
Validating Knee Varus Alignment Measurements Using Markerless Motion Capture

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Subject
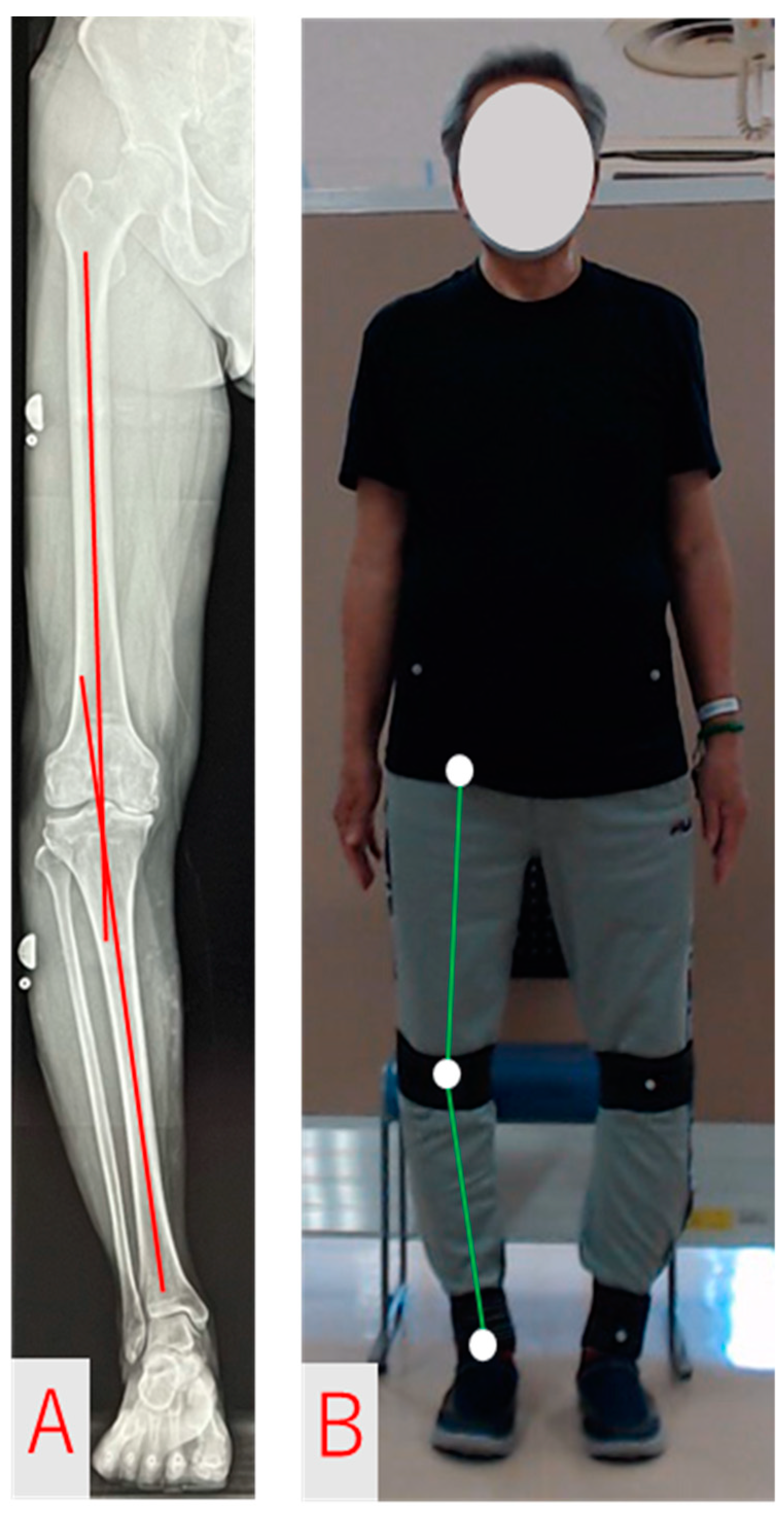
2.3. FTA Measurement and Analysis Methods
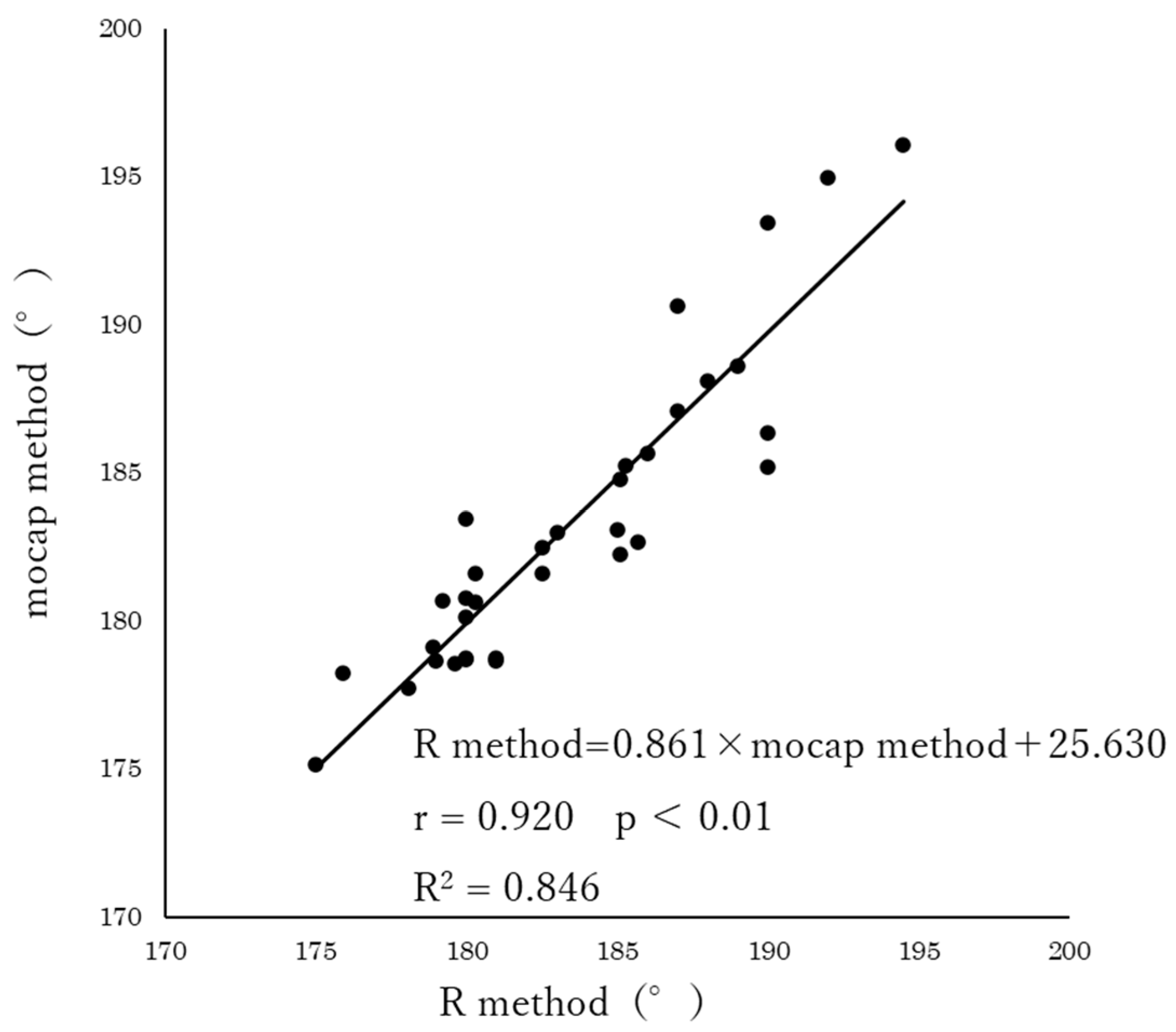
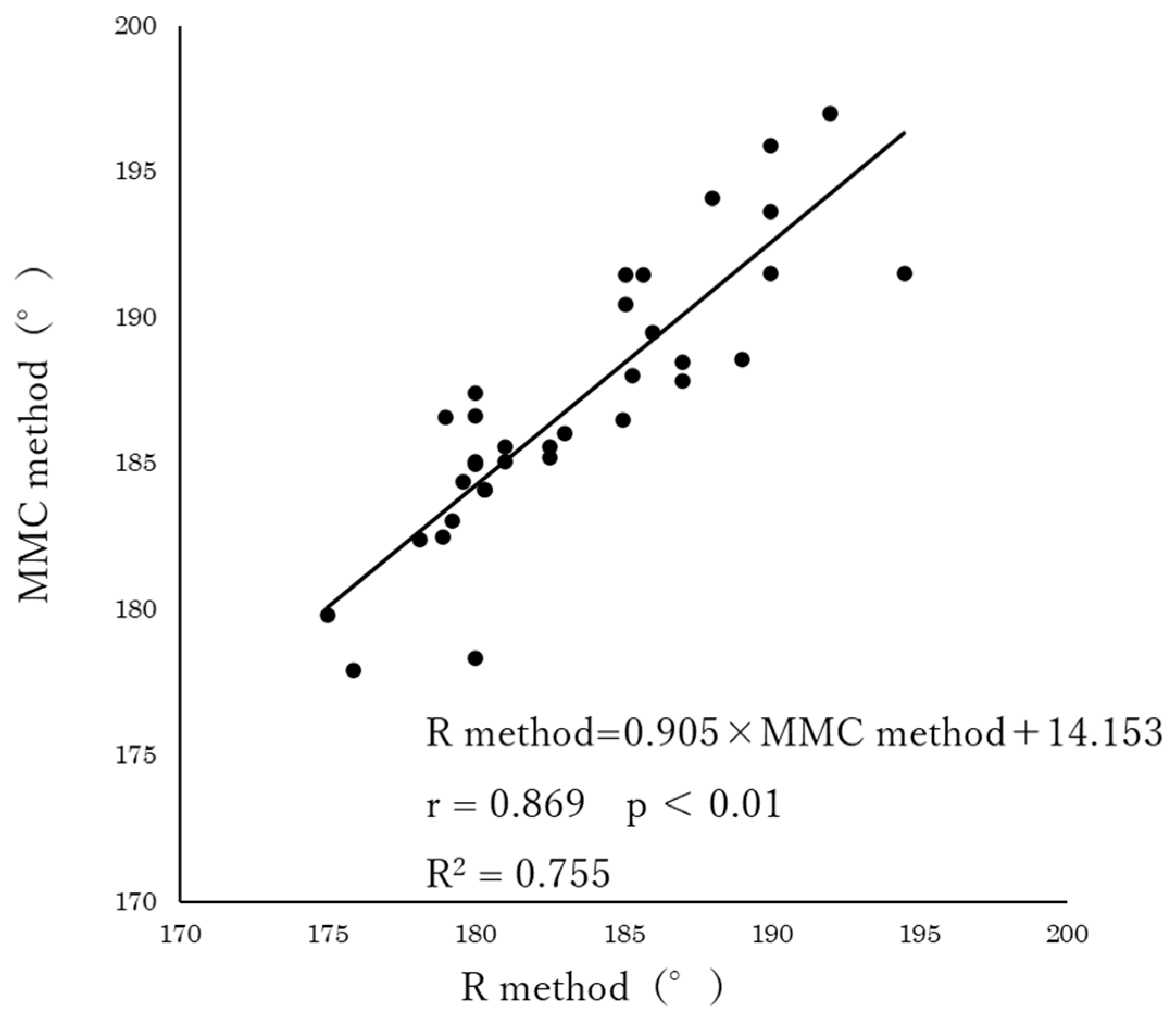
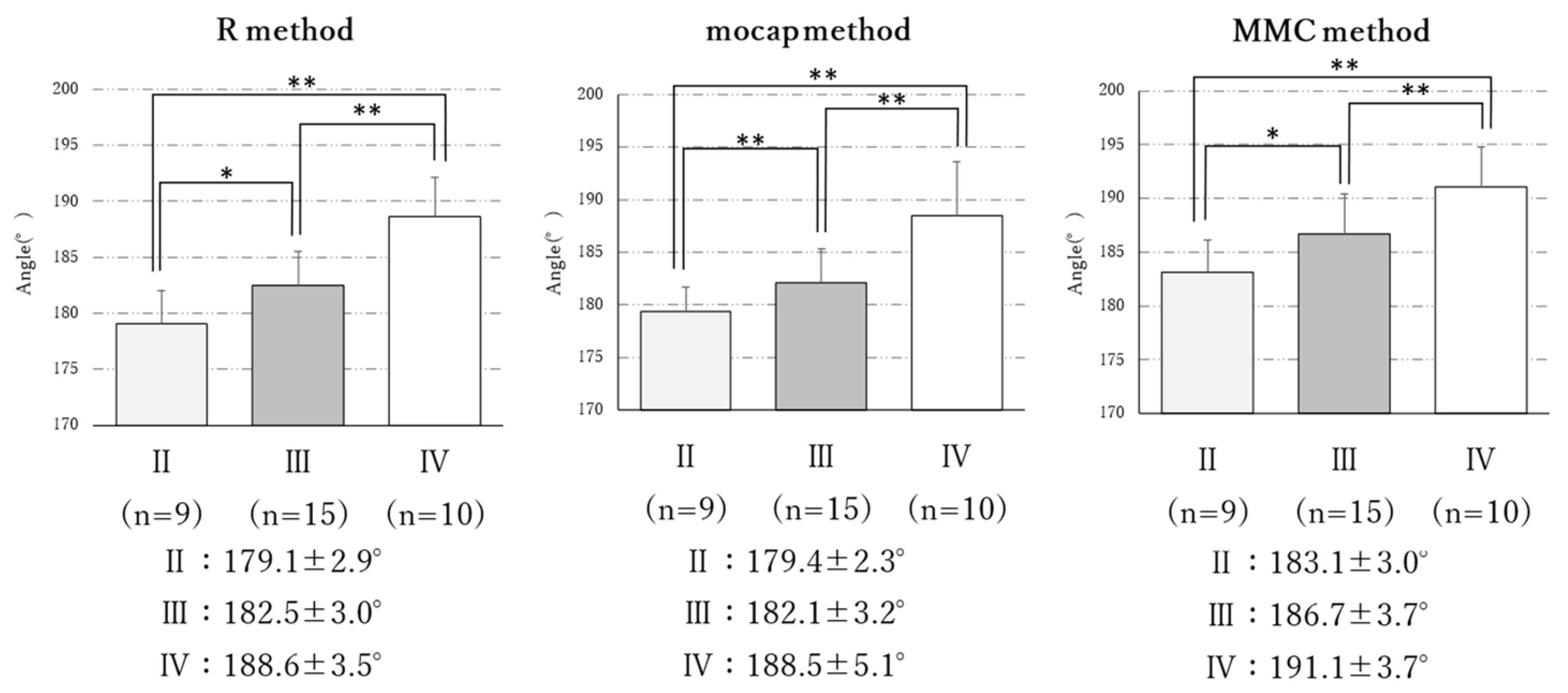
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grotle, M.; Hagen, K.B.; Natvig, B.; Dahl, F.A.; Kvien, T.K. Prevalence and burden of osteoarthritis: Results from a population survey in Norway. J. Rheumatol. 2008, 35, 677–684. [Google Scholar] [PubMed]
- Wang, S.; Wang, S.; Pillinger, M.H.; Krasnokutsky, S.; Barbour, K.E. The association between asymptomatic hyperuricemia and knee osteoarthritis: Data from the third National Health and Nutrition Examination Survey. Osteoarthr. Cartil. 2019, 27, 1301–1308. [Google Scholar] [CrossRef] [PubMed]
- Muraki, S.; Akune, T.; Oka, H.; Ishimoto, Y.; Nagata, K.; Yoshida, M.; Tokimura, F.; Nakamura, K.; Kawaguchi, H.; Yoshimura, N. Incidence and risk factors for radiographic knee osteoarthritis and knee pain in Japanese men and women: A longitudinal population-based cohort study. Arthritis Rheum. 2012, 64, 1447–1456. [Google Scholar] [CrossRef] [PubMed]
- Øiestad, B.E.; White, D.K.; Booton, R.D.; Niu, J.; Zhang, Y.; Torner, J.C.; Lewis, C.E.; Nevitt, M.C.; LaValley, M.P.; Felson, D.T. Longitudinal Course of Physical Function in People with Symptomatic Knee Osteoarthritis: Data from the Multicenter Osteoarthritis Study and the Osteoarthritis Initiative. Arthritis Care Res. 2016, 68, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Vitaloni, M.; Botto-van Bemden, A.; Sciortino Contreras, R.M.; Scotton, D.; Bibas, M.; Quintero, M.; Monfort, J.; Carné, X.; de Abajo, F.J.; Oswald, E.; et al. Global management of patients with knee osteoarthritis begins with quality of life assessment: A systematic review. BMC Musculoskelet. Disord. 2019, 20, 493. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, N.; Muraki, S.; Nakamura, K.; Tanaka, S. Epidemiology of the locomotive syndrome: The research on osteoarthritis/osteoporosis against disability study 2005–2015. Mod. Rheumatol. 2017, 27, 1–7. [Google Scholar] [CrossRef] [PubMed]
- King, L.K.; Kendzerska, T.; Waugh, E.J.; Hawker, G.A. Impact of Osteoarthritis on Difficulty Walking: A Population-Based Study. Arthritis Care Res. 2018, 70, 71–79. [Google Scholar] [CrossRef]
- Turkiewicz, A.; Kiadaliri, A.A.; Englund, M. Cause-specific mortality in osteoarthritis of peripheral joints. Osteoarthr. Cartil. 2019, 27, 848–854. [Google Scholar] [CrossRef]
- Hsu, P.-S.; Lin, H.-H.; Li, C.-R.; Chung, W.-S.; Chung, W.-S.; Chung, W.-S. Increased risk of stroke in patients with osteoarthritis: A population-based cohort study. Osteoarthr. Cartil. 2017, 25, 1026–1031. [Google Scholar] [CrossRef]
- Bedson, J.; Mottram, S.; Thomas, E.; Peat, G. Knee pain and osteoarthritis in the general population: What influences patients to consult? Fam. Pract. 2007, 24, 443–453. [Google Scholar] [CrossRef]
- Matsumoto, T.; Hashimura, M.; Takayama, K.; Ishida, K.; Kawakami, Y.; Matsuzaki, T.; Nakano, N.; Matsushita, T.; Kuroda, R.; Kurosaka, M. A radiographic analysis of alignment of the lower extremities–initiation and progression of varus-type knee osteoarthritis. Osteoarthr. Cartil. 2015, 23, 217–223. [Google Scholar] [CrossRef]
- Sharma, L.; Song, J.; Dunlop, D.D.; Felson, D.T.; Lewis, C.E.; Segal, N.A.; Torner, J.C.; Cooke, T.D.V.; Hietpas, J.; Lynch, J.A.; et al. Varus and valgus alignment and incident and progressive knee osteoarthritis. Ann. Rheum. Dis. 2010, 69, 1940–1945. [Google Scholar] [CrossRef] [PubMed]
- Sharma, L.; Song, J.; Felson, D.T.; Cahue, S.; Shamiyeh, E.; Dunlop, D.D. The Role of Knee Align-ment in Disease Progression and Functional Decline in Knee Osteoarthritis. JAMA 2001, 286, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Rannou, F.; Poiraudeau, S.; Beaudreuil, J. Role of bracing in the management of knee osteoarthritis. Curr. Opin. Rheumatol. 2010, 22, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Marks, R.; Penton, L. Are foot orthotics efficacious for treating painful medial compartment knee osteoarthritis? A review of the literature. Int. J. Clin. Pract. 2004, 58, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, G.M.; van Tol, A.; Bergink, A.P.; Belo, J.N.; Bernsen, R.M.D.; Reijman, M.; Pols, H.A.P.; Bierma-Zeinstra, S.M.A. Association bet-ween valgus and varus alignment and the development and progression of radiographic osteoarthritis of the knee. Arthritis Rheum. 2007, 56, 1204–1211. [Google Scholar] [CrossRef]
- Issa, S.N.; Dunlop, D.D.; Chang, A.H.; Song, J.; Prasad, P.V.; Guermazi, A.; Peterfy, C.; Cahue, S.; Marshall, M.; Kapoor, D.; et al. Full-limb and knee radiography assessments of varus-valgus alignment and their relationship to osteoarthritis disease features by magnetic resonance imaging. Arthritis Rheum. 2007, 57, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Stief, F.; Feja, Z.; Holder, J.; van Drongelen, S.; Adolf, S.; Braun, S.; Böhm, H.; Meurer, A. Non-invasive determination of frontal plane lower limb alignment using motion capture technique-An alternative for full-length radiographs in young patients treated by a temporary hemi epiphysiodesis? Gait Posture 2020, 79, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Next-System: Vision Pose. Available online: https://www.next-system.com/visionpose (accessed on 15 March 2023).
- Moreland, J.R.; Bassett, L.W.; Hanker, G.J. Radiographic analysis of the axial alignment of the lower extremity. J. Bone Jt. Surg. Am. 1987, 69, 745–749. [Google Scholar] [CrossRef]
- Yang, N.H.; Nayeb-Hashemi, H.; Canavan, P.K.; Canavan, P.K.; Vaziri, A. Effect of frontal plane tibiofemoral angle on the stress and strain at the knee cartilage during the stance phase of gait. J. Orthop. Res. 2010, 28, 1539–1547. [Google Scholar] [CrossRef]
- Saita, Y.; Kobayashi, Y.; Nishio, H.; Wakayama, T.; Fukusato, S.; Uchino, S.; Momoi, Y.; Ikeda, H.; Kaneko, K. Predictors of Effectiveness of Platelet-Rich Plasma Therapy for Knee Osteoarthritis: A Retrospective Cohort Study. J. Clin. Med. 2021, 10, 4514. [Google Scholar] [CrossRef] [PubMed]
- Kraus, V.B.; Vail, T.P.; Worrell, T.W.; McDaniel, G. A comparative assessment of alignment angle of the knee by radiographic and physical examination methods. Arthritis Rheum. 2005, 52, 1730–1735. [Google Scholar] [CrossRef]
- Moyer, R.; Wirth, W.; Eckstein, F. Sensitivity of different measures of frontal plane alignment to medial and lateral joint space narrowing: From the osteoarthritis initiative. Semin. Arthritis Rheum. 2015, 45, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Hinman, R.S.; May, R.L.; Crossley, K.M. Is there an alternative to the full-leg radiograph for determining knee joint alignment in osteoarthritis? Arthritis Rheum. 2006, 55, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Ohnishi, T.; Hida, M.; Nakamura, Y.; Wada, C. Novel method for evaluation of frontal plane knee alignment using bony prominences in patients with osteoarthritis. J. Phys. Ther. Sci. 2018, 30, 1168–1172. [Google Scholar] [CrossRef] [PubMed]
- Todoriki, K.; Kai, Y.; Terao, J.; Mochizuki, H.; Murata, S. Reproducibility and validity of knee joint position estimation using markerless motion capture. Jpn. J. Health Promot. Phys. 2023, 13, 7–11. [Google Scholar] [CrossRef]
- Cerejo, R.; Dunlop, D.D.; Cahue, S.; Channin, D.S.; Song, J.; Sharma, L. The influence of alignment on risk of knee osteoarthritis progression according to baseline stage of disease. Arthritis Rheum. 2002, 46, 2632–2636. [Google Scholar] [CrossRef]
- Teichtahl, A.J.; Cicuttini, F.M.; Janakiramanan, N.; Davis, S.R.; Wluka, A.E.; Wluka, A.E. Static knee alignment and its association with radiographic knee osteoarthritis. Osteoarthr. Cartil. 2006, 14, 958–962. [Google Scholar] [CrossRef]
- Riddle, D.L. Validity of clinical measures of frontal plane knee alignment: Data from the Osteoarthritis Initiative. Man. Ther. 2012, 17, 459–465. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| R Method (A) | Mocap Method (B) | MMC Method (C) | p-Value | Multiple Comparison | |
|---|---|---|---|---|---|
| Measurements | 183.4 ± 4.8 | 183.3 ± 5.1 | 187.1 ± 4.6 | <0.01 | A, B < C ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Todoriki, K.; Kai, Y.; Mukai, S.; Murata, S. Validating Knee Varus Alignment Measurements Using Markerless Motion Capture. Geriatrics 2023, 8, 109. https://doi.org/10.3390/geriatrics8060109
Todoriki K, Kai Y, Mukai S, Murata S. Validating Knee Varus Alignment Measurements Using Markerless Motion Capture. Geriatrics. 2023; 8(6):109. https://doi.org/10.3390/geriatrics8060109
Chicago/Turabian StyleTodoriki, Kensuke, Yoshihiro Kai, Shogo Mukai, and Shin Murata. 2023. "Validating Knee Varus Alignment Measurements Using Markerless Motion Capture" Geriatrics 8, no. 6: 109. https://doi.org/10.3390/geriatrics8060109