
Tongue Strength of Older Adults Requiring Long-Term Care Varies throughout the Day

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
Collection of Participant Data
2.2. Procedure
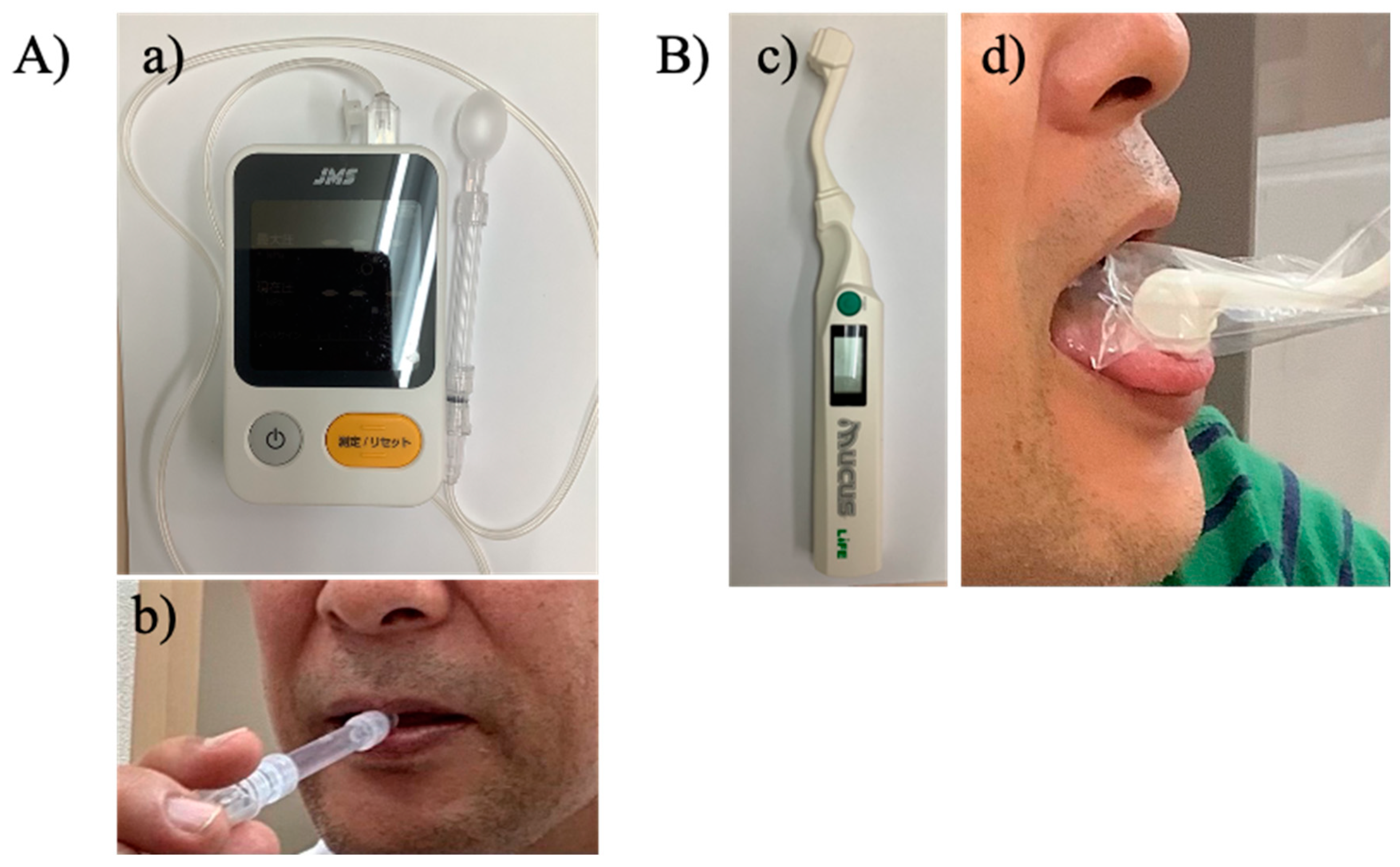
2.3. TS, HGS, and Oral Mucosal Moisture
2.4. Frailty
2.5. Cognitive Function
2.5.1. MMSE
2.5.2. HDS-R
2.6. Statistics
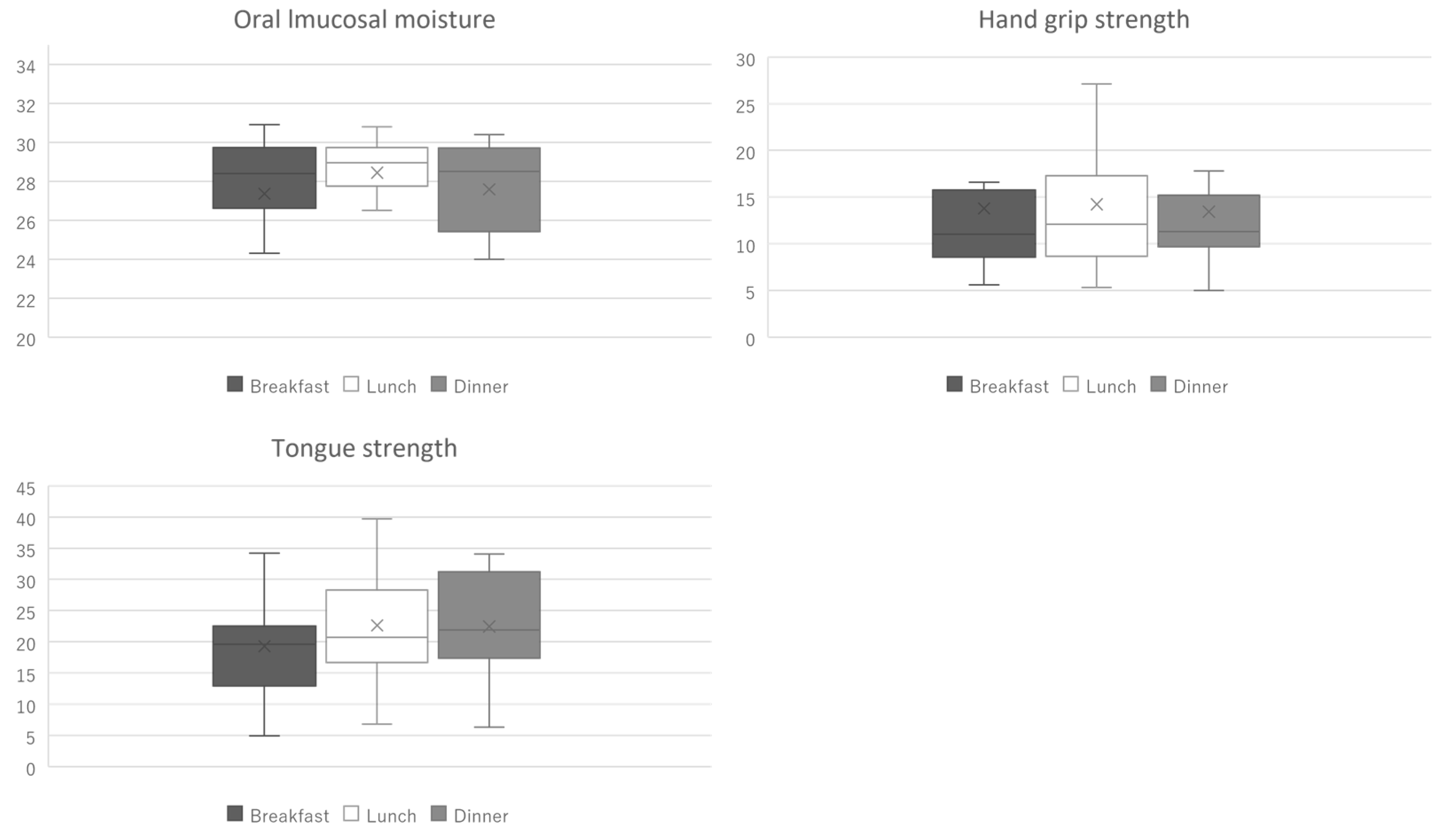
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bass, J.; Takahashi, J.S. Circadian integration of metabolism and energetics. Science 2010, 330, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- Duffy, J.F.; Dijk, D.J.; Klerman, E.B.; Czeisler, C.A. Later endogenous circadian temperature nadir relative to an earlier wake time in older people. Am. J. Physiol. 1998, 275, R1478–R1487. [Google Scholar] [CrossRef]
- Curtis, A.M.; Cheng, Y.; Kapoor, S.; Reilly, D.; Price, T.S.; Fitzgerald, G.A. Circadian variation of blood pressure and the vascular response to asynchronous stress. Proc. Natl Acad. Sci. USA 2007, 104, 3450–3455. [Google Scholar] [CrossRef] [PubMed]
- Perelis, M.; Marcheva, B.; Ramsey, K.M.; Schipma, M.J.; Hutchison, A.L.; Taguchi, A.; Peek, C.B.; Hong, H.; Huang, W.; Omura, C.; et al. Pancreatic β cell enhancers regulate rhythmic transcription of genes controlling insulin secretion. Science 2015, 350, aac4250. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, K.; Kikutani, T.; Tamura, F. Survey of suspected dysphagia prevalence in home-dwelling older people using the 10-Item Eating Assessment Tool (EAT-10). PLoS ONE 2019, 14, e0211040. [Google Scholar] [CrossRef]
- Sura, L.; Madhavan, A.; Carnaby, G.; Crary, M.A. Dysphagia in the elderly: Management and nutritional considerations. Clin. Interv. Aging 2012, 7, 287–298. [Google Scholar] [CrossRef]
- Utanohara, Y.; Hayashi, R.; Yoshikawa, M.; Yoshida, M.; Tsuga, K.; Akagawa, Y. Standard values of maximum tongue pressure taken using newly developed disposable tongue pressure measurement device. Dysphagia 2008, 23, 286–290. [Google Scholar] [CrossRef]
- Limpuangthip, N.; Komin, O.; Tatiyapongpaiboon, T. A simplified method for evaluating swallowing ability and estimating malnutrition risk: A pilot study in older adults. PLoS ONE 2022, 17, e0263896. [Google Scholar] [CrossRef]
- Nagano, A.; Ueshima, J.; Tsutsumiuchi, K.; Inoue, T.; Shimizu, A.; Mori, N.; Maeda, K. Effect of tongue strength on clinical outcomes of patients: A systematic review. Arch. Gerontol. Geriatr. 2022, 102, 104749. [Google Scholar] [CrossRef]
- Arakawa-Kaneko, I.; Watarai, Y.; Schimmel, M.; Abou-Ayash, S. Relationship between tongue pressure and handgrip strength: A systematic review and meta-analysis. J. Oral Rehabil. 2022, 49, 1087–1105. [Google Scholar] [CrossRef]
- Kletzien, H.; Russell, J.A.; Leverson, G.E.; Connor, N.P. Differential effects of targeted tongue exercise and treadmill running on aging tongue muscle structure and contractile properties. J. Appl. Physiol. (1985) 2013, 114, 472–481. [Google Scholar] [CrossRef] [PubMed]
- Nagano, A.; Maeda, K.; Koike, M.; Murotani, K.; Ueshima, J.; Shimizu, A.; Inoue, T.; Sato, K.; Suenaga, M.; Ishida, Y.; et al. Effects of physical rehabilitation and nutritional intake management on improvement in tongue strength in sarcopenic patients. Nutrients 2020, 12, 3104. [Google Scholar] [CrossRef] [PubMed]
- Yokota, J.; Endo, R.; Takahashi, R. Improving physical performance reduces dysphagia via improvement of tongue strength in patients with acute heart failure: A two-wave cross-lagged mediation model analysis. Aging Clin. Exp. Res. 2023, 35, 2237–2246. [Google Scholar] [CrossRef]
- Facer-Childs, E.; Brandstaetter, R. The impact of circadian phenotype and time since awakening on diurnal performance in athletes. Curr. Biol. 2015, 25, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Hiiemae, K.M.; Palmer, J.B. Food transport and bolus formation during complete feeding sequences on foods of different initial consistency. Dysphagia 1999, 14, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Dawes, C. Circadian rhythms in human salivary flow rate and composition. J. Physiol. 1972, 220, 529–545. [Google Scholar] [CrossRef]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. Can. Med. Assoc. J. 2005, 173, 489–495. [Google Scholar] [CrossRef]
- Shimizu, A.; Fujishima, I.; Maeda, K.; Wakabayashi, H.; Nishioka, S.; Ohno, T.; Nomoto, A.; Shigematsu, T.; Kayashita, J.; Japanese Working Group on Sarcopenic Dysphagia. Effect of low tongue pressure on nutritional status and improvement of swallowing function in sarcopenic dysphagia. Nutrition 2021, 90, 111295. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Nakagawa, K.; Yoshimi, K.; Ariya, C.; Nakane, A.; Furuya, J.; Tohara, H. Age-related changes in swallowing muscle intramuscular adipose tissue deposition and related factors. Exp. Gerontol. 2021, 153, 111505. [Google Scholar] [CrossRef]
- Fukushima, Y.; Yoda, T.; Araki, R.; Sakai, T.; Toya, S.; Ito, K.; Funayama, S.; Enoki, Y.; Sato, T. Evaluation of oral wetness using an improved moisture-checking device for the diagnosis of dry mouth. Oral Sci. Int. 2017, 14, 33–36. [Google Scholar] [CrossRef]
- Tsoi, K.K.; Chan, J.Y.; Hirai, H.W.; Wong, S.Y.; Kwok, T.C. Cognitive tests to detect dementia: A systematic review and meta-analysis. JAMA Intern. Med. 2015, 175, 1450–1458. [Google Scholar] [CrossRef]
- Kaufer, D.I.; Williams, C.S.; Braaten, A.J.; Gill, K.; Zimmerman, S.; Sloane, P.D. Cognitive screening for dementia and mild cognitive impairment in assisted living: Comparison of 3 tests. J. Am. Med. Dir. Assoc. 2008, 9, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Katoh, S.; Shimogaki, H.; Onodera, A.; Ueda, H.; Oikawa, K.; Ikeda, K.; Kosaka, A.; Imai, Y.; Hagesawa, K. Development of the revised version of Hasegawa’s Dementia Scale (HDS-R) (in Japanese). Jpn. J. Geriatr. Psychiatry 1991, 2, 1339–1347. [Google Scholar]
- Fujishima, I.; Fujiu-Kurachi, M.; Arai, H.; Hyodo, M.; Kagaya, H.; Maeda, K.; Mori, T.; Nishioka, S.; Oshima, F.; Ogawa, S.; et al. Sarcopenia and dysphagia: Position paper by four professional organizations. Geriatr. Gerontol. Int. 2019, 19, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Pullinger, S.A.; Brocklehurst, E.L.; Iveson, R.P.; Burniston, J.G.; Doran, D.A.; Waterhouse, J.M.; Edwards, B.J. Is there a diurnal variation in repeated sprint ability on a non-motorised treadmill? Chronobiol. Int. 2014, 31, 421–432. [Google Scholar] [CrossRef]
- Kline, C.E.; Durstine, J.L.; Davis, J.M.; Moore, T.A.; Devlin, T.M.; Zielinski, M.R.; Youngstedt, S.D. Circadian variation in swim performance. J. Appl. Physiol. (1985) 2007, 102, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.X.; Seto-Poon, M.; Wheatley, J.R. Breathing route dependence of upper airway muscle activity during hyperpnea. J. Appl. Physiol. (1985) 1998, 84, 1701–1706. [Google Scholar] [CrossRef]
- VanRavenhorst-Bell, H.A.; Mefferd, A.S.; Coufal, K.L.; Scudder, R.; Patterson, J. Tongue strength and endurance: Comparison in active and non-active young and older adults. Int. J. Speech Lang. Pathol. 2017, 19, 77–86. [Google Scholar] [CrossRef]
- Nagayoshi, M.; Higashi, M.; Takamura, N.; Tamai, M.; Koyamatsu, J.; Yamanashi, H.; Kadota, K.; Sato, S.; Kawashiri, S.Y.; Koyama, Z.; et al. Social networks, leisure activities and maximum tongue pressure: Cross-sectional associations in the Nagasaki Islands Study. BMJ 2017, 7, e014878. [Google Scholar] [CrossRef]
- Jawad, B.N.; Petersen, J.; Andersen, O.; Pedersen, M.M. Variations in physical activity and sedentary behavior during and after hospitalization in acutely admitted older medical patients: A longitudinal study. BMC. Geriatr. 2022, 22, 209. [Google Scholar] [CrossRef]
- Sanders, I.; Mu, L.; Amirali, A.; Su, H.; Sobotka, S. The human tongue slows down to speak: Muscle fibers of the human tongue. Anat. Rec. 2013, 296, 1615–1627. [Google Scholar] [CrossRef] [PubMed]
- Monemi, M.; Eriksson, P.O.; Eriksson, A.; Thornell, L.E. Adverse changes in fibre type composition of the human masseter versus biceps brachii muscle during aging. J. Neurol. Sci. 1998, 154, 35–48. [Google Scholar] [CrossRef] [PubMed]
- Ciciliot, S.; Rossi, A.C.; Dyar, K.A.; Blaauw, B.; Schiaffino, S. Muscle type and fiber type specificity in muscle wasting. Int. J. Biochem. Cell Biol. 2013, 45, 2191–2199. [Google Scholar] [CrossRef] [PubMed]
- Lexell, J.; Taylor, C.C.; Sjöström, M. What is the cause of the ageing atrophy? Total number, size and proportion of different fiber types studied in whole vastus lateralis muscle from 15- to 83-year-old men. J. Neurol. Sci. 1988, 84, 275–294. [Google Scholar] [CrossRef] [PubMed]
- Andrews, J.L.; Zhang, X.; McCarthy, J.J.; McDearmon, E.L.; Hornberger, T.A.; Russell, B.; Campbell, K.S.; Arbogast, S.; Reid, M.B.; Walker, J.R.; et al. CLOCK and BMAL1 regulate MyoD and are necessary for maintenance of skeletal muscle phenotype and function. Proc. Natl. Acad. Sci. USA 2010, 107, 19090–19095. [Google Scholar] [CrossRef]
- Fischer, D.; Ship, J.A. Effect of age on variability of parotid salivary gland flow rates over time. Age Ageing 1999, 28, 557–561. [Google Scholar] [CrossRef]
- O’Day, C.; Frank, E.; Montgomery, A.; Nichols, M.; McDade, H. Repeated tongue and hand strength measurements in normal adults and individuals with Parkinson’s disease. Int. J. Orofac. Myol. 2005, 31, 15–25. [Google Scholar] [CrossRef]
- Wu, X.S.; Miles, A.; Braakhuis, A. Texture-modified diets, nutritional status and mealtime satisfaction: A systematic review. Healthcare 2021, 9, 624. [Google Scholar] [CrossRef]
- Smaoui, S.; Langridge, A.; Steele, C.M. The effect of lingual resistance training interventions on adult swallow function: A systematic review. Dysphagia 2020, 35, 745–761. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Factor | Category | Oral Mucosal Moisture (n = 12 Individuals) | Hand Grip Strength (Kg) (n = 13 Individuals) | Tongue Strength (kPa) (n = 12 Individuals) |
|---|---|---|---|---|
| Coefficient (95% CI) | Coefficient (95% CI) | Coefficient (95% CI) | ||
| Time | morning | Reference | Reference | Reference |
| noon | 1.083 (−1.764–3.930) | 0.438 (−1.122–1.999) | 3.065 (1.257–4.873) * | |
| evening | 0.225 (−1.934–2.384) | −0.362 (−2.122–1.399) | 2.600 (−0.095–5.295) | |
| Sex | women | Reference | Reference | Reference |
| men | −1.896 (−3.399–−0.392) * | 11.284 (1.843–20.725) * | 4.017 (−7.145–15.178) | |
| Age | −0.135 (−0.268–0.001) * | −0.241 (−0.491–0.008) | −0.349 (−0.846–0.148) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshinaka, S.; Yamaguchi, K.; Yanagida, R.; Ishii, M.; Nakagawa, K.; Yoshimi, K.; Nakane, A.; Matsuyama, Y.; Aida, J.; Tohara, H. Tongue Strength of Older Adults Requiring Long-Term Care Varies throughout the Day. Geriatrics 2023, 8, 107. https://doi.org/10.3390/geriatrics8060107
Yoshinaka S, Yamaguchi K, Yanagida R, Ishii M, Nakagawa K, Yoshimi K, Nakane A, Matsuyama Y, Aida J, Tohara H. Tongue Strength of Older Adults Requiring Long-Term Care Varies throughout the Day. Geriatrics. 2023; 8(6):107. https://doi.org/10.3390/geriatrics8060107
Chicago/Turabian StyleYoshinaka, Shin, Kohei Yamaguchi, Ryosuke Yanagida, Miki Ishii, Kazuharu Nakagawa, Kanako Yoshimi, Ayako Nakane, Yusuke Matsuyama, Jun Aida, and Haruka Tohara. 2023. "Tongue Strength of Older Adults Requiring Long-Term Care Varies throughout the Day" Geriatrics 8, no. 6: 107. https://doi.org/10.3390/geriatrics8060107