
Characteristics and Prognostic Relevance of Ventricular Arrhythmia in Patients with Myocarditis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ventricular Arrhythmia Characteristics
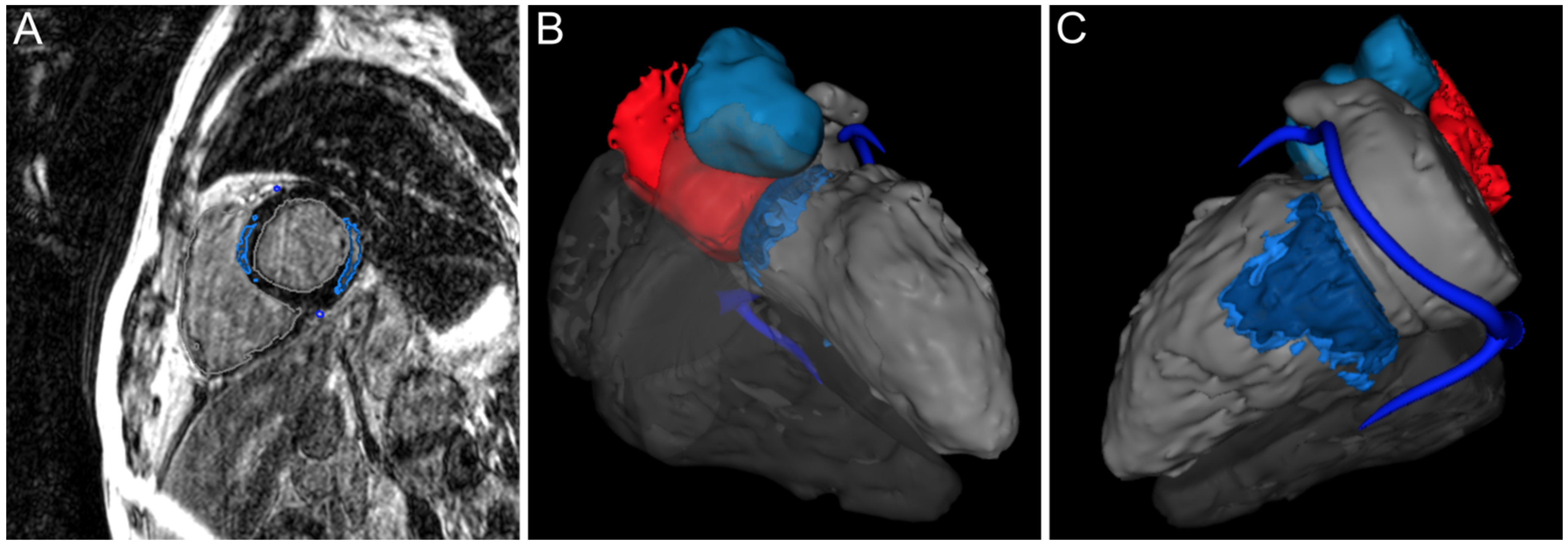
2.3. Cardiac Magnetic Resonance Imaging
2.4. Treatment and Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Ventricular Arrhythmia Characteristics
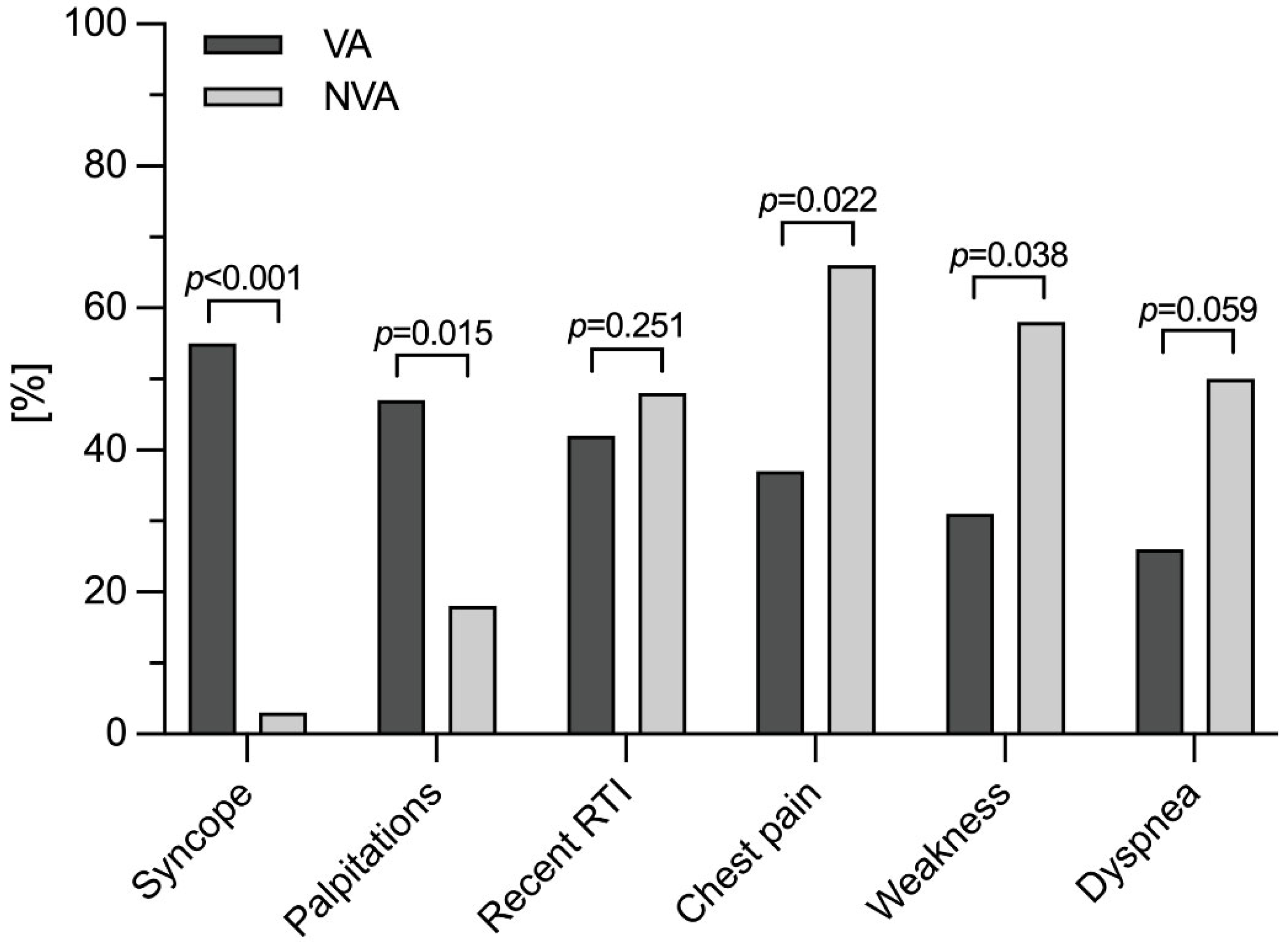
3.3. Diagnostic Characteristics
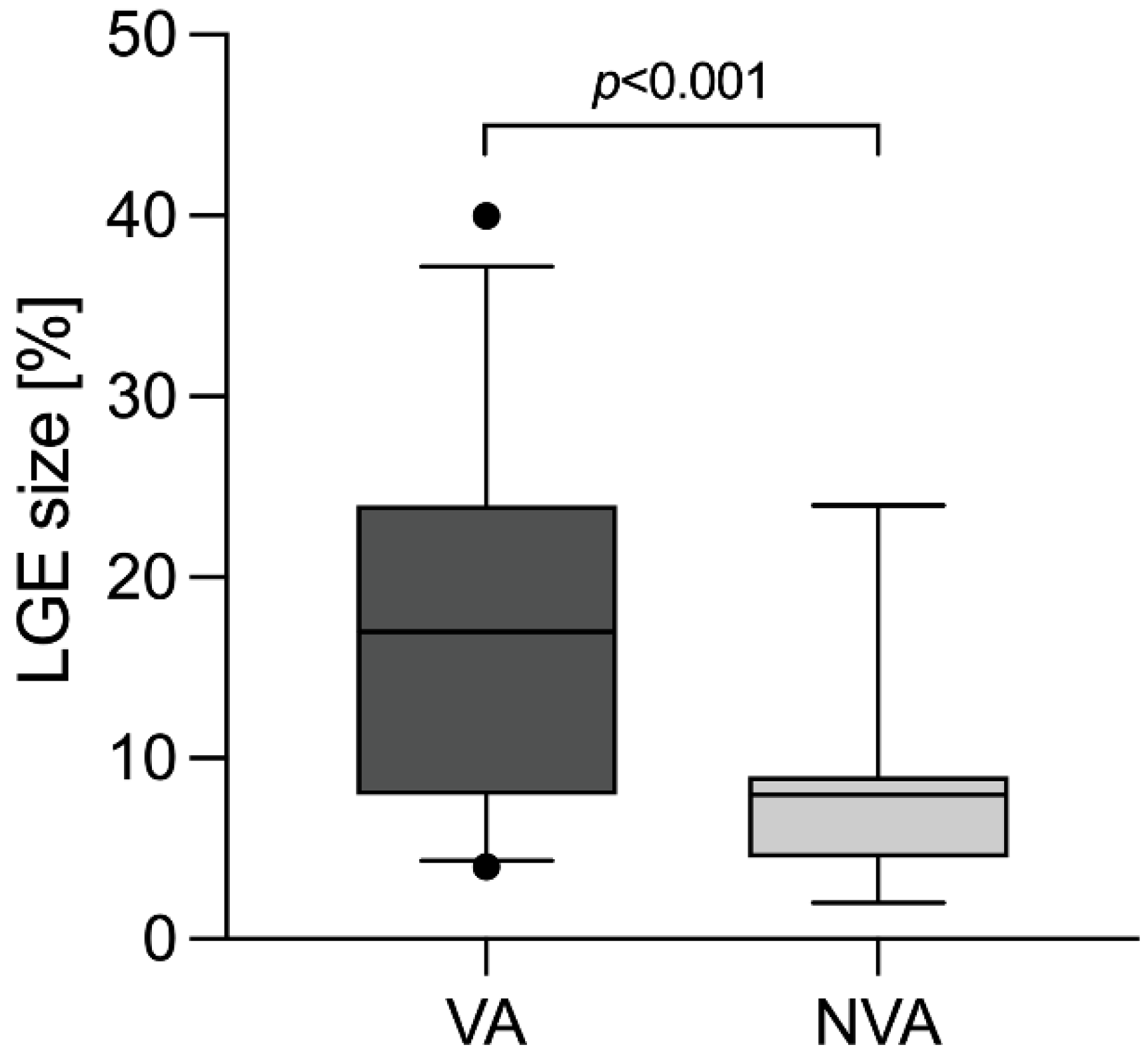
3.4. Cardiac Magnetic Resonance Imaging
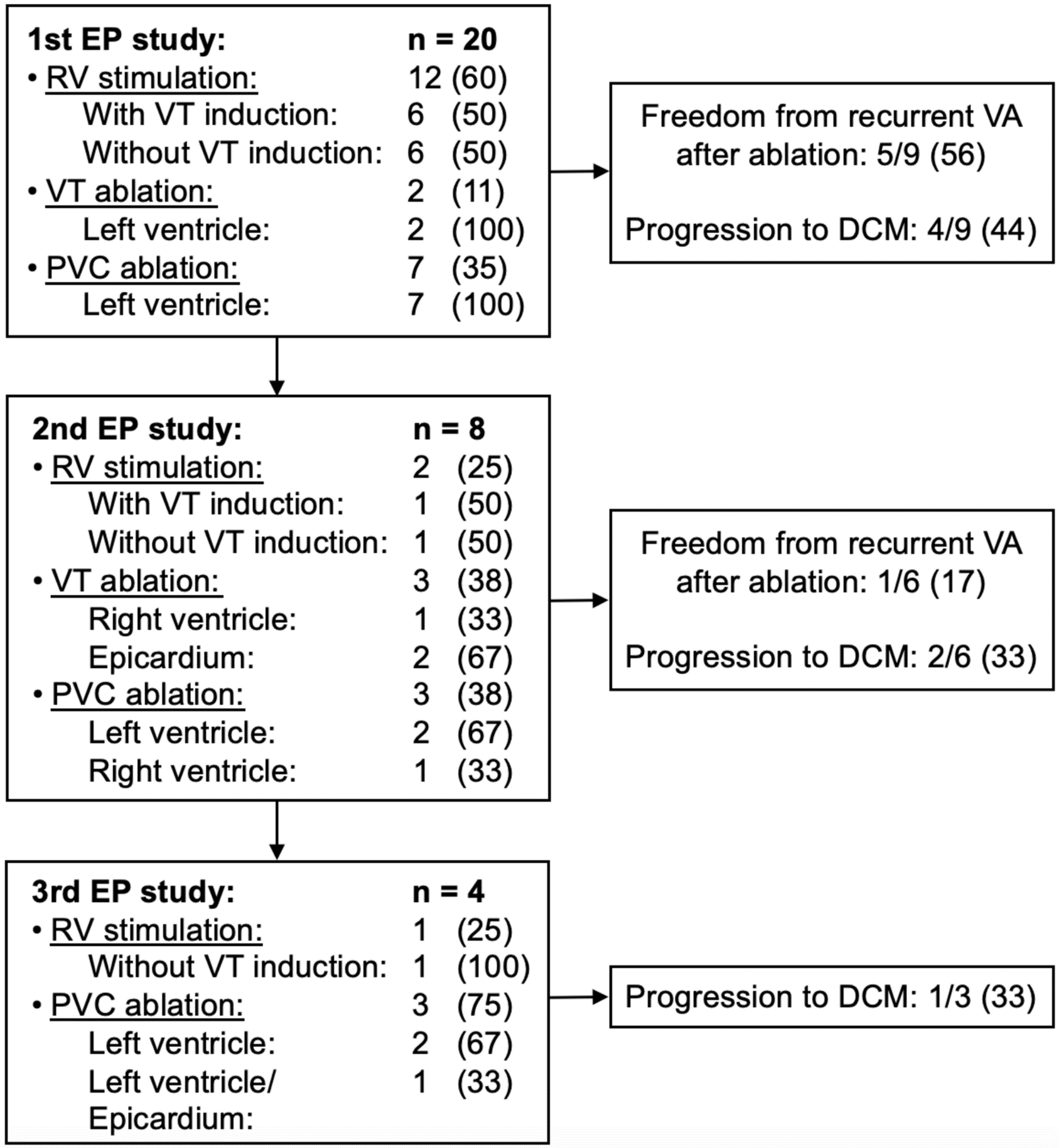
3.5. Myocarditis Treatment
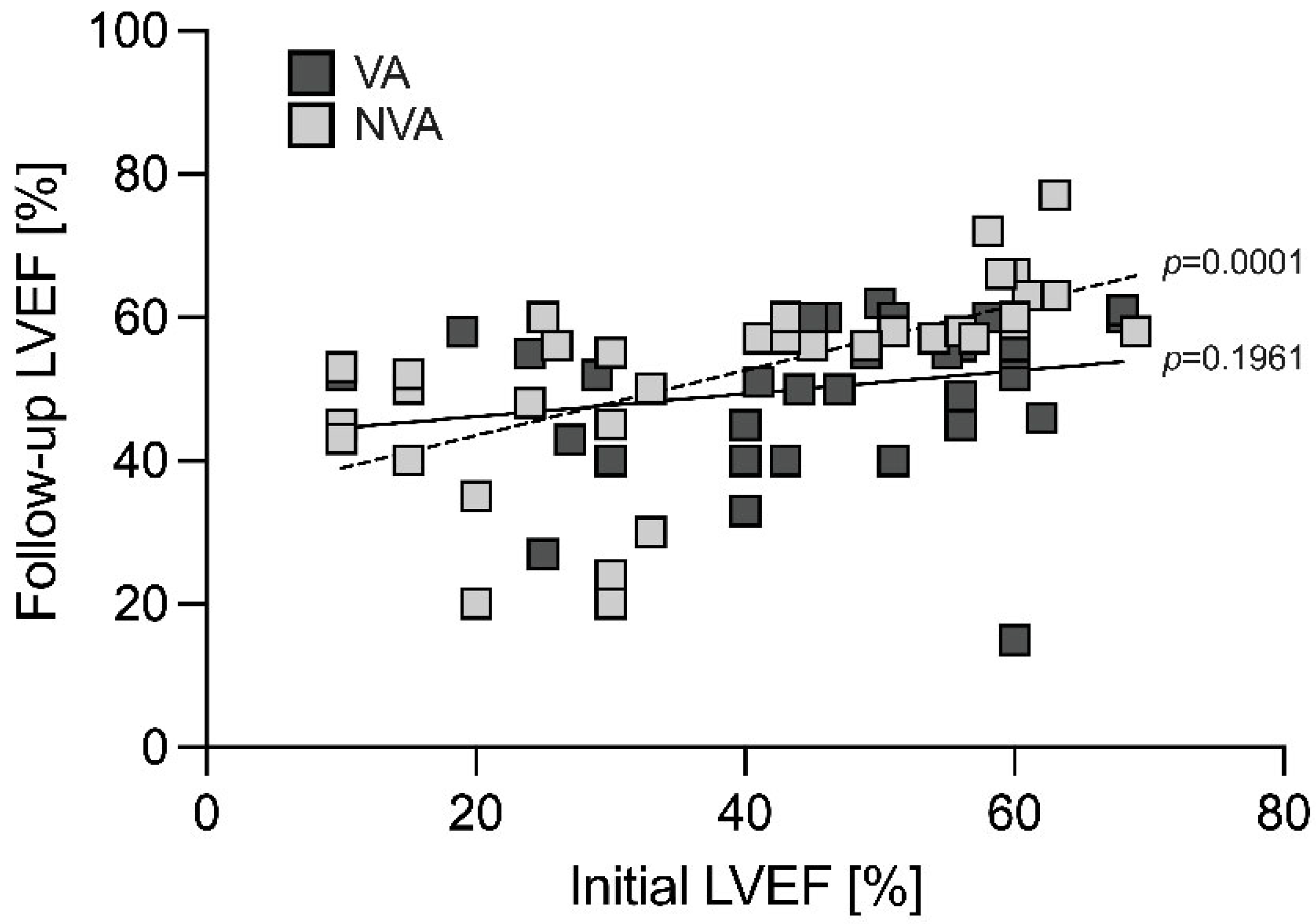
3.6. Follow-Up
3.7. Cases with Fatal Outcome
4. Discussion
4.1. Prognostic Value of Left Ventricular Ejection Fraction
4.2. Importance of Cardiac Magnetic Resonance Imaging
4.3. Treatment of Ventricular Arrhythmia in Patients with Myocarditis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tung, R.; Bauer, B.; Schelbert, H.; Lynch, J.P.; Auerbach, M.; Gupta, P.; Schiepers, C.; Chan, S.; Ferris, J.; Barrio, M.; et al. Incidence of abnormal positron emission tomography in patients with unexplained cardiomyopathy and ventricular arrhythmias: The potential role of occult inflammation in arrhythmogenesis. Heart Rhythm 2015, 12, 2488–2498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakkireddy, D.; Turagam, M.K.; Yarlagadda, B.; Dar, T.; Hamblin, M.; Krause, M.; Parikh, V.; Bommana, S.; Atkins, D.; Di Biase, L.; et al. Myocarditis Causing Premature Ventricular Contractions: Insights from the MAVERIC Registry. Circ. Arrhythm. Electrophysiol. 2019, 12, e007520. [Google Scholar] [CrossRef] [PubMed]
- Anzini, M.; Merlo, M.; Sabbadini, G.; Barbati, G.; Finocchiaro, G.; Pinamonti, B.; Salvi, A.; Perkan, A.; Di Lenarda, A.; Bussani, R.; et al. Long-term evolution and prognostic stratification of biopsy-proven active myocarditis. Circulation 2013, 128, 2384–2394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caforio, A.L.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart. J. 2013, 34, 2636–2648, 2648a–2648d. [Google Scholar] [CrossRef] [PubMed]
- Priori, S.G.; Blomström-Lundqvist, C.; Mazzanti, A.; Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.M.; Fitzsimons, D.; Hatala, R.; Hindricks, G.; et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur. Heart. J. 2015, 36, 2793–2867. [Google Scholar]
- Te, A.L.D.; Wu, T.C.; Lin, Y.J.; Chen, Y.Y.; Chung, F.P.; Chang, S.L.; Lo, L.W.; Hu, Y.F.; Tuan, T.C.; Chao, T.F.; et al. Increased risk of ventricular tachycardia and cardiovascular death in patients with myocarditis during the long-term follow-up: A national representative cohort from the National Health Insurance Research Database. Medicine 2017, 96, e6633. [Google Scholar] [CrossRef]
- Richardson, P.; McKenna, W.; Bristow, M.; Maisch, B.; Mautner, B.; O’Connell, J.; Olsen, E.; Thiene, G.; Goodwin, J.; Gyarfas, I.; et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of cardiomyopathies. Circulation 1996, 93, 841–842. [Google Scholar]
- Aretz, H.T.; Billingham, M.E.; Edwards, W.D.; Factor, S.M.; Fallon, J.T.; Fenoglio, J.J.; Olsen, E.G.; Schoen, F.J. Myocarditis. A histopathologic definition and classification. Am. J. Cardiovasc. Pathol. 1987, 1, 3–14. [Google Scholar]
- Caforio, A.L.; Calabrese, F.; Angelini, A.; Tona, F.; Vinci, A.; Bottaro, S.; Ramondo, A.; Carturan, E.; Iliceta, S.; Thiene, G.; et al. A prospective study of biopsy-proven myocarditis: Prognostic relevance of clinical and aetiopathogenetic features at diagnosis. Eur. Heart. J. 2007, 28, 1326–1333. [Google Scholar] [CrossRef] [Green Version]
- Narducci, M.L.; Rio, T.; Perna, F.; D’Amario, D.; Merlino, B.; Marano, R.; Bencardino, G.; Inzani, F.; Pelargonio, G.; Crea, F. A Challenging Case Of Ventricular Arrhythmia In A Patient With Myocarditis: ICD Yes/No After Ablation. J. Atr. Fibrillation. 2014, 7, 1121. [Google Scholar]
- Dello Russo, A.; Casella, M.; Pieroni, M.; Pelargonio, G.; Bartoletti, S.; Santangeli, P.; Zucchetti, M.; Innocenti, E.; Di Biase, L.; Carbucicchio, C.; et al. Drug-refractory ventricular tachycardias after myocarditis: Endocardial and epicardial radiofrequency catheter ablation. Circ. Arrhythm. Electrophysiol. 2012, 5, 492–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarzl, J.M.; Schleberger, R.; Kahle, A.K.; Höller, A.; Schwarzl, M.; Schaeffer, B.N.; Münkler, P.; Moser, J.; Akbulak, R.Ö.; Eickholt, C.; et al. Specific electrogram characteristics impact substrate ablation target area in patients with scar-related ventricular tachycardia-insights from automated ultrahigh-density mapping. J. Cardiovasc. Electrophysiol. 2021, 32, 376–388. [Google Scholar] [CrossRef]
- Friedrich, M.G.; Sechtem, U.; Schulz-Menger, J.; Holmvang, G.; Alakija, P.; Cooper, L.T.; White, J.A.; Abdel-Aty, H.; Gutberlet, M.; Prasad, S.; et al. Cardiovascular magnetic resonance in myocarditis: A JACC White Paper. J. Am. Coll. Cardiol. 2009, 53, 1475–1487. [Google Scholar] [CrossRef] [Green Version]
- Radunski, U.K.; Lund, G.K.; Säring, D.; Bohnen, S.; Stehning, C.; Schnackenburg, B.; Avanesov, M.; Tahir, E.; Adam, G.; Blankenberg, S.; et al. T1 and T2 mapping cardiovascular magnetic resonance imaging techniques reveal unapparent myocardial injury in patients with myocarditis. Clin. Res. Cardiol. 2017, 106, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Radunski, U.K.; Lund, G.K.; Stehning, C.; Schnackenburg, B.; Bohnen, S.; Adam, G.; Blankenberg, S.; Muellerleile, K. CMR in patients with severe myocarditis: Diagnostic value of quantitative tissue markers including extracellular volume imaging. J. Am. Coll. Cardiol. Img. 2014, 7, 667–675. [Google Scholar] [CrossRef] [Green Version]
- Schulz-Menger, J.; Bluemke, D.A.; Bremerich, J.; Flamm, S.D.; Fogel, M.A.; Friedrich, M.G.; Kim, R.J.; von Knobelsdorff-Brenkenhoff, F.; Kramer, C.M.; Pennell, D.J.; et al. Standardized image interpretation and post-processing in cardiovascular magnetic resonance—2020 update: Society for Cardiovascular Magnetic Resonance (SCMR): Board of Trustees Task Force on Standardized Post-Processing. J. Cardiovasc. Magn. Reson. 2020, 22, 19. [Google Scholar] [CrossRef] [PubMed]
- Cerqueira, M.D.; Weissman, N.J.; Dilsizian, V.; Jacobs, A.K.; Kaul, S.; Laskey, W.K.; Pennell, D.J.; Rumberger, J.A.; Ryan, T.; Verani, M.S.; et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation 2002, 105, 539–542. [Google Scholar] [PubMed] [Green Version]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart. J. 2021, 42, 3599–3726. [Google Scholar]
- Ghimire, A.; Fine, N.; Ezekowitz, J.A.; Howlett, J.; Youngson, E.; McAlister, F.A. Frequency, predictors, and prognosis of ejection fraction improvement in heart failure: An echocardiogram-based registry study. Eur. Heart. J. 2019, 40, 2110–2117. [Google Scholar] [CrossRef]
- Vermes, E.; Childs, H.; Faris, P.; Friedrich, M.G. Predictive value of CMR criteria for LV functional improvement in patients with acute myocarditis. Eur. Heart. J. Cardiovasc. Imaging. 2014, 15, 1140–1144. [Google Scholar] [CrossRef] [Green Version]
- Grün, S.; Schumm, J.; Greulich, S.; Wagner, A.; Schneider, S.; Bruder, O.; Kispert, E.M.; Hill, S.; Ong, P.; Klingel, K.; et al. Long-term follow-up of biopsy-proven viral myocarditis: Predictors of mortality and incomplete recovery. J. Am. Coll. Cardiol. 2012, 59, 1604–1615. [Google Scholar] [CrossRef] [PubMed]
- Di Bella, G.; Camastra, G.; Monti, L.; Dellegrottaglie, S.; Piaggi, P.; Moro, C.; Pepe, A.; Lanzillo, C.; Pontone, G.; Perazzolo Marra, M.; et al. Left and right ventricular morphology, function and late gadolinium enhancement extent and localization change with different clinical presentation of acute myocarditis Data from the ITAlian multicenter study on MYocarditis (ITAMY). J. Cardiovasc. Med. 2017, 18, 881–887. [Google Scholar] [CrossRef]
- Francone, M.; Chimenti, C.; Galea, N.; Scopelliti, F.; Verardo, R.; Galea, R.; Carbone, I.; Catalano, C.; Fedele, F.; Frustaci, A. CMR sensitivity varies with clinical presentation and extent of cell necrosis in biopsy-proven acute myocarditis. J. Am. Coll. Cardiol. Img. 2014, 7, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Frustaci, A.; Chimenti, C. Images in cardiovascular medicine. Cryptogenic ventricular arrhythmias and sudden death by Fabry disease: Prominent infiltration of cardiac conduction tissue. Circulation 2007, 116, e350–e351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Münkler, P.; Klatt, N.; Willems, S.; Meyer, C. High-density mapping-based ablation strategy in a 30-year-old patient with a history of myocarditis. Europace 2019, 21, iii11–iii12. [Google Scholar] [CrossRef]
- De Cobelli, F.; Pieroni, M.; Esposito, A.; Chimenti, C.; Belloni, E.; Mellone, R.; Canu, T.; Perseghin, G.; Faudio, C.; Maseri, A.; et al. Delayed gadolinium-enhanced cardiac magnetic resonance in patients with chronic myocarditis presenting with heart failure or recurrent arrhythmias. J. Am. Coll. Cardiol. 2006, 47, 1649–1654. [Google Scholar] [CrossRef] [Green Version]
- Maccabelli, G.; Tsiachris, D.; Silberbauer, J.; Esposito, A.; Bisceglia, C.; Baratto, F.; Colantoni, C.; Trecisi, B.; Palmisano, A.; Vergara, P.; et al. Imaging and epicardial substrate ablation of ventricular tachycardia in patients late after myocarditis. Europace 2014, 16, 1363–1372. [Google Scholar] [CrossRef]
- Peretto, G.; Sala, S.; Basso, C.; Rizzo, S.; Radinovic, A.; Frontera, A.; Rosaio Limite, L.; Paglino, G.; Bisceglia, C.; De Luca, A.; et al. Inflammation as a Predictor of Recurrent Ventricular Tachycardia After Ablation in Patients with Myocarditis. J. Am. Coll. Cardiol. 2020, 76, 1644–1656. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | VA (n = 38) | NVA (n = 38) | p Value |
|---|---|---|---|
| Age | 45 ± 3 | 38 ± 2 | 0.074 |
| Male sex | 26 (68) | 32 (84) | 0.109 |
| Symptoms | |||
| Syncope | 21 (55) | 1 (3) | <0.001 |
| Chest pain | 14 (37) | 25 (66) | 0.022 |
| Dyspnea | 10 (26) | 19 (50) | 0.059 |
| Weakness | 12 (31) | 22 (58) | 0.038 |
| Recent respiratory infection | 16 (42) | 22 (58) | 0.251 |
| Palpitations | 18 (47) | 7 (18) | 0.015 |
| Laboratory | |||
| Hs-cTnT, pg/mL | 54 (13.15–549.5) | 102 (23.5–408.5) | 0.568 |
| Hs-cTnT < 14 pg/mL | 8 (25) | 3 (9) | 0.168 |
| CRP, mg/L | 25 ± 6 | 54 ± 12 | 0.003 |
| CRP < 5 mg/L | 18 (53) | 6 (17) | 0.004 |
| NT-proBNP, ng/L | 3584 ± 1984 | 3959 ± 1099 | 0.040 |
| NT-proBNP < 248 ng/L | 9 (32) | 5 (18) | 0.314 |
| Echocardiography | |||
| LVEF, % | 47 ± 2 | 40 ± 3 | 0.069 |
| LVEDD, mm | 54 ± 2 | 53 ± 2 | 0.956 |
| LVEF < 30% | 6 (16) | 12 (32) | 0.177 |
| LVEF ≥ 54% | 16 (42) | 12 (32) | 0.476 |
| TAPSE < 17 mm | 2 (5) | 9 (13) | 0.050 |
| Endomyocardial biopsy | |||
| Positive EMB | 22 (79) | 20 (95) | 0.214 |
| Active myocarditis | 12 (55) | 12 (60) | 0.964 |
| Borderline myocarditis | 6 (27) | 5 (25) | 0.854 |
| Previous myocarditis | 4 (18) | 3 (15) | 1.0 |
| Detection of viral infection | 6 (27) | 8 (40) | 0.585 |
| Parvovirus B19 | 2 (33) | 6 (75) | 0.277 |
| Human herpesvirus 6 | 4 (66) | 1 (13) | 0.091 |
| Epstein-Barr virus | 0 (0) | 1 (13) | 1.0 |
| Therapy | |||
| Immunosuppression | 9 (24) | 8 (21) | 0.952 |
| Azathioprine + Prednisolone | 5 (56) | 7 (88) | 0.294 |
| Cyclosporine + MMF + Prednisolone | 1 (11) | 0 (0) | 1.0 |
| Cyclosporine + Prednisolone | 0 (0) | 1 (13) | 1.0 |
| Azathioprine Interferone Prednisolone | 1 (11) 1 (11) 1 (11) | 0 (0) 0 (0) 0 (0) | 1.0 1.0 1.0 |
| Beta-receptor blockers | 31 (82) | 25 (66) | 0.192 |
| Amiodarone | 7 (18) | 1 (3) | 0.056 |
| Variable | VA (n = 34) | NVA (n = 35) | p-Value |
|---|---|---|---|
| LGE | 32 (94) | 24 (69) | 0.016 |
| Edema | 17 (50) | 9 (26) | 0.067 |
| LGE mass, % | 17.6 ± 1.8 | 8.2 ± 1.3 | <0.001 |
| LGE mass, g | 24.7 ± 3.2 | 11.8 ± 2.4 | 0.002 |
| Segments with LGE | 5.5 ± 0.5 | 3.9 ± 0.5 | 0.062 |
| LVEDV, mL | 179.6 ± 12.1 | 180.7 ± 10.8 | 0.849 |
| LVESV, mL | 90 ± 9.5 | 102.8 ± 12 | 0.693 |
| LVSV, mL | 90 ± 5.1 | 80.9 ± 5.8 | 0.210 |
| LVEF, % | 52.3 ± 2.2 | 47.2 ± 3.4 | 0.595 |
| LVEDM, g | 156.1 ± 7.1 | 159 ± 7.1 | 0.665 |
| Variable | VA (n = 36) | NVA (n = 35) | p Value |
|---|---|---|---|
| LVEF, % | 51 ± 2 | 53 ± 2 | 0.326 |
| DCM with LVEF ≤ 45% | 10 (28) | 9 (26) | 1.0 |
| Initial LVEF, % | 45 ± 4 | 21 ± 3 | <0.001 |
| WCD equipment | 14 (39) | 6 (17) | 0.076 |
| ICD over time | 5 (36) | 1 (17) | 0.613 |
| LVEF improvement | 12 (33) | 18 (52) | 1.0 |
| ICD implantation | 17 (47) | 6 (17) | 0.014 |
| ICD shock delivery | 5 (29) | 1 (17) | 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kahle, A.-K.; Güde, R.; Schwarzl, J.M.; Münkler, P.; Akbulak, R.Ö.; Jahnke, C.; Bohnen, S.; Würger, T.; Schwarzl, M.; Willems, S.; et al. Characteristics and Prognostic Relevance of Ventricular Arrhythmia in Patients with Myocarditis. J. Cardiovasc. Dev. Dis. 2022, 9, 243. https://doi.org/10.3390/jcdd9080243
Kahle A-K, Güde R, Schwarzl JM, Münkler P, Akbulak RÖ, Jahnke C, Bohnen S, Würger T, Schwarzl M, Willems S, et al. Characteristics and Prognostic Relevance of Ventricular Arrhythmia in Patients with Myocarditis. Journal of Cardiovascular Development and Disease. 2022; 9(8):243. https://doi.org/10.3390/jcdd9080243
Chicago/Turabian StyleKahle, Ann-Kathrin, Rebekka Güde, Jana M. Schwarzl, Paula Münkler, Ruken Ö. Akbulak, Charlotte Jahnke, Sebastian Bohnen, Tilman Würger, Michael Schwarzl, Stephan Willems, and et al. 2022. "Characteristics and Prognostic Relevance of Ventricular Arrhythmia in Patients with Myocarditis" Journal of Cardiovascular Development and Disease 9, no. 8: 243. https://doi.org/10.3390/jcdd9080243