4.1. Agreement between Invasive Brachial and Aortic Blood Pressure (Aim 1)
First, invasive brachial and aortic DBP and MBP showed differences. On average (mean error), the MBP and DBP values were, respectively, ~4 mmHg (95% CI: 1.5–6.1 mmHg) and ~2 mmHg (95% CI: 0.4–4.2 mmHg) higher in the brachial artery (
Table 3). Althoughit is generally accepted that aortic and brachial MBP and DBP were similar when a subject was supine in our study, there were differences between central and peripheral data. Regarding this, there were subjects whose aoMBP was higher than the brachial, and others whose bMBP was higher. This is an important finding, as the constancy of the DBP and MAP values along the great arteries (when a subject is supine) is widely accepted and frequently used in the development of hemodynamic models applied to characterize and understand physiological and pathophysiological phenomena of the arterial system. In fact, the assessment of aoBP by most of the non-invasive methods is based on the described hemodynamic assumption (identical MBP and DBP in the aorta and brachial artery). Although the mean difference in MBP was only 3–4 mmHg (with a 95% CI for the mean error between 1.47 and 6.12 mmHg), 95% of the readings werewithin the range of differences between −8.63 and 16.22 mmHg (
Table 3). Consequently, there were subjects in whom it would be clearly inaccurate to assume that the MBP (and DBP) values obtained peripherally or centrally weresimilar. Previous studies showed data (trends) similar to the described in this work. In subjects (n = 40) referred for diagnostic coronary catheterization, Shih et al. reported that bMBP was significantly higher than aoMBP (simultaneous measurements with custom-made dual pressure sensor catheter) [
20]. Additionally, Nakaomi et al. (2017) reported invasive BP measurements (fluid-filled catheter) in patients who underwent elective coronary angiography. The authors found that bDBP values were on average 1 mmHg higher than those registered in the aorta (they did not perform statistical comparisons) [
21]. Further studies must be performed to clarify the issue and to identify the explanatory factors for the differences between the central and peripheral BP data. In this regard, future work should analyze whether the (unexpected) findings mentioned above are associated with specific biological characteristics of the cardiovascular system of the studied subjects and/or with technical factors related to the methodological approach considered (e.g., the height of the hydrostatic column in the external pressure transducer would be different when the catheter tip is placed in the aorta vs. in the brachial).
On the other hand, SBP levels tended to be higher in the brachial artery than in the aorta (
Table 2 and
Table 3), which is in agreement with the known SBP and PP peripheral amplification phenomenon. In turn, the differences were reduced in older subjects, which is consistent with BPb being considered “more representative” (more alike) aoBP.
Finally, it is worth mentioning that the differences observed between bBP and aoBP were not influenced by BP levels (no proportional error was detected) (
Table 3). This observation would “simplify the situation”, based onthe understanding that potential models that could correct the calibration methods considering the differences in the levels of DBP and MBP between the brachial artery and aorta should not consider the specific BP data.
4.2. Agreement between Invasive and Non-Invasive (Oscillometric) Brachial Blood Pressure (Aim 2)
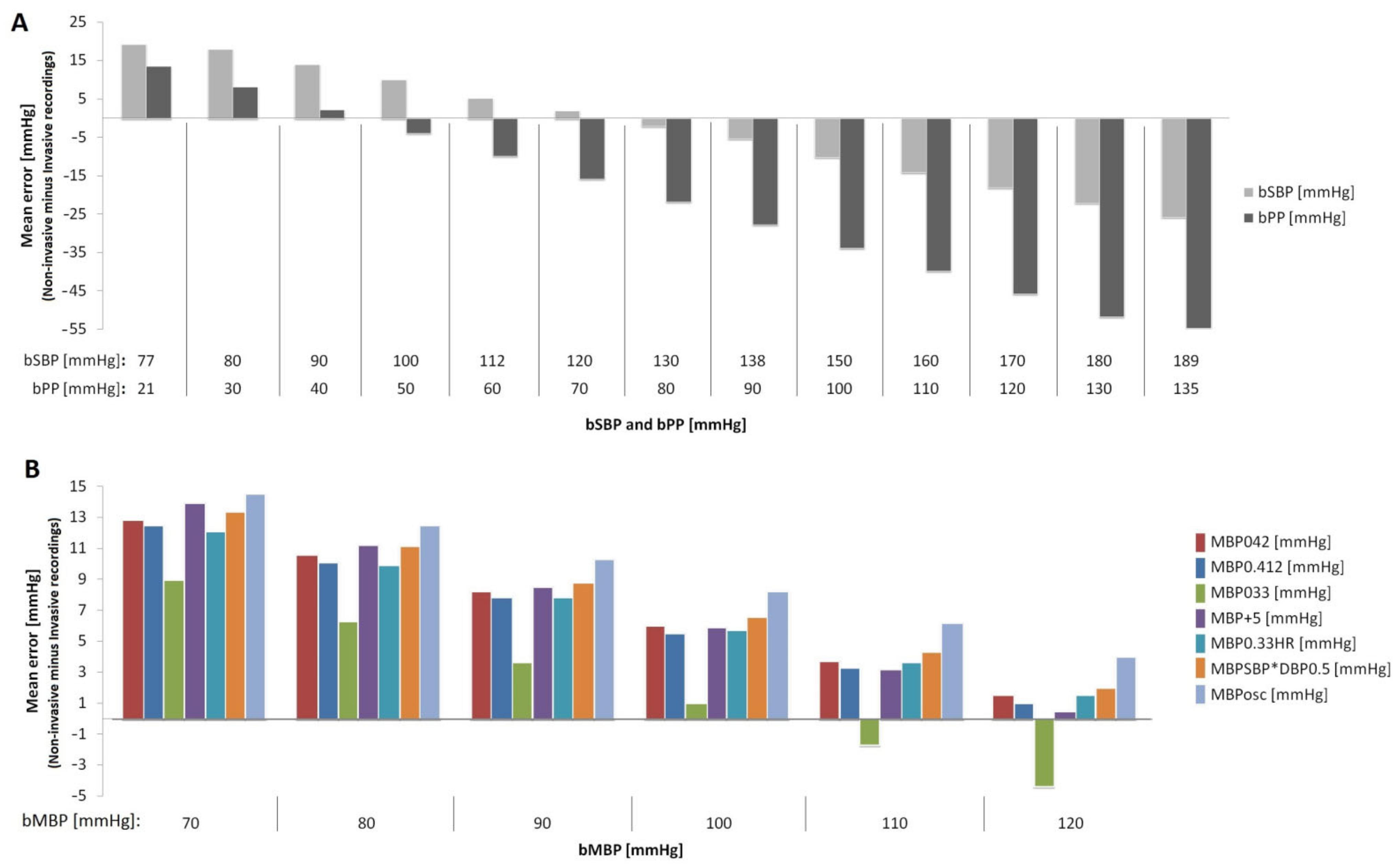
Second, the oscillometric-derived bSBP and bPP values (mean error) were, respectively,~8 mmHg and ~19 mmHg lower than those obtained invasively. In addition, proportional errors were observed (
Table 4,
Figure 2). Invasive bSBP levels within the rangeof 77–125 and 125–189 mmHg were overestimated and underestimated by non-invasive oscillometric measurements, respectively (
Figure 2A). Only volunteers in whom bSBP was in the range of 112–138 mmHg had a calculated error <5 mmHg (
Figure 2A). On the other hand, invasive bPP levels within 21–44 and 44–135 mmHg were, respectively, overestimated and underestimated by non-invasive oscillometric measurements, respectively. In turn, the non-invasive oscillometric bDBP values were, on average, ~11 mmHg higher than those obtained invasively, but no proportional error was observed (
Table 4). Thus, this difference of about 8 (for SBP) and 19 mmHg (for PP) suggests that this misestimation of bSBP and bPP could significantly impact the accurate estimate of the cardiovascular risk in the clinical practice.
This result adds to previous reports [
1,
2,
3] in which the investigators found, on average, that non-invasive SBP and DBP data underestimated and overestimated the invasive BP, respectively. The most important finding, however, was the different situations in terms of BP “over- and underestimation” depending on bBP levels. Undoubtedly, “the worst” situation would be when the real (invasive) bBP is underestimated, which would lead to under diagnosis, a lack of treatment initiation and inaccurate cardiovascular risk prediction. Conversely, when invasive bSBP is optimal or within normal range, oscillometric-based measurements may overestimate the BP, leading to an inappropriate diagnosis, potential unnecessary treatments, adverse effects of medications and higher costs.
4.3. Mean Blood Pressure: Agreement between Invasive and Non-Invasive Data (Aim 3) and Approach to Be Used with Applanation Tonometry (Aim 4)
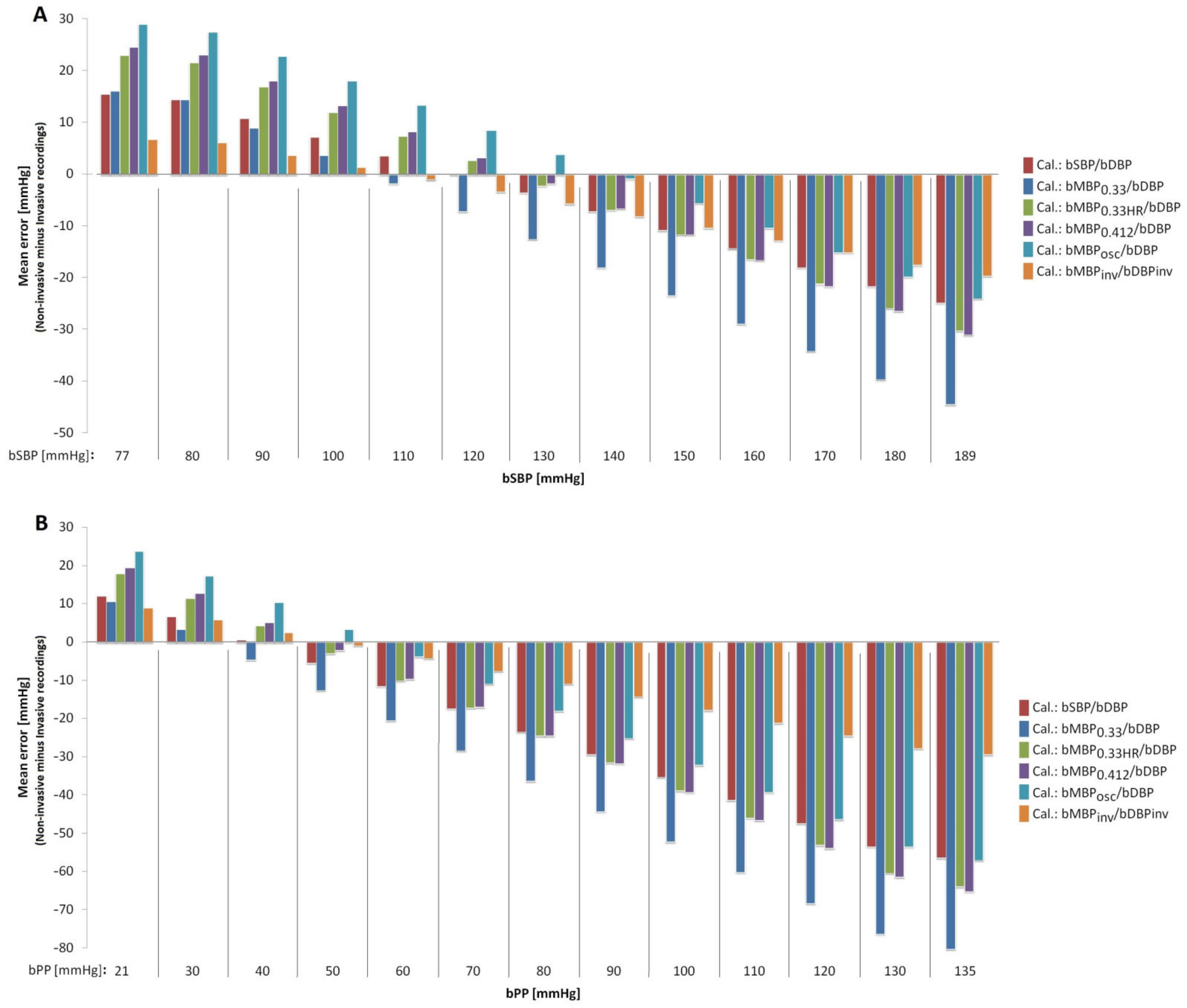
Third and fourth, our analysis showed that (i) the best approach to estimate real (invasive) bMBP through oscillometric measurements (resulting in lower mean error) would be the equation that considers the form factor 33% (except for invasive bMBP values in the upper limit; 120 mmHg); (ii) the calibration of applanation tonometry-derived bBP waves with oscillometricbMBP (bMBP
osc) provides the best approach to estimate the real (invasive) bSBP. Conversely, the worst association was observed when applanation tonometry-derived waves were calibrated using bMBP
033 (bMBP = DBP + PP/3; form factor of 33%;
Table 4 and
Table 5,
Figure 2 and
Figure 3). Disregarding bMBP level, the values measured by the oscillometric device showed the greatest differences with respect to invasive bMBP. Fifth, in general terms, the differences between oscillometry-derived bMBP (regardless of the equation used) and the invasive bMBP measurements were always higher at lower bMBP levels (
Figure 2B). This underlies the need for more accurate devices to measure BP, in order to minimize proportional error.
Looking at our findings, it could be said that if bMBP values are calculated in order to minimize differences with respect to invasive bMBP, the best method to use would be MBP033; however, when calculating BP derived from applanation tonometry, the best option would be to calibrate it with MBPosc. Our findings support the idea that “the best strategy” to calculate (quantify) bMBP depends on the aim that drives its estimation and/or on the approach and devices used. Taking into account the above, perhaps we should abandon the idea of a “false dichotomy” as to whether a given “bMBP formula” is better or worse than another, as this could vary depending on the objective pursued (and the approach considered). Our findings stress the need for methodological transparency and consensus for the non-invasive assessment of peripheral and central hemodynamic parameters. In this regard, it should be noted that, unfortunately, many studies do not describe the way in which bMBP and/or aoBP is quantified.
4.4. Strengths and Limitations
Our results should be analyzed in the context of the strengths and limitations of the present work. First, like most studies of this type, the work was not carried out in healthy subjects, since an invasive study is only indicated in the context of suspected or confirmed cardiovascular disease. Nevertheless, the subjects evaluated in this study are representative of the group of subjects in which the accurate knowledge of cardiovascular data is of particular clinical importance (e.g., to define the risk; to evaluate therapy).
Second, in a sample of 34 subjects we performed both a single (n = 34) analysis and an analysis based on multiple samples (n = 193) per subject. Similar and conclusive results were obtained. Although the simple analysis (n = 34) may be considered by some investigators to be carried out in an “average size n”, it should be noted that it was sufficient to detect important statistical differences, and consequently, it reached sufficient statistical power (avoiding type 2 statistical error). In addition, the concordance (agreement) of invasive and non-invasive bBP levels was estimated with several statistical methods, which increased the reliability of the findings. The invasive recordings in the contralateral brachial artery, as well as the second invasive recording at the level of the aorta, were a part of the research protocol and not of the medical diagnostic evaluation (catheterization for diagnostic purposes). The same consideration applies to the non-invasive oscillometric and tonometric recordings. The work measurements increased the duration of the catheterization by at least 30 min, limiting the number of subjects to be included in the study. Nevertheless, having 34 subjects and over 190 comparative analyses between invasive and non-invasive recordings is an important sample size for a study intended to demonstrate the relevance of several issues, but not necessarily conclusive on this important topic which will necessarily require further study.
Third, we used “fluid column” pressure transducers instead of solid-state pressure sensors. Clearly, solid-state sensors are characterized by a higher accuracy in obtaining BP waveforms, mainly because they are able to detect high-frequency components. However, fluid column transducers are widely used in clinical practice to obtain aoSBP and bSBP levels, and they are used in our University Hospital. It should be noted that in the ARTERY Society task force consensus statement on protocol standardization (“Validation of non-invasive central blood pressure devices”), Sharman et al. state that although micromanometer-tipped catheters are the preferred instruments to use, meticulously managed fluid column catheters may also be acceptable to accurately measure intra-arterial BP [
22]. On the other hand, in the systematic review and meta-analysis carried out by Papaioannou et al. [
1], it was reported that mean errors in the non-invasive estimation of aoSBP were similar between studies using fluid-filled and catheter-tipped transducers. Of course, compared to the high-fidelity micro-tipped catheters, the low-cost liquid-filled catheter manometer systems require more cautious handling and operation (in terms of calibration, frequency response, positioning, zeroing, etc.). However, it should also be recognized that the use of liquid-filled manometer-catheter systems (if proven accurate), should be limited only to the assessment of the maximum and minimum values of the arterial pressure waveform (as in this work), due to the damping of the wave characteristics. Conversely, in studies intended to assess the validity of the pulse waveform-derived indexes (e.g., augmented pressure or augmentation index), a high-fidelity micromanometer-tipped probe should be used to accurately assess the first systolic inflection point. In this context, considering the levels of natural frequency and damping coefficient of our catheter-tubing-external transducer system, and despite using widely validated equipment and measurement methodologies, it is clear that the invasively obtained peak systolic and minimum diastolic pressure levels may have been slightly over- and under-estimated, respectively.
Fourth, it is worth mentioning that in our work we evaluated different approaches (e.g., equations) to quantify bMBP, selecting them among the main empirical approaches (equations) proposed to estimate bMBP in the medical literature. These approaches are based on quantifying bMBP from bSBP and bDBP values, assuming different form factors (33%, 40% or 41.2%). However, despite being widely used, these equations assume that in there is a fixed relationship in each individual between bMBP, bSBP and bDBP. Additionally, the estimation of bMBP considering a fixed ratio between bDBP and bSBP may lead to a correct estimate at the population level but, unfortunately, this method may not be appropriate for estimating bMBP in the individual patient, as there are significant inter-individual variations. In this respect, recently, Grillo et al. [
23] demonstrated that due to the high inter- and intra-individual variability of the pulse waveform, the estimation of bMBP based on fixed equations derived from bDBP and bSBP is not reliable. Basically, the authors demonstrated in both normotensive and hypertensive patients that in different individuals the bMBP value fluctuates widely between the bDBP and bSBP values; therefore, the relationship between bMBP and bDBP and bSBP is not fixed, predetermined or easily predictable. Secondly, they reported that there are short-term intra-individual variations in the ratio of bMBP to bSBP and bDBP. That is, in each individual, this relationship may change in relation to functional elements, such as changes in bBP or HR (e.g., stress-induced), as our own results suggested (
Figure 3). Furthermore, we found that the agreement between invasive bBP and their respective non-invasive measurements (oscillometry) showed significant dependence on the bBP level. Based on this, Grillo et al. proposed that a more accurate estimation of bMBP should be ‘ideally’ based ona pulse waveform analysis, rather than on knowledge of the bSBP and bDBP values (although as they themselves mention, thisis currently difficult in daily clinical practice). In this context, future work should evaluate whether other methods of bMBP determination would allow obtaining bSBP levels closer to those recorded invasively.
Finally, as mentioned, the pattern of differences between invasive and non-invasive bBP levels could vary with age, indicating that (at least in theory) age, as well as other variables (e.g., anthropometric characteristics, sex), could be a confounding factor. Consequently, it would be important to conduct future multicenter studies with a larger number of subjects to assess the impact of age and other potentially confounding variables on the results (e.g., by performing stratification analyses by sex and/or age).






{kind=link}
{kind=link}
{kind=link}