

Lipoprotein a Combined with Fibrinogen as an Independent Predictor of Long-Term Prognosis in Patients with Acute Coronary Syndrome: A Multi-Center Retrospective Study
Abstract
:1. Introduction
2. Materials and Methods
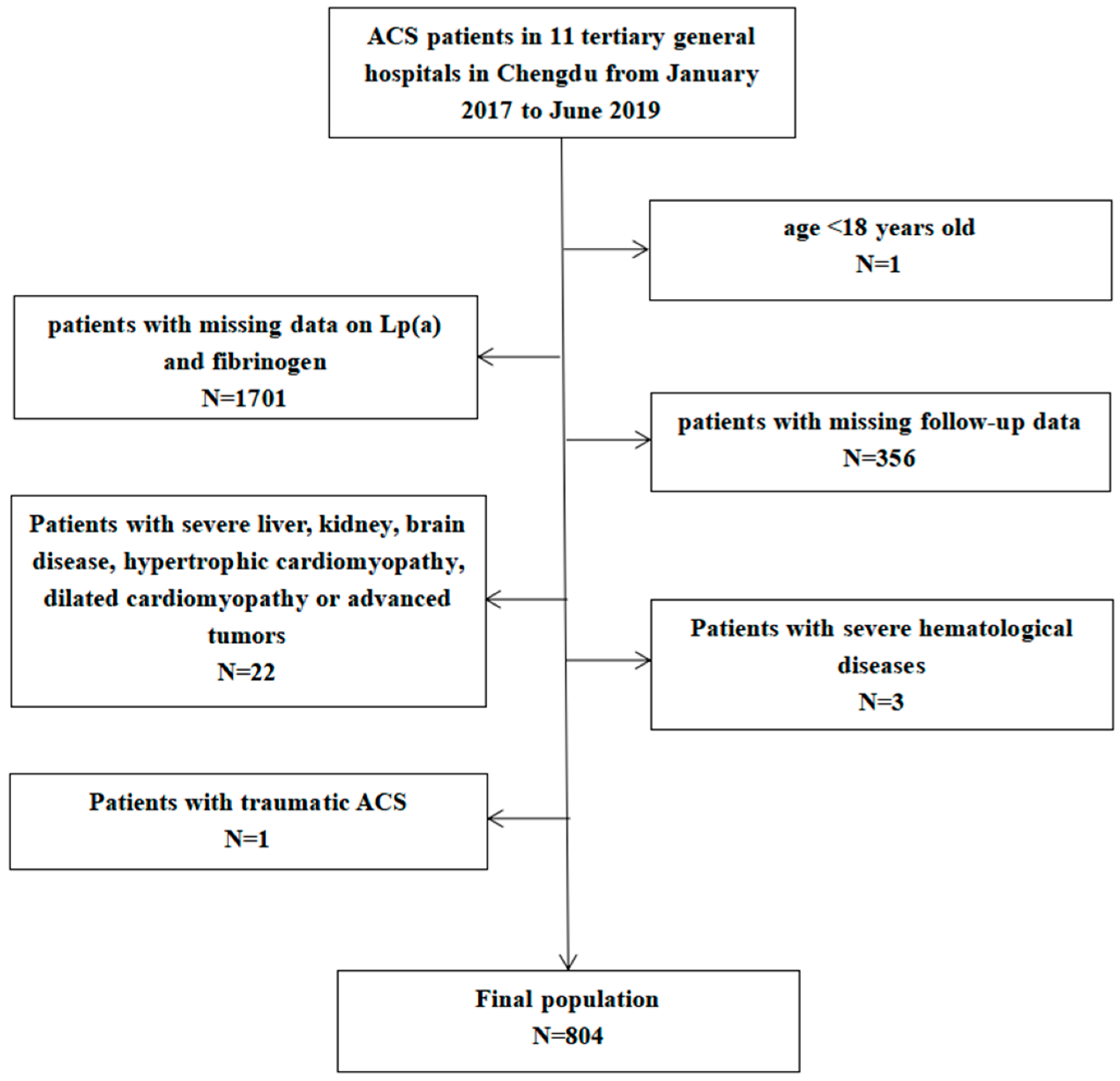
2.1. Study Population
2.2. Definitions
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
3.2. Comparison of Cumulative Incidence of MACCE
3.2.1. Comparison of the Cumulative Incidence of MACCE between Non-High-Lp(a) Group and High-Lp(a) Group
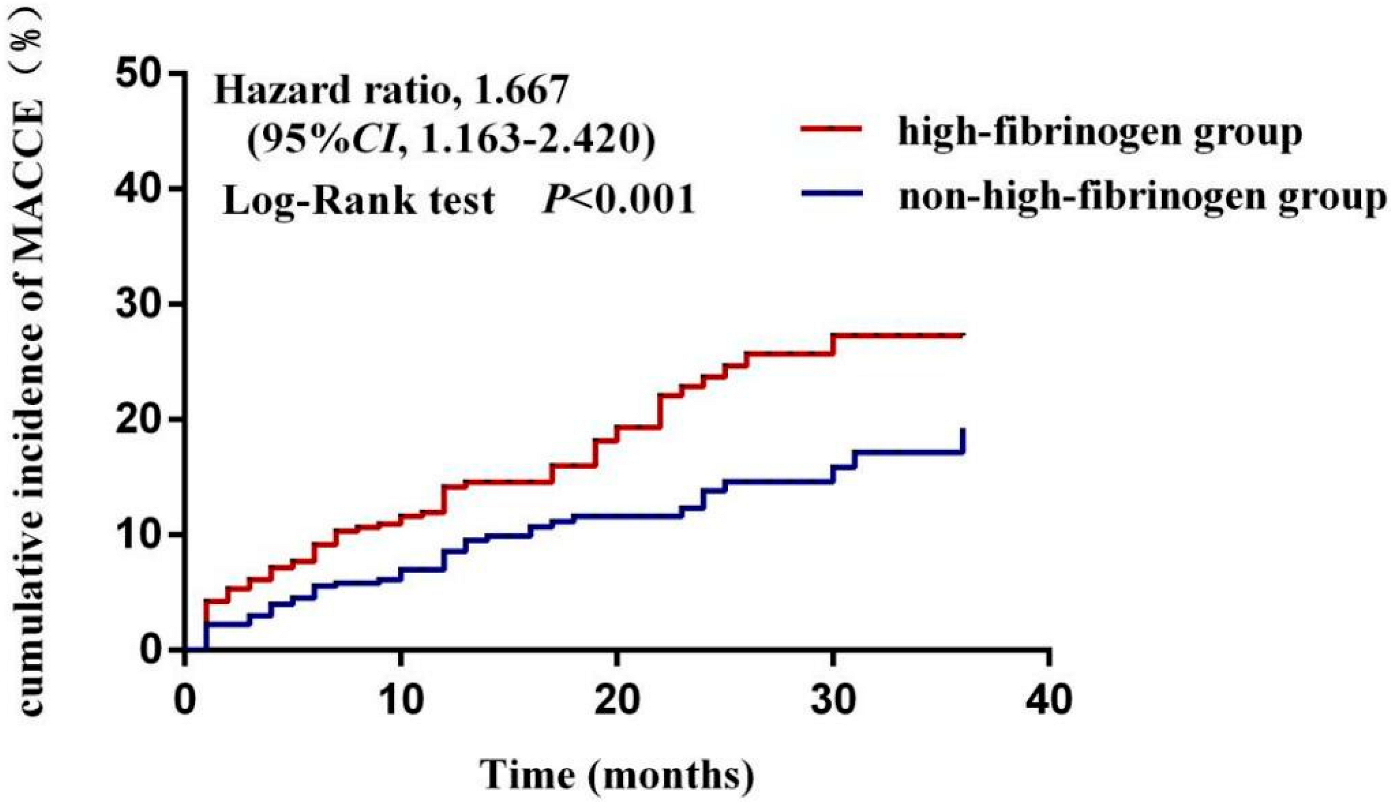
3.2.2. Comparison of the Cumulative Incidence of MACCE between Non-High-Fibrinogen Group and High-Fibrinogen Group
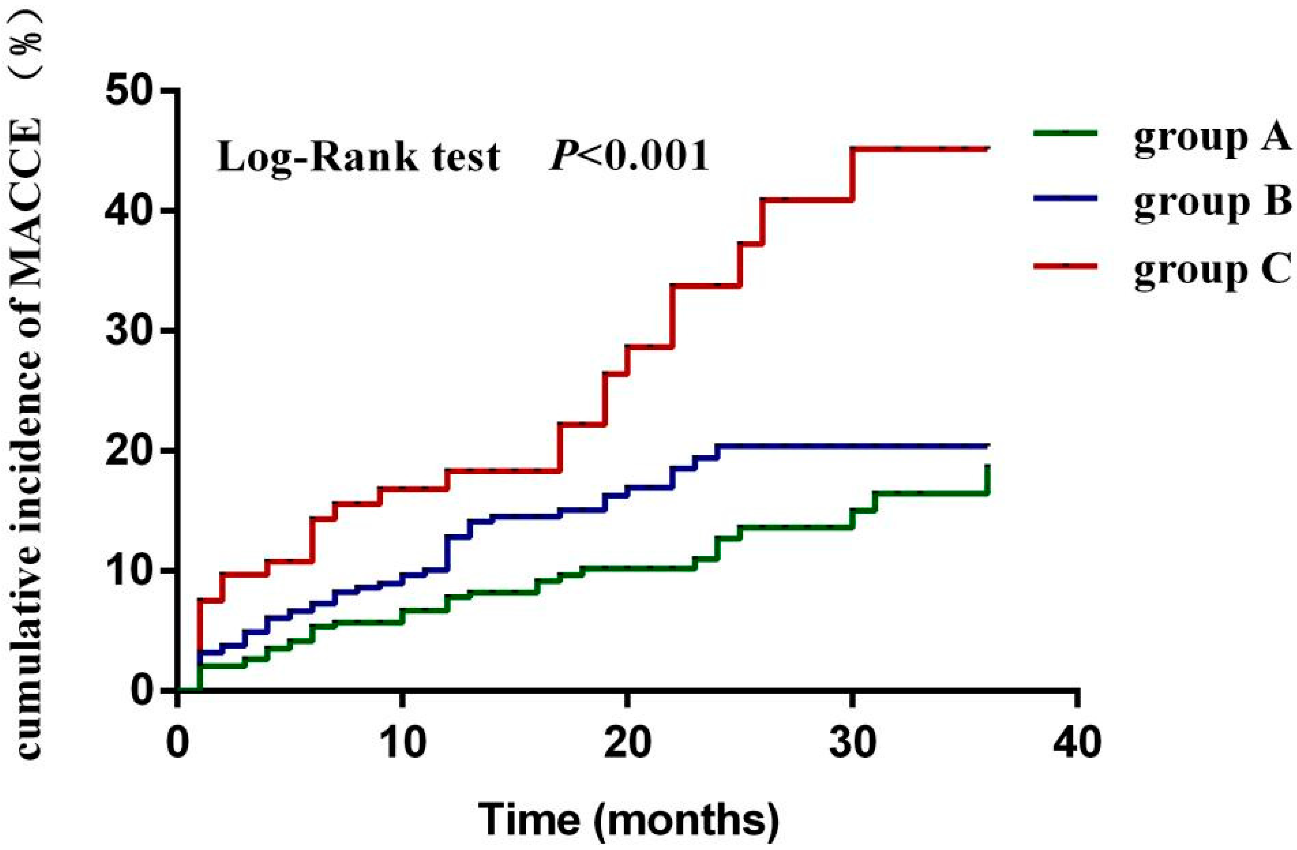
3.2.3. Comparison of the Cumulative MACCE Incidence between Groups of Lp(a) Combined with Fibrinogen
3.3. Multivariate Cox Regression Analysis of MACCE in Patients with ACS
3.4. The Construction of MACCE Risk Forecast Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Corbett, S.J.; Ftouh, S.; Lewis, S.; Lovibond, K.; Guideline Committee. Acute coronary syndromes: Summary of updated NICE guidance. BMJ 2021, 15, 372. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Kochar, A.; Chen, A.Y.; Sharma, P.P.; Pagidipati, N.J.; Fonarow, G.C.; Cowper, P.A.; Roe, M.T.; Peterson, E.D.; Wang, T.Y. Long-Term Mortality of Older Patients with Acute Myocardial Infarction Treated in US Clinical Practice. J. Am. Heart Assoc. 2018, 13, e007230. [Google Scholar] [CrossRef] [PubMed]
- LaMori, J.C.; Shoheiber, O.; Dudash, K.; Crivera, C.; Mody, S.H. The economic impact of acute coronary syndrome on length of stay: An analysis using the Healthcare Cost and Utilization Project (HCUP) databases. J. Med Econ. 2014, 17, 191–197. [Google Scholar] [CrossRef]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Zhang, Y.-M.; Cheng, L.-C.; Zhou, M.-G.; Chen, Y.-Z.; Zhu, F.; Cui, C.-Y.; Li, S.-Y.; Cai, L. Effect of regional cooperative rescue systems based on chest pain centers for patients with acute myocardial infarction in a first-tier city in China. Intern. Emerg. Med. 2021, 16, 2069–2076. [Google Scholar] [CrossRef] [PubMed]
- Enezate, T.H.; Omran, J.; Al-Dadah, A.S.; Alpert, M.; Mahmud, E.; Patel, M.; Aronow, H.D.; Bhatt, D.L. Comparison of Outcomes of ST-Elevation Myocardial Infarction Treated by Percutaneous Coronary Intervention During Off-Hours Versus On-Hours. Am. J. Cardiol. 2017, 120, 1742–1754. [Google Scholar] [CrossRef]
- Gencer, B.; Kronenberg, F.; Stroes, E.S.; Mach, F. Lipoprotein(a): The revenant. Eur. Heart J. 2017, 38, 1553–1560. [Google Scholar] [CrossRef]
- Ruscica, M.; Sirtori, C.R.; Corsini, A.; Watts, G.F.; Sahebkar, A. Lipoprotein(a): Knowns, unknowns and uncertainties. Pharmacol. Res. 2021, 173, 105812. [Google Scholar] [CrossRef]
- Boffa, M.B.; Koschinsky, M. Oxidized phospholipids as a unifying theory for lipoprotein(a) and cardiovascular disease. Nat. Rev. Cardiol. 2019, 16, 305–318. [Google Scholar] [CrossRef]
- Sugimoto, M.A.; Ribeiro, A.L.C.; Costa, B.R.C.; Vago, J.P.; Lima, K.M.; Carneiro, F.S.; Ortiz, M.M.O.; Lima, G.L.N.; Carmo, A.A.F.; Rocha, R.M.; et al. Plasmin and plasminogen induce macrophage reprogramming and regulate key steps of inflammation resolution via annexin A1. Blood 2017, 129, 2896–2907. [Google Scholar] [CrossRef]
- Soma, P.; Pretorius, E. Interplay between ultrastructural findings and atherothrombotic complications in type 2 diabetes mellitus. Cardiovasc. Diabetol. 2015, 14, 96. [Google Scholar] [CrossRef] [PubMed]
- Willeit, P.; Ridker, P.M.; Nestel, P.J.; Simes, J.; Tonkin, A.M.; Pedersen, T.R.; Schwartz, G.G.; Olsson, A.G.; Colhoun, H.M.; Kronenberg, F.; et al. Baseline and on-statin treatment lipoprotein(a) levels for prediction of cardiovascular events: Individual patient-data meta-analysis of statin outcome trials. Lancet 2018, 392, 1311–1320. [Google Scholar] [CrossRef]
- Hu, Y.; Tao, J.-Y.; Cai, D.-P.; He, Y.-M. Interaction of lipoprotein(a) with low-density lipoprotein cholesterol on first incident acute myocardial infarction. Clin. Chim. Acta 2020, 501, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.-L.; Wu, N.-Q.; Shi, H.-W.; Dong, Q.; Dong, Q.-T.; Gao, Y.; Guo, Y.-L.; Li, J.-J. Fibrinogen is associated with glucose metabolism and cardiovascular outcomes in patients with coronary artery disease. Cardiovasc. Diabetol. 2020, 19, 36. [Google Scholar] [CrossRef]
- Zhang, J.; Du, R.; Peng, K.; Wu, X.; Hu, C.; Li, M.; Xu, Y.; Xu, M.; Wang, S.; Bi, Y.; et al. Serum lipoprotein (a) is associated with increased risk of stroke in Chinese adults: A prospective study. Atherosclerosis 2019, 289, 8–13. [Google Scholar] [CrossRef]
- Anderson, T.J.; Grégoire, J.; Pearson, G.J.; Barry, A.R.; Couture, P.; Dawes, M.; Francis, G.A.; Genest, J., Jr.; Grover, S.; Gupta, M.; et al. 2016 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in the Adult. Can. J. Cardiol. 2016, 32, 1263–1282. [Google Scholar] [CrossRef]
- Liu, H.-H.; Cao, Y.-X.; Jin, J.-L.; Zhang, H.-W.; Hua, Q.; Li, Y.-F.; Guo, Y.-L.; Zhu, C.-G.; Wu, N.-Q.; Gao, Y.; et al. Association of lipoprotein(a) levels with recurrent events in patients with coronary artery disease. Heart 2020, 106, 1228–1235. [Google Scholar] [CrossRef]
- Teo, K.K.; Ounpuu, S.; Hawken, S.; Pandey, M.R.; Valentin, V.; Hunt, D.; Diaz, R.; Rashed, W.; Freeman, R.; Jiang, L.; et al. Tobacco use and risk of myocardial infarction in 52 countries in the INTERHEART study: A case-control study. Lancet 2006, 368, 647–658. [Google Scholar] [CrossRef]
- American Diabetes Association Introduction: Standards of Medical Care in Diabetes—2022. Diabetes Care 2022, 45, S1–S2. [CrossRef]
- Al-Makki, A.; DiPette, D.; Whelton, P.K.; Murad, M.H.; Mustafa, R.A.; Acharya, S.; Beheiry, H.M.; Champagne, B.; Connell, K.; Cooney, M.T.; et al. Hypertension Pharmacological Treatment in Adults: A World Health Organization Guideline Executive Summary. Hypertension 2022, 79, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Cai, A.; Li, L.; Zhang, Y.; Mo, Y.; Li, Z.; Mai, W.; Zhou, Y. Baseline LDL-C and Lp(a) Elevations Portend a High Risk of Coronary Revascularization in Patients after Stent Placement. Dis. Markers 2013, 35, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Khera, A.V.; Everett, B.M.; Caulfield, M.P.; Hantash, F.M.; Wohlgemuth, J.; Ridker, P.M.; Mora, S. Lipoprotein(a) Concentrations, Rosuvastatin Therapy, and Residual Vascular Risk. Circulation 2014, 129, 635–642. [Google Scholar] [CrossRef]
- Gencer, B.; Rigamonti, F.; Nanchen², D.; Vuilleumier, N.; Kern, I.; Aghlmandi, S.; Klingenberg, R.; Räber, L.; Auer, R.; Carballo, D.; et al. Prognostic value of elevated lipoprotein(a) in patients with acute coronary syndromes. Eur. J. Clin. Investig. 2019, 49, e13117. [Google Scholar] [CrossRef]
- da Silva, A.R.; Fraga-Silva, R.A.; Stergiopulos, N.; Montecucco, F.; Mach, F. Update on the role of angiotensin in the pathophysiology of coronary atherothrombosis. Eur. J. Clin. Investig. 2015, 45, 274–287. [Google Scholar] [CrossRef]
- Santulli, G.; Campanile, A.; Spinelli, L.; Assante di Panzillo, E.A.; Ciccarelli, M.; Trimarco, B.; Iaccarino, G. G Protein-Coupled Receptor Kinase 2 in Patients with Acute Myocardial Infarction. Am. J. Cardiol. 2011, 107, 1125–1130. [Google Scholar] [CrossRef] [PubMed]
- Vergallo, R.; Papafaklis, M.I.; Yonetsu, T.; Bourantas, C.V.; Andreou, I.; Wang, Z.; Fujimoto, J.G.; McNulty, I.; Lee, H.; Biasucci, L.M.; et al. Endothelial Shear Stress and Coronary Plaque Characteristics in Humans. Circ. Cardiovasc. Imaging 2014, 7, 905–911. [Google Scholar] [CrossRef]
- Catena, C.; Colussi, G.; Brosolo, G.; A Sechi, L. A Prothrombotic State is Associated with Early Arterial Damage in Hypertensive Patients. J. Atheroscler. Thromb. 2012, 19, 471–478. [Google Scholar] [CrossRef]
- Konstantinou, K.; Tsioufis, C.; Koumelli, A.; Mantzouranis, M.; Kasiakogias, A.; Doumas, M.; Tousoulis, D. Hypertension and patients with acute coronary syndrome: Putting blood pressure levels into perspective. J. Clin. Hypertens. 2019, 21, 1135–1143. [Google Scholar] [CrossRef]
- Burlacu, A.; Genovesi, S.; Ortiz, A.; Kanbay, M.; Rossignol, P.; Banach, M.; Małyszko, J.; Goldsmith, D.; Covic, A. The quest for equilibrium: Exploring the thin red line between bleeding and ischaemic risks in the management of acute coronary syndromes in chronic kidney disease patients. Nephrol. Dial. Transplant. 2017, 32, 1967–1976. [Google Scholar] [CrossRef]
- Uemura, Y.; Ishikawa, S.; Takemoto, K.; Negishi, Y.; Tanaka, A.; Takagi, K.; Yoshioka, N.; Umemoto, N.; Inoue, Y.; Morishima, I.; et al. Clinical outcomes after percutaneous coronary intervention in non-dialysis patients with acute coronary syndrome and advanced renal dysfunction. Clin. Exp. Nephrol. 2020, 24, 339–348. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, R.; Morici, N.; De Servi, S.; De Luca, G.; Galasso, G.; Piscione, F.; A Ferri, L.; Piatti, L.; Grosseto, D.; Tortorella, G.; et al. Impact of renal dysfunction and acute kidney injury on outcome in elderly patients with acute coronary syndrome undergoing percutaneous coronary intervention. Eur. Heart J. Acute Cardiovasc. Care 2020, 6, 2048872620920475. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group A (n = 345) | Group B (n = 359) | Group C (n = 100) | Statistic | p-Value | |
|---|---|---|---|---|---|
| Demographic | |||||
| Age ( ± s, years) | 65 ± 13 | 66 ± 14 | 66 ± 14 | 1.453 | 0.235 |
| Male [n(%)] | 258 (74.8) | 258 (71.9) | 77 (77) | 1.394 | 0.498 |
| Medical history | |||||
| Smoking [n(%)] | 4.921 | 0.295 | |||
| Never smoking | 175 (50.7) | 176 (49.2) | 38 (38.4) | ||
| Quit smoking | 40 (11.6) | 40 (11.2) | 14 (14.1) | ||
| Continue smoking | 130 (37.7) | 142 (39.7) | 47 (47.5) | ||
| Drinking history [n(%)] | 0.178 | 0.996 | |||
| Never drinking | 242 (70.6) | 251 (70.5) | 68 (69.4) | ||
| Quit drinking | 34 (9.9) | 33 (9.3) | 10 (10.2) | ||
| Continue drinking | 67 (19.5) | 72 (20.2) | 20 (20.4) | ||
| Hypertension [n(%)] | 191 (44.6) | 232 (35.4) | 47 (47.0) | 8.068 | 0.018 |
| Diabetes [n(%)] | 83 (24.1) | 106 (29.5) | 24 (24.0) | 3.066 | 0.216 |
| Coronary heart disease [n(%)] | 66 (19.1) | 58 (16.2) | 17 (17.0) | 1.066 | 0.587 |
| Abnormal kidney function [n(%)] | 4 (1.25) | 16 (4.5) | 6 (6.1) | 9.061 | 0.011 |
| ACS [n(%)] | 32.628 | <0.001 | |||
| UA | 86 (24.9) | 66 (18.4) | 9 (9.0) | ||
| NSTEMI | 92 (26.7) | 102 (28.4) | 12 (12.0) | ||
| STEMI | 167 (48.4) | 191 (53.2) | 79 (79.0) | ||
| Clinical characteristic | |||||
| Clinical signs [n(%)] | |||||
| Chest pain | 322 (95.3) | 340 (95.0) | 96 (97.0) | 0.631 | 0.729 |
| Nausea and vomiting | 20 (5.9) | 32 (9.0) | 5 (5.1) | 3.307 | 0.191 |
| Profuse sweating | 75 (22.2) | 77 (21.8) | 26 (26.3) | 0.936 | 0.626 |
| Dyspnea | 10 (3.0) | 18 (5.1) | 3 (3.0) | 2.313 | 0.315 |
| syncope | 9 (2.7) | 10 (2.8) | 1 (1.0) | 1.077 | 0.584 |
| ± s, mmHg) | 132 ± 25 | 134 ± 25 | 132 ± 25 | 3.744 | 0.024 |
| Heart rate [M(QR)] | 85 (69,110) | 80 (71,91) | 90 (73,102) | 8.467 | 0.015 |
| Laboratory values | |||||
| BNP [M(QR), ng/L] | 145.12 (33.15,465.37) | 341.70 (133.10,711.64) | 165.6 (79.80,2192.80) | 27.677 | <0.001 |
| Serum creatinine [M(QR), μmol/L] | 76.40 (62.50,90.00) | 86.30 (66.95,112.30) | 92.70 (65.10,176.83) | 4.988 | 0.083 |
| eGFR [M(QR), mL/min/1.73 m2] | 92.4 (67.8,117.8) | 82.7 (60.8,106.0) | 82.6 (62.0,106.8) | 0.617 | 0.734 |
| Triglyceride [M(QR), mmol/L] | 1.12 (0.84,2.38) | 1.44 (1.16,2.26) | 1.61 (1.26,2.27) | 7.758 | 0.021 |
| Total cholesterol [M(QR), mmol/L] | 3.95 (3.32,4.50) | 4.49 (3.84,5.13) | 4.46 (2.88,5.56) | 3.700 | 0.157 |
| LDL-C [M(QR), mmol/L] | 2.29 (1.47,3.08) | 2.71 (2.17,3.28) | 2.75 (2.24,3.68) | 4.751 | 0.093 |
| HDL-C [M(QR), mmol/L] | 1.19 (0.95,1.51) | 1.14 (0.93,1.22) | 1.17 (0.83,1.37) | 1.841 | 0.398 |
| CRP [M(QR), mg/L] | 4.60(2.65,6.30) | 10.90 (3.35,43.24) | 10.97 (1.68,34.60) | 49.007 | <0.001 |
| Hemoglobin [M(QR),g/L] | 135 (120,145) | 135 (119,146) | 134 (100,141) | 10.714 | 0.005 |
| Blood glucose [M(QR), mmol/L] | 6.81 (5.79,9.76) | 6.84 (5.77,8.90) | 6.60 (5.08,8.35) | 2.824 | 0.244 |
| PCI [n(%)] | 224 (64.9) | 256 (71.3) | 78 (78.0) | 7.349 | 0.025 |
| Multiple coronary arteries lesion [n(%)] | 82 (33.7) | 109 (38.2) | 42 (47.7) | 5.411 | 0.067 |
| Left main or anterior descending lesion [n(%)] | 123 (56.9) | 158 (61.5) | 52 (64.2) | 1.668 | 0.434 |
| Drug [n(%)] | |||||
| Dual antiplatelet drugs | 266 (90.8) | 296 (93.1) | 83 (94.3) | 3.798 | 0.434 |
| Lipid-lowering drugs | 304 (94.1) | 328 (97.9) | 85 (93.4) | 7.149 | 0.028 |
| β-blockers | 231 (72.2) | 241 (71.9) | 60 (64.9) | 1.471 | 0.479 |
| ACEI/ARB | 181 (57.6) | 172 (52.0) | 38 (46.9) | 6.237 | 0.044 |
| Variable | β Value | p Value | HR | 95%CI | |
|---|---|---|---|---|---|
| Gender (Male vs. Female) | 0.301 | 0.242 | 1.351 | 0.816 | 2.234 |
| Age | 0.043 | <0.001 | 1.044 | 1.023 | 1.066 |
| Systolic blood pressure | −0.009 | 0.075 | 0.991 | 0.982 | 1.001 |
| Heart rate | 0.008 | 0.141 | 1.008 | 0.997 | 1.018 |
| Serum creatinine | 0.002 | 0.417 | 0.998 | 1.002 | 1.003 |
| Blood glucose | 0.012 | 0.663 | 1.012 | 0.959 | 1.068 |
| White blood cells | 0.097 | 0.001 | 1.102 | 1.043 | 1.164 |
| Hematocrit | −0.010 | 0.677 | 0.990 | 0.947 | 1.036 |
| Multiple coronary artery lesions | 0.768 | <0.001 | 2.156 | 1.400 | 3.321 |
| Variable | β Value | p Value | HR | 95%CI | |
|---|---|---|---|---|---|
| Lp(a) ≥ 300 mg/L | 0.785 | 0.001 | 2.193 | 1.400 | 3.436 |
| Fibrinogen ≥ 3.08 g/L | 0.596 | 0.015 | 1.814 | 1.120 | 2.937 |
| Lp(a) combined with fibrinogen | 0.001 | ||||
| Group A | — | — | — | — | — |
| Group B | 0.612 | 0.029 | 1.844 | 1.064 | 3.195 |
| Group C | 1.220 | <0.001 | 3.388 | 1.816 | 6.321 |
| Model. | MACCE | ||
|---|---|---|---|
| C-Statistic (95%CI) | NRI | IDI | |
| Basic model | 0.694 (0.664–0.725) | — | — |
| Basic model + Lp(a) classification | 0.723 (0.694–0.752) | 0.057 | 0.067 |
| Basic model + fibrinogen classification | 0.721 (0.691–0.751) | 0.074 | 0.040 |
| Basic model + Lp(a) combined fibrinogen classification | 0.736 (0.707–0.766) | 0.095 | 0.094 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, C.-Y.; Ye, T.; Cheng, L.-C.; Tong, L.; Tong, L.; Zhang, Z.; Cai, L. Lipoprotein a Combined with Fibrinogen as an Independent Predictor of Long-Term Prognosis in Patients with Acute Coronary Syndrome: A Multi-Center Retrospective Study. J. Cardiovasc. Dev. Dis. 2022, 9, 322. https://doi.org/10.3390/jcdd9100322
Cui C-Y, Ye T, Cheng L-C, Tong L, Tong L, Zhang Z, Cai L. Lipoprotein a Combined with Fibrinogen as an Independent Predictor of Long-Term Prognosis in Patients with Acute Coronary Syndrome: A Multi-Center Retrospective Study. Journal of Cardiovascular Development and Disease. 2022; 9(10):322. https://doi.org/10.3390/jcdd9100322
Chicago/Turabian StyleCui, Cai-Yan, Tao Ye, Lian-Chao Cheng, Lin Tong, Lan Tong, Zhen Zhang, and Lin Cai. 2022. "Lipoprotein a Combined with Fibrinogen as an Independent Predictor of Long-Term Prognosis in Patients with Acute Coronary Syndrome: A Multi-Center Retrospective Study" Journal of Cardiovascular Development and Disease 9, no. 10: 322. https://doi.org/10.3390/jcdd9100322