

Cardiac Fibrosis and Innervation State in Uncorrected and Corrected Transposition of the Great Arteries: A Postmortem Histological Analysis and Systematic Review
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
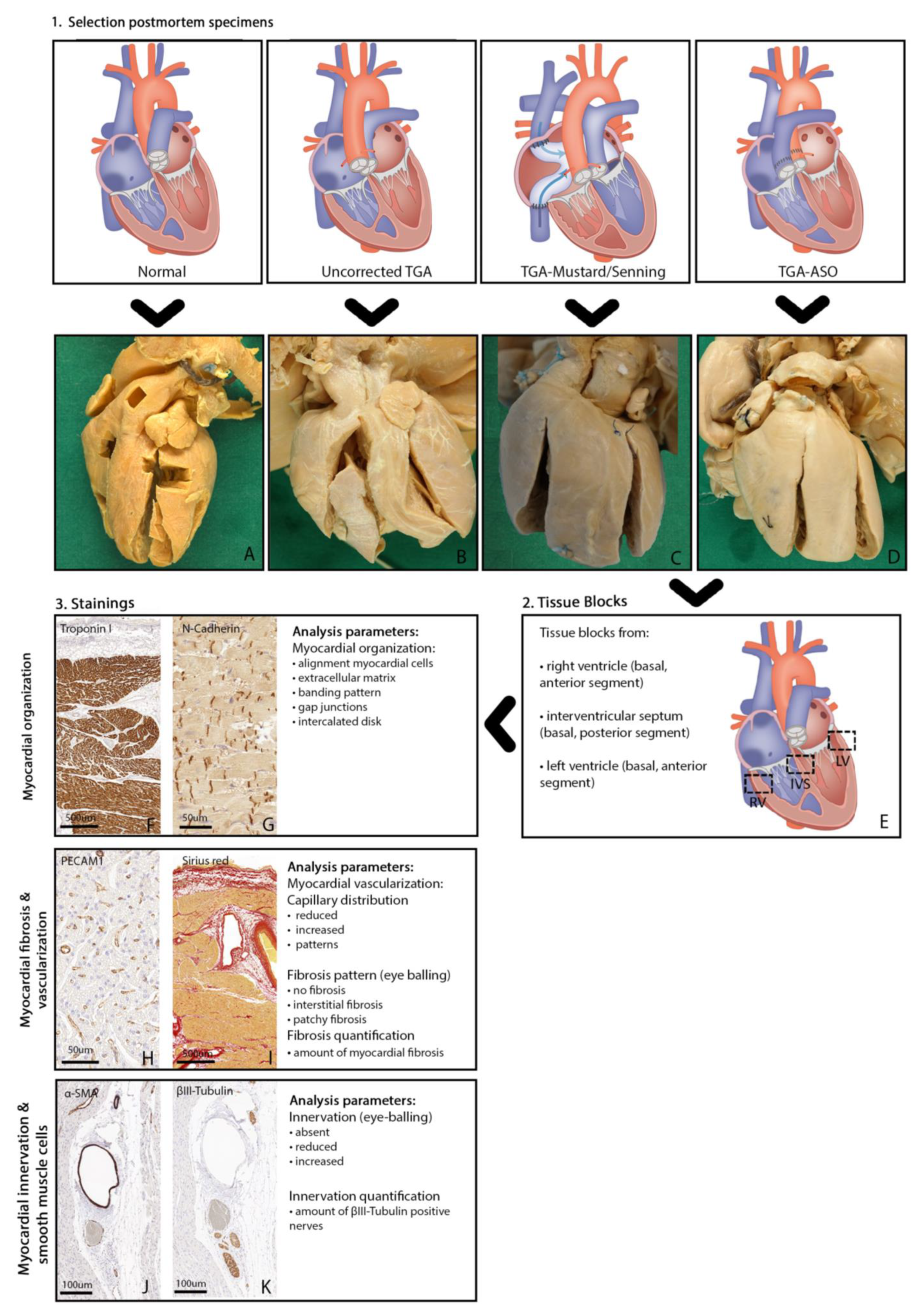
2.1. Study Design
2.2. Selection Criteria Postmortem Hearts
2.3. Tissue Blocks of Postmortem Hearts
2.4. Immunohistochemical Staining and Analysis
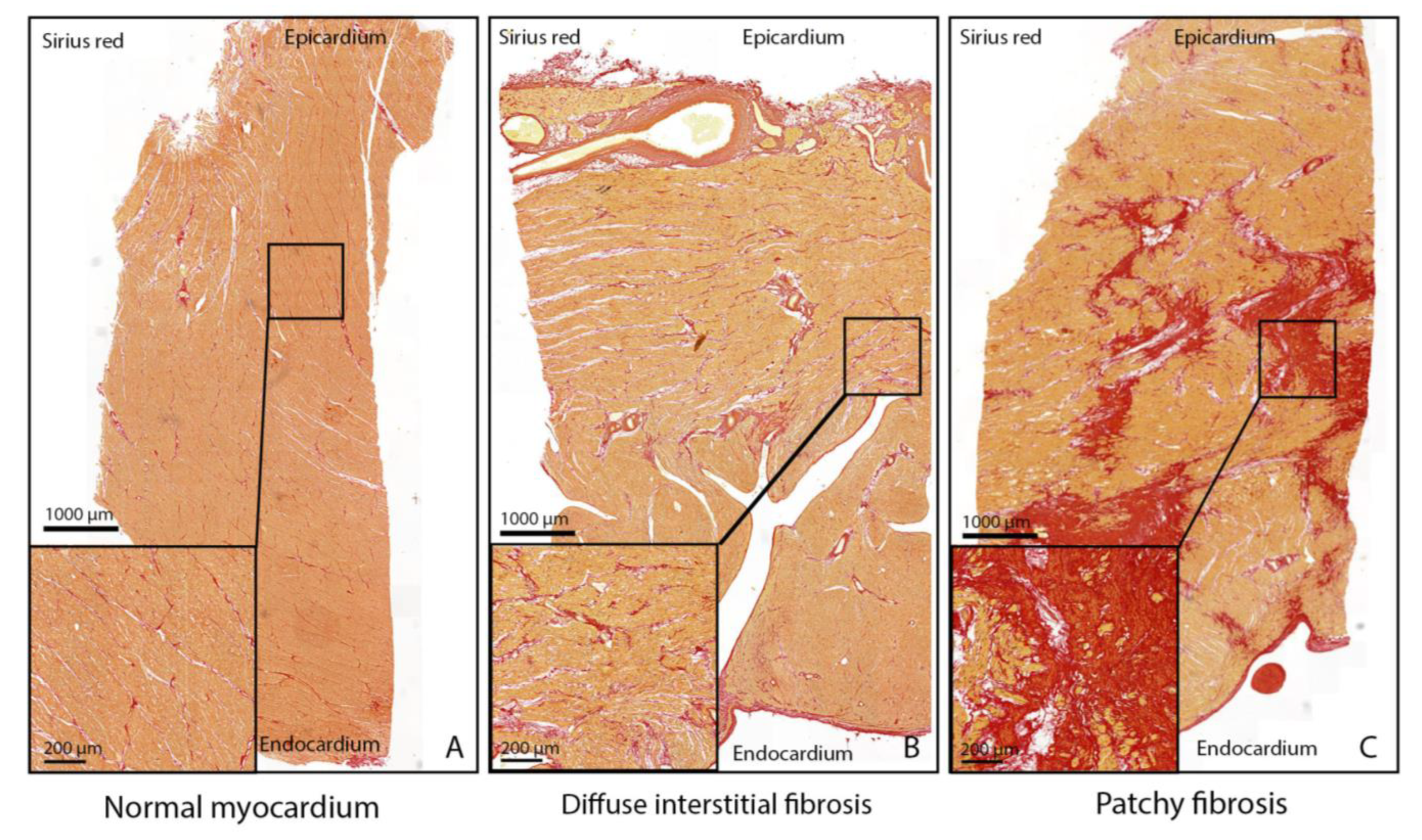
2.5. Myocardial Fibrosis Patterns and Quantification
2.6. Myocardial Innervation: βIII-Tubulin Patterns and Quantification
2.7. Literature Review
2.8. Statistical Analysis
3. Results
3.1. Postmortem Hearts
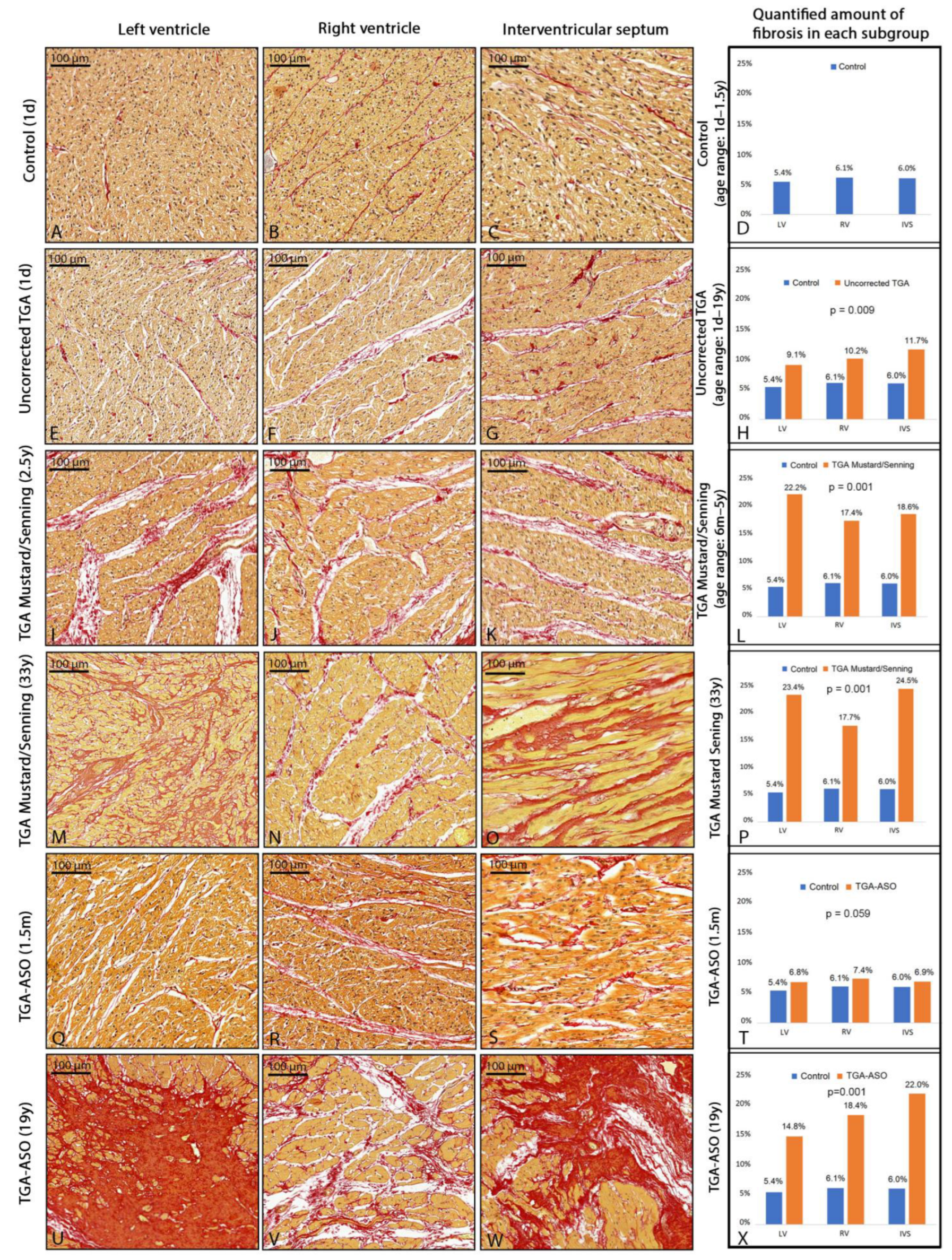
3.2. Myocardial Fibrosis
3.2.1. Myocardial Fibrosis in Control Group
3.2.2. Myocardial Fibrosis in Uncorrected TGA
3.2.3. Myocardial Fibrosis in TGA-Mustard/Senning
3.2.4. Myocardial Fibrosis in TGA-ASO Specimens
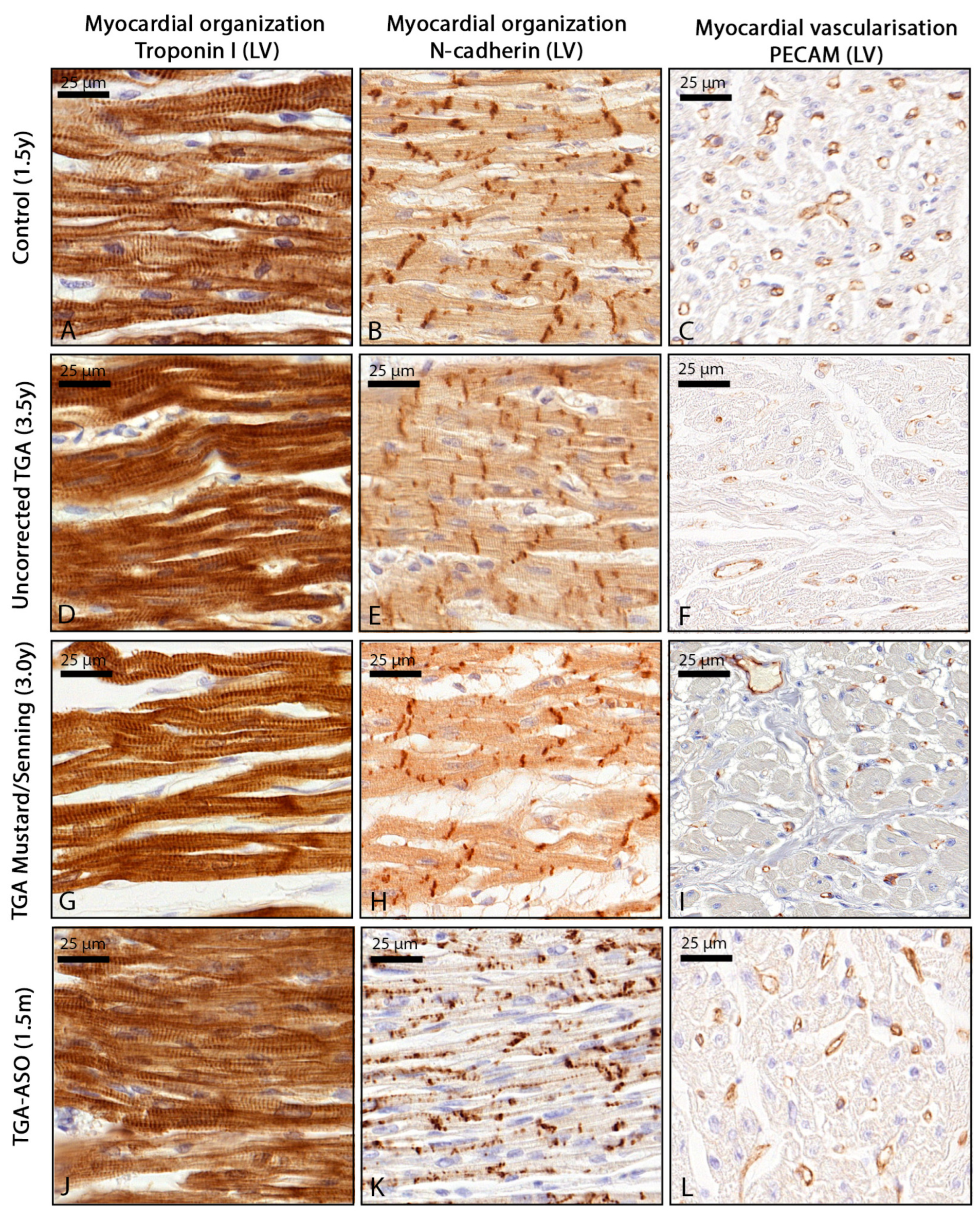
3.3. Myocardial Organization and Vascularization
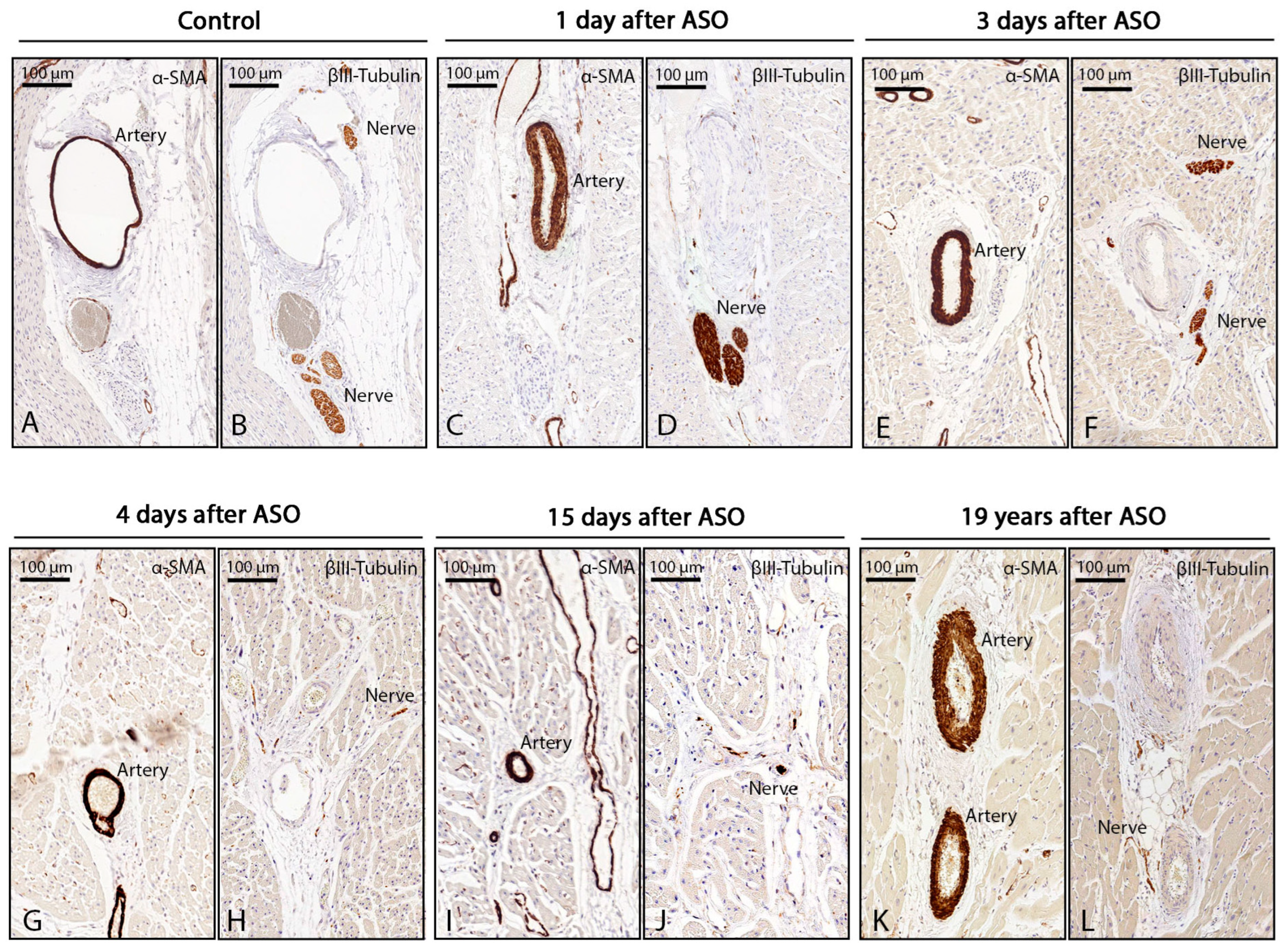
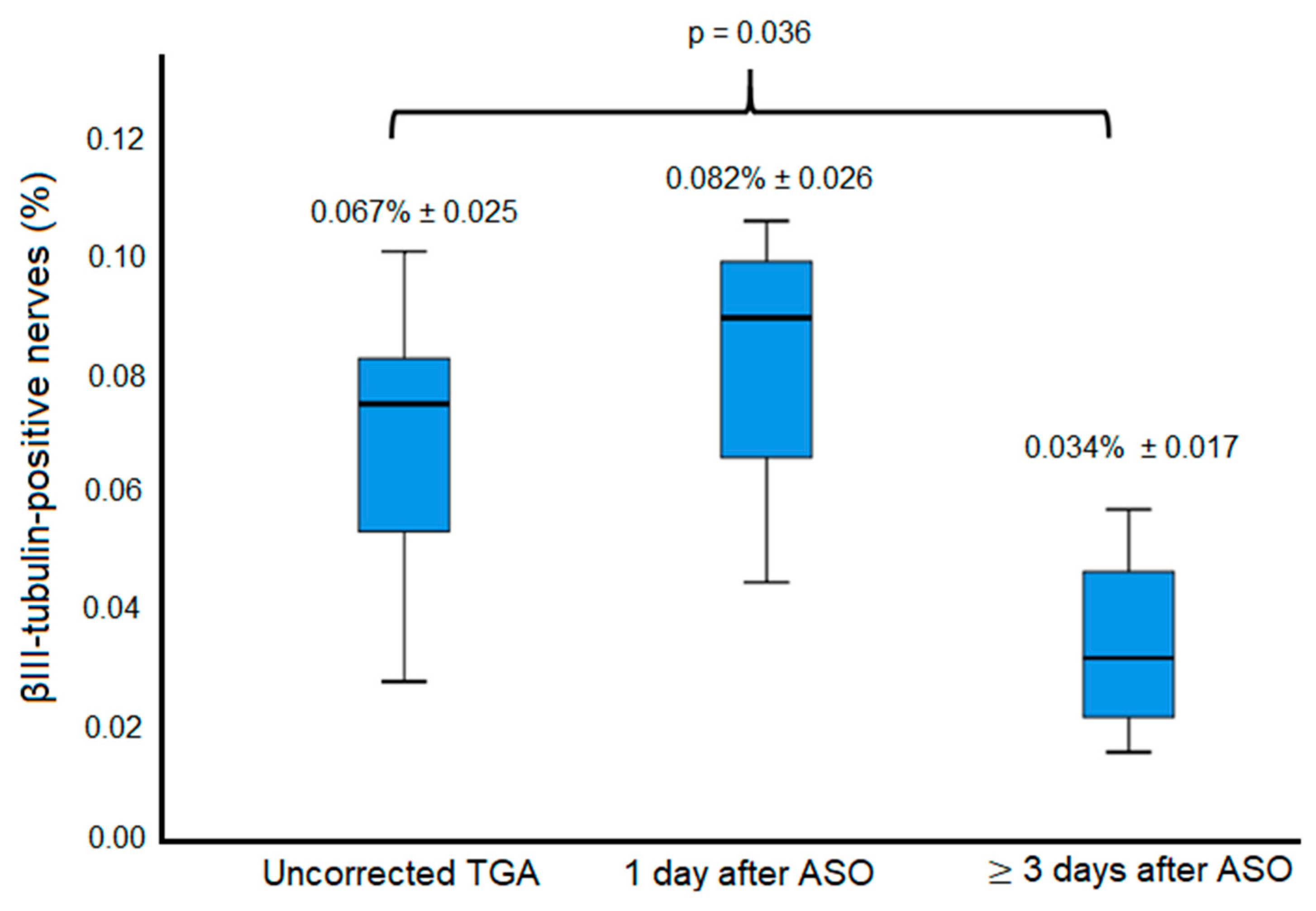
3.4. Innervation Post-ASO
3.5. Literature Review on Myocardial Fibrosis in TGA
3.5.1. CMR Imaging Studies after Mustard/Senning Correction
3.5.2. Histological Studies after Mustard/Senning Correction
3.5.3. CMR Imaging Studies after TGA-ASO
3.6. Literature Review on Cardiac Innervation in TGA-ASO
4. Discussion
4.1. Early Interstitial Myocardial Fibrosis in TGA
4.2. Myocardial Fibrosis after Surgical Correction
4.3. Myocardial Innervation Post-ASO
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hoffman, J.I. Congenital heart disease: Incidence and inheritance. Pediatr. Clin. N. Am. 1990, 37, 25–43. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, A.M. Aortopulmonary transposition in the fetus: Speculation on pathophysiology and therapy. Pediatr. Res. 2007, 61, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Iles, L.; Pfluger, H.; Phrommintikul, A.; Cherayath, J.; Aksit, P.; Gupta, S.N.; Kaye, D.M.; Taylor, A.J. Evaluation of diffuse myocardial fibrosis in heart failure with cardiac magnetic resonance contrast-enhanced T1 mapping. J. Am. Coll. Cardiol. 2008, 52, 1574–1580. [Google Scholar] [CrossRef]
- Schwarz, F.; Mall, G.; Zebe, H.; Blickle, J.; Derks, H.; Manthey, J.; Kubler, W. Quantitative morphologic findings of the myocardium in idiopathic dilated cardiomyopathy. Am. J. Cardiol. 1983, 51, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Broberg, C.S.; Valente, A.M.; Huang, J.; Burchill, L.J.; Holt, J.; Van Woerkom, R.; Powell, A.J.; Pantely, G.A.; Jerosch-Herold, M. Myocardial fibrosis and its relation to adverse outcome in transposition of the great arteries with a systemic right ventricle. Int. J. Cardiol. 2018, 271, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Grotenhuis, H.B.; Cifra, B.; Mertens, L.L.; Riessenkampff, E.; Manlhiot, C.; Seed, M.; Yoo, S.J.; Grosse-Wortmann, L. Left ventricular remodelling in long-term survivors after the arterial switch operation for transposition of the great arteries. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Kimura, K.; Ieda, M.; Fukuda, K. Development, maturation, and transdifferentiation of cardiac sympathetic nerves. Circ. Res. 2012, 110, 325–336. [Google Scholar] [CrossRef]
- Nademanee, K.; Raju, H.; de Noronha, S.V.; Papadakis, M.; Robinson, L.; Rothery, S.; Makita, N.; Kowase, S.; Boonmee, N.; Vitayakritsirikul, V.; et al. Fibrosis, Connexin-43, and Conduction Abnormalities in the Brugada Syndrome. J. Am. Coll. Cardiol. 2015, 66, 1976–1986. [Google Scholar] [CrossRef]
- Glashan, C.A.; Androulakis, A.F.A.; Tao, Q.; Glashan, R.N.; Wisse, L.J.; Ebert, M.; de Ruiter, M.C.; van Meer, B.J.; Brouwer, C.; Dekkers, O.M.; et al. Whole human heart histology to validate electroanatomical voltage mapping in patients with non-ischaemic cardiomyopathy and ventricular tachycardia. Eur. Heart J. 2018, 39, 2867–2875. [Google Scholar] [CrossRef]
- Cheung, Y.F.; Lam, W.W.M.; So, E.K.F.; Chow, P.C. Differential myocardial fibrosis of the systemic right ventricle and subpulmonary left ventricle after atrial switch operation for complete transposition of the great arteries. Int. J. Cardiol. Heart Vasc. 2020, 30, 100612. [Google Scholar] [CrossRef]
- Ladouceur, M.; Bruneval, P.; Mousseaux, E. Cardiovascular flashlight. Magnetic resonance assessment of fibrosis in systemic right ventricle after atrial switch procedure. Eur. Heart J. 2009, 30, 2613. [Google Scholar] [CrossRef] [PubMed]
- Rydman, R.; Gatzoulis, M.A.; Ho, S.Y.; Ernst, S.; Swan, L.; Li, W.; Wong, T.; Sheppard, M.; McCarthy, K.P.; Roughton, M.; et al. Systemic right ventricular fibrosis detected by cardiovascular magnetic resonance is associated with clinical outcome, mainly new-onset atrial arrhythmia, in patients after atrial redirection surgery for transposition of the great arteries. Circ. Cardiovasc. Imaging 2015, 8, e002628. [Google Scholar] [CrossRef] [PubMed]
- Gorenflo, M.; Serpi, M.; Schnabel, P.A.; Huging, M.; Schmidt, K.G.; Hagl, S.; Ulmer, H.E. Pathological changes of the myocardium in patients after atrial repair for transposition of the great arteries: A possible explanation for left ventricular dysfunction after secondary arterial switch. Z. Kardiol. 2003, 92, 742–746. [Google Scholar] [CrossRef] [PubMed]
- Babu-Narayan, S.V.; Goktekin, O.; Moon, J.C.; Broberg, C.S.; Pantely, G.A.; Pennell, D.J.; Gatzoulis, M.A.; Kilner, P.J. Late gadolinium enhancement cardiovascular magnetic resonance of the systemic right ventricle in adults with previous atrial redirection surgery for transposition of the great arteries. Circulation 2005, 111, 2091–2098. [Google Scholar] [CrossRef] [PubMed]
- Plymen, C.M.; Sado, D.M.; Taylor, A.M.; Bolger, A.P.; Lambiase, P.D.; Hughes, M.; Moon, J.C. Diffuse myocardial fibrosis in the systemic right ventricle of patients late after mustard or Senning surgery: An equilibrium contrast cardiovascular magnetic resonance study. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 963–968. [Google Scholar] [CrossRef] [PubMed]
- Ladouceur, M.; Baron, S.; Nivet-Antoine, V.; Maruani, G.; Soulat, G.; Pereira, H.; Blanchard, A.; Boutouyrie, P.; Paul, J.L.; Mousseaux, E. Role of myocardial collagen degradation and fibrosis in right ventricle dysfunction in transposition of the great arteries after atrial switch. Int. J. Cardiol. 2018, 258, 76–82. [Google Scholar] [CrossRef]
- Shehu, N.; Meierhofer, C.; Messroghli, D.; Mkrtchyan, N.; Martinoff, S.; Ewert, P.; Stern, H. Diffuse fibrosis is common in the left, but not in the right ventricle in patients with transposition of the great arteries late after atrial switch operation. Int. J. Cardiovasc. Imaging 2018, 34, 1241–1248. [Google Scholar] [CrossRef]
- Shepard, C.W.; Germanakis, I.; White, M.T.; Powell, A.J.; Co-Vu, J.; Geva, T. Cardiovascular Magnetic Resonance Findings Late After the Arterial Switch Operation. Circ. Cardiovasc. Imaging 2016, 9, e004618. [Google Scholar] [CrossRef]
- Suther, K.R.; Hopp, E.; Geier, O.; Brun, H.; Nguyen, B.; Tomterstad, A.H.; Smevik, B.; Fiane, A.E.; Lindberg, H.L.; de Lange, C. Diffuse myocardial fibrosis in adolescents operated with arterial switch for transposition of the great arteries—A CMR study. Int. J. Cardiol. 2019, 276, 100–106. [Google Scholar] [CrossRef]
- Kondo, C.; Nakazawa, M.; Momma, K.; Kusakabe, K. Sympathetic denervation and reinnervation after arterial switch operation for complete transposition. Circulation 1998, 97, 2414–2419. [Google Scholar] [CrossRef]
- Kuehn, A.; Vogt, M.; Schwaiger, M.; Ewert, P.; Hauser, M. Ventricular sympathetic innervation in patients with transposition of the great arteries after arterial switch operation and Rastelli procedure: Impact of arterial dissection and coronary reimplantation. Circ. J. 2014, 78, 1717–1722. [Google Scholar] [CrossRef] [PubMed]
- Possner, M.; Buechel, R.R.; Vontobel, J.; Mikulicic, F.; Grani, C.; Benz, D.C.; Clerc, O.F.; Fuchs, T.A.; Tobler, D.; Stambach, D.; et al. Myocardial blood flow and cardiac sympathetic innervation in young adults late after arterial switch operation for transposition of the great arteries. Int. J. Cardiol. 2020, 299, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Zwanenburg, F.; DeRuiter, M.C.; Wisse, L.J.; van Munsteren, C.J.; Bartelings, M.M.; Goumans, M.J.; Ten Harkel, A.D.J.; Jongbloed, M.R.M.; Haak, M.C. Deficient Myocardial Organization and Pathological Fibrosis in Fetal Aortic Stenosis-Association of Prenatal Ultrasound with Postmortem Histology. J. Cardiovasc. Dev. Dis. 2021, 8, 121. [Google Scholar] [CrossRef] [PubMed]
- Miles, C.; Westaby, J.; Ster, I.C.; Asimaki, A.; Boardman, P.; Joshi, A.; Papadakis, M.; Sharma, S.; Behr, E.R.; Sheppard, M.N. Morphometric characterization of collagen and fat in normal ventricular myocardium. Cardiovasc. Pathol. 2020, 48, 107224. [Google Scholar] [CrossRef]
- Schipke, J.; Brandenberger, C.; Rajces, A.; Manninger, M.; Alogna, A.; Post, H.; Muhlfeld, C. Assessment of cardiac fibrosis: A morphometric method comparison for collagen quantification. J. Appl. Physiol. 2017, 122, 1019–1030. [Google Scholar] [CrossRef]
- Andersen, S.; Nielsen-Kudsk, J.E.; Vonk Noordegraaf, A.; de Man, F.S. Right Ventricular Fibrosis. Circulation 2019, 139, 269–285. [Google Scholar] [CrossRef]
- Woudstra, O.I.; Zandstra, T.E.; Vogel, R.F.; van Dijk, A.P.J.; Vliegen, H.W.; Kies, P.; Jongbloed, M.R.M.; Egorova, A.D.; Doevendans, P.; Konings, T.C.; et al. Clinical Course Long after Atrial Switch: A Novel Risk Score for Major Clinical Events. J. Am. Heart Assoc. 2021, 10, e018565. [Google Scholar] [CrossRef]
- Klitsie, L.M.; Roest, A.A.; Kuipers, I.M.; Hazekamp, M.G.; Blom, N.A.; Ten Harkel, A.D. Left and right ventricular performance after arterial switch operation. J. Thorac. Cardiovasc. Surg. 2014, 147, 1561–1567. [Google Scholar] [CrossRef]
- Di Salvo, G.; Al Bulbul, Z.; Issa, Z.; Fadel, B.; Al-Sehly, A.; Pergola, V.; Al Halees, Z.; Al Fayyadh, M. Left ventricular mechanics after arterial switch operation: A speckle-tracking echocardiography study. J. Cardiovasc. Med. 2016, 17, 217–224. [Google Scholar] [CrossRef]
- van der Palen, R.L.F.; Blom, N.A.; Kuipers, I.M.; Rammeloo, L.A.J.; Jongbloed, M.R.M.; Konings, T.C.; Bouma, B.J.; Koolbergen, D.R.; Hazekamp, M.G. Long-term outcome after the arterial switch operation: 43 years of experience. Eur. J. Cardiothorac. Surg. 2021, 59, 968–977. [Google Scholar] [CrossRef]
- Gallego-Page, J.C.; Segovia, J.; Alonso-Pulpon, L.; Alonso-Rodriguez, M.; Salas, C.; Ortiz-Berrocal, J. Reinnervation after heart transplantation: A multidisciplinary study. J. Heart Lung Transplant. 2004, 23, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Schwaiger, M.; Hutchins, G.D.; Kalff, V.; Rosenspire, K.; Haka, M.S.; Mallette, S.; Deeb, G.M.; Abrams, G.D.; Wieland, D. Evidence for regional catecholamine uptake and storage sites in the transplanted human heart by positron emission tomography. J. Clin. Investig. 1991, 87, 1681–1690. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Uncorrected TGA (n = 8) | TGA-Mustard/Senning (n = 6) | TGA-ASO (n = 8) | |
|---|---|---|---|
| Age (years), median | 3.9 | 3.5 | 3.7 |
| Age category, n (%) | |||
| 1 day | 1 (13%) | 0 (0%) | 1 (13%) |
| 1–3.5 months | 2 (25%) | 0 (0%) | 3 (38%) |
| 1–5 years | 4 (50%) | 5 (83%) | 3 (38%) |
| 19–33 years | 1 (13%) | 1 (17%) | 1 (13%) |
| Sex (male), n (%) | 6 (75%) | 4 (67%) | 7 (88%) |
| TGA subtype, n (%) | |||
| TGA-IVS | 3 (38%) | 3 (50%) | 2 (25%) |
| TGA-VSD | 3 (38%) | 1 (17%) | 4 (50%) |
| TB-DORV | 2 (25%) | 2 (33%) | 2 (25%) |
| Shunts | |||
| Foramen ovale, n (%) | |||
| Open | 8 (100%) | - | 0 (0%) |
| Closed after ASO | – | - | 8 (100%) |
| Closed | 0 (0%) | - | 0 (0%) |
| Ductus arteriosus, n (%) | |||
| Open | 4 (50%) | 0 (0%) | 0 (0%) |
| Closed (after surgery) | 0 (0%) | 1 (17%) | 4 (50%) |
| Unknown | 4 (50%) | 5 (83%) | 4 (50%) |
| Cause of death, n (%) | |||
| Cardiac death | 4 (50%) | 5 (83%) | 7 (88%) |
| Other | 2 (25%) | 1 (17%) | 1 (13%) |
| Unknown | 2 (25%) | 0 (0%) | 0 (0%) |
| Procedures, n (%) | |||
| Rashkind | 2 (25%) | 3 (50%) | 0 (0%) |
| Blalock-Hanlon | 1 (13%) | 1 (17%) | 1 (13%) |
| Time between surgical correction and death, category, n (%) | |||
| 1–4 days | - | 0 (0%) | 6 (75%) |
| 15 days | - | 1 (13%) | |
| 6 months | - | 1 (17%) | - |
| 1–3 years | - | 4 (67%) | - |
| >19 years | - | 1 (17%) | 1 (13%) |
| Control | Diagnosis | Age | Systemic LV | Subpulmonary RV | IVS | Mean a | |
|---|---|---|---|---|---|---|---|
| #1 | No-CHD | 1 day | 4.2% | 4.9% | 5.4% | 4.8% | |
| #2 | No-CHD | 1 month | 5.2% | 6.4% | 6.1% | 5.9% | |
| #3 | No-CHD | 1.5 years | 6.7% | 7.1% | 6.5% | 6.8% | |
| mean b | 5.4% | 6.1% | 6.0% | ||||
| Uncorrected TGA | Diagnosis | Age | Subpulmonary LV | Systemic RV | IVS | Mean a | |
| #4 | TGA-IVS | 1 day | 5.2% | 6.1% | 8.7% | 6.7% | |
| #5 | TB-DORV | 1 month | 6.6% | 8.9% | 8.4% | 8.0% | |
| #6 | TB-DORV | 1.5 months | 13.8% | 13.4% | 8.6% | 11.9% | |
| #7 | TGA-VSD | 2.5 years | 5.8% | 9.7% | 7.1% | 7.5% | |
| #8 | TGA-IVS | 2.5 years | 17.9% | 16.2% | 22.2% | 18.8% | |
| #9 | TGA-VSD | 3.5 years | 9.2% | 10.5% | 10.7% | 10.1% | |
| #10 | TGA-IVS | 5.5 years | 6.2% | 8.9% | 8.0% | 7.7% | |
| #11 | TGA-VSD | 20 years | 7.8% | 8.0% | 19.8% | 11.9% | |
| mean b | 9.1% | 10.2% | 11.7% | ||||
| TGA-Mustard/Senning | Diagnosis | Age | Subpulmonary LV | Systemic RV | IVS | Mean a | |
| #12 | TGA-VSD | 1 year | 36.7% | 21.8% | 23.5% | 27.3% | |
| #13 | TGA-IVS | 1.8 years | 11.9% | 16.1% | 10.7% | 12.9% | |
| #14 | TGA-IVS | 2.5 years | 14.9% | 15.1% | 17.1% | 15.7% | |
| #15 | TB-DORV | 3.5 years | 26.2% | 17.5% | 20.8% | 21.5% | |
| #16 | TGA-IVS | 5 years | 21.3% | 16.5% | 21.1% | 19.6% | |
| #17 | TB-DORV | 33 years | 23.4% | 17.7% | 24.5% | 21.9% | |
| mean b | 22.4% | 17.5% | 19.6% | ||||
| TGA-ASO | Diagnosis | Age | Systemic LV | Subpulmonary RV | IVS | Mean a | |
| #18 | TGA-IVS | 1 day | - | - | - | - | |
| #19 | TGA-VSD | 1 month | - | - | - | - | |
| #20 | TGA-IVS | 1.5 months | 6.8% | 7.4% | 6.9% | 7.0% | |
| #21 | TGA-VSD | 3.5 months | - | - | - | - | |
| #22 | TGA-VSD | 2 years | - | - | - | - | |
| #23 | TGA-VSD | 3.5 years | - | - | - | - | |
| #24 | TB-DORV | 4.5 years | - | - | - | - | |
| #25 | TGA-IVS | 19 years | 14.8% | 18.4% | 22.0% | 18.4% | |
| mean b | 10.8% | 12.9% | 14.5% |
| Author and Year | Surgical Correction | (n) | Age | Controls (n) | Age | Examination | Protocol | Main Findings/Conclusions |
|---|---|---|---|---|---|---|---|---|
| Broberg et al. 2018 [5] | Mustard/Senning | 53 | Mean 34.6 years | 22 | Mean 40.2 years | CMR | T1 mapping and ECV before and after gadolineum | Significantly higher ECV for the systemic RV (28.7 ± 4.4%) compared to controls (26.1 ± 2.8%, p = 0.0104). |
| Cheung et al. 2020 [10] | Mustard/Senning | 31 | Mean 33.3 years | - | - | CMR | T1 mapping and ECV before and after gadolineum | Patients had significantly greater RV and LV native T1 times and ECV values (all p < 0.001). |
| Ladouceur et al. 2009 [11] | Senning | 1 | 27.1 years | - | - | CMR and microscopic | LGE before transplantation and RV biopsies post-transplantation | LGE in RV inferior wall and septum. Dense and contiguous fibrosis (25%) in RV inferior wall and diffuse interstitial fibrosis at many sites. |
| Rydman et al. 2015 [12] | Mustard/Senning | 55 | Mean 27.0 years | - | - | CMR and microscopic | CMR and histological assessment | RV LGE was present in 31 patients (56%). Histological assessment post-transplantation (n = 1): focal fibrosis in RV and diffuse fibrosis in the septum, and no fibrosis in LV. |
| Gorenflo et al. 2003 [13] | Mustard/Senning | 12 | Median 16.9 years | - | - | Microscopic | Endomyocardial biopsies from LV and RV | All systemic RV biopsies showed interstitial fibrosis, and 6/12 patients showed fibrous and fatty degeneration of the subpulmonary LV. |
| Babu-Narayan et al. 2005 [14] | Mustard/Senning | 36 | Mean 27.0 years | - | - | CMR | LGE | Late gadolineum RV enhancement was seen in 61% of patients with various patterns. The extent of LGE correlated with age. |
| Plymen et al. 2013 [15] | Mustard/Senning | 14 | Median 33.7 years | 14 | Mean 32.0 years | CMR | T1 mapping and ECV before and after gadolineum | No transmural LGE was observed. Septal ECV was significantly higher in patients than in controls. |
| Ladouceur et al. 2018 [16] | Mustard/Senning | 48 | Median 32 years | - | - | CMR | LGE | LGE was present in RV in 17 patients (35%), mainly at basal segment (54%). |
| Shehu et al. 2018 [17] | Mustard/Senning | 10 | Mean 36.8 years | - | - | CMR | T1 mapping and ECV before and after gadolineum | ECV of the inferior and lateral wall of the LV was significantly increased compared to the RV. |
| Grotenhuis et al. 2018 [6] | ASO | 30 | Mean 15.4 years | 28 | Mean 14.1 years | CMR | ECV, native T1 times and LGE | Native T1 times were significantly higher in the entire LV and septum. No myocardial scarring. |
| Shepard et al. 2016 [18] | ASO | 220 | Median 15.4 years | - | - | CMR | Late enhancement | LGE was found in either the inferior or the superior septal-free wall (most had a nonischemic pattern). |
| Suther et al. 2018 [19] | ASO | 30 | Mean 11.7 years | 15 | Mean 22.4 years | CMR | ECV, pre- and post-contrast T1 mapping and LGE | Increased ECV in all coronary territories. |
| Author and Year | ASO (n) | Age | Controls (n) | Age | Examination | Main Findings/Conclusions |
|---|---|---|---|---|---|---|
| Kondo et al. 1998 [20] | 51 | Mean 4,8 years | 4 | Mean 3.0 months | MIBG scintigraphy | Early after ASO (<1 month) complete absence of MIBG uptake (n = 4) was seen. Although, late after ASO (15 months–10.1 years), there were various degrees of MIBG uptake |
| Kuehn et al. 2014 [21] | 9 | Mean 20.8 years | 9 | Mean 22.1 years | PET: epinephrine retention LV | Signs of reinnervation in most of the patients after ASO and only 1 patient in each group showed complete denervation with epinephrine retention <7%/min |
| Possner et al. 2020 [22] | 12 | Mean 22.5 years | 10 | Mean 22.0 years | PET: meta-hydroxyephedrine uptake | Global meta-hydroxyephedrine uptake was significantly lower in patients compared to controls |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Engele, L.J.; van der Palen, R.L.F.; Egorova, A.D.; Bartelings, M.M.; Wisse, L.J.; Glashan, C.A.; Kiès, P.; Vliegen, H.W.; Hazekamp, M.G.; Mulder, B.J.M.; et al. Cardiac Fibrosis and Innervation State in Uncorrected and Corrected Transposition of the Great Arteries: A Postmortem Histological Analysis and Systematic Review. J. Cardiovasc. Dev. Dis. 2023, 10, 180. https://doi.org/10.3390/jcdd10040180
Engele LJ, van der Palen RLF, Egorova AD, Bartelings MM, Wisse LJ, Glashan CA, Kiès P, Vliegen HW, Hazekamp MG, Mulder BJM, et al. Cardiac Fibrosis and Innervation State in Uncorrected and Corrected Transposition of the Great Arteries: A Postmortem Histological Analysis and Systematic Review. Journal of Cardiovascular Development and Disease. 2023; 10(4):180. https://doi.org/10.3390/jcdd10040180
Chicago/Turabian StyleEngele, Leo J., Roel L. F. van der Palen, Anastasia D. Egorova, Margot M. Bartelings, Lambertus J. Wisse, Claire A. Glashan, Philippine Kiès, Hubert W. Vliegen, Mark G. Hazekamp, Barbara J. M. Mulder, and et al. 2023. "Cardiac Fibrosis and Innervation State in Uncorrected and Corrected Transposition of the Great Arteries: A Postmortem Histological Analysis and Systematic Review" Journal of Cardiovascular Development and Disease 10, no. 4: 180. https://doi.org/10.3390/jcdd10040180