
Association of Coronary Collaterals and Myocardial Salvage Measured by Serial Cardiac Magnetic Resonance Imaging after Acute Myocardial Infarction
 , , ,
, , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Coronary Angiography
2.3. Cardiovascular Magnetic Resonance
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dani, S.S.; Lone, A.N.; Javed, Z.; Khan, M.S.; Khan, M.Z.; Kaluski, E.; Virani, S.S.; Shapiro, M.D.; Cainzos-Achirica, M.; Nasir, K.; et al. Trends in Premature Mortality From Acute Myocardial Infarction in the United States, 1999 to 2019. J. Am. Heart Assoc. 2022, 11, e021682. [Google Scholar] [CrossRef]
- Greulich, S.; Mayr, A.; Gloekler, S.; Seitz, A.; Birkmeier, S.; Schäufele, T.; Bekeredjian, R.; Zuern, C.S.; Seizer, P.; Geisler, T.; et al. Time-Dependent Myocardial Necrosis in Patients With ST-Segment–Elevation Myocardial Infarction Without Angiographic Collateral Flow Visualized by Cardiac Magnetic Resonance Imaging: Results From the Multicenter STEMI-SCAR Project. J. Am. Heart Assoc. 2019, 8, e012429. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; Aletras, A.H.; Arai, A.E.; Arheden, H.; Bax, J.; Berry, C.B.-D.C. Cardiac MRI Endpoints in Myocardial Infarction Experimental and Clinical Trials. J. Am. Coll. Cardiol. 2019, 74, 238–256. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Jiménez, R.; Galán-Arriola, C.; Sánchez-González, J.; Agüero, J.; López-Martín, G.J.; Gomez-Talavera, S.; Garcia-Prieto, J.; Benn, A.; Molina-Iracheta, A.; Barreiro-Pérez, M.; et al. Effect of Ischemia Duration and Protective Interventions on the Temporal Dynamics of Tissue Composition after Myocardial Infarction. Circ. Res. 2017, 121, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Fulton, W.F.M. Arterial Anastomoses in the Coronary Circulation. Scott. Med. J. 1963, 8, 466–474. [Google Scholar] [CrossRef] [PubMed]
- Seiler, C.; Stoller, M.; Pitt, B.; Meier, P. The Human Coronary Collateral Circulation: Development and Clinical Importance. Eur. Heart J. 2013, 34, 2674–2682. [Google Scholar] [CrossRef] [PubMed]
- Wustmann, K.; Zbinden, S.; Windecker, S.; Meier, B.; Seiler, C. Is There Functional Collateral Flow during Vascular Occlusion in Angiographically Normal Coronary Arteries? Circulation 2003, 107, 2213–2220. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Pérez, J.T.; Lee, D.C.; Meyers, S.N.; Davidson, C.J.; Bonow, R.O.; Wu, E. Determinants of Myocardial Salvage during Acute Myocardial Infarction: Evaluation with a Combined Angiographic and CMR Myocardial Salvage Index. JACC Cardiovasc. Imaging 2010, 3, 491–500. [Google Scholar] [CrossRef]
- Alsanjari, O.; Chouari, T.; Williams, T.; Myat, A.; Sambu, N.; Blows, L.; Cockburn, J.; de Belder, A.; Hildick-Smith, D. Angiographically Visible Coronary Artery Collateral Circulation Improves Prognosis in Patients Presenting with Acute ST Segment-Elevation Myocardial Infarction. Catheter. Cardiovasc. Interv. 2020, 96, 528–533. [Google Scholar] [CrossRef]
- Meier, P.; Hemingway, H.; Lansky, A.J.; Knapp, G.; Pitt, B.; Seiler, C. The Impact of the Coronary Collateral Circulation on Mortality: A Meta-Analysis. Eur. Heart J. 2012, 33, 614–621. [Google Scholar] [CrossRef]
- Buchner, S.; Eglseer, M.; Debl, K.; Hetzenecker, A.; Luchner, A.; Husser, O.; Stroszczynski, C.; Hamer, O.W.; Fellner, C.; Zeman, F.; et al. Sleep Disordered Breathing and Enlargement of the Right Heart after Myocardial Infarction. Eur. Respir. J. 2015, 45, 680–690. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.; Rentrop, K.P. Limitation of Myocardial Ischemia by Collateral Circulation during Sudden Controlled Coronary Artery Occlusion in Human Subjects: A Prospective Study. Circulation 1986, 74, 469–476. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Buchner, S.; Satzl, A.; Debl, K.; Hetzenecker, A.; Luchner, A.; Husser, O.; Hamer, O.W.; Poschenrieder, F.; Fellner, C.; Zeman, F.; et al. Impact of Sleep-Disordered Breathing on Myocardial Salvage and Infarct Size in Patients with Acute Myocardial Infarction. Eur. Heart J. 2014, 35, 192–199. [Google Scholar] [CrossRef]
- O’Donnell, T.; Dikici, E.; Setser, R.; White, R.D. Tracking and Analysis of Cine-Delayed Enhancement MR. In Lecture Notes in Computer Science, Proceedings of the Medical Image Computing and Computer-Assisted Intervention—MICCAI 2005, 8th International Conference, Palm Springs, CA, USA, 26–29 October 2005; Springer: Berlin/Heidelberg, Germany, 2005; Volume 8, pp. 692–700. [Google Scholar] [CrossRef]
- Kim, H.W.; Farzaneh-Far, A.; Kim, R.J. Cardiovascular Magnetic Resonance in Patients with Myocardial Infarction: Current and Emerging Applications. J. Am. Coll. Cardiol. 2009, 55, 1–16. [Google Scholar] [CrossRef]
- Eitel, I.; Friedrich, M.G. T2-Weighted Cardiovascular Magnetic Resonance in Acute Cardiac Disease. J. Cardiovasc. Magn. Reson. Off. J. Soc. Cardiovasc. Magn. Reson. 2011, 13, 13. [Google Scholar] [CrossRef] [PubMed]
- Carbone, I.; Childs, H.; Mikami, Y.; Ferreira, V.M.; Eitel, I.; Friedrich, M.G. Standardizing T2 Measurements for the Quantitative Assessment of Regional Myocardial Edema. J. Cardiovasc. Magn. Reson. 2011, 13, P121. [Google Scholar] [CrossRef]
- Desch, S.; Eitel, I.; Schmitt, J.; Sareban, M.; Fuernau, G.; Schuler, G.; Thiele, H. Effect of Coronary Collaterals on Microvascular Obstruction as Assessed by Magnetic Resonance Imaging in Patients With Acute ST-Elevation Myocardial Infarction Treated by Primary Coronary Intervention. Am. J. Cardiol. 2009, 104, 1204–1209. [Google Scholar] [CrossRef]
- Lønborg, J.; Kelbæk, H.; Vejlstrup, N.; Bøtker, H.E.; Kim, W.Y.; Holmvang, L.; Jørgensen, E.; Helqvist, S.; Saunamäki, K.; Thuesen, L.; et al. Influence of Pre- Infarction Angina, Collateral Flow, and Pre-Procedural TIMI Flow on Myocardial Salvage Index by Cardiac Magnetic Resonance in Patients with ST-Segment Elevation Myocardial Infarction. Eur. Heart J. Cardiovasc. Imaging 2012, 13, 433–443. [Google Scholar] [CrossRef]
- Kim, E.K.; Choi, J.H.; Song, Y.B.; Hahn, J.Y.; Chang, S.A.; Park, S.J.; Lee, S.C.; Choi, S.H.; Choe, Y.H.; Park, S.W.; et al. A Protective Role of Early Collateral Blood Flow in Patients with ST-Segment Elevation Myocardial Infarction. Am. Heart J. 2016, 171, 56–63. [Google Scholar] [CrossRef]
- Yoon, S.J.; Ko, Y.G.; Kim, J.S.; Moon, J.Y.; Kim, Y.J.; Park, S.; Ha, J.W.; Choi, D.; Jang, Y.; Chung, N.; et al. Impact of Coronary Artery Collaterals on Infarct Size Assessed by Serial Cardiac Magnetic Resonance Imaging after Primary Percutaneous Coronary Intervention in Patients with Acute Myocardial Infarction. Coron. Artery Dis. 2009, 20, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Eitel, I.; Desch, S.; Fuernau, G.; Hildebrand, L.; Gutberlet, M.; Schuler, G.; Thiele, H. Prognostic Significance and Determinants of Myocardial Salvage Assessed by Cardiovascular Magnetic Resonance in Acute Reperfused Myocardial Infarction. J. Am. Coll. Cardiol. 2010, 55, 2470–2479. [Google Scholar] [CrossRef] [PubMed]
- Reto, B.M.; Seiler, C. The Human Coronary Collateral Circulation, Its Extracardiac Anastomoses and Their Therapeutic Promotion. Int. J. Mol. Sci. 2019, 20, 3726. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the Management of Acute Myocardial Infarction in Patients Presenting with ST-Segment Elevation. Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients | CRS 0–1 | CRS 2–3 | ||
|---|---|---|---|---|
| (n = 36) | (n = 28) | (n = 8) | p Value | |
| Age, years | 56 (±9) | 55 (±9) | 57 (±10) | 0.57 |
| Male gender, n (%) | 29 (80.6) | 24 (86) | 5 (63) | 0.17 |
| BMI, kg/m2 | 28.1 (±3.4) | 29 (±3) | 27 (±3) | 0.16 |
| Systolic blood pressure, mmHg | 128 (±23) | 128 (±25) | 128 (±18) | 0.99 |
| Diastolic blood pressure, mmHg | 79 (±13) | 80 (±14) | 77 (±7) | 0.55 |
| Heart rate, bpm | 67 (59–78) | 67 (59–78) | 68 (63–77) | 0.76 |
| Arterial hypertension, n (%) | 19 (53) | 16 (57) | 3 (38) | 0.43 |
| Diabetes mellitus, n (%) | 6 (17) | 5 (18) | 1 (13) | 1.00 |
| History of smoking, n (%) | 26 (72) | 20 (71) | 6 (75) | 1.00 |
| Pre-infarction angina (CCS I-IV), n (%) | 6 (16.7) | 4 (17) | 2 (33) | 0.58 |
| AHI,/h | 8 (4–23) | 14 (4–28) | 6 (4–9) | 0.20 |
| Troponin I before PCI, ng/mL | 2.54 (0.03–17.25) | 2.66 (0.02–23.25) | 2.53 (0.05–5.54) | 0.90 |
| CK-MB max, U/L | 37 (±21) | 38 (±22) | 31 (±4) | 0.60 |
| NT-proBNP max, pg/mL | 897 (497–1406) | 721 (240–1239) | 897 (505–1442) | 0.28 |
| LDL, mg/dL | 117 (±24) | 119 (±22) | 111 (±32) | 0.38 |
| Creatinine, mg/dL | 0.98 (±0.25) | 0.89 (±0.21) | 1.06 (±0.54) | 0.40 |
| eGFR, mL/min/1.73 m2 | 89 (±19) | 92 (±16) | 78 (±26) | 0.07 |
| CRP, mg/L | 4.4 (1.9–13.5) | 4.8 (2.4–14.7) | 2 (0.9–9.8) | 0.16 |
| STEMI, n (%) | 31 (86) | 24 (86) | 7 (86) | 1.00 |
| Multivessel disease, n (%) | 15 (42) | 10 (36) | 5 (63) | 0.24 |
| Chronic total occlusion, n (%) | 0 (0) | 0 (0) | 0 (0) | 1.00 |
| Culprit vessel | <0.001 | |||
| LAD, n (%) | 14 (39) | 14 (50) | 0 | |
| LCX, n (%) | 9 (25) | 9 (32) | 0 | |
| RCA, n (%) | 13 (36) | 5 (18) | 8 (100) | |
| Culprit lesion location | 0.59 | |||
| Proximal, n (%) | 17 (47) | 12 (43) | 5 (62.5) | |
| Medial, n (%) | 13 (36) | 11 (39) | 2 (25) | |
| Distal, n (%) | 3 (8) | 2 (7) | 1 (12.5) | |
| Side branch, n (%) | 3 (8) | 3 (11) | 0 | |
| TIMI flow before PCI | 0.57 | |||
| TIMI 0, n (%) | 31 (86) | 23 (82) | 8 (100) | |
| TIMI 1, n (%) | 5 (14) | 5 (18) | 0 | |
| TIMI flow after PCI | 1.00 | |||
| TIMI 2, n (%) | 3 (8) | 3 (11) | 0 | |
| TIMI 3, n (%) | 33 (92) | 25 (89) | 8 (100) | |
| Pain-to-balloon time, min | 234 (170–487) | 234 (170–603) | 254 (167–381) | 0.72 |
| ST deviation, mV | 0.11 (0.08–0.17) | 0.12 (0.08–0.19) | 0.09 (0.04–0.13) | 0.15 |
| Glycoprotein IIb/IIIa inhibitor, n (%) | 31 (86) | 23 (82) | 8 (100) | 0.57 |
| Thrombus aspiration, n (%) | 19 (53) | 15 (54) | 4 (50) | 1.00 |
| CRS 0–1 | CRS 2–3 | ||
|---|---|---|---|
| (n = 28) | (n = 8) | p Value | |
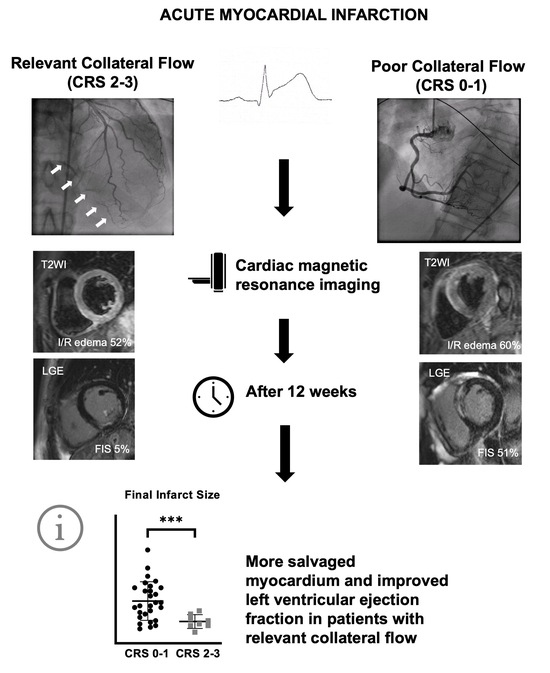
| Infarct size at baseline, % | 23 (±11) | 14 (±5) | 0.004 |
| Final infarct size, % | 20 (±12) | 7 (±4) | <0.001 |
| I/R edema at baseline, % | 44 (±12) | 36 (±11) | 0.098 |
| Myocardial salvage index, % | 57 (±19) | 78 (14) | 0.006 |
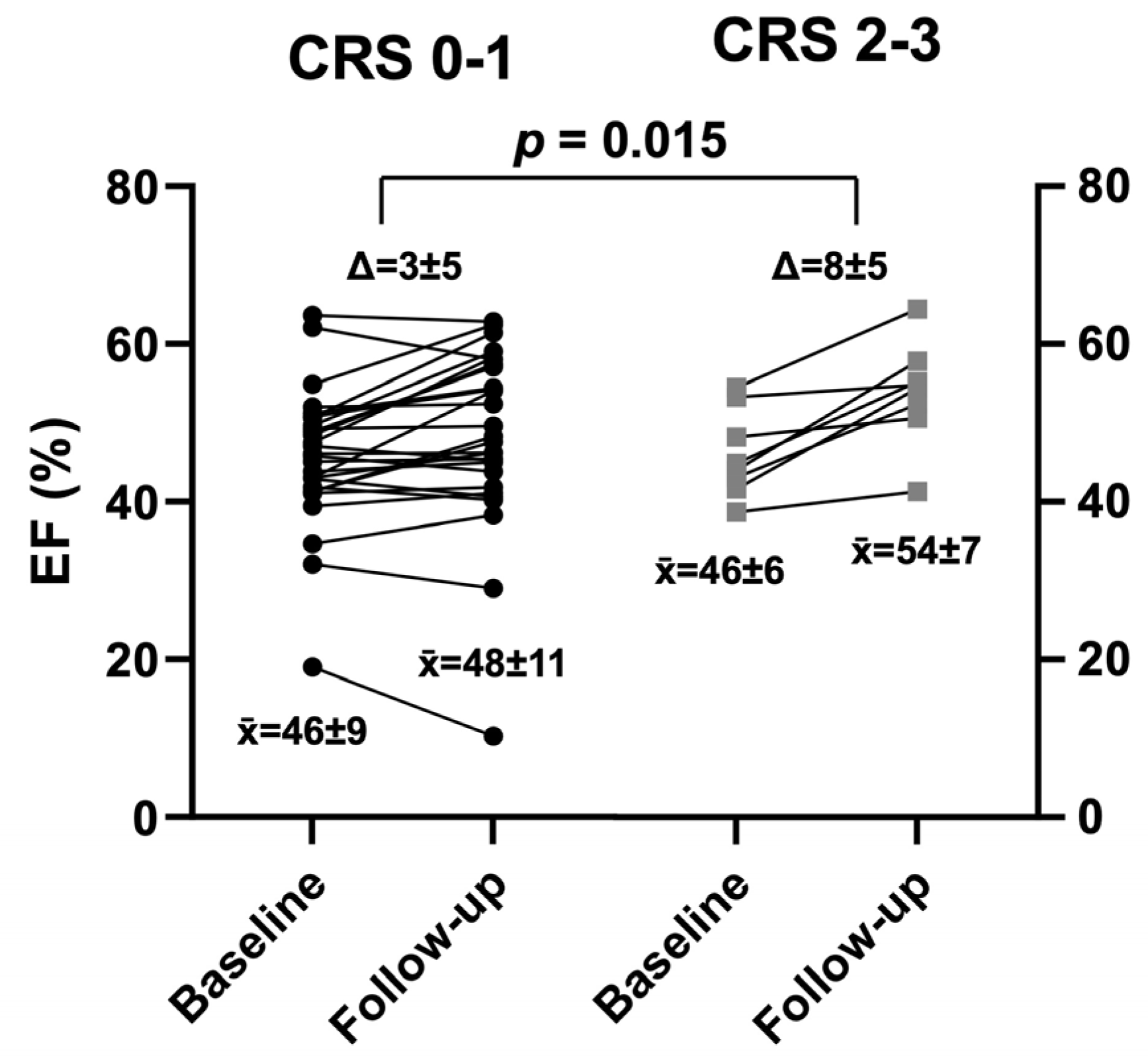
| Left ventricular ejection fraction | |||
| EF at baseline, % | 46 (±9) | 46 (±6) | 0.89 |
| EF at follow-up, % | 48 (±11) | 54 (±7) | 0.18 |
| Difference between baseline and follow-up | |||
| Infarct size, % | −3 (±5) | −7 (±5) | 0.051 |
| EF, % | 3 (±5) | 8 (±5) | 0.015 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pec, J.; Buchner, S.; Wester, M.; Debl, K.; Hamer, O.W.; Poschenrieder, F.; Maier, L.S.; Arzt, M.; Stadler, S. Association of Coronary Collaterals and Myocardial Salvage Measured by Serial Cardiac Magnetic Resonance Imaging after Acute Myocardial Infarction. J. Cardiovasc. Dev. Dis. 2023, 10, 473. https://doi.org/10.3390/jcdd10120473
Pec J, Buchner S, Wester M, Debl K, Hamer OW, Poschenrieder F, Maier LS, Arzt M, Stadler S. Association of Coronary Collaterals and Myocardial Salvage Measured by Serial Cardiac Magnetic Resonance Imaging after Acute Myocardial Infarction. Journal of Cardiovascular Development and Disease. 2023; 10(12):473. https://doi.org/10.3390/jcdd10120473
Chicago/Turabian StylePec, Jan, Stefan Buchner, Michael Wester, Kurt Debl, Okka W. Hamer, Florian Poschenrieder, Lars S. Maier, Michael Arzt, and Stefan Stadler. 2023. "Association of Coronary Collaterals and Myocardial Salvage Measured by Serial Cardiac Magnetic Resonance Imaging after Acute Myocardial Infarction" Journal of Cardiovascular Development and Disease 10, no. 12: 473. https://doi.org/10.3390/jcdd10120473