
Life-Space Activities Are Associated with the Prognosis of Older Adults with Cardiovascular Disease
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Clinical Characteristics
2.3. LSA
2.4. Measurements
2.4.1. CPX
2.4.2. SPPB
2.4.3. GDS
2.4.4. MMSE
2.5. Cardiovascular Events
2.6. Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristics
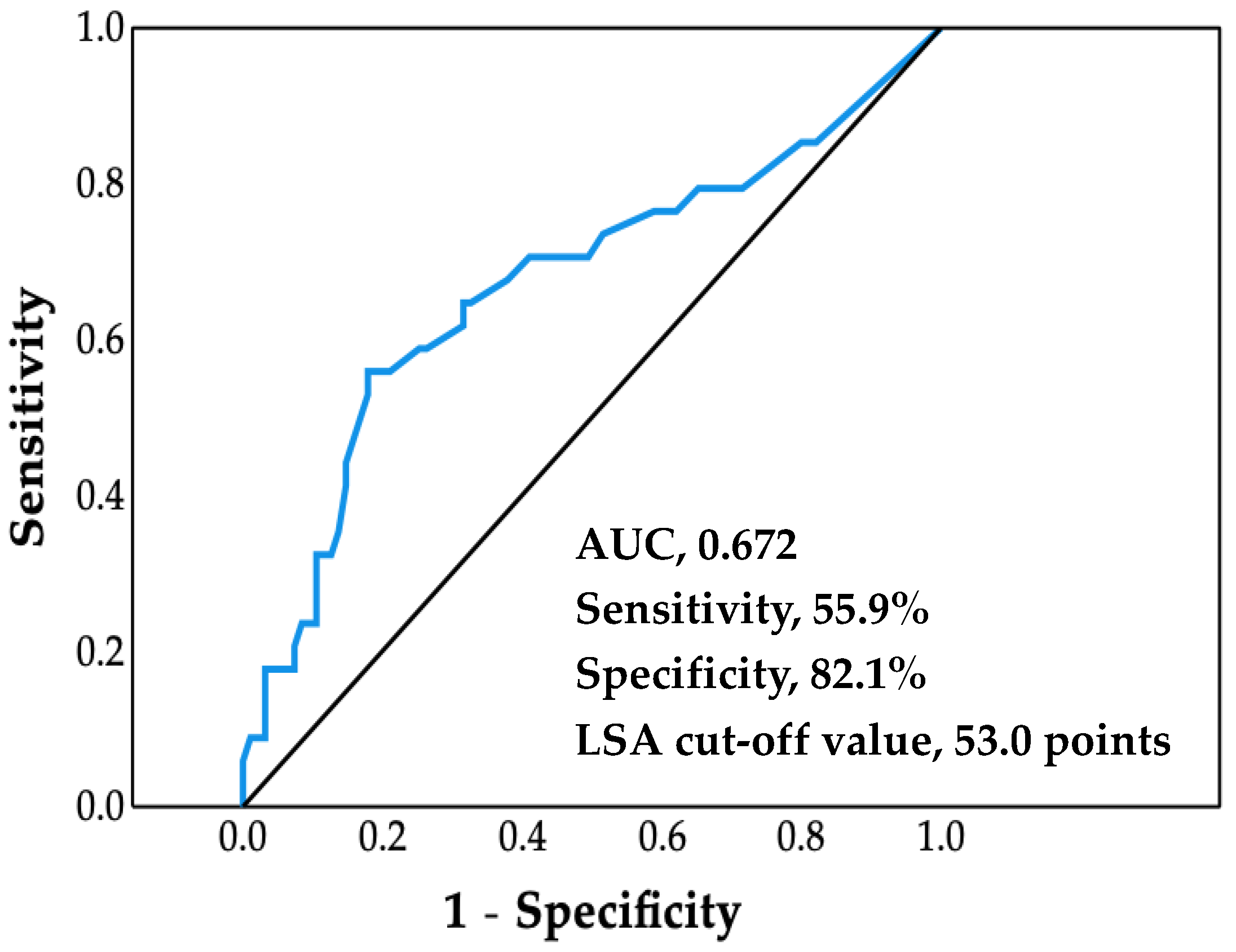
3.2. ROC Analysis
3.3. Comparison of Baseline Clinical Characteristics between LSA Groups
3.4. Survival Time Analysis
3.5. Cox Proportional Hazards Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministry of Health, L.A.W. Statistics and Information Department. Vital Statistics. Available online: https://www.mhlw.go.jp/toukei/list/10-20.html (accessed on 15 February 2022).
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics-2022 Update: A Report From the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef]
- Chung, K.; Wilkinson, C.; Veerasamy, M.; Kunadian, V. Frailty Scores and Their Utility in Older Patients with Cardiovascular Disease. Interv. Cardiol. 2021, 16, e05. [Google Scholar] [CrossRef]
- Bekfani, T.; Pellicori, P.; Morris, D.A.; Ebner, N.; Valentova, M.; Steinbeck, L.; Wachter, R.; Elsner, S.; Sliziuk, V.; Schefold, J.C.; et al. Sarcopenia in patients with heart failure with preserved ejection fraction: Impact on muscle strength, exercise capacity and quality of life. Int. J. Cardiol. 2016, 222, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Ullrich, P.; Werner, C.; Abel, B.; Hummel, M.; Bauer, J.M.; Hauer, K. Assessing life-space mobility: A systematic review of questionnaires and their psychometric properties. Z. Gerontol. Geriatr. 2022. [Google Scholar] [CrossRef]
- Johnson, J.; Rodriguez, M.A.; Al Snih, S. Life-Space Mobility in the Elderly: Current Perspectives. Clin. Interv. Aging 2020, 15, 1665–1674. [Google Scholar] [CrossRef] [PubMed]
- Baker, P.S.; Bodner, E.V.; Allman, R.M. Measuring life-space mobility in community-dwelling older adults. J. Am. Geriatr. Soc. 2003, 51, 1610–1614. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.K.; Buchan, I.E.; van der Veer, S.N. Assessing life-space mobility for a more holistic view on wellbeing in geriatric research and clinical practice. Aging Clin. Exp. Res. 2019, 31, 439–445. [Google Scholar] [CrossRef]
- Iyer, A.S.; Wells, J.M.; Bhatt, S.P.; Kirkpatrick, D.P.; Sawyer, P.; Brown, C.J.; Allman, R.M.; Bakitas, M.A.; Dransfield, M.T. Life-Space mobility and clinical outcomes in COPD. Int. J. Chronic Obstr. Pulmon. Dis. 2018, 13, 2731–2738. [Google Scholar] [CrossRef]
- Lo, A.X.; Flood, K.L.; Kennedy, R.E.; Bittner, V.; Sawyer, P.; Allman, R.M.; Brown, C.J. The Association Between Life-Space and Health Care Utilization in Older Adults with Heart Failure. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 1442–1447. [Google Scholar] [CrossRef]
- Weintraub, R.G.; Semsarian, C.; Macdonald, P. Dilated cardiomyopathy. Lancet 2017, 390, 400–414. [Google Scholar] [CrossRef]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Guyton, R.A.; O’Gara, P.T.; Ruiz, C.E.; Skubas, N.J.; Sorajja, P.; et al. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, e521–e643. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, B.; Coats, A.J.S.; Tsutsui, H.; Abdelhamid, C.M.; Adamopoulos, S.; Albert, N.; Anker, S.D.; Atherton, J.; Bohm, M.; Butler, J.; et al. Universal definition and classification of heart failure: A report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur. J. Heart Fail. 2021, 23, 352–380. [Google Scholar] [CrossRef] [PubMed]
- Satake, S.; Arai, H. The revised Japanese version of the Cardiovascular Health Study criteria (revised J-CHS criteria). Geriatr. Gerontol. Int. 2020, 20, 992–993. [Google Scholar] [CrossRef] [PubMed]
- Peel, C.; Sawyer Baker, P.; Roth, D.L.; Brown, C.J.; Brodner, E.V.; Allman, R.M. Assessing mobility in older adults: The UAB Study of Aging Life-Space Assessment. Phys. Ther. 2005, 85, 1008–1119. [Google Scholar] [CrossRef]
- Ross, R.M. ATS/ACCP statement on cardiopulmonary exercise testing. Am. J. Respir. Crit. Care Med. 2003, 167, 1451, Author reply 1451. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Mijnarends, D.M.; Meijers, J.M.; Halfens, R.J.; ter Borg, S.; Luiking, Y.C.; Verlaan, S.; Schoberer, D.; Cruz Jentoft, A.J.; van Loon, L.J.; Schols, J.M. Validity and reliability of tools to measure muscle mass, strength, and physical performance in community-dwelling older people: A systematic review. J. Am. Med. Dir. Assoc. 2013, 14, 170–178. [Google Scholar] [CrossRef]
- Sugishita, K.; Sugishita, M.; Hemmi, I.; Asada, T.; Tanigawa, T. A Validity and Reliability Study of the Japanese Version of the Geriatric Depression Scale 15 (GDS-15-J). Clin. Gerontol. 2017, 40, 233–240. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Portegijs, E.; Rantakokko, M.; Viljanen, A.; Sipila, S.; Rantanen, T. Identification of Older People at Risk of ADL Disability Using the Life-Space Assessment: A Longitudinal Cohort Study. J. Am. Med. Dir. Assoc. 2016, 17, 410–414. [Google Scholar] [CrossRef] [Green Version]
- Shimada, H.; Sawyer, P.; Harada, K.; Kaneya, S.; Nihei, K.; Asakawa, Y.; Yoshii, C.; Hagiwara, A.; Furuna, T.; Ishizaki, T. Predictive validity of the classification schema for functional mobility tests in instrumental activities of daily living decline among older adults. Arch. Phys. Med. Rehabil. 2010, 91, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Silberschmidt, S.; Kumar, A.; Raji, M.M.; Markides, K.; Ottenbacher, K.J.; Al Snih, S. Life-Space Mobility and Cognitive Decline Among Mexican Americans Aged 75 Years and Older. J. Am. Geriatr. Soc. 2017, 65, 1514–1520. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, K.; Hirashiki, A.; Kawamura, K.; Sugioka, J.; Mizuno, Y.; Tanioku, S.; Sato, K.; Ueda, I.; Itoh, N.; Nomoto, K.; et al. Short physical performance battery score and driving a car are independent factors associated with life-space activities in older adults with cardiovascular disease. Geriatr. Gerontol. Int. 2021, 21, 900–906. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [CrossRef]
- Sato, T.; Yamauchi, H.; Kanno, Y.; Suzuki, S.; Yoshihisa, A.; Yamaki, T.; Sugimoto, K.; Kunii, H.; Nakazato, K.; Suzuki, H.; et al. Comparisons of prognostic factors between young and elderly patients with chronic heart failure. Geriatr. Gerontol. Int. 2015, 15, 435–442. [Google Scholar] [CrossRef]
- Portegijs, E.; Tsai, L.T.; Rantanen, T.; Rantakokko, M. Moving through Life-Space Areas and Objectively Measured Physical Activity of Older People. PLoS ONE 2015, 10, e0135308. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Age (years) | 79.2 ± 7.6 |
| Sex (male, n (%)) | 60 (46.5) |
| Body mass index (kg/m2) | 22.3 ± 3.9 |
| Underlying diseases | |
| Worsening heart failure (n, %) | 113 (87.7) |
| Non-ischemic cardiomyopathy (n, %) | 8 (6.2) |
| Ischemic heart disease (n, %) | 31 (24.0) |
| Tachycardia-induced (n, %) | 34 (26.4) |
| Bradycardia (n, %) | 10 (7.8) |
| Valve (n, %) | 14 (10.9) |
| Hypertension (n, %) | 10 (7.8) |
| Other (n, %) | 6 (4.6) |
| Post PCI or CABG (n, %) | 16 (12.3) |
| Medication | |
| Diuretic (n, %) | 61 (47.3) |
| Tolvaptan (n, %) | 17 (13.2) |
| ACE-I/ARB (n, %) | 55 (42.6) |
| β blocker (n, %) | 59 (45.7) |
| Spironolactone (n, %) | 26 (20.2) |
| Anticoagulant (n, %) | 55 (42.6) |
| Antiplatelet (n, %) | 59 (45.7) |
| Laboratory data | |
| BNP (pg/mL) | 163.8 ± 157.2 |
| Hemoglobin (mg/dL) | 12.5 ± 1.8 |
| Total protein (g/dL) | 6.8 ± 0.6 |
| Albumin (d/dL) | 3.8 ± 0.5 |
| Total cholesterol (mg/dL) | 172.8 ± 34.6 |
| eGFR (mL/min/1.73 m2) | 56.0 ± 18.5 |
| Echocardiography | |
| LVEF (%) | 56.7 ± 13.2 |
| E/e′ | 15.6 ± 6.6 |
| Frailty | |
| J-CHS (robust/prefrailty/frailty) (%) | 4.4/54.4/41.2 |
| Other status | |
| LSA (points) | 74.1 ± 32.5 |
| Peak VO2 (mL/min/kg) | 13.1 ± 3.4 |
| SPPB (points) | 9.4 ± 2.8 |
| GDS (points) | 4.0 ± 3.2 |
| MMSE (points) | 27.0 ± 2.9 |
| Cardiovascular events | |
| Cardiovascular hospitalization (n, %) | 36 (27.9) |
| Cardiovascular death (n, %) | 11 (8.5) |
| Low LSA Group (n = 36) | High LSA Group (n = 93) | p Value | |
|---|---|---|---|
| LSA (points) | 32.3 ± 15.5 | 90.3 ± 20.8 | <0.001 |
| Age (years) | 84.4 ± 6.4 | 77.4 ± 6.7 | <0.001 |
| Male (n, %) | 20 (56) | 40 (43) | 0.166 |
| Underlying diseases | |||
| Worsening heart failure (n, %) | 35 (94.4) | 65 (85.0) | 0.142 |
| Non-ischemic cardiomyopathy (n, %) | 3 (8.3) | 5 (5.4) | |
| Ischemic heart disease (n, %) | 6 (16.7) | 25 (26.9) | |
| Tachycardia-induced (n, %) | 7 (19.3) | 27 (29.0) | |
| Bradycardia (n, %) | 6 (16.7) | 4 (4.3) | |
| Valve (n, %) | 6 (16.7) | 8 (8.6) | |
| Hypertension (n, %) | 4 (11.1) | 6 (6.5) | |
| Other (n, %) | 2 (5.6) | 4 (4.3) | |
| Post PCI or CABG (n, %) | 2 (5.6) | 14 (15.0) | |
| Medication | |||
| Diuretic (n, %) | 22 (61.1) | 39 (41.9) | 0.051 |
| Tolvaptan (n, %) | 6 (16.7) | 11 (11.8) | 0.466 |
| ACE-I/ARB (n, %) | 14 (38.9) | 41 (44.1) | 0.592 |
| β blocker (n, %) | 12 (33.3) | 47 (50.5) | 0.079 |
| Spironolactone (n, %) | 8 (22.2) | 18 (19.4) | 0.716 |
| Anticoagulant (n, %) | 14 (38.9) | 41 (44.1) | 0.592 |
| Antiplatelet (n, %) | 12 (33.3) | 47 (50.5) | 0.079 |
| BNP (pg/mL) | 199.3 ± 139.7 | 139.2 ± 142.1 | 0.035 |
| LVEF (%) | 58.1 ± 13.4 | 56.9 ± 12.5 | 0.644 |
| Peak VO2 (mL/min/kg) | 11.3 ± 3.0 | 13.9 ± 3.4 | 0.001 |
| SPPB (points) | 6.8 ± 3.2 | 10.3 ± 2.0 | <0.001 |
| GDS (points) | 6.1 ± 3.1 | 3.3 ± 2.9 | <0.001 |
| MMSE (points) | 25.3 ± 3.2 | 27.6 ± 2.6 | <0.001 |
| Cardiovascular hospitalization (n, %) | 19 (52.8) | 17 (17.0) | <0.001 |
| Cardiovascular death (n, %) | 8 (22.2) | 3 (3.0) | 0.012 |
| Model 1 | Model 2 | Model 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | HR | 95% CI | p Value | |
| LSA | |||||||||
| ≥53 points | Reference | Reference | Reference | ||||||
| <53 points | 3.717 | 1.928–7.164 | <0.001 | 2.420 | 1.156–5.069 | 0.019 | 2.515 | 1.154–5.482 | 0.020 |
| Age | 1.064 | 1.013–1.117 | 0.013 | 1.039 | 0.989–1.092 | 0.126 | |||
| Sex | 0.901 | 0.461–1.760 | 0.760 | 0.921 | 0.467–1.816 | 0.812 | |||
| LVEF | 0.989 | 0.996–1.013 | 0.367 | ||||||
| Log BNP | 2.639 | 1.129–6.166 | 0.025 | ||||||
| Model 1 | Model 2 | Model 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | HR | 95% CI | p Value | |
| LSA | |||||||||
| ≥53 points | Reference | Reference | Reference | ||||||
| <53 points | 11.27 | 2.392–53.081 | 0.002 | 4.791 | 1.119–20.502 | 0.035 | 8.192 | 1.507–44.541 | 0.015 |
| Age | 1.090 | 0.995–1.194 | 0.065 | 1.052 | 0.948–1.167 | 0.337 | |||
| Sex | 1.129 | 0.327–3.902 | 0.847 | 1.315 | 0.353–4.902 | 0.683 | |||
| LVEF | 0.989 | 0.946–1.034 | 0.626 | ||||||
| Log BNP | 2.006 | 0.379–10.613 | 0.413 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hashimoto, K.; Hirashiki, A.; Oya, K.; Sugioka, J.; Tanioku, S.; Sato, K.; Ueda, I.; Itoh, N.; Kokubo, M.; Shimizu, A.; et al. Life-Space Activities Are Associated with the Prognosis of Older Adults with Cardiovascular Disease. J. Cardiovasc. Dev. Dis. 2022, 9, 323. https://doi.org/10.3390/jcdd9100323
Hashimoto K, Hirashiki A, Oya K, Sugioka J, Tanioku S, Sato K, Ueda I, Itoh N, Kokubo M, Shimizu A, et al. Life-Space Activities Are Associated with the Prognosis of Older Adults with Cardiovascular Disease. Journal of Cardiovascular Development and Disease. 2022; 9(10):323. https://doi.org/10.3390/jcdd9100323
Chicago/Turabian StyleHashimoto, Kakeru, Akihiro Hirashiki, Koharu Oya, Junpei Sugioka, Shunya Tanioku, Kenji Sato, Ikue Ueda, Naoki Itoh, Manabu Kokubo, Atsuya Shimizu, and et al. 2022. "Life-Space Activities Are Associated with the Prognosis of Older Adults with Cardiovascular Disease" Journal of Cardiovascular Development and Disease 9, no. 10: 323. https://doi.org/10.3390/jcdd9100323