children. J. Otolaryngol. 1996, 25, 366–370. [Google Scholar] [PubMed]
- Gode, S.; Turhal, G.; Ozturk, K.; Aysel, A.; Midilli, R.; Karci, B. Acute Invasive Fungal Rhinosinusitis: Survival Analysis and the Prognostic Indicators. Am. J. Rhinol. Allergy 2015, 29, e164–e169. [Google Scholar] [CrossRef] [PubMed]
- Bhadada, S.; Bhansali, A.; Reddy, K.S.S.; Bhat, R.V.; Khandelwal, N.; Gupta, A.K. Rhino-orbital-cerebral mucormycosis in type 1 diabetes mellitus. Indian J. Pediatr. 2005, 72, 671–674. [Google Scholar] [CrossRef] [PubMed]
- Dhiwakar, M.; Thakar, A.; Bahadur, S. Improving outcomes in rhinocerebral mucormycosis—Early diagnostic pointers and prognostic factors. J. Laryngol. Otol. 2003, 117, 861–865. [Google Scholar] [CrossRef]
- Monroe, M.M.; McLean, M.; Sautter, N.; Wax, M.K.; Andersen, P.E.; Smith, T.L.; Gross, N.D. Invasive Fungal Rhinosinusitis. Laryngoscope 2013, 123, 1583–1587. [Google Scholar] [CrossRef]
- Sun, H.-Y.; Forrest, G.; Gupta, K.L.; Aguado, J.M.; Lortholary, O.; Julia, M.B.; Safdar, N.; Patel, R.; Kusne, S.; Singh, N. Rhino-Orbital-Cerebral Zygomycosis in Solid Organ Transplant Recipients. Transplantation 2010, 90, 85–92. [Google Scholar] [CrossRef] [Green Version]
- Hargrove, R.N.; Wesley, R.E.; Klippenstein, K.A.; Fleming, J.C.; Haik, B.G. Indications for Orbital Exenteration in Mucormycosis. Ophthalmic Plast. Reconstr. Surg. 2006, 22, 286–291. [Google Scholar] [CrossRef]
- Cho, H.-J.; Jang, M.-S.; Hong, S.D.; Chung, S.-K.; Kim, H.Y.; Dhong, H.-J. Prognostic Factors for Survival in Patients with Acute Invasive Fungal Rhinosinusitis. Am. J. Rhinol. Allergy 2015, 29, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Thurtell, M.J.; Chiu, A.L.S.; Goold, L.A.; Akdal, G.; Crompton, J.L.; Ahmed, R.; Madge, S.N.; Selva, D.; Francis, I.; Ghabrial, R.; et al. Neuro-ophthalmology of invasive fungal sinusitis: 14 consecutive patients and a review of the literature. Clin. Exp. Ophthalmol. 2013, 41, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, S.M.S.; Borghei, P. Rhinocerebral mucormycosis: Pathways of spread. Eur. Arch. Oto-Rhino-Laryngology 2005, 262, 932–938. [Google Scholar] [CrossRef]
- Galetta, S.L.; Wulc, A.E.; Goldberg, H.I.; Nichols, C.W.; Glaser, J.S. Rhinocerebral mucormycosis: Management and survival after carotid occlusion. Ann. Neurol. 1990, 28, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Breadmore, R.; Desmond, P.; Opeskin, K. Intracranial aspergillosis producing cavernous sinus syndrome and rupture of internal carotid artery. Australas. Radiol. 1994, 38, 72–75. [Google Scholar] [CrossRef]
- Hurst, R.W.; Judkins, A.; Bolger, W.; Chu, A.; Loevner, L.A. Mycotic Aneurysm and Cerebral Infarction Resulting from Fungal Sinusitis: Imaging and Pathologic Correlation. Am. J. Neuroradiol. 2001, 22, 858–863. [Google Scholar] [PubMed]
- Parikh, S.L.; Venkatraman, G.; DelGaudio, J.M. Invasive Fungal Sinusitis: A 15-Year Review from a Single Institution. Am. J. Rhinol. 2004, 18, 75–81. [Google Scholar] [CrossRef]
- Chandrasekharan, R.; Thomas, M.; Rupa, V. Comparative study of orbital involvement in invasive and non-invasive fungal sinusitis. J. Laryngol. Otol. 2011, 126, 152–158. [Google Scholar] [CrossRef]
- Trief, D.; Gray, S.T.; Jakobiec, F.A.; Durand, M.L.; Fay, A.; Freitag, S.K.; Lee, N.; Lefebvre, D.; Holbrook, E.; Bleier, B.; et al. Invasive fungal disease of the sinus and orbit: A comparison between mucormycosis and Aspergillus. Br. J. Ophthalmol. 2015, 100, 184–188. [Google Scholar] [CrossRef]
- Drakos, P.E.; Nagler, A.; Or, R.; Naparstek, E.; Kapelushnik, J.; Engelhard, D.; Rahav, G.; Ne’Emean, D.; Slavin, S. Invasive fungal sinusitis in patients undergoing bone marrow transplantation. Bone Marrow Transplant. 1993, 12, 203–208. [Google Scholar] [PubMed]
- Deutsch, P.G.; Whittaker, J.; Prasad, S. Invasive and Non-Invasive Fungal Rhinosinusitis—A Review and Update of the Evidence. Medicina 2019, 55, 319. [Google Scholar] [CrossRef] [Green Version]
- Stringer, S.P.; Ryan, M.W. Chronic invasive fungal rhinosinusitis. Otolaryngol. Clin. N. Am. 2000, 33, 375–387. [Google Scholar] [CrossRef]
- Garcia-Giraldo, A.M.; Mora, B.L.; Loaiza-Castaño, J.M.; Cedano, J.A.; Rosso, F. Invasive fungal infection by Aspergillus flavus in immunocompetent hosts: A case series and literature review. Med. Mycol. Case Rep. 2019, 23, 12–15. [Google Scholar] [CrossRef]
- Poddighe, D.; Vangelista, L. Staphylococcus aureus Infection and Persistence in Chronic Rhinosinusitis: Focus on Leukocidin ED. Toxins 2020, 12, 678. [Google Scholar] [CrossRef]
- Duell, B.L.; Su, Y.-C.; Riesbeck, K. Host-pathogen interactions of nontypeableHaemophilus influenzae: From commensal to pathogen. FEBS Lett. 2016, 590, 3840–3853. [Google Scholar] [CrossRef]
- Lu, Y.-T.; Wang, S.-H.; Liou, M.-L.; Shen, T.-A.; Lu, Y.-C.; Hsin, C.-H.; Yang, S.-F.; Chen, Y.-Y.; Chang, T.-H. Microbiota Dysbiosis in Fungal Rhinosinusitis. J. Clin. Med. 2019, 8, 1973. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.C.; Bassiouni, A.; Tanjararak, K.; Vreugde, S.; Psaltis, A.J.; Wormald, P.-J. Role of fungi in chronic rhinosinusitis through ITS sequencing. Laryngoscope 2018, 128, 16–22. [Google Scholar] [CrossRef]
- Zhang, I.; Pletcher, S.; Goldberg, A.N.; Barker, B.; Cope, E.K. Fungal Microbiota in Chronic Airway Inflammatory Disease and Emerging Relationships with the Host Immune Response. Front. Microbiol. 2017, 8, 2477. [Google Scholar] [CrossRef] [Green Version]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology 2020, 58, 1–464. [Google Scholar] [CrossRef] [PubMed]
- Herbrecht, R.; Denning, D.; Patterson, T.F.; Bennett, J.E.; Greene, R.E.; Oestmann, J.-W.; Kern, W.V.; Marr, K.A.; Ribaud, P.; Lortholary, O.; et al. Voriconazole versus Amphotericin B for Primary Therapy of Invasive Aspergillosis. N. Engl. J. Med. 2002, 347, 408–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maertens, J.A.; Raad, I.I.; Marr, K.A.; Patterson, T.; Kontoyiannis, D.P.; Cornely, O.; Bow, E.J.; Rahav, G.; Neofytos, D.; Aoun, M.; et al. Isavuconazole versus voriconazole for primary treatment of invasive mould disease caused by Aspergillus and other filamentous fungi (SECURE): A phase 3, randomised-controlled, non-inferiority trial. Lancet 2016, 387, 760–769. [Google Scholar] [CrossRef]
- Fadda, G.L.; Martino, F.; Andreani, G.; Succo, G.; Catalani, M.; Di Girolamo, S.; Cavallo, G. Definition and management of invasive fungal rhinosinusitis: A single-centre retrospective study. Acta Otorhinolaryngol. Ital. 2021, 41, 43–50. [Google Scholar] [CrossRef]
- Andreani, G.; Fadda, G.; Gned, D.; Dragani, M.; Cavallo, G.; Monticone, V.; Morotti, A.; De Gobbi, M.; Guerrasio, A.; D’Avolio, A.; et al. Rhino-Orbital-Cerebral Mucormycosis after Allogeneic Hematopoietic Stem Cell Transplantation and Isavuconazole Therapeutic Drug Monitoring during Intestinal Graft versus Host Disease. Mediterr. J. Hematol. Infect. Dis. 2019, 11, e2019061. [Google Scholar] [CrossRef]
- Khor, B.-S.; Lee, M.-H.; Leu, H.-S.; Liu, J.-W. Rhinocerebral mucormycosis in Taiwan. J. Microbiol. Immunol. Infect. 2003, 36, 266–269. [Google Scholar] [PubMed]
- Chen, C.-Y.; Sheng, W.-H.; Cheng, A.; Chen, Y.-C.; Tsay, W.; Tang, J.-L.; Huang, S.-Y.; Chang, S.-C.; Tien, H.-F. Invasive fungal sinusitis in patients with hematological malignancy: 15 years experience in a single university hospital in Taiwan. BMC Infect. Dis. 2011, 11, 250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasapoglu, F.; Coskun, H.; Ozmen, O.A.; Akalin, H.; Ener, B. Acute invasive fungal rhinosinusitis: Evaluation of 26 patients treated with endonasal or open surgical procedures. Otolaryngol. Neck Surg. 2010, 143, 614–620. [Google Scholar] [CrossRef] [PubMed]
- Payne, S.J.; Mitzner, R.; Kunchala, S.; Roland, L.; McGinn, J. Acute Invasive Fungal Rhinosinusitis. Otolaryngol. Neck Surg. 2016, 154, 759–764. [Google Scholar] [CrossRef]
- Roxbury, C.R.; Smith, D.F.; Higgins, T.S.; Lee, S.E.; Gallia, G.L.; Ishii, M.; Lane, A.P.; Reh, D.D. Complete Surgical Resection and Short-Term Survival in Acute Invasive Fungal Rhinosinusitis. Am. J. Rhinol. Allergy 2017, 31, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Wandell, G.; Miller, C.; Rathor, A.; Wai, T.H.; Guyer, R.A.; Schmidt, R.A.; Turner, J.; Hwang, P.H.; Davis, G.E.; Humphreys, I.M. A multi-institutional review of outcomes in biopsy-proven acute invasive fungal sinusitis. Int. Forum Allergy Rhinol. 2018, 8, 1459–1468. [Google Scholar] [CrossRef]
- Hirabayashi, K.E.; Idowu, O.; Kalin-Hajdu, E.; Oldenburg, C.E.; Brodie, F.L.; Kersten, R.C.; Vagefi, M.R. Invasive Fungal Sinusitis: Risk Factors for Visual Acuity Outcomes and Mortality. Ophthalmic Plast. Reconstr. Surg. 2019, 35, 535–542. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2019, 71, 1367–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hua, M.-W.; Wu, C.-Y.; Jiang, R.-S.; Chang, C.-Y.; Liang, K.-L. Validate the classification of fungal rhinosinusitis: A retrospective analysis of 162 patients at a single institution. Clin. Otolaryngol. 2019, 44, 1131–1137. [Google Scholar] [CrossRef] [PubMed]
- Kosmidis, C.; Denning, D. The clinical spectrum of pulmonary aspergillosis. Thorax 2014, 70, 270–277. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 38) No. (%) | IFSsOC (n = 29) No. (%) | IFSwOC (n = 9) No. (%) | p Value | |
|---|---|---|---|---|
| Age (mean ± SD) | 61.18 ± 12.30 | 60.03 ± 12.10 | 64.89 ± 12.96 | 0.308 |
| Gender (male: female) | 14:24 | 11:18 | 3:6 | 1.000 |
| Classification | <0.001 | |||
| Acute invasive | 6 (15.8) | 0 (0.0) | 6 (66.7) | |
| Chronic invasive | 32 (84.2) | 29 (100.0) | 3 (33.3) | |
| Side | ||||
| Left | 22 (57.9) | 17 (58.6) | 5 (55.6) | 1.000 |
| Right | 18 (47.4) | 12 (41.4) | 6 (66.7) | 0.260 |
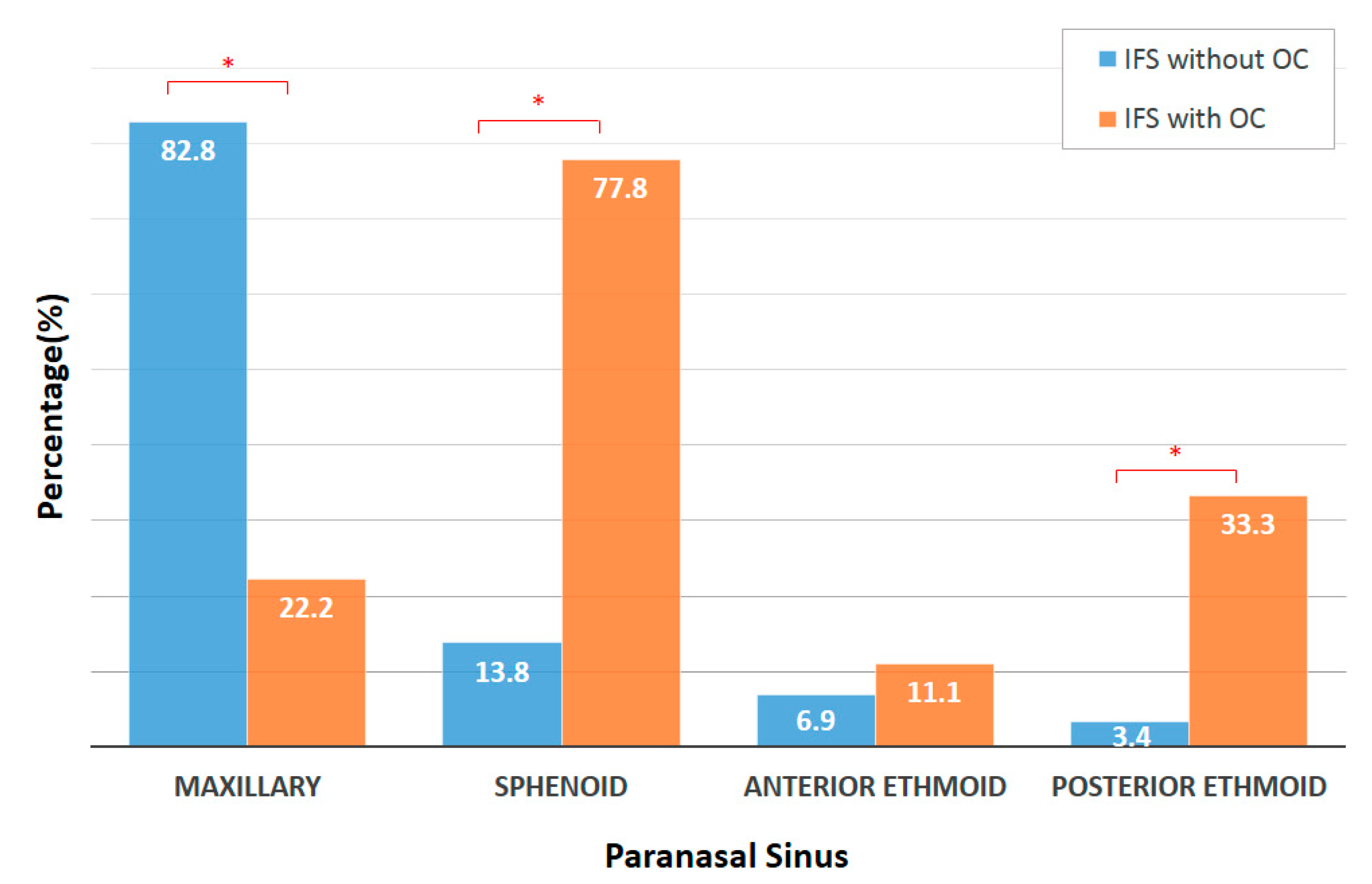
| Location | ||||
| Maxillary | 26 (68.4) | 24 (82.8) | 2 (22.2) | 0.002 |
| Sphenoid | 11 (28.9) | 4 (13.8) | 7 (77.8) | 0.001 |
| Anterior ethmoid | 3 (7.9) | 2 (6.9) | 1 (11.1) | 1.000 |
| Posterior ethmoid | 4 (10.5) | 1 (3.4) | 3 (33.3) | 0.035 |
| Others * | 2 (5.3) | 2 (6.9) | 0 (0.0) | 1.000 |
| Underlying Diseases | ||||
| Hypertension | 11 (28.9) | 6 (20.7) | 5 (55.6) | 0.088 |
| Diabetes mellitus | 7 (18.4) | 4 (13.8) | 3 (33.3) | 0.322 |
| Coronary artery disease | 5 (13.2) | 3 (10.3) | 2 (22.2) | 0.574 |
| Chronic kidney disease | 1 (2.6) | 1 (3.4) | 0 (0.0) | 1.000 |
| Hyperlipidemia | 5 (13.2) | 4 (13.8) | 1 (11.1) | 1.000 |
| Atrial fibrillation | 2 (5.3) | 1 (3.4) | 1 (11.1) | 0.422 |
| Autoimmune disease | 2 (5.3) | 2 (6.9) | 0 (0.0) | 1.000 |
| Lab Data | ||||
| WBC (/μL) | 8252.63 ± 5850.74 | 6686.21 ± 1796.97 | 13,300.00 ± 10,462.43 | 0.066 |
| ANC (/μL) | 5623.95 ± 5660.50 | 4194.62 ± 1619.37 | 10,229.56 ± 10,379.96 | 0.103 |
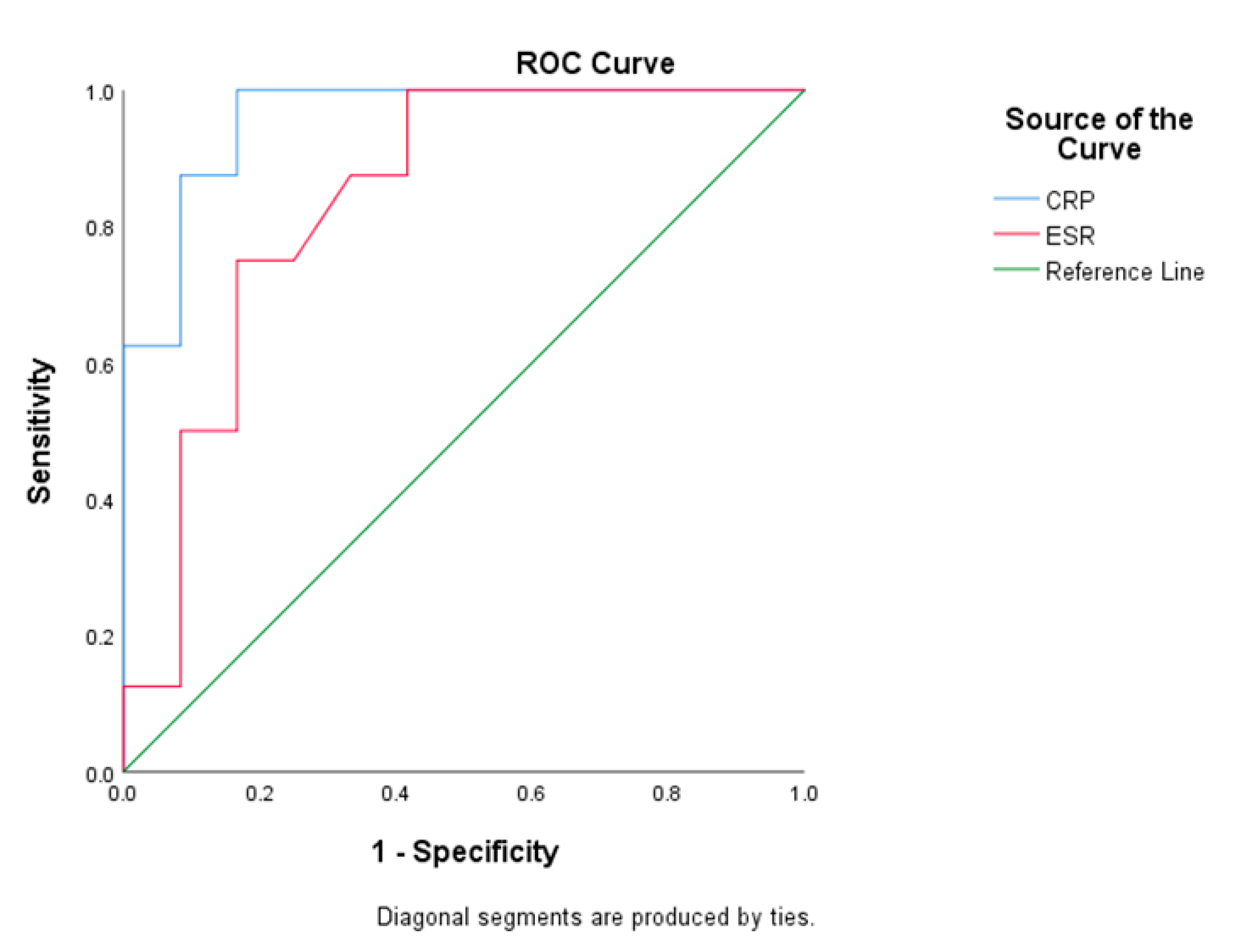
| CRP (mg/dL) | 4.50 ± 8.17 | 0.53 ± 0.92 | 9.79 ± 10.52 | <0.001 |
| ESR (mm/h) | 42.35 ± 32.37 | 28.67 ± 23.34 | 62.88 ± 34.44 | 0.031 |
| Symptoms Duration (days, mean ± SD) | 236.22 ± 631.58 | 297.52 ± 736.53 | 79.56 ± 124.36 | 0.389 |
| Purulent rhinorrhea | 14 (36.8) | 14 (48.3) | 0 (0.0) | 0.014 |
| Headache | 12 (31.6) | 5 (17.2) | 7 (77.8) | 0.002 |
| Nasal obstruction | 8 (21.1) | 8 (27.6) | 0 (0.0) | 0.159 |
| Diplopia | 6 (15.8) | 0 (0.0) | 6 (66.7) | <0.001 |
| Fever | 5 (13.2) | 0 (0.0) | 5 (55.6) | <0.001 |
| Foul odor | 5 (13.2) | 5 (17.2) | 0 (0.0) | 0.312 |
| Blood-tinged rhinorrhea | 4 (10.5) | 4 (13.8) | 0 (0.0) | 0.554 |
| Facial pain/fullness | 4 (10.5) | 4 (13.8) | 0 (0.0) | 0.554 |
| Blurred vision | 3 (7.9) | 0 (0.0) | 3 (33.3) | 0.010 |
| Proptosis | 2 (5.3) | 0 (0.0) | 2 (22.2) | 0.051 |
| Ptosis | 2 (5.3) | 0 (0.0) | 2 (22.2) | 0.051 |
| Facial numbness | 2 (5.3) | 2 (6.9) | 0 (0.0) | 1.000 |
| Facial swelling | 2 (5.3) | 1 (3.4) | 1 (11.1) | 0.422 |
| Consciousness disturbance | 1 (2.6) | 0 (0.0) | 1 (11.1) | 0.237 |
| Imaging Results | ||||
| Cavernous sinus or orbital involvement suspected on CT/MRI | 7 (18.4) | 0 (0.0) | 7 (77.8) | <0.001 |
| All Patients (n = 38) No. (%) | IFSsOC (n = 29) No. (%) | IFSwOC (n = 9) No. (%) | p Value | |
|---|---|---|---|---|
| Follow-up Duration (days) | 275.43 ± 262.01 | 286.76 ± 284.83 | 220.67 ± 90.26 | 0.983 |
| Surgery | ||||
| Interval between onset of symptoms and surgery (days) | 107.13 ± 99.19 | 145.14 ± 93.77 | 14.22 ± 11.38 | <0.001 |
| Antifungal Therapy | ||||
| Voriconazole | 24 (63.2) | 17 (58.6) | 7 (77.8) | 0.438 |
| Amphotericin B | 1 (2.6) | 0 (0.0) | 1 (11.1) | 0.237 |
| Liposomal amphotericin B | 2 (5.3) | 0 (0.0) | 2 (22.2) | 0.051 |
| Others * | 4 (10.5) | 2 (6.9) | 2 (22.2) | 0.233 |
| Duration (days) | 73.85 ± 67.86 | 70.11 ± 79.32 | 82.25 ± 32.41 | 0.140 |
| Antibiotic | ||||
| Duration (days) | 27.71 ± 39.76 | 22.95 ± 43.83 | 42.00 ± 19.82 | 0.005 |
| Sequelae | 2 (5.3) | 0 (0.0) | 2 (22.2) | 0.051 |
| Mortality | 1 (2.6) | 0 (0.0) | 1 (11.1) | 0.237 |
| Sequelae or Mortality | 3 (7.9) | 0 (0.0) | 3 (33.3) | 0.010 |
| Odds Ratio | 95% CI | p Value | |
|---|---|---|---|
| Location | |||
| Maxillary | 0.060 | 0.009–0.376 | 0.002 |
| Sphenoid | 21.875 | 3.295–145.237 | 0.001 |
| Posterior ethmoid | 14.000 | 1.234–158.844 | 0.035 |
| Symptoms | |||
| Headache | 16.800 | 2.659–106.135 | 0.002 |
| Fever | 8.25 * | <0.001 | |
| Lab Data | |||
| CRP (≥1.025 mg/dL) | 88.000 | 4.758–1627.704 | <0.001 |
| ESR (≥46.5 mm/h) | 15.000 | 1.652–136.172 | 0.019 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Twu, K.-H.; Kuo, Y.-J.; Ho, C.-Y.; Kuan, E.C.; Wang, W.-H.; Lan, M.-Y. Invasive Fungal Rhinosinusitis with and without Orbital Complications: Clinical and Laboratory Differences. J. Fungi 2021, 7, 573. https://doi.org/10.3390/jof7070573
Twu K-H, Kuo Y-J, Ho C-Y, Kuan EC, Wang W-H, Lan M-Y. Invasive Fungal Rhinosinusitis with and without Orbital Complications: Clinical and Laboratory Differences. Journal of Fungi. 2021; 7(7):573. https://doi.org/10.3390/jof7070573
Chicago/Turabian StyleTwu, Kuan-Hsiang, Ying-Ju Kuo, Ching-Yin Ho, Edward C. Kuan, Wei-Hsin Wang, and Ming-Ying Lan. 2021. "Invasive Fungal Rhinosinusitis with and without Orbital Complications: Clinical and Laboratory Differences" Journal of Fungi 7, no. 7: 573. https://doi.org/10.3390/jof7070573