
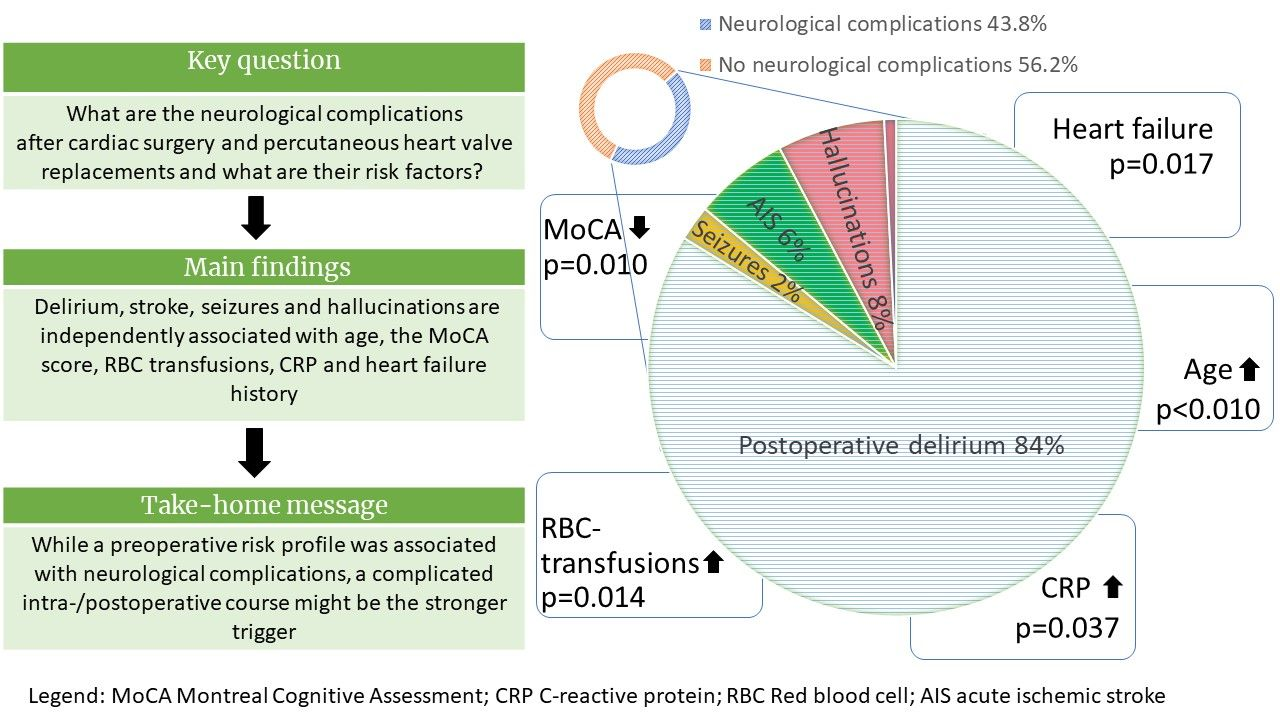
Stroke, Seizures, Hallucinations and Postoperative Delirium as Neurological Complications after Cardiac Surgery and Percutaneous Valve Replacement
 , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Screening of Neurological Complications
2.3. Clinical Data Warehouse
2.4. Statistical Analysis
3. Results
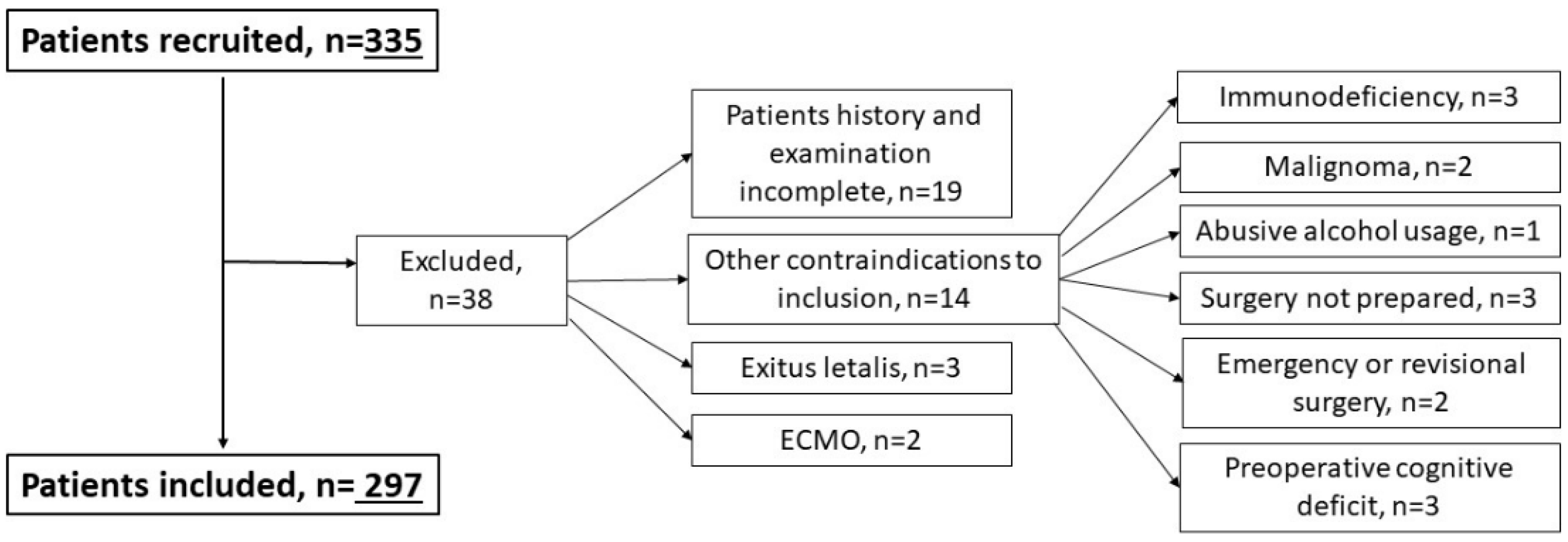
3.1. Legend: ECMO Extracorporeal Membrane Oxygenation
3.1.1. Patients’ Characteristics
3.1.2. POD Characteristics
3.1.3. Characteristics of AIS, Seizures and Hallucinations
3.1.4. Risk Factors for Postoperative Neurological Complications
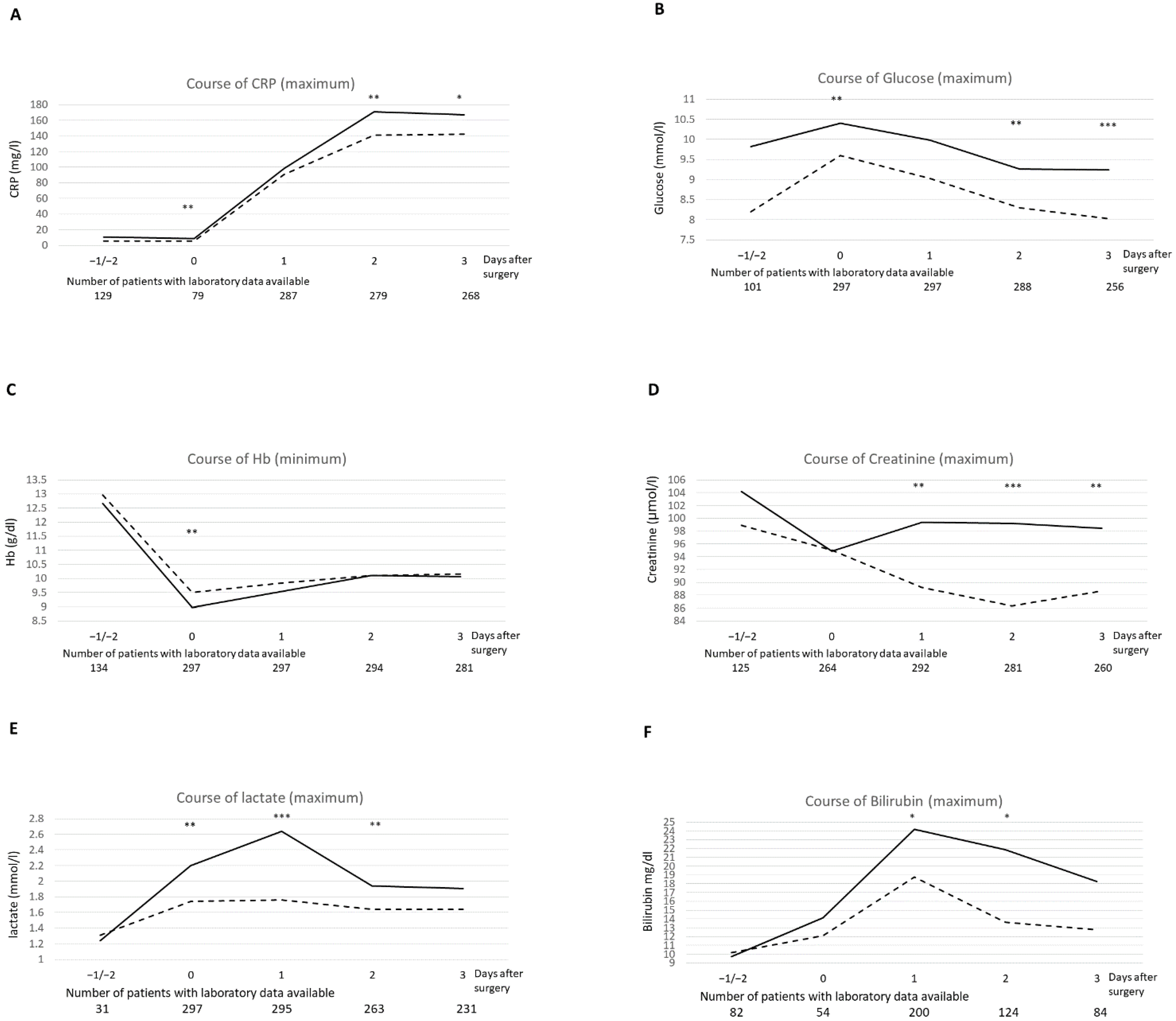
3.1.5. Laboratory Risk Factors
3.1.6. Multivariable Analysis of Risk Factors for Postoperative Neurological Complications
3.1.7. Hallucinations as Postoperative Neurological Complications
3.1.8. Comparison of Percutaneous Valve Replacement and Cardiac Surgery
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACI | arteria carotid interna |
| AIS | acute ischemic stroke |
| ASA | American Society of Anaesthesiologists |
| CAM | Confusion Assessment Method |
| CAM-ICU | Confusion Assessment Method for intensive care unit |
| ECMO | Extracorporeal membrane oxygenation |
| EEG | Electroencephalography |
| IQR | Interquartile range |
| MI | Myocardial infarction |
| MoCA | Montreal Cognitive Assessment |
| MRI | Magnetic resonance imaging |
| MST | Malnutrition Screening Tool |
| NIHSS | National Institutes of Health Stroke Scale |
| NRS | Numeric pain rating scale |
| PHQ-2 | Patient Health Questionnaire-2 |
| POD | postoperative delirium |
| RBC | Red blood cell |
| SD | Standard deviation |
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Total Cohort (n = 297 pat.) | Neurological Complications (n = 130 pat.) | No Neurological Complications (n = 167 pat.) | p-Value | |
|---|---|---|---|---|
| CRP max. [mg/L], mean (SD) | 164.25 (90.3) | 180.87 (87.9) | 151.31 (90.27) | 0.005 + |
| Lactate max. [mmol/L], mean (SD) | 2.74 (1.76) | 3.24 (2.16) | 2.35 (1.24) | <0.001 + |
| Hb min. [g/dl], mean (SD) | 8.56 (1.67) | 8.33 (1.73) | 8.75 (1.6) | 0.004 + |
| Sodium max. [mmol/L], mean (SD) | 143.44 (3.15) | 144.3 (3.85) | 142.77 (2.27) | <0.001 + |
| Sodium min. [mmol/L], mean (SD) | 134.9 (2.95) | 134.89 (3.41) | 134.91 (2.54) | 0.316 + |
| Potassium max. [mmol/L], mean (SD) | 5.57 (0.81) | 5.7 (0.85) | 5.48 (0.76) | 0.141 + |
| Potassium min. [mmol/L], mean (SD) | 3.71 (0.35) | 3.72 (0.38) | 3.7 (0.32) | 0.397 + |
| Glucose max. [mmol/L], mean (SD) | 11.11 (2.95) | 11.7 (3.1) | 10.66 (2.76) | 0.001 + |
| Glucose min. [mmol/L], mean (SD) | 5.2 (1.04) | 5.26 (1.04) | 5.16 (1.04) | 0.846 + |
| Creatinine max. [μmol/L], mean (SD) | 104.71 (61.5) | 109.2 (38.96) | 101.22 (74.45) | 0.003 + |
| Leucocytes max. [cells/µL], mean (SD) | 12.97 (4.52) | 13.68 (4.78) | 12.41 (4.23) | 0.021 + |
| Calcium max. [mmol/L], mean (SD) | 1.9 (0.43) | 1.91 (0.40) | 1.91 (0.45) | 0.474 + |
| Calcium min. [mmol/L], mean (SD) | 1.13 (0.07) | 1.12 (0.08) | 1.13 (0.07) | 0.743 + |
| Percutaneous Valve Replacement (n = 61) | Cardiac Surgery (n = 236) | p-Value | |
|---|---|---|---|
| Neurological complications, postoperative | 22 (36.1%) | 108 (45.8%) | 0.174 |
| Hallucinations, postoperative | 10 (16.4%) | 53 (22.5%) | 0.302 |
| Isolated POD, postoperative | 22 (36.1%) | 96 (42.7%) | 0.353 |
| AIS, postoperative | 0 (0%) | 8 (3.4%) | 0.368 * |
| Focal/generalized seizure, postoperative | 0 (0%) | 4 (1.7%) | 0.585 * |
| Sex, female | 36 (59%) | 74 (31.4%) | <0.001 + |
| Age [years], median (IQR) | 83 (79–87) | 70.5 (63–77) | <0.001 |
| aHTN, preoperative | 18 (29.5%) | 50 (21.2%) | 0.168 |
| DM | 17 (27.9%) | 62 (26.3%) | 0.801 |
| History of MI | 3 (4.9%) | 43 (18.2%) | 0.010 |
| History of AF | 25 (41%) | 60 (25.4%) | 0.017 |
| Coronary heart disease | 54 (88.5%) | 208 (88.1%) | 0.933 |
| HF | 46 (75.4%) | 124 (52.5%) | 0.001 |
| History of POD | 5 (8.2%) | 16 (6.8%) | 0.700 |
| MoCA severity range preoperative, Median (IQR) | 2 (2–2) | 2 (1–2) | 0.001 * |
| History of neurotrauma | 19 (31.1%) | 86 (36.4%) | 0.441 |
| PHQ-score, median (IQR) | 0 (0–1) | 0 (0–1) | 0.890 * |
| Malnutrition-score, median (IQR) | 0 (0–1) | 0 (0–1) | 0.451 * |
| Premedication sedatives | 5 (8.2%) | 72 (30.5%) | <0.001 |
| ASA-classification, median (IQR) | 3 (3–4) | 3 (3–3) | <0.001 * |
| Duration of surgery [minutes], median (IQR) | 55 (43.5–76.5) | 205 (172–249) | <0.001 + |
| MAP intraoperative min. [mmHg], mean (SD) | 51.97 (13.52) | 30.3 (9.13) | <0.001 + |
| MAP mean [mmHg], mean (SD) | 85.47 (16.93) | 68.32 (4.96) | <0.001 + |
| MAP intraoperative variance [mmHg], mean (SD) | 14.64 (98.21) | 203.12 (88.32) | <0.001 + |
| MAP under 60mmHg | 28 (45.9%) | 232 (98.3%) | <0.001 |
| Number of RBC transfusions (intraop.), median (IQR) | 0 (0–0) | 0 (0–2) | <0.001 + |
| Administration of FFP (intraop.) | 0 (0%) | 14 (5.9%) | 0.082 * |
| Administration of thrombocyte concentrates (intraop.) | 0 (0%) | 30 (12.7%) | 0.003 |
| AF postoperative | 7 (11.5%) | 57 (24.2%) | 0.032 |
| Number of RBC transfusions (total),median (IQR) | 0 (0–0) | 2 (0–4) | <0.001 + |
| Administration of FFP (total) | 0 (0%) | 45 (19.1%) | <0.001 |
| Administration of thrombocyte concentrates (total) | 0 (0%) | 68 (28.8%) | <0.001 |
| Stay in hospital in days, median (IQR) | 7 (6–7) | 9 (7.5–12) | <0.001 + |
| CRP max. [mg/L], mean (SD) | 47.95 (34.94) | 194.31 (74.41) | <0.001 + |
| Lactate max. [mmol/L], mean (SD) | 1.78 (0.71) | 2.98 (1.86) | <0.001 + |
| Hb min. [g/dl], mean (SD) | 9.63 (1.83) | 8.3 (1.5) | <0.001 + |
| Sodium max. [mmol/L], mean (SD) | 141.92 (2.74) | 143.83 (3.13) | <0.001 + |
| Glucose max. [mmol/L], mean (SD) | 9.91 (2.3) | 11.42 (3.02) | <0.001 + |
| Glucose min. [mmol/L], mean (SD) | 5.71 (0.93) | 5.07 (1.02) | <0.001 + |
| Potassium max. [mmol/L], mean (SD) | 4.64 (0.37) | 5.82 (0.70) | <0.001 + |
| Calcium max. [mmol/L], mean (SD) | 1.3 (0.17) | 2.1 (0.32) | <0.001 + |
| Creatinine max. [μmol/L], mean (SD) | 104.72 (33.06) | 104.70 (66.92) | 0.238 + |
| Hallucinations Positive (n = 63 pat.) | Hallucinations Negative (n = 234 pat.) | p-Value | |
|---|---|---|---|
| Sex, female | 18 (28.6%) | 92 (39.3%) | 0.117 |
| Age [years], median (IQR) | 72 (65–79) | 74 (64–80) | 0.765 |
| BMI [kg/m²], mean (SD) | 26.96 (5.01) | 27.62 (5.3) | 0.404 |
| aHTN preoperative | 29 (46%) | 39 (16.7%) | <0.001 |
| History of neurotrauma | 34 (54%) | 71 (30.3%) | <0.001 |
| History of alcohol abuse | 7 (11.1%) | 19 (8.1%) | 0.456 |
| Benzodiazepines, preoperative | 1 (1.6%) | 2 (0.9%) | 1.000 |
| Antidepressants, preoperative | 6 (9.5%) | 7 (3%) | 0.036 * |
| MoCA severity range preoperative, Median (IQR) | 2 (1–2) | 2 (1–2) | 0.744 * |
| sedatives intraoperative | 58 (92.1%) | 188 (80.3%) | 0.029 |
| Hb min. [g/dL], mean (SD), intraoperative | 8.86 (1.4) | 9.35 (1.7) | 0.019 + |
| sodium max. at day 1 postoperative [mmol/L], mean (SD) | 142.76 (3.8) | 141.74 (3.38) | 0.044 + |
| Patient | Type of Surgery | Age | Sex | Postoperative Day of Detection | Localisation Infarction | TOAST Criteria (Aetiology) | Stenosis of Cerebral Vessels | NIHSS Baseline | mRS Baseline | mRS at Discharge | Cerebrovascular Risk Factors | Antithrombotic Treatment |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Valve surgery with cardio-pulmonary-bypass | 74 | m | Day 1 | Brainstem | Cardio-embolic | - | 10 | 5 | 4 | DM, aHTN, AF, CHD, HLP | Phenprocoumon |
| 2 | Valve surgery with cardio-pulmonary-bypass | 74 | f | Day 1 | Territory of MCA (left) | Cardio-embolic | ACI (bifurcation) right and Left (low-grade),ACI (siphon, moderate) | 1 | 2 | 2 | AF, CHD, HF | Phenprocoumon |
| 3 | Valve and bypass surgery with cardio-pulmonary-bypass | 78 | m | Day 1 | Territory of MCA (double-sided) | Cardio-embolic | ICA, right (high-grade) | 29 | 5 | 5 | AIS, CHD, HF, pAOD, MI, HF | Phenprocoumon |
| 4 | Valve surgery with cardio-pulmonary-bypass | 78 | m | Day 1 | Territory of MCA (right) | Cardio-embolic | - | 3 | 3 | 1 | ACI, aHTN, AF, CHD, HF, HLP, adiposis, sclerosis | Phenprocoumon |
| 5 | Valve and bypass surgery with cardio-pulmonary-bypass | 74 | m | Day 1 | Brain stem | Makro-angiopathy competing with cardio-embolic | VA left (high-grade), BA (low-grade), ACI right (moderate) | 12 | 5 | 3 | AIS, DM, aHTN, CHD, HF, pAOD, HLP, history of carotis TEA (right) | Phenprocoumon |
| 6 | Valve surgery with cardio-pulmonary-bypass | 67 | m | Day 1 | Territory of MCA (left) | Cardio-embolic | - | 5 | 4 | 1 | aHTN, AIS, CHD, HF, HLP | Phenprocoumon |
| 7 | Bypass surgery with cardio-pulmonary-bypass | 77 | m | Day 1 | Territory of MCA (left) | Cardio-embolic | - | 4 | 3 | 0 | aHTN, CHD, HF, HLP | ASA |
| 8 | Bypass surgery with cardio-pulmonary-bypass | 78 | m | Day 1 | Cerebellum (double-sided) brain stem | Cardio-embolic | ACI right (high-grade) and left (moderate) | 28 | 5 | 5 | aHTN, AIS, CHD, pAOD, HF, MI, smoking cigarettes | ASA |
References
- Seese, L.; Sultan, I.; Gleason, T.G.; Navid, F.; Wang, Y.; Thoma, F.; Kilic, A. The impact of major postoperative complications on long-term survival after cardiac surgery. Ann. Thorac. Surg. 2020, 110, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Ottens, T.H.; Sommer, I.E.C.; Begemann, M.J.; Schutte, M.; Cramer, M.J.; Suyker, W.J.; van Dijk, D.; Slooter, A.J.C. Hallucinations after cardiac surgery: A prospective observational study. Medicina 2020, 56, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cropsey, C.; Kennedy, J.; Han, J.; Pandharipande, P. Cognitive dysfunction, delirium, and stroke in cardiac surgery patients. Semin. Cardiothorac. Vasc. Anesth. 2015, 19, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.Y.; Chung, A.M.; Farkouh, M.E.; van Diepen, S.; Weinberger, J.; Bourke, M.; Ruel, M. Defining an intraoperative hypotension threshold in association with stroke in cardiac surgery. Anesthesiology 2018, 129, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Tarakji, K.G.; Sabik, J.F.; Bhudia, S.K.; Batizy, L.H.; Blackstone, E.H. Temporal onset, risk factors, and outcomes associated with stroke after coronary artery bypass grafting. JAMA 2011, 305, 381–390. [Google Scholar] [CrossRef]
- Vedel, A.G.; Holmgaard, F.; Rasmussen, L.S.; Langkilde, A.; Paulson, O.B.; Lange, T.; Thomsen, C.; Olsen, P.S.; Ravn, H.B.; Nilsson, J.C. High-target versus low-target blood pressure management during cardiopulmonary bypass to prevent cerebral injury in cardiac surgery patients: A randomized controlled trial. Circulation 2018, 137, 1770–1780. [Google Scholar] [CrossRef]
- Rudolph, J.L.; Jones, R.N.; Levkoff, S.E.; Rockett, C.; Inouye, S.K.; Sellke, F.W.; Khuri, S.F.; Lipsitz, L.A.; Ramlawi, B.; Levitsky, S.; et al. Derivation and validation of a preoperative prediction rule for delirium after cardiac surgery. Circulation 2009, 119, 229–236. [Google Scholar] [CrossRef] [Green Version]
- Raffa, G.M.; Agnello, F.; Occhipinti, G.; Miraglia, R.; Lo Re, V.; Marrone, G.; Tuzzolino, F.; Arcadipane, A.; Pilato, M.; Luca, A. Neurological complications after cardiac surgery: A retrospective case-control study of risk factors and outcome. J. Cardiothorac. Surg. 2019, 14, 23. [Google Scholar] [CrossRef]
- Inouye, S.K.; Westendorp, R.G.J.; Saczynski, J.S. Delirium in elderly people. Lancet 2014, 383, 911–922. [Google Scholar] [CrossRef] [Green Version]
- Peritogiannis, V.; Bolosi, M.; Lixouriotis, C.; Rizos, D.V. Recent insights on prevalence and corelations of hypoactive delirium. Behav. Neurol. 2015, 2015, 416792. [Google Scholar] [CrossRef]
- Marcantonio, E.R.; Ngo, L.H.; O’Connor, M.; Jones, R.N.; Crane, P.K.; Metzger, E.D.; Inouye, S.K. 3d-cam: Derivation and validation of a 3-minute diagnostic interview for cam-defined delirium: A cross-sectional diagnostic test study. Ann. Intern. Med. 2014, 161, 554–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meagher, D.; O’Regan, N.; Ryan, D.; Connolly, W.; Boland, E.; O’Caoimhe, R.; Clare, J.; Mcfarland, J.; Tighe, S.; Leonard, M.; et al. Frequency of delirium and subsyndromal delirium in an adult acute hospital population. Br. J. Psychiatry J. Ment. Sci. 2014, 205, 478–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serafim, R.B.; Soares, M.; Bozza, F.A.; Lapa e Silva, J.R.; Dal-Pizzol, F.; Paulino, M.C.; Povoa, P.; Salluh, J.I.F. Outcomes of subsyndromal delirium in icu: A systematic review and meta-analysis. Crit. Care 2017, 21, 179. [Google Scholar] [CrossRef] [Green Version]
- Telles-Correia, D.; Moreira, A.L.; Gonçalves, J.S. Hallucinations and related concepts-their conceptual background. Front. Psychol. 2015, 6, 991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bramley, P.; McArthur, K.; Blayney, A.; McCullagh, I. Risk factors for postoperative delirium: An umbrella review of systematic reviews. Int. J. Surg. 2021, 93, 106063. [Google Scholar] [CrossRef] [PubMed]
- Danielson, M.; Reinsfelt, B.; Westerlind, A.; Zetterberg, H.; Blennow, K.; Ricksten, S.-E. Effects of methylprednisolone on blood-brain barrier and cerebral inflammation in cardiac surgery-a randomized trial. J. Neuroinflamm. 2018, 15, 283. [Google Scholar] [CrossRef]
- Hovens, I.B.; van Leeuwen, B.L.; Mariani, M.A.; Kraneveld, A.D.; Schoemaker, R.G. Postoperative cognitive dysfunction and neuroinflammation; cardiac surgery and abdominal surgery are not the same. Brain Behav. Immun. 2016, 54, 178–193. [Google Scholar] [CrossRef]
- Rudiger, A.; Begdeda, H.; Babic, D.; Krüger, B.; Seifert, B.; Schubert, M.; Spahn, D.R.; Bettex, D. Intra-operative events during cardiac surgery are risk factors for the development of delirium in the icu. Crit. Care 2016, 20, 264. [Google Scholar] [CrossRef] [Green Version]
- Paparella, D.; Rotunno, C.; Guida, P.; Travascia, M.; de Palo, M.; Paradiso, A.; Carrozzo, A.; Rociola, R. Minimally invasive heart valve surgery: Influence on coagulation and inflammatory response. Interact. Cardiovasc. Thorac. Surg. 2017, 25, 225–232. [Google Scholar] [CrossRef]
- Abawi, M.; Pagnesi, M.; Agostoni, P.; Chiarito, M.; van Jaarsveld, R.C.; van Dongen, C.S.; Slooter, A.J.C.; Colombo, A.; Kooistra, N.H.M.; Doevendans, P.A.F.M.; et al. Postoperative delirium in individuals undergoing transcatheter aortic valve replacement: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2018, 66, 2417–2424. [Google Scholar] [CrossRef]
- Hoogma, D.F.; Venmans, E.; Al Tmimi, L.; Tournoy, J.; Verbrugghe, P.; Jacobs, S.; Fieuws, S.; Milisen, K.; Adriaenssens, T.; Dubois, C.; et al. Postoperative delirium and quality of life after transcatheter and surgical aortic valve replacement: A prospective observational study. J. Thorac. Cardiovasc. Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Shehata, N.; Mistry, N.; Da Costa, B.R.; Pereira, T.V.; Whitlock, R.; Curley, G.F.; Scott, D.A.; Hare, G.M.T.; Jüni, P.; Mazer, C.D. Restrictive compared with liberal red cell transfusion strategies in cardiac surgery: A meta-analysis. Eur. Heart J. 2019, 40, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.N.; Avlonitis, V.S.; Jones, H.E.; Reeves, B.C.; Sterne, J.A.C.; Murphy, G.J. Indications for red blood cell transfusion in cardiac surgery: A systematic review and meta-analysis. Lancet Haematol. 2015, 2, e543–e553. [Google Scholar] [CrossRef] [Green Version]
- Czok, M.; Pluta, M.P.; Putowski, Z.; Krzych, Ł.J. Postoperative neurocognitive disorders in cardiac surgery: Investigating the role of intraoperative hypotension. A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 786. [Google Scholar] [CrossRef]
- Tachibana, M.; Inada, T.; Ichida, M.; Ozaki, N. Factors affecting hallucinations in patients with delirium. Sci. Rep. 2021, 11, 13005. [Google Scholar] [CrossRef]
- Dziadzko, V.; Dziadzko, M.A.; Johnson, M.M.; Gajic, O.; Karnatovskaia, L.V. Acute psychological trauma in the critically ill: Patient and family perspectives. Gen. Hosp. Psychiatry 2017, 47, 68–74. [Google Scholar] [CrossRef]
- Inoue, S.; Hatakeyama, J.; Kondo, Y.; Hifumi, T.; Sakuramoto, H.; Kawasaki, T.; Taito, S.; Nakamura, K.; Unoki, T.; Kawai, Y.; et al. Post-intensive care syndrome: Its pathophysiology, prevention, and future directions. Acute Med. Surg. 2019, 6, 233–246. [Google Scholar] [CrossRef] [Green Version]
- Sommer, I.E.; Kleijer, H.; Hugdahl, K. Toward personalized treatment of hallucinations. Curr. Opin. Psychiatry 2018, 31, 237–245. [Google Scholar] [CrossRef]
- Palanca, B.J.A.; Wildes, T.S.; Ju, Y.S.; Ching, S.; Avidan, M.S. Electroencephalography and delirium in the postoperative period. Br. J. Anaesth. 2017, 119, 294–307. [Google Scholar] [CrossRef] [Green Version]
- Pagnesi, M.; Martino, E.A.; Chiarito, M.; Mangieri, A.; Jabbour, R.J.; van Mieghem, N.M.; Kodali, S.K.; Godino, C.; Landoni, G.; Colombo, A.; et al. Silent cerebral injury after transcatheter aortic valve implantation and the preventive role of embolic protection devices: A systematic review and meta-analysis. Int. J. Cardiol. 2016, 221, 97–106. [Google Scholar] [CrossRef]
- Shaw, R.; Drozdowska, B.; Taylor-Rowan, M.; Elliott, E.; Cuthbertson, G.; Stott, D.J.; Quinn, T.J. Delirium in an acute stroke setting, occurrence, and risk factors. Stroke 2019, 50, 3265–3268. [Google Scholar] [CrossRef] [PubMed]
- van Norden, J.; Spies, C.D.; Borchers, F.; Mertens, M.; Kurth, J.; Heidgen, J.; Pohrt, A.; Mueller, A. The effect of peri-operative dexmedetomidine on the incidence of postoperative delirium in cardiac and non-cardiac surgical patients: A randomised, double-blind placebo-controlled trial. Anaesthesia 2021, 76, 1342–1351. [Google Scholar] [CrossRef] [PubMed]


| Total Cohort (n = 297 pat.) | Neurological Complications (n = 130 pat.) | No Neurological Complications (n = 167 pat.) | p-Value | |
|---|---|---|---|---|
| Sex | 0.446 | |||
| female | 110 (37%) | 45(34.6%) | 65 (38.9%) | |
| male | 187 (63%) | 85 (65.4%) | 102 (61.1%) | |
| Age [years], median (IQR) | 74 (64–80) | 76 (69.75–80.25) | 71 (62–79) | 0.001 + |
| BMI [kg/m²], mean (SD) | 27.48 (5.23) | 27.182 (4.25) | 27.71 (5.76) | 0.643 + |
| DM | 79 (26.6%) | 44 (33.8%) | 35 (21%) | 0.017 |
| CHD | 262 (88.6%) | 122 (93.8%) | 140 (83.8%) | 0.008 |
| HF | 170 (57.2%) | 86 (66.2%) | 84 (50.3%) | 0.006 |
| aHTN | 68 (22.9%) | 34 (26.2%) | 34 (20.4%) | 0.238 |
| Obesity | 74 (24.92%) | 32 (24.6%) | 42 (25.1%) | 0.916 |
| History of MI | 46 (15.5) | 26 (20%) | 20 (12%) | 0.058 |
| History of AF | 85 (28.62%) | 38 (29.2%) | 47 (28.1%) | 0.837 |
| History of chronic alcoholism | 26 (8.75%) | 11 (8.5%) | 15 (9%) | 0.875 |
| History of neurotrauma | 105 (35.35%) | 43 (33.1%) | 62 (37.1%) | 0.469 |
| History of AIS | 32 (10.8%) | 18 (13.8%) | 14 (8.4%) | 0.132 |
| History of delirium | 21 (7.1%) | 14 (10.8%) | 7 (4.2%) | 0.028 |
| History of surgery < 6 months | 20 (6.73%) | 11 (8.5%) | 9 (5.4%) | 0.295 |
| History of depression | 21 (7.07%) | 9 (6.9%) | 12 (7.2%) | 0.930 |
| History of malignoma > 2 years | 35 (11.78%) | 19 (14.6%) | 16 (9.6%) | 0.182 |
| MoCA severity range preoperative, median (IQR) | 2 (1–2) | 2 (2–2) | 2 (1–2) | <0.001 * |
| PHQ-2, median (IQR) | 0 (0–1) | 0 (0–1) | 0 (0–1) | 0.121 * |
| MST, median (IQR) | 0 (0–1) | 0 (0–1) | 0 (0–1) | 0.365 * |
| ASA-classification, median (IQR) | 3 (3–3) | 3 (3-3) | 3 (3–3) | 0.472 * |
| Pre-medication sedatives or benzodiazepines | 10 (3.37%) | 5 (3.8%) | 5 (3%) | 0.753 |
| Stay in hospital in days, median (IQR) | 8 (7–11) | 9 (7–12) | 8 (7–10) | 0.012 + |
| Total Cohort (n = 297 pat.) | Neurological Complications (n = 130 pat.) | No Neurological Complications (n = 167 pat.) | p-Value | |
|---|---|---|---|---|
| Percutaneous valve replacement | 61 (20.5%) | 22 (16.9%) | 39 (23.4%) | 0.174 |
| Cardiac surgery | 236 (79.5%) | 108 (83.1%) | 128 (76.6%) | |
| Premedication midazolam | 77 (25.9%) | 30 (23.1%) | 47 (28.1%) | 0.323 |
| Premedication midazolam standardized, 7.5 mg 3.5 mg | 35 (11.8%) 44 (14.8%) | 12 (9.2%) 20 (15.4%) | 23 (13.8%) 24 (14.4%) | 0.483 |
| Duration of surgery [minutes], median (IQR) | 189 (135.5–239) | 199 (157.75–248.5) | 182 (111–223) | 0.006 + |
| Cardio-pulmonary-bypass time [minutes], mean (SD) 1 | 116.62 (47.985) | 123.69 (51.55) | 110.8 (44.23) | 0.035 + |
| Aorta clamping time, mean (SD) 2 | 68.92 (31.68) | 71.84 (32.55) | 66.46 (30.86) | 0.186 + |
| MAP under 60 mmHg | 260 (87.5%) | 121 (93.1%) | 139 (83.2%) | 0.011 |
| MAP minimum [mmHg], mean (SD) | 34.75 (13.42) | 32.32 (11.95) | 36.64 (14.21) | 0.016 + |
| MAP mean, mean (SD) | 71.84 (11.21) | 71.10 (9.53) | 72.44 (12.36) | 0.408 + |
| MAP variance [mmHg], mean (SD) | 190.90 (93.42) | 203.86 (99.35) | 180.82 (87.50) | 0.027 + |
| Administration of glucocorticoids | 11 (3.7%) | 3 (2.3%) | 8 (4.8%) | 0.358 * |
| Medication of vasopressor | 179 (60.3%) | 81 (62.3%) | 98 (58.7%) | 0.526 |
| Medication of inotropica | 58 (19.5%) | 31 (23.8%) | 27 (16.2%) | 0.098 |
| Number of RBC transfusion (intraop.), median (IQR) | 0 (0–2) | 0 (0–2) | 0 (0–0) | <0.001 + |
| Administration of FFP (intraop.) | 14 (4.7%) | 9 (6.9%) | 5 (3%) | 0.113 |
| Administration of thrombocyte concentrate (intraoperative) | 30 (10.1%) | 18 (13.8%) | 12 (7.2%) | 0.059 |
| Revisional surgery | 15 (5.1%) | 8 (6.2%) | 7 (4.2%) | 0.444 |
| Number of RBC transfusions (total), median (IQR) | 2 (0–4) | 3 (0.75–6) | 0 (0–3) | 0.028 + |
| Administration of FFP (total) | 45 (15.2%) | 27 (20.8%) | 18 (10.8%) | 0.017 |
| Administration of thrombocyte concentrate (total) | 68 (22.9%) | 38 (29.2%) | 30 (18%) | 0.022 + |
| Neuroleptics postoperative | 15 (5.05%) | 13 (10%) | 2 (1.2%) | 0.001 |
| Opioids postoperative | 250 (84.17%) | 114 (87.7%) | 136 (81.4%) | 0.143 |
| Sedatives postoperative | 228 (76.8%) | 107 (82.3%) | 121 (72.5%) | 0.046 |
| AF postoperative | 64 (21.55%) | 32 (24.6%) | 32 (19.2%) | 0.257 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teller, J.; Gabriel, M.M.; Schimmelpfennig, S.-D.; Laser, H.; Lichtinghagen, R.; Schäfer, A.; Fegbeutel, C.; Weissenborn, K.; Jung, C.; Hinken, L.; et al. Stroke, Seizures, Hallucinations and Postoperative Delirium as Neurological Complications after Cardiac Surgery and Percutaneous Valve Replacement. J. Cardiovasc. Dev. Dis. 2022, 9, 365. https://doi.org/10.3390/jcdd9110365
Teller J, Gabriel MM, Schimmelpfennig S-D, Laser H, Lichtinghagen R, Schäfer A, Fegbeutel C, Weissenborn K, Jung C, Hinken L, et al. Stroke, Seizures, Hallucinations and Postoperative Delirium as Neurological Complications after Cardiac Surgery and Percutaneous Valve Replacement. Journal of Cardiovascular Development and Disease. 2022; 9(11):365. https://doi.org/10.3390/jcdd9110365
Chicago/Turabian StyleTeller, Johannes, Maria Magdalena Gabriel, Svea-Dorothee Schimmelpfennig, Hans Laser, Ralf Lichtinghagen, Andreas Schäfer, Christine Fegbeutel, Karin Weissenborn, Carolin Jung, Lukas Hinken, and et al. 2022. "Stroke, Seizures, Hallucinations and Postoperative Delirium as Neurological Complications after Cardiac Surgery and Percutaneous Valve Replacement" Journal of Cardiovascular Development and Disease 9, no. 11: 365. https://doi.org/10.3390/jcdd9110365