
Waist Circumference as a Risk Factor for Non-Alcoholic Fatty Liver Disease in Older Adults in Guayaquil, Ecuador



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
- Mild (Grade 1): slight, diffuse increase in fine echoes in liver parenchyma with normal visualization of diaphragm and intrahepatic vessel borders;
- Moderate (Grade 2): moderate, diffuse increase in fine echoes with slightly impaired visualization of intrahepatic vessels and diaphragm;
- Severe (Grade 3): marked increase in fine echoes with poor or non-visualization of the intrahepatic vessel borders, diaphragm, and posterior right lobe of the liver.
2.3. Statistical Analysis
3. Results
3.1. Participants
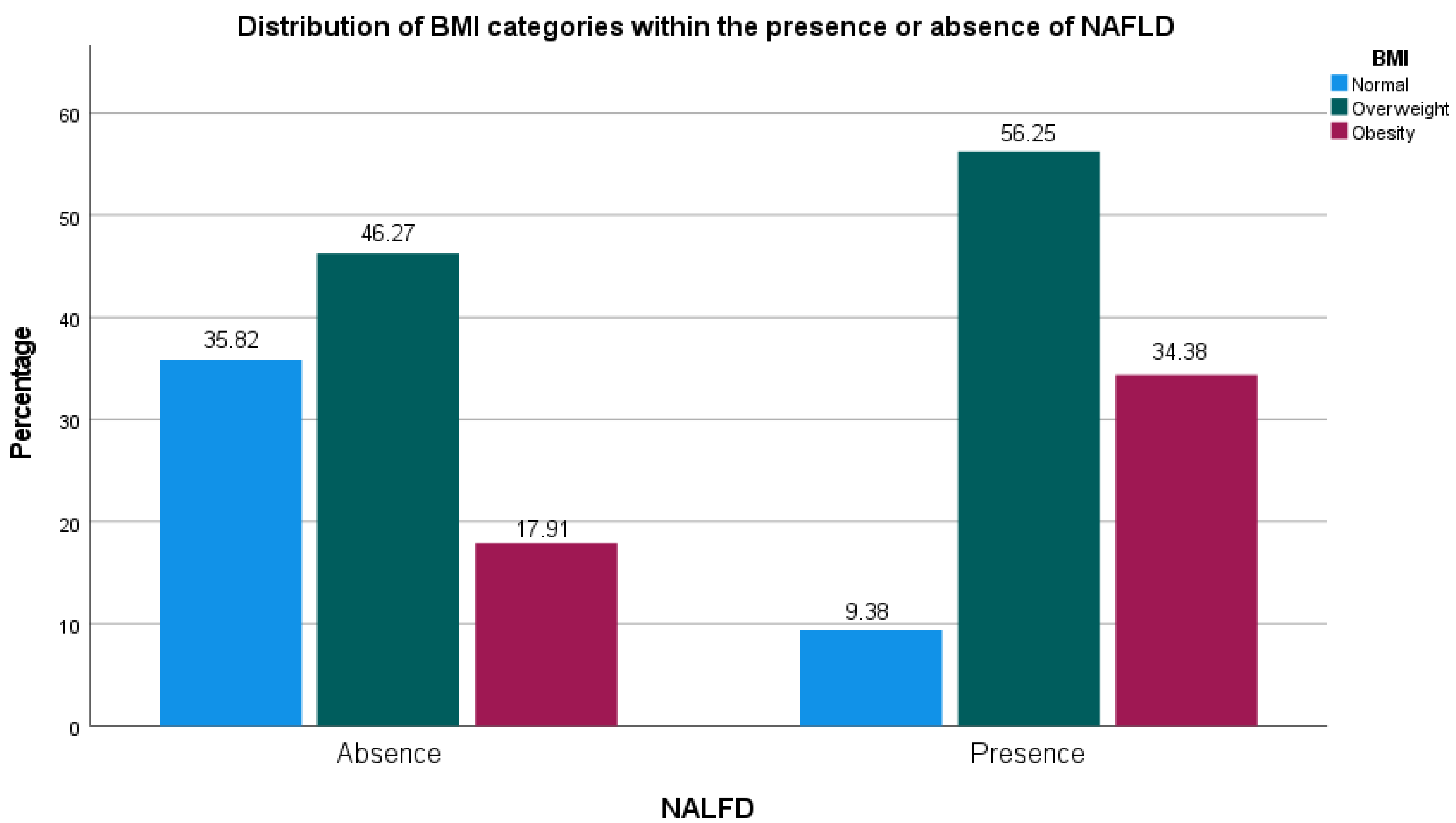
3.2. Association of Variables with NAFLD
3.3. Logistic Regression Explaining the Absence or Presence of NAFLD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ludwig, J.; Viggiano, T.R.; McGill, D.B.; Oh, B.J. Nonalcoholic Steatohepatitis: Mayo Clinic Experiences with a Hitherto Unnamed Disease. Mayo Clin. Proc. 1980, 55, 434–438. [Google Scholar]
- Yari, Z.; Hekmatdoost, A. Chapter 20—Dietary Interventions in Fatty Liver. In Dietary Interventions in Gastrointestinal Diseases; Watson, R.R., Preedy, V.R., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 245–255. [Google Scholar] [CrossRef]
- Dharmalingam, M.; Yamasandhi, P.G. Nonalcoholic Fatty Liver Disease and Type 2 Diabetes Mellitus. Indian J. Endocrinol. Metab. 2018, 22, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global Epidemiology of Nonalcoholic Fatty Liver Disease-Meta-Analytic Assessment of Prevalence, Incidence, and Outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moctezuma-Velázquez, C. Current Treatment for Non-Alcoholic Fatty Liver Disease. Rev. Gastroenterol. Mex. 2018, 83, 125–133. [Google Scholar] [CrossRef]
- Alqahtani, S.A.; Schattenberg, J.M. NAFLD in the Elderly. CIA 2021, 16, 1633–1649. [Google Scholar] [CrossRef] [PubMed]
- Perumpail, B.J.; Khan, M.A.; Yoo, E.R.; Cholankeril, G.; Kim, D.; Ahmed, A. Clinical Epidemiology and Disease Burden of Nonalcoholic Fatty Liver Disease. World J. Gastroenterol. 2017, 23, 8263–8276. [Google Scholar] [CrossRef]
- Sapmaz, F.; Uzman, M.; Basyigit, S.; Ozkan, S.; Yavuz, B.; Yeniova, A.; Kefeli, A.; Asilturk, Z.; Nazligül, Y. Steatosis Grade Is the Most Important Risk Factor for Development of Endothelial Dysfunction in NAFLD. Medicine 2016, 95, e3280. [Google Scholar] [CrossRef]
- Gambino, R.; Bugianesi, E.; Rosso, C.; Mezzabotta, L.; Pinach, S.; Alemanno, N.; Saba, F.; Cassader, M. Different Serum Free Fatty Acid Profiles in NAFLD Subjects and Healthy Controls after Oral Fat Load. Int. J. Mol. Sci. 2016, 17, 479. [Google Scholar] [CrossRef] [Green Version]
- Reyes, M.; Cabrera, D.; Alvarado, G. Valoración Integral de Adultos Mayores En Centros Gerontológicos de Guayaquil. Rev. Cienc. Unemi 2017, 10, 116–123. [Google Scholar] [CrossRef] [Green Version]
- Koehler, E.M.; Schouten, J.N.L.; Hansen, B.E.; van Rooij, F.J.A.; Hofman, A.; Stricker, B.H.; Janssen, H.L.A. Prevalence and Risk Factors of Non-Alcoholic Fatty Liver Disease in the Elderly: Results from the Rotterdam Study. J. Hepatol. 2012, 57, 1305–1311. [Google Scholar] [CrossRef]
- Nestlé Nutrition Institute. Mini Nutritional Assessment MNA. Available online: https://www.mna-elderly.com/ (accessed on 18 May 2021).
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J.; IDF Epidemiology Task Force Consensus Group. The Metabolic Syndrome—A New Worldwide Definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef] [PubMed]
- Santos, L.F.; Hernández, G.; Varón Puerta, A.; Beltrán, Ó.; Botero, R.C.; Mejía, G. Enfermedad hepática por infiltración grasa no alcohólica: La nueva pandemia del milenio. Rev. Colomb. Gastroenterol. 2010, 25, 380–398. [Google Scholar]
- Ma, X.; Holalkere, N.-S.; R, A.K.; Mino-Kenudson, M.; Hahn, P.F.; Sahani, D.V. Imaging-Based Quantification of Hepatic Fat: Methods and Clinical Applications. RadioGraphics 2009, 29, 1253–1277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saadeh, S.; Younossi, Z.M.; Remer, E.M.; Gramlich, T.; Ong, J.P.; Hurley, M.; Mullen, K.D.; Cooper, J.N.; Sheridan, M.J. The Utility of Radiological Imaging in Nonalcoholic Fatty Liver Disease. Gastroenterology 2002, 123, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Colombo, M.; Cortez-Pinto, H.; Huang, T.T.-K.; Miller, V.; Ninburg, M.; Schattenberg, J.M.; Seim, L.; Wong, V.W.S.; Zelber-Sagi, S. NAFLD—Sounding the Alarm on a Silent Epidemic. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 377–379. [Google Scholar] [CrossRef]
- Rodríguez, J.H.; Domínguez, Y.A.; Espinal, O.M.M. Prevalence and Trend of Overweight and Obesity in Adults Worldwide. Rev. Cuba. Endoc. 2019, 30. Available online: https://www.medigraphic.com/cgi-bin/new/resumenI.cgi?IDARTICULO=96712# (accessed on 23 September 2020).
- Sheka, A.C.; Adeyi, O.; Thompson, J.; Hameed, B.; Crawford, P.A.; Ikramuddin, S. Nonalcoholic Steatohepatitis: A Review. JAMA 2020, 323, 1175–1183. [Google Scholar] [CrossRef]
- Ballestri, S.; Nascimbeni, F.; Baldelli, E.; Marrazzo, A.; Romagnoli, D.; Lonardo, A. NAFLD as a Sexual Dimorphic Disease: Role of Gender and Reproductive Status in the Development and Progression of Nonalcoholic Fatty Liver Disease and Inherent Cardiovascular Risk. Adv. Ther. 2017, 34, 1291–1326. [Google Scholar] [CrossRef]
- Golabi, P.; Paik, J.; Reddy, R.; Bugianesi, E.; Trimble, G.; Younossi, Z.M. Prevalence and Long-Term Outcomes of Non-Alcoholic Fatty Liver Disease among Elderly Individuals from the United States. BMC Gastroenterol. 2019, 19, 56. [Google Scholar] [CrossRef]
- Chao, Y.-P.; Chen, W.-L.; Peng, T.-C.; Wu, L.-W.; Liaw, F.-Y.; Kao, T.-W. Examining the Association between Muscle Mass, Muscle Function, and Fat Indexes in an Elderly Population. Nutrition 2021, 83, 111071. [Google Scholar] [CrossRef]
- Kupusinac, A.; Stokić, E.; Doroslovački, R. Predicting Body Fat Percentage Based on Gender, Age and BMI by Using Artificial Neural Networks. Comput. Methods Programs Biomed. 2014, 113, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Macek, P.; Terek-Derszniak, M.; Biskup, M.; Krol, H.; Smok-Kalwat, J.; Gozdz, S.; Zak, M. Assessment of Age-Induced Changes in Body Fat Percentage and BMI Aided by Bayesian Modelling: A Cross-Sectional Cohort Study in Middle-Aged and Older Adults. Clin. Interv. Aging 2020, 15, 2301–2311. [Google Scholar] [CrossRef] [PubMed]
- Csak, T.; Ganz, M.; Pespisa, J.; Kodys, K.; Dolganiuc, A.; Szabo, G. Fatty Acid and Endotoxin Activate Inflammasomes in Mouse Hepatocytes That Release Danger Signals to Stimulate Immune Cells. Hepatology 2011, 54, 133–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, J.-H.; Ferrell, L.D.; Tan, V.; Yeh, M.M.; Sarkar, M.; Gill, R.M. Aggressive Non-Alcoholic Steatohepatitis Following Rapid Weight Loss and/or Malnutrition. Mod. Pathol. 2017, 30, 834–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattar, S.G.; Velcu, L.M.; Rabinovitz, M.; Demetris, A.J.; Krasinskas, A.M.; Barinas-Mitchell, E.; Eid, G.M.; Ramanathan, R.; Taylor, D.S.; Schauer, P.R. Surgically-Induced Weight Loss Significantly Improves Nonalcoholic Fatty Liver Disease and the Metabolic Syndrome. Ann. Surg. 2005, 242, 610–617, discussion 618–620. [Google Scholar] [CrossRef] [PubMed]
- Della Pepa, G.; Vetrani, C.; Lombardi, G.; Bozzetto, L.; Annuzzi, G.; Rivellese, A.A. Isocaloric Dietary Changes and Non-Alcoholic Fatty Liver Disease in High Cardiometabolic Risk Individuals. Nutrients 2017, 9, 1065. [Google Scholar] [CrossRef] [Green Version]
- Miller, E.F. Nutrition Management Strategies for Nonalcoholic Fatty Liver Disease: Treatment and Prevention. Clin. Liver Dis. 2020, 15, 144–148. [Google Scholar] [CrossRef]
- Pineda, M.G.; Benítez, A.; Figueredo, R.; Ayala, F.; Argüello, R. Frecuencia de hígado graso no alcohólico diagnosticado por ecografía abdominal en pacientes obesos. An. Fac. Cienc. Méd. 2017, 50, 35–50. [Google Scholar] [CrossRef]
- Albhaisi, S.; Chowdhury, A.; Sanyal, A.J. Non-Alcoholic Fatty Liver Disease in Lean Individuals. JHEP Rep. 2019, 1, 329–341. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-Cruz, A.; Gómez-Miranda, L.M.; Díaz Ramírez, G.; Carvalí Meza, N.Y.; Bacardí-Gascón, M. La Adiposidad Como Factor de Riesgo Del Hígado Graso No Alcohólico: Revisión Sistemática. Nutr. Hosp. 2014, 29, 771–775. [Google Scholar] [CrossRef]
- Meneses Moreno, D.; Negrin Rangel, E. Esteatosis hepática no alcohólica: Relación con la circunferencia de cintura. Gen 2017, 71, 74–80. [Google Scholar]
- Lizardi-Cervera, J.; Laparra, I.B.; Chávez-Tapia, N.C.; Ostos, M.E.R.; Esquivel, M.U. Prevalencia de hígado graso no alcohólico y síndrome metabólico en población asintomática. Rev. Gastroenterol. Mex. 2006, 71, 453–459. [Google Scholar]
- Polyzos, S.A.; Kountouras, J.; Mantzoros, C.S. Obesity and Nonalcoholic Fatty Liver Disease: From Pathophysiology to Therapeutics. Metabolism 2019, 92, 82–97. [Google Scholar] [CrossRef] [PubMed]
- Tchernof, A.; Després, J.-P. Pathophysiology of Human Visceral Obesity: An Update. Physiol. Rev. 2013, 93, 359–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, R.; Neeland, I.J.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; Cuevas, A.; Hu, F.B.; et al. Waist Circumference as a Vital Sign in Clinical Practice: A Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat. Rev. Endocrinol. 2020, 16, 177–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelley, D.E.; McKolanis, T.M.; Hegazi, R.A.F.; Kuller, L.H.; Kalhan, S.C. Fatty Liver in Type 2 Diabetes Mellitus: Relation to Regional Adiposity, Fatty Acids, and Insulin Resistance. Am. J. Physiol. Endocrinol. Metab. 2003, 285, E906–E916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Poorten, D.; Milner, K.-L.; Hui, J.; Hodge, A.; Trenell, M.I.; Kench, J.G.; London, R.; Peduto, T.; Chisholm, D.J.; George, J. Visceral Fat: A Key Mediator of Steatohepatitis in Metabolic Liver Disease. Hepatology 2008, 48, 449–457. [Google Scholar] [CrossRef]
- Cariou, B. The Metabolic Triad of Non-Alcoholic Fatty Liver Disease, Visceral Adiposity and Type 2 Diabetes: Implications for Treatment. Diabetes Obes. Metab. 2022, 24 (Suppl. 2), 15–27. [Google Scholar] [CrossRef]
- Park, B.J.; Kim, Y.J.; Kim, D.H.; Kim, W.; Jung, Y.J.; Yoon, J.H.; Kim, C.Y.; Cho, Y.M.; Kim, S.H.; Lee, K.B.; et al. Visceral Adipose Tissue Area Is an Independent Risk Factor for Hepatic Steatosis. J. Gastroenterol. Hepatol. 2008, 23, 900–907. [Google Scholar] [CrossRef]
- Kim, H.Y.; Baik, S.J.; Lee, H.A.; Lee, B.K.; Lee, H.S.; Kim, T.H.; Yoo, K. Relative Fat Mass at Baseline and Its Early Change May Be a Predictor of Incident Nonalcoholic Fatty Liver Disease. Sci. Rep. 2020, 10, 17491. [Google Scholar] [CrossRef]
- Jones, G.S.; Graubard, B.I.; Alvarez, C.S.; McGlynn, K.A. Prediction of Nonalcoholic Fatty Liver Disease Using Anthropometry and Body Fat Measures by Sex and Race/Ethnicity in the United States. Obesity 2022, 30, 1760–1765. [Google Scholar] [CrossRef] [PubMed]
- Milić, S.; Lulić, D.; Štimac, D. Non-Alcoholic Fatty Liver Disease and Obesity: Biochemical, Metabolic and Clinical Presentations. World J. Gastroenterol. 2014, 20, 9330–9337. [Google Scholar] [CrossRef] [PubMed]
- Yaqub, S.; Ananias, P.; Shah, A.; Luenam, K.; Jose, A.M.; Melo, J.P.; Turkistani, A.; Mohammed, L. Decoding the Pathophysiology of Non-Alcoholic Fatty Liver Disease Progressing to Non-Alcoholic Steatohepatitis: A Systematic Review. Cureus 2021, 13, e18201. [Google Scholar] [CrossRef] [PubMed]
- Fang, H.; Judd, R.L. Adiponectin Regulation and Function. Compr. Physiol. 2018, 8, 1031–1063. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Kusminski, C.M.; Scherer, P.E. Adiponectin, Leptin and Cardiovascular Disorders. Circ. Res. 2021, 128, 136–149. [Google Scholar] [CrossRef]
- Tomono, Y.; Hiraishi, C.; Yoshida, H. Age and Sex Differences in Serum Adiponectin and Its Association with Lipoprotein Fractions. Ann. Clin. Biochem. 2018, 55, 165–171. [Google Scholar] [CrossRef] [Green Version]
- Obata, Y.; Yamada, Y.; Takahi, Y.; Baden, M.Y.; Saisho, K.; Tamba, S.; Yamamoto, K.; Umeda, M.; Furubayashi, A.; Matsuzawa, Y. Relationship between Serum Adiponectin Levels and Age in Healthy Subjects and Patients with Type 2 Diabetes. Clin. Endocrinol. 2013, 79, 204–210. [Google Scholar] [CrossRef]
- Koh, S.J.; Hyun, Y.J.; Choi, S.Y.; Chae, J.S.; Kim, J.Y.; Park, S.; Ahn, C.-M.; Jang, Y.; Lee, J.H. Influence of Age and Visceral Fat Area on Plasma Adiponectin Concentrations in Women with Normal Glucose Tolerance. Clin. Chim. Acta 2008, 389, 45–50. [Google Scholar] [CrossRef]
- Guo, W.; Zhao, X.; Miao, M.; Liang, X.; Li, X.; Qin, P.; Lu, J.; Zhu, W.; Wu, J.; Zhu, C.; et al. Association Between Skeletal Muscle Mass and Severity of Steatosis and Fibrosis in Non-Alcoholic Fatty Liver Disease. Front. Nutr. 2022, 9, 883015. [Google Scholar] [CrossRef]
- Paul, J. Recent Advances in Non-Invasive Diagnosis and Medical Management of Non-Alcoholic Fatty Liver Disease in Adult. Egypt. Liver J. 2020, 10, 37. [Google Scholar] [CrossRef]
- Park, C.C.; Nguyen, P.; Hernandez, C.; Bettencourt, R.; Ramirez, K.; Fortney, L.; Hooker, J.; Sy, E.; Savides, M.T.; Alquiraish, M.H.; et al. Magnetic Resonance Elastography vs Transient Elastography in Detection of Fibrosis and Noninvasive Measurement of Steatosis in Patients With Biopsy-Proven Nonalcoholic Fatty Liver Disease. Gastroenterology 2017, 152, 598–607.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uematsu, T.; Kasami, M.; Kiyohara, Y. B-Mode Ultrasound Imaging, Doppler Imaging, and Real-Time Elastography in Cutaneous Malignant Melanoma and Lymph Node Metastases. Healthcare 2013, 1, 84–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petzold, G. Role of Ultrasound Methods for the Assessment of NAFLD. J. Clin. Med. 2022, 11, 4581. [Google Scholar] [CrossRef] [PubMed]
- Hernaez, R.; Lazo, M.; Bonekamp, S.; Kamel, I.; Brancati, F.L.; Guallar, E.; Clark, J.M. Diagnostic Accuracy and Reliability of Ultrasonography for the Detection of Fatty Liver: A Meta-Analysis. Hepatology 2011, 54, 1082–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baygi, F.; Mohammadi-Nasrabadi, F.; Zyriax, B.-C.; Jensen, O.C.; Bygvraa, D.A.; Oldenburg, M.; Nielsen, J.B. Global Overview of Dietary Outcomes and Dietary Intake Assessment Methods in Maritime Settings: A Systematic Review. BMC Public Health 2021, 21, 1579. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n = 99 | Percentage (%) | ||
|---|---|---|---|
| Sex | Man | 15 | 15.2% |
| Woman | 84 | 84.8% | |
| Age | 71–75 | 20 | 20.2% |
| 76–80 | 45 | 45.5% | |
| 81–85 | 19 | 19.2% | |
| 86–90 | 13 | 13.1% | |
| 91–95 | 2 | 2.0% | |
| NAFLD | Normal | 67 | 67.7% |
| Grade I | 29 | 29.3% | |
| Grade II | 3 | 3.0% | |
| Lives independently | No | 4 | 4.1% |
| Yes | 94 | 95.9% | |
| Complete meals | Two meals | 19 | 19.2% |
| Three meals | 80 | 80.8% | |
| MNA Classification | Well-nourished | 82 | 82.8% |
| Risk of malnutrition | 17 | 17.2% | |
| BMI Classification | Normal | 27 | 27.3% |
| Overweight | 49 | 49.5% | |
| Obesity | 23 | 23.2% | |
| Fat Mass | Athlete | 2 | 2.0% |
| Fitness | 6 | 6.1% | |
| Acceptable | 23 | 23.5% | |
| Obesity | 67 | 68.4% | |
| Normal | NAFLD | p Value | |
|---|---|---|---|
| Mean (SD) | Mean (SD) | ||
| Age | 79.75 (5.12) | 77.69 (3.86) | 0.198 |
| Waist circumference (cm) | 87.50 (8.32) | 94.50 (9.74) | 0.001 * |
| MNA | 26.00 (2.54) | 26.94 (2.64) | 0.152 |
| BMI | 26.36 (3.58) | 28.85 (3.83) | 0.005 * |
| Percentage of fat mass | 31.98 (7.27) | 36.55 (5.67) | 0.009 * |
| Variables | B | Sig. | OR | OR 95% CI | |
|---|---|---|---|---|---|
| Inferior | Superior | ||||
| Age | −0.115 | 0.045 * | 0.892 | 0.797 | 0.998 |
| Waist circumference (cm) | 0.092 | 0.016 * | 1.097 | 1.017 | 1.183 |
| Overweight | 0.473 | 0.565 | 1.605 | 0.321 | 8.036 |
| Obesity | −0.657 | 0.586 | 0.518 | 0.049 | 5.498 |
| Percentage of fat mass | 0.07 | 0.186 | 1.073 | 0.967 | 1.191 |
| Constant | −2.641 | 0.614 | 0.071 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabrera, D.; Moncayo-Rizzo, J.; Cevallos, K.; Alvarado-Villa, G. Waist Circumference as a Risk Factor for Non-Alcoholic Fatty Liver Disease in Older Adults in Guayaquil, Ecuador. Geriatrics 2023, 8, 42. https://doi.org/10.3390/geriatrics8020042
Cabrera D, Moncayo-Rizzo J, Cevallos K, Alvarado-Villa G. Waist Circumference as a Risk Factor for Non-Alcoholic Fatty Liver Disease in Older Adults in Guayaquil, Ecuador. Geriatrics. 2023; 8(2):42. https://doi.org/10.3390/geriatrics8020042
Chicago/Turabian StyleCabrera, Dayana, Jorge Moncayo-Rizzo, Karen Cevallos, and Geovanny Alvarado-Villa. 2023. "Waist Circumference as a Risk Factor for Non-Alcoholic Fatty Liver Disease in Older Adults in Guayaquil, Ecuador" Geriatrics 8, no. 2: 42. https://doi.org/10.3390/geriatrics8020042