
Clinical Characteristics Predicting Worse Long-Term Outcomes in Patients with Myocardial Infarction and Non-Obstructive Coronary Arteries (MINOCA)

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Demographic and Laboratory Data
2.2. Echocardiography
2.3. Angiography
2.4. Follow-Up
2.5. Statistical Methods
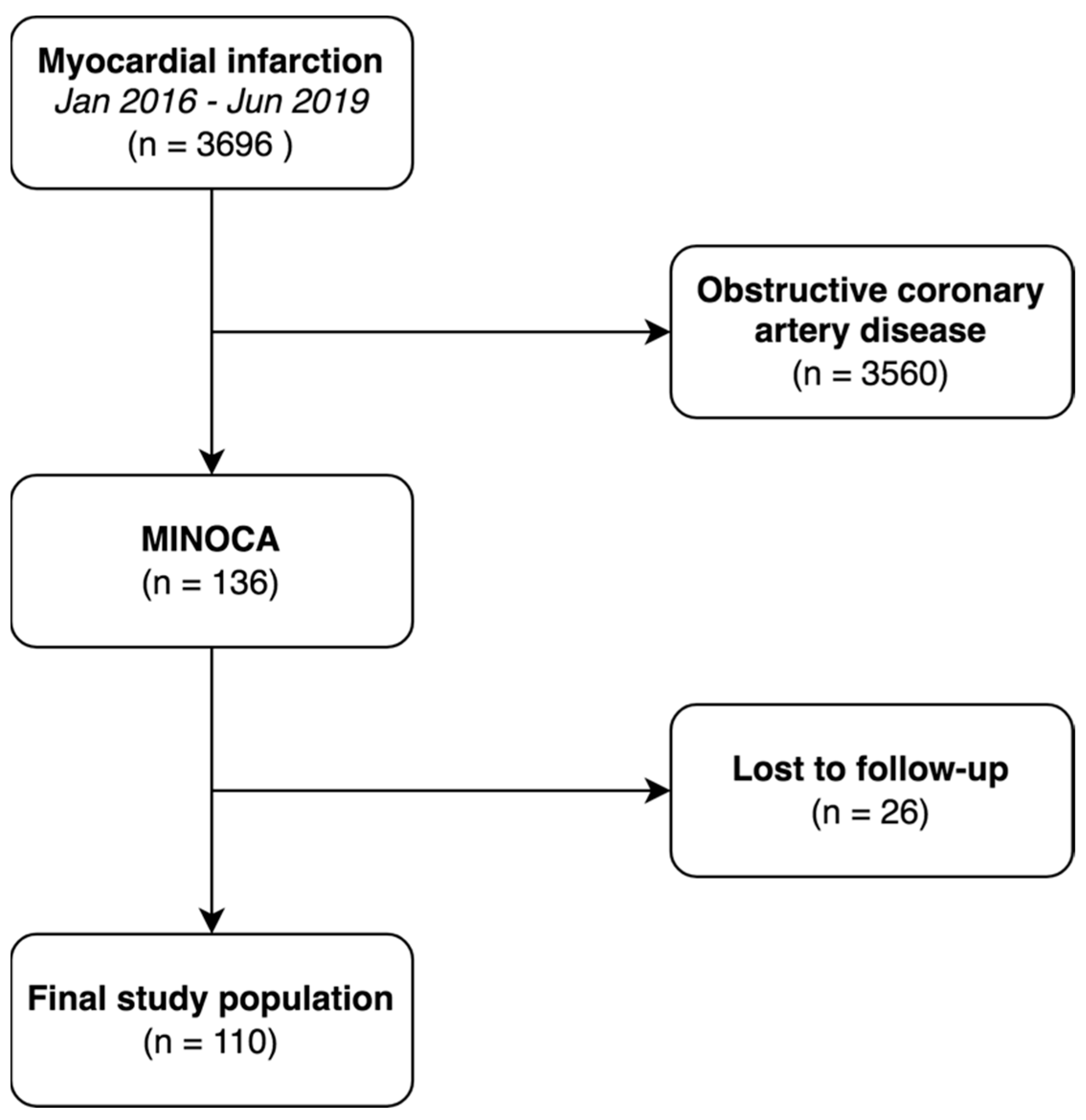
3. Results
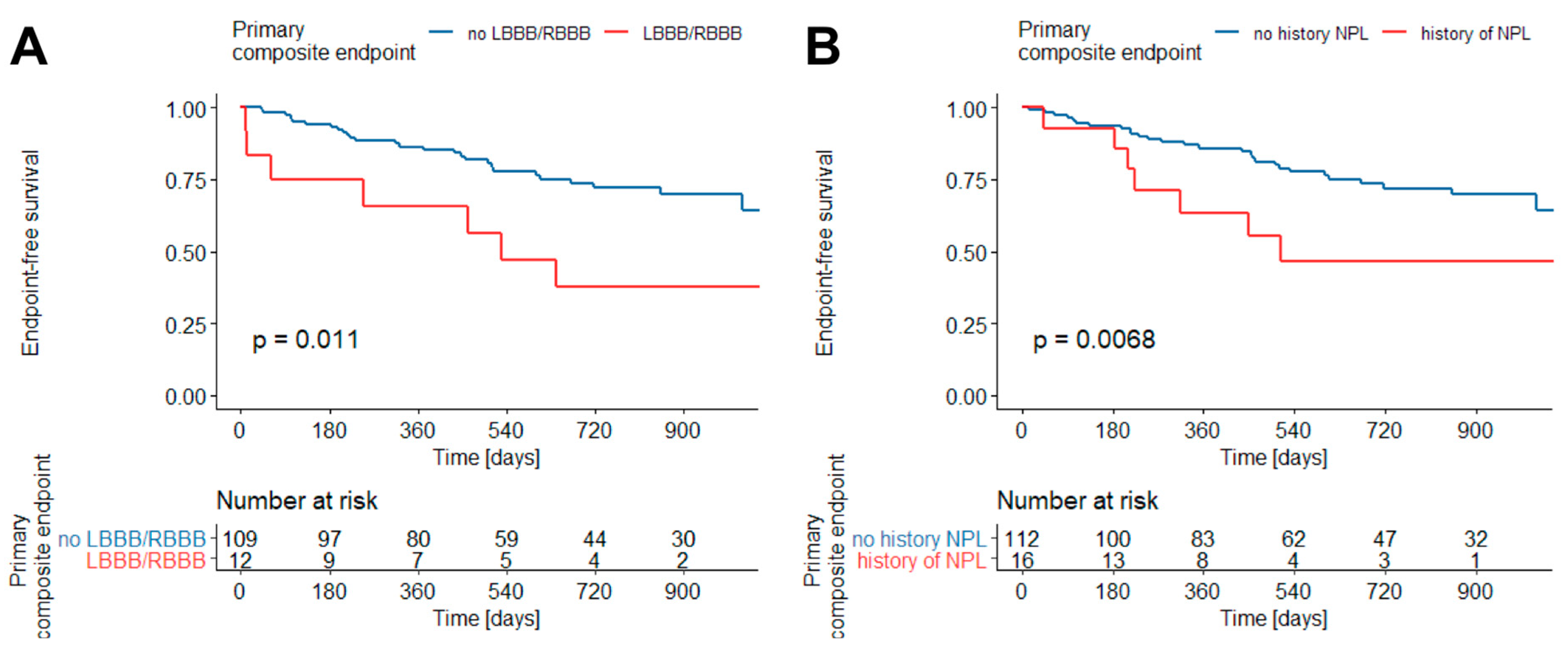
3.1. Kaplan–Meier Survival Estimator
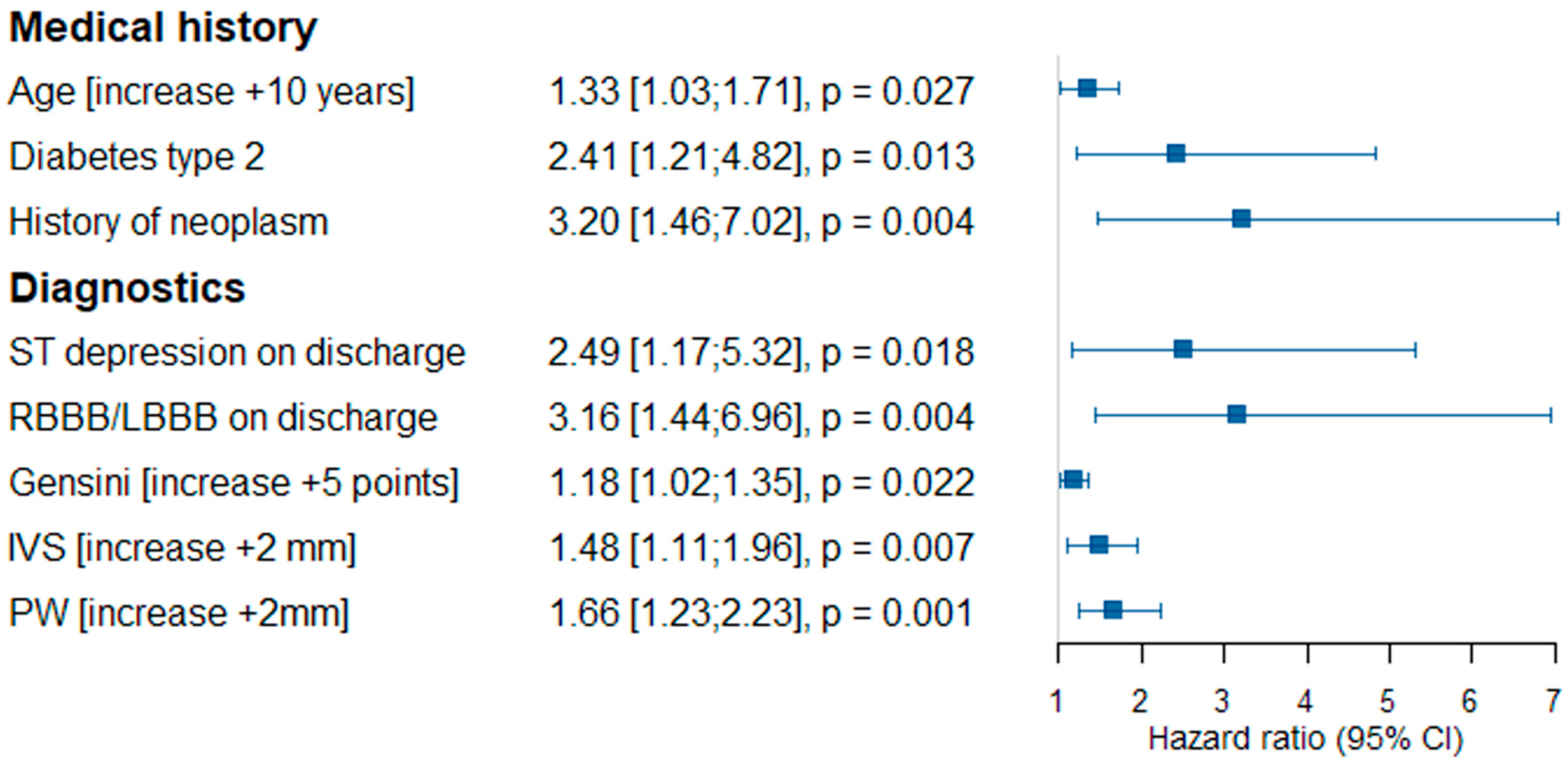
3.2. The Univariate Cox Proportional Hazards Model Analysis
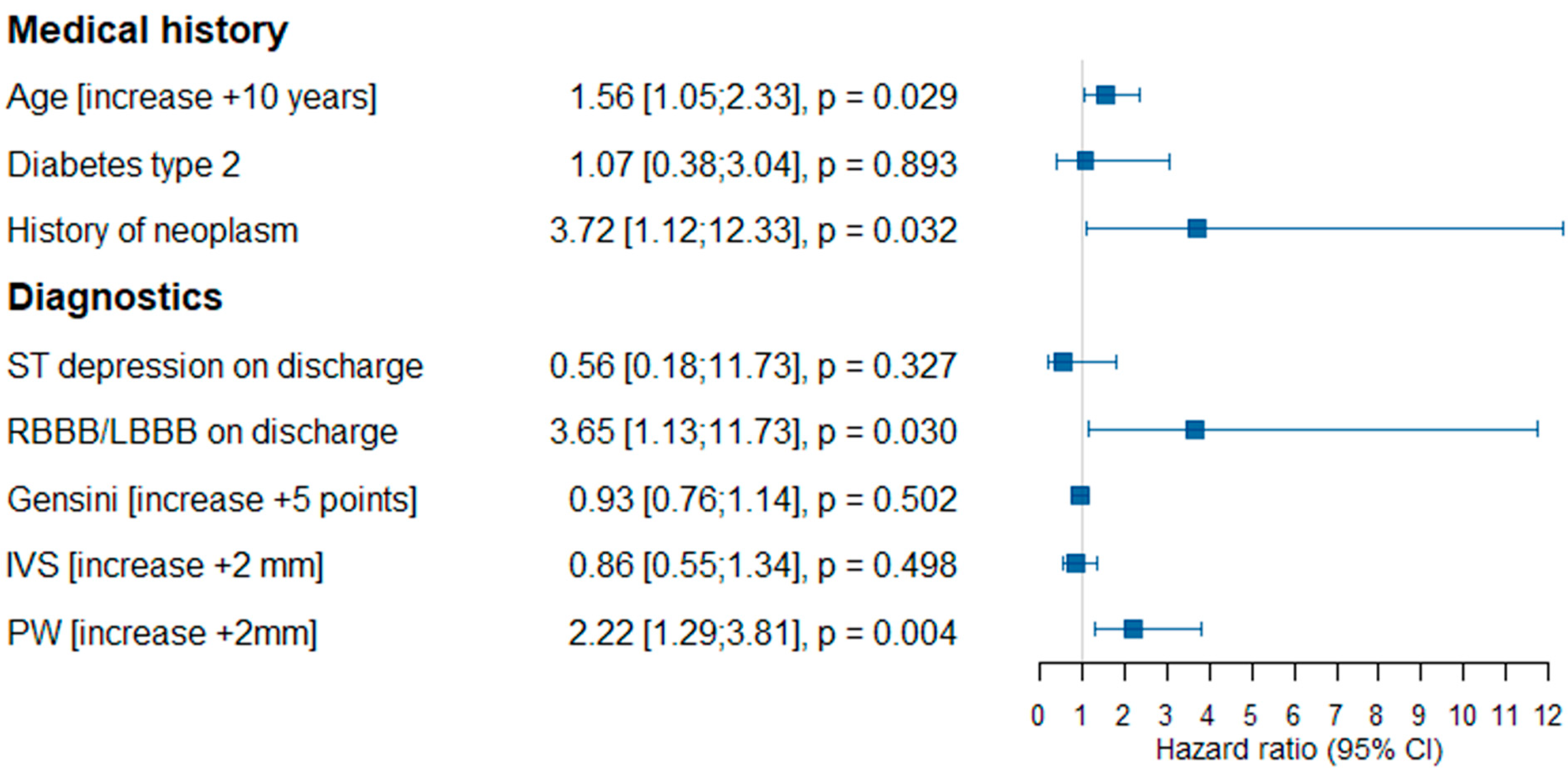
3.3. The Multivariate Cox Proportional Hazards Model
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pelliccia, F.; Marzilli, M.; Boden, W.E.; Camici, P.G. Why the Term MINOCA Does Not Provide Conceptual Clarity for Actionable Decision-Making in Patients with Myocardial Infarction with No Obstructive Coronary Artery Disease. J. Clin. Med. 2021, 10, 4630. [Google Scholar] [CrossRef] [PubMed]
- Tamis-Holland, J.E.; Jneid, H.; Reynolds, H.R.; Agewall, S.; Brilakis, E.S.; Brown, T.M.; Lerman, A.; Cushman, M.; Kumbhani, D.J.; Arslanian-Engoren, C.; et al. Contemporary Diagnosis and Management of Patients with Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: A Scientific Statement from the American Heart Association. Circulation 2019, 139, E891–E908. [Google Scholar] [CrossRef] [PubMed]
- Niccoli, G.; Camici, P.G. Myocardial infarction with non-obstructive coronary arteries: What is the prognosis? Eur. Heart. J. Suppl. 2020, 22, E40. [Google Scholar] [CrossRef] [PubMed]
- Dees, D.; Rahimi, F.; Amann, M.; Nührenberg, T.G.; Löffelhardt, N.; Schmitz, R.; Valina, C.M.; Neumann, F.-J.; Hochholzer, W. Prevalence and Causes of Myocardial Infarction with Non-Obstructive Coronary Arteries in a Contemporary Cohort of Patients with Suspected Myocardial Infarction. J. Clin. Med. 2021, 10, 5188. [Google Scholar] [CrossRef]
- Lindahl, B.; Baron, T.; Erlinge, D.; Hadziosmanovic, N.; Nordenskjöld, A.; Gard, A.; Jernberg, T. Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients with Myocardial Infarction with Nonobstructive Coronary Artery Disease. Circulation 2017, 135, 1481–1489. [Google Scholar] [CrossRef]
- Agewall, S.; Beltrame, J.F.; Reynolds, H.R.; Niessner, A.; Rosano, G.; Caforio, A.L.P.; De Caterina, R.; Zimarino, M.; Roffi, M.; Kjeldsen, K.; et al. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur. Heart J. 2016, 38, ehw149. [Google Scholar] [CrossRef]
- Bryniarski, K.; Gasior, P.; Legutko, J.; Makowicz, D.; Kedziora, A.; Szolc, P.; Bryniarski, L.; Kleczynski, P.; Jang, I.-K. OCT Findings in MINOCA. J. Clin. Med. 2021, 10, 2759. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth Universal Definition of Myocardial Infarction (2018). Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Victor, M.A.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed]
- Gensini, G.G. A more meaningful scoring system for determining the severity of coronary heart disease. Am. J. Cardiol. 1983, 51, 606. [Google Scholar] [CrossRef]
- Larsen, A.I.; Galbraith, P.D.; Ghali, W.A.; Norris, C.M.; Graham, M.M.; Knudtson, M.L. Characteristics and outcomes of patients with acute myocardial infarction and angiographically normal coronary arteries. Am. J. Cardiol. 2005, 95, 261–263. [Google Scholar] [CrossRef] [PubMed]
- Gehrie, E.R.; Reynolds, H.R.; Chen, A.Y.; Neelon, B.H.; Roe, M.T.; Gibler, W.B.; Ohman, E.M.; Newby, L.K.; Peterson, E.D.; Hochman, J.S. Characterization and outcomes of women and men with non-ST-segment elevation myocardial infarction and nonobstructive coronary artery disease: Results from the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines (CRUSADE) quality improvement initiative. Am. Heart J. 2009, 158, 688–694. [Google Scholar] [CrossRef]
- Rakowski, T.; De Luca, G.; Siudak, Z.; Plens, K.; Dziewierz, A.; Kleczyński, P.; Tokarek, T.; Węgiel, M.; Sadowski, M.; Dudek, D. Characteristics of patients presenting with myocardial infarction with non-obstructive coronary arteries (MINOCA) in Poland: Data from the ORPKI national registry. J. Thromb. Thrombolysis 2019, 47, 462. [Google Scholar] [CrossRef]
- Pasupathy, S.; Lindahl, B.; Litwin, P.; Tavella, R.; Williams, M.J.A.; Air, T.; Zeitz, C.; Smilowitz, N.R.; Reynolds, H.R.; Eggers, K.M.; et al. Survival in Patients with Suspected Myocardial Infarction with Nonobstructive Coronary Arteries: A Comprehensive Systematic Review and Meta-Analysis from the MINOCA Global Collaboration. Circ. Cardiovasc. Qual. Outcomes 2021, 14, e007880. [Google Scholar] [CrossRef]
- Safdar, B.; Spatz, E.S.; Dreyer, R.P.; Beltrame, J.F.; Lichtman, J.H.; Spertus, J.A.; Reynolds, H.R.; Geda, M.; Bueno, H.; Dziura, J.D.; et al. Presentation, clinical profile, and prognosis of young patients with myocardial infarction with nonobstructive coronary arteries (MINOCA): Results from the VIRGO study. J. Am. Heart Assoc. 2018, 7, e009174. [Google Scholar] [CrossRef]
- Kang, W.Y.; Jeong, M.H.; Ahn, Y.K.; Kim, J.H.; Chae, S.C.; Kim, Y.J.; Hur, S.H.; Seong, I.W.; Hong, T.J.; Choi, D.H.; et al. Are patients with angiographically near-normal coronary arteries who present as acute myocardial infarction actually safe? Int. J. Cardiol. 2011, 146, 207–212. [Google Scholar] [CrossRef]
- Dreyer, R.P.; Tavella, R.; Curtis, J.P.; Wang, Y.; Pauspathy, S.; Messenger, J.; Rumsfeld, J.S.; Maddox, T.M.; Krumholz, H.M.; Spertus, J.A.; et al. Myocardial infarction with non-obstructive coronary arteries as compared with myocardial infarction and obstructive coronary disease: Outcomes in a Medicare population. Eur. Heart J. 2020, 41, 870–878. [Google Scholar] [CrossRef]
- Nordenskjöld, A.M.; Lagerqvist, B.; Baron, T.; Jernberg, T.; Hadziosmanovic, N.; Reynolds, H.R.; Tornvall, P.; Lindahl, B. Reinfarction in Patients with Myocardial Infarction with Nonobstructive Coronary Arteries (MINOCA): Coronary Findings and Prognosis. Am. J. Med. 2019, 132, 335–346. [Google Scholar] [CrossRef] [Green Version]
- Olesen, K.K.W.; Madsen, M.; Gyldenkerne, C.; Thrane, P.G.; Thim, T.; Jensen, L.O.; Bøtker, H.E.; Sørensen, H.T.; Maeng, M. Ten-year cardiovascular risk in diabetes patients without obstructive coronary artery disease: A retrospective Western Denmark cohort study. Cardiovasc. Diabetol. 2021, 20, 23. [Google Scholar] [CrossRef] [PubMed]
- Paolisso, P.; Donati, F.; Bergamaschi, L.; Toniolo, S.; D’Angelo, E.; Magnani, I.; Angeli, F.; Bartoli, L.; Stefanizzi, A.; Foa’, A.; et al. Impact of type 2 diabetes mellitus and blood glucose admission levels in patients with myocardial infarction with non obstructive coronary artery disease (MINOCA). Eur. Heart J. 2020, 41 (Suppl. 2), ehaa946.1808. [Google Scholar] [CrossRef]
- Lopez-Pais, J.; Coronel, B.I.; Gil, D.G.; Jesús, M.; Pascual, E.; Durán, B.A.; Peredo, C.G.M.; Vinués, C.M.; García, P.A.; Gonzalez-Juanatey, J.R.; et al. Clinical characteristics and prognosis of myocardial infarction with non-obstructive coronary arteries (MINOCA): A prospective single-center study. Cardiol. J. 2020; epub ahead of print. [Google Scholar] [CrossRef]
- Kobo, O.M.; Vainer Evgrafov, E.; Cohen, Y.; Lerner, Y.; Khatib, A.; Hoffman, R.; Roguin, A.; Tzoran, I. Non-ST-Elevation Myocardial Infarction with Non-significant Coronary Artery Disease as a Symptom of Occult or New Malignancy—PubMed. Isr. Med. Assoc. J. 2019, 21, 381–385. [Google Scholar]
- Bansilal, S.; Aneja, A.; Mathew, V.; Reeder, G.S.; Smars, P.A.; Lennon, R.J.; Wiste, H.J.; Traverse, K.; Farkouh, M.E. Long-term cardiovascular outcomes in patients with angina pectoris presenting with bundle branch block. Am. J. Cardiol. 2011, 107, 1565–1570. [Google Scholar] [CrossRef]
- Ciliberti, G.; Coiro, S.; Tritto, I.; Benedetti, M.; Guerra, F.; Del Pinto, M.; Finocchiaro, G.; Cavallini, C.; Capucci, A.; Kaski, J.C.; et al. Predictors of poor clinical outcomes in patients with acute myocardial infarction and non-obstructed coronary arteries (MINOCA). Int. J. Cardiol. 2018, 267, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Miao, B.; Hernandez, A.V.; Alberts, M.J.; Mangiafico, N.; Roman, Y.M.; Coleman, C.I. Incidence and Predictors of Major Adverse Cardiovascular Events in Patients with Established Atherosclerotic Disease or Multiple Risk Factors. J. Am. Heart Assoc. 2020, 9, e014402. [Google Scholar] [CrossRef]
- Eskerud, I.; Gerdts, E.; Larsen, T.H.; Lønnebakken, M.T. Left ventricular hypertrophy contributes to Myocardial Ischemia in Non-obstructive Coronary Artery Disease (the MicroCAD study). Int. J. Cardiol. 2019, 286, 1–6. [Google Scholar] [CrossRef]
- Stiermaier, T.; Pöss, J.; Eitel, C.; de Waha, S.; Fuernau, G.; Desch, S.; Thiele, H.; Eitel, I. Impact of left ventricular hypertrophy on myocardial injury in patients with ST-segment elevation myocardial infarction. Clin. Res. Cardiol. 2018, 107, 1013–1020. [Google Scholar] [CrossRef]
- Paolisso, P.; Bergamaschi, L.; Saturi, G.; D’Angelo, E.C.; Magnani, I.; Toniolo, S.; Stefanizzi, A.; Rinaldi, A.; Bartoli, L.; Angeli, F.; et al. Secondary prevention medical therapy and outcomes in patients with myocardial infarction with non-obstructive coronary artery disease. Front. Pharmacol. 2020, 10, 1606. [Google Scholar] [CrossRef]
- Ciliberti, G.; Verdoia, M.; Merlo, M.; Zilio, F.; Vatrano, M.; Bianco, F.; Mancone, M.; Zaffalon, D.; Bonci, A.; Boscutti, A.; et al. Pharmacological therapy for the prevention of cardiovascular events in patients with myocardial infarction with non-obstructed coronary arteries (MINOCA): Insights from a multicentre national registry. Int. J. Cardiol. 2021, 327, 9–14. [Google Scholar] [CrossRef]
- Legutko, J.; Niewiara, L.; Bartus, S.; Dobrzycki, S.; Gasior, M.; Gierlotka, M.; Kochman, J.; Lesiak, M.; Matysek, J.; Ochała, A.; et al. Decline in the number of coronary angiography and percutaneous coronary intervention procedures in patients with acute myocardial infarction in Poland during the coronavirus disease 2019 pandemic. Kardiol. Pol. 2020, 78, 574–576. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Group | Primary Composite Endpoint | p Value | ||
|---|---|---|---|---|
| No | Yes | |||
| n = 110 | n = 70 (63.7%) | n = 40 (36.3%) | ||
| Sex, male n (%) | 42 (38.2%) | 27 (38.6%) | 15 (37.5%) | 0.917 |
| Age | 64.9 (13.5) | 62.9 (13.4) | 68.4 (13.3) | 0.040 * |
| BMI | 27.7 (5.44) | 27.5 (5.04) | 28.2 (6.27) | 0.607 |
| Follow-up duration (days) | 724 (308) | 725 (305) | 721 (317) | 0.939 |
| Medical history: | ||||
| Arterial hypertension | 76 (69.1%) | 44 (62.9%) | 32 (80.0%) | 0.064 |
| Dyslipidemia | 58 (52.7%) | 34 (48.6%) | 24 (60.0%) | 0.257 |
| Diabetes type 2 | 21 (19.1%) | 9 (12.9%) | 12 (30.0%) | 0.035 * |
| Smoking | 24 (21.8%) | 16 (22.9%) | 8 (20.0%) | 0.743 |
| Neoplasm | 11 (10.0%) | 3 (4.29%) | 8 (20.0%) | 0.013 * |
| Prior ACS | 11 (10.0%) | 4 (5.71%) | 7 (17.5%) | 0.063 |
| Laboratory tests: | ||||
| Peak hsT troponin | 0.48 (0.59) | 0.53 (0.66) | 0.39 (0.42) | 0.238 |
| Peak CKMB | 38.2 (30.0) | 40.9 (33.1) | 33.5 (23.4) | 0.230 |
| WBC | 9.59 (4.06) | 9.74 (4.15) | 9.32 (3.94) | 0.595 |
| HGB | 13.6 (1.91) | 13.8 (2.14) | 13.4 (1.42) | 0.324 |
| LDL | 2.85 (1.08) | 2.86 (1.06) | 2.83 (1.14) | 0.880 |
| CRP | 13.2 (42.5) | 16.8 (53.1) | 7.42 (13.3) | 0.399 |
| D-dimer | 1399 (2198) | 1116 (1340) | 1977 (3298) | 0.180 |
| eGFR | 76.5 (21.5) | 79.4 (22.0) | 71.3 (19.9) | 0.061 |
| Coronary angiography: | ||||
| Gensini score | 9.02 (7.41) | 7.78 (5.77) | 11.2 (9.33) | 0.034 * |
| ECG on discharge | ||||
| Rhythm: | ||||
| Sinus | 102 (92.7%) | 67 (95.7%) | 35 (87.5%) | 0.242 |
| AF | 5 (4.55%) | 2 (2.86%) | 3 (7.50%) | |
| Stimulation | 3 (2.73%) | 1 (1.43%) | 3 (5.00%) | |
| ST depression | 15 (14.4%) | 6 (8.82%) | 9 (25.0%) | 0.035 * |
| Reversed T wave | 56 (53.8%) | 33 (48.5%) | 23 (63.9%) | 0.142 |
| LBBB/RBBB | 11 (10.6%) | 3 (4.41%) | 8 (22.2%) | 0.009 * |
| Echocardiography on discharge: | ||||
| IVS | 11.2 (2.14) | 10.8 (1.86) | 12.1 (2.39) | 0.006 * |
| PW | 10.3 (1.98) | 9.93 (1.60) | 11.1 (2.39) | 0.006 * |
| LVEF | 54.2 (11.4) | 54.9 (11.4) | 53.1 (11.5) | 0.441 |
| . | Study Group | Primary Composite Endpoint | p Value | |
|---|---|---|---|---|
| No | Yes | |||
| n = 110 | n = 70 (63.7%) | n = 40 (36.3%) | ||
| Pharmacological treatment: | ||||
| B-blocker | 81 (73.6%) | 54 (77.1%) | 27 (67.5%) | 0.282 |
| Ca-blocker | 39 (35.5%) | 24 (34.3%) | 15 (37.5%) | 0.737 |
| ACEI/ARB | 88 (80%) | 54 (77.1%) | 34 (85.0%) | 0.337 |
| Statin | 98 (89.1%) | 64 (91.4%) | 34 (85.0%) | 0.321 |
| SAPT | 31 (28.2%) | 23 (32.9%) | 8 (20.0%) | 0.156 |
| DAPT | 48 (43.6%) | 29 (41.4%) | 19 (47.5%) | 0.544 |
| DAPT+OAC | 10 (9.1%) | 6 (8.6%) | 4 (10.0%) | 0.798 |
| OAC | 16 (14.5%) | 8 (11.4%) | 8 (20.0%) | 0.239 |
| Composite Endpoint | 40 (36.4%) |
|---|---|
| Re-hospitalization due to CVD | 16 (14.6%) |
| All-cause death | 13 (11.8%) |
| Re-MI | 7 (6.4%) |
| Stroke/TIA | 3 (2.7%) |
| Revascularization (PCI/CABG) | 1 (0.9%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szolc, P.; Niewiara, Ł.; Kleczyński, P.; Bryniarski, K.; Ostrowska-Kaim, E.; Szkodoń, K.; Brzychczy, P.; Żmudka, K.; Legutko, J.; Guzik, B. Clinical Characteristics Predicting Worse Long-Term Outcomes in Patients with Myocardial Infarction and Non-Obstructive Coronary Arteries (MINOCA). J. Cardiovasc. Dev. Dis. 2022, 9, 286. https://doi.org/10.3390/jcdd9090286
Szolc P, Niewiara Ł, Kleczyński P, Bryniarski K, Ostrowska-Kaim E, Szkodoń K, Brzychczy P, Żmudka K, Legutko J, Guzik B. Clinical Characteristics Predicting Worse Long-Term Outcomes in Patients with Myocardial Infarction and Non-Obstructive Coronary Arteries (MINOCA). Journal of Cardiovascular Development and Disease. 2022; 9(9):286. https://doi.org/10.3390/jcdd9090286
Chicago/Turabian StyleSzolc, Piotr, Łukasz Niewiara, Paweł Kleczyński, Krzysztof Bryniarski, Elżbieta Ostrowska-Kaim, Kornelia Szkodoń, Piotr Brzychczy, Krzysztof Żmudka, Jacek Legutko, and Bartłomiej Guzik. 2022. "Clinical Characteristics Predicting Worse Long-Term Outcomes in Patients with Myocardial Infarction and Non-Obstructive Coronary Arteries (MINOCA)" Journal of Cardiovascular Development and Disease 9, no. 9: 286. https://doi.org/10.3390/jcdd9090286