
Hypertensive Blood Pressure and Its Impact on Functional Outcomes among Older Adults Receiving Comprehensive Geriatric Care

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Patients
- (1)
- Hospitalization for CGC between May 2019 and April 2020;
- (2)
- 24-h blood pressure monitoring (BPM) during their hospital stay;
- (3)
- Complete documentation of outcome parameters (Barthel index, BI; Tinetti balance and gait test, TBGT; timed up and go test, TUG).
2.2. Comprehensive Geriatric Care (CGC)
2.3. Outcome Parameters
2.3.1. Barthel Index
2.3.2. Tinetti Balance and Gait Test
2.3.3. Timed Up and Go Test
2.4. 24 h Blood Pressure Monitoring
2.5. Data Collection and Statistical Analyses
2.6. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cassell, A.; Edwards, D.; Harshfield, A.; Rhodes, K.; Brimicombe, J.; Payne, R.; Simon, G. The epidemiology of multimorbidity in primary care: A retrospective cohort study. Br. J. Gen. Pract. 2018, 68, 245–251. [Google Scholar] [CrossRef] [Green Version]
- Salisbury, C.; Johnson, L.; Purdy, S.; Valderas, J.M.; Montgomery, A.A. Epidemiology and impact of multimorbidity in primary care: A retrospective cohort study. Br. J. Gen. Pract. 2011, 61, 12–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baztán, J.J.; Suárez-García, F.M.; López-Arrieta, J.; Rodríguez-Mañas, L.; Rodríguez-Artalejo, F. Effectiveness of acute geriatric units on functional decline, living at home, and case fatality among older patients admitted to hospital for acute medical disorders: Meta-analysis. BMJ 2009, 338, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landefeld, C.S.; Palmer, R.M.; Kresevic, D.M.; Fortinsky, R.H.; Kowal, J. A randomized trial of care in a hospital medical unit especially designed to improve the functional outcomes of acutely ill older patients. N. Engl. J. Med. 1995, 332, 1338–1344. [Google Scholar] [CrossRef] [PubMed]
- Prestmo, A.; Hagen, G.; Sletvold, O.; Helbostad, J.L.; Thingstad, P.; Taraldsen, K.; Lydersen, S.; Halsteinli, V.; Saltnes, T.; Lamb, S.E.; et al. Comprehensive geriatric care for patients with hip fractures: A prospective, randomised, controlled trial. Lancet 2015, 385, 1623–1633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taraldsen, K.; Sletvold, O.; Thingstad, P.; Saltvedt, I.; Granat, M.H.; Lydersen, S.; Helbostad, J.L. Physical behavior and function early after hip fracture surgery in patients receiving comprehensive geriatric care or orthopedic care—A randomized controlled trial. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Buford, T.W. Hypertension and aging. Ageing Res. Rev. 2016, 26, 96–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef]
- Paul, S.L.; Sturm, J.W.; Dewey, H.M.; Donnan, G.A.; Macdonell, R.A.L.; Thrift, A.G. Long-term outcome in the North East Melbourne Stroke Incidence Study: Predictors of quality of life at 5 years after stroke. Stroke 2005, 36, 2082–2086. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Shulman, K.I.; Shedletsky, R.; Silver, I.L. The challenge of time: Clock-drawing and cognitive function in the elderly. Int. J. Geriatr. Psychiatry 1986, 1, 135–140. [Google Scholar] [CrossRef]
- Shulman, K.I.; Pushkar Gold, D.; Cohen, C.A.; Zucchero, C.A. Clock-drawing and dementia in the community: A longitudinal study. Int. J. Geriatr. Psychiatry 1993, 8, 487–496. [Google Scholar] [CrossRef]
- Sheikh, J.I.; Yesavage, J.A. Geriatric Depression Scale (GDS): Recent evidence and development of a shorter version. Clin. Gerontol. 1986, 5, 165–173. [Google Scholar]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [PubMed]
- Lübke, N.; Meinck, M.; Von Renteln-Kruse, W. The Barthel Index in geriatrics. A context analysis of the Hamburg Classification Manual. Z. Gerontol. Geriatr. 2004, 37, 316–326. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Tinetti, M.E. Performance-oriented assessment of mobility problems in elderly patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, A.; Oparil, S. Hypertension in Women: Recent Advances and Lingering Questions. Hypertension 2017, 70, 19–26. [Google Scholar] [CrossRef]
- Ettehad, D.; Emdin, C.A.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Blood pressure lowering for prevention of cardiovascular disease and death: A systematic review and meta-analysis. Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef] [Green Version]
- Cautela, J.; Tartiere, J.; Cohen-Solal, A.; Bellemain-Appaix, A.; Theron, A.; Tibi, T.; Januzzi, J.L., Jr.; Roubille, F.; Girerd, N. Management of low blood pressure in ambulatory heart failure with reduced ejection fraction patients. Eur. J. Heart Fail. 2020, 22, 1357–1365. [Google Scholar] [CrossRef]
- Sorrentino, M.J. The Evolution from Hypertension to Heart Failure. Heart Fail. Clin. 2019, 15, 447–453. [Google Scholar] [CrossRef]
- Carlisle, M.A.; Fudim, M.; DeVore, A.D.; Piccini, J.P. Heart Failure and Atrial Fibrillation, Like Fire and Fury. JACC Heart Fail. 2019, 7, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Morbach, C.; Wagner, M.; Güntner, S.; Malsch, C.; Oezkur, M.; Wood, D.; Kotseva, K.; Leyh, R.; Ertl, G.; Karmann, W. Heart failure in patients with coronary heart disease: Prevalence, characteristics and guideline implementation—Results from the German EuroAspire IV cohort. BMC Cardiovasc. Disord. 2017, 17, 108. [Google Scholar] [CrossRef] [PubMed]
- Hogenson, K.D. Acute postoperative hypertension in the hypertensive patient. J. Post Anesth. Nurs. 1992, 7, 38–44. [Google Scholar] [PubMed]
- Meng, L.; Yu, W.; Wang, T.; Zhang, L.; Heerdt, P.M.; Gelb, A.W. Blood Pressure Targets in Perioperative Care. Hypertension 2018, 72, 806–817. [Google Scholar] [CrossRef]
- Saccò, M.; Meschi, M.; Regolisti, G.; Detrenis, S.; Bianchi, L.; Bertorelli, M.; Pioli, S.; Magnano, A.; Spagnoli, F.; Giuri, P.G.; et al. The relationship between blood pressure and pain. J. Clin. Hypertens. 2013, 15, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Trayes, K.P.; Studdiford, J.S.; Pickle, S.; Tully, A.S. Edema: Diagnosis and management. Am. Fam. Phys. 2013, 88, 102–110. [Google Scholar]
- Oliveros, E.; Patel, H.; Kyung, S.; Fugar, S.; Goldberg, A.; Madan, N.; Williams, K.A. Hypertension in older adults: Assessment, management, and challenges. Clin. Cardiol. 2020, 43, 99–107. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.D.; Sato, R.; Morley, J.E. Association between Pneumonia, Fracture, Stroke, Heart Attack and Other Hospitalizations with Changes in Mobility Disability and Gait Speed in Older Adults. J. Clin. Med. 2021, 10, 3802. [Google Scholar] [CrossRef] [PubMed]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [PubMed]


{kind=link}
| Total Group (n = 490) | Blood Pressure ≥ 130/80 mmHg (n = 302) | Blood Pressure < 130/80 mmHg (n = 188) | p-Value | |
|---|---|---|---|---|
| Age | 83.86 ± 6.17 | 83.95 ± 6.47 | 83.72 ± 5.67 | 0.684 |
| Sex | ||||
| Female | 354 (72.2%) | 238 (78.8%) | 116 (61.7%) | <0.001 |
| Male | 136 (27.8%) | 64 (21.2%) | 72 (38.3%) | |
| Comorbidities | ||||
| Hypertension | 415 (84.7%) | 265 (87.7%) | 150 (79.8%) | 0.020 |
| Heart failure | 124 (25.3%) | 54 (17.9%) | 70 (37.2%) | <0.001 |
| Coronary heart disease | 163 (33.3%) | 79 (26.2%) | 84 (44.7%) | <0.001 |
| Atrial fibrillation | 160 (32.7%) | 71 (23.5%) | 89 (47.3%) | <0.001 |
| Diabetes mellitus | 152 (31.0%) | 87 (28.8%) | 65 (34.6%) | 0.192 |
| Chronic obstructive pulmonary disease | 46 (9.4%) | 24 (7.9%) | 22 (11.7%) | 0.202 |
| Asthma | 9 (1.8%) | 5 (1.7%) | 4 (2.1%) | 0.738 |
| Dementia | 100 (20.4%) | 62 (20.5%) | 38 (20.2%) | >0.999 |
| Depression | 57 (11.6%) | 36 (11.9%) | 21 (11.2%) | 0.885 |
| Current fracture | 240 (49.0%) | 166 (55.0%) | 74 (39.4%) | 0.001 |
| Short-term adverse events while hospitalized | ||||
| Delirium | 19 (3.9%) | 10 (3.3%) | 9 (4.8%) | 0.473 |
| Pneumonia | 18 (3.7%) | 8 (2.6%) | 10 (5.3%) | 0.143 |
| Urinary tract infection | 59 (12.0%) | 28 (9.3%) | 31 (16.5%) | 0.022 |
| Hypokalemia | 168 (34.3%) | 101 (33.4%) | 67 (35.6%) | 0.626 |
| Hyperkalemia | 46 (9.4%) | 24 (7.9%) | 22 (11.7%) | 0.202 |
| Hyponatremia | 60 (12.2%) | 36 (11.9%) | 24 (12.8%) | 0.779 |
| Hypernatremia | 25 (5.1%) | 15 (5.0%) | 10 (5.3%) | 0.837 |
| Hypocalcemia | 198 (40.4%) | 109 (36.1%) | 89 (47.3%) | 0.014 |
| Hypercalcemia | 20 (4.1%) | 11 (3.6%) | 9 (4.8%) | 0.640 |
| Functional assessments | ||||
| Barthel index on admission * | 45 (35–60) | 50 (35–60) | 45 (31.25–60) | 0.240 |
| Barthel index at discharge * | 65 (50–80) | 65 (50–80) | 65 (45–80) | 0.692 |
| Tinetti on admission * | 13 (5–18) | 13 (5.75–18) | 12 (3–18) | 0.573 |
| Tinetti at discharge * | 17 (12–21) | 17 (12–21) | 17 (11–21) | 0.502 |
| Geriatric depression scale * (n = 431) | 4 (2–6) | 3 (2–6) | 4 (2–6) | 0.017 |
| Timed up and go on admission * | 4 (3–5) | 4 (3–5) | 4 (3–5) | 0.309 |
| Timed up and go at discharge * | 3 (2–4) | 3 (2–4) | 3 (3–4) | 0.279 |
| Mini mental status examination * (n = 430) | 26 (22–28) | 26 (22–29) | 26 (22.25–28) | 0.901 |
| Shulman’s clock-drawing test * (n = 357) | 3 (2–4) | 3 (2–4) | 3 (2–4) | 0.706 |
| Prior to CGC | After CGC | p-Value | |
|---|---|---|---|
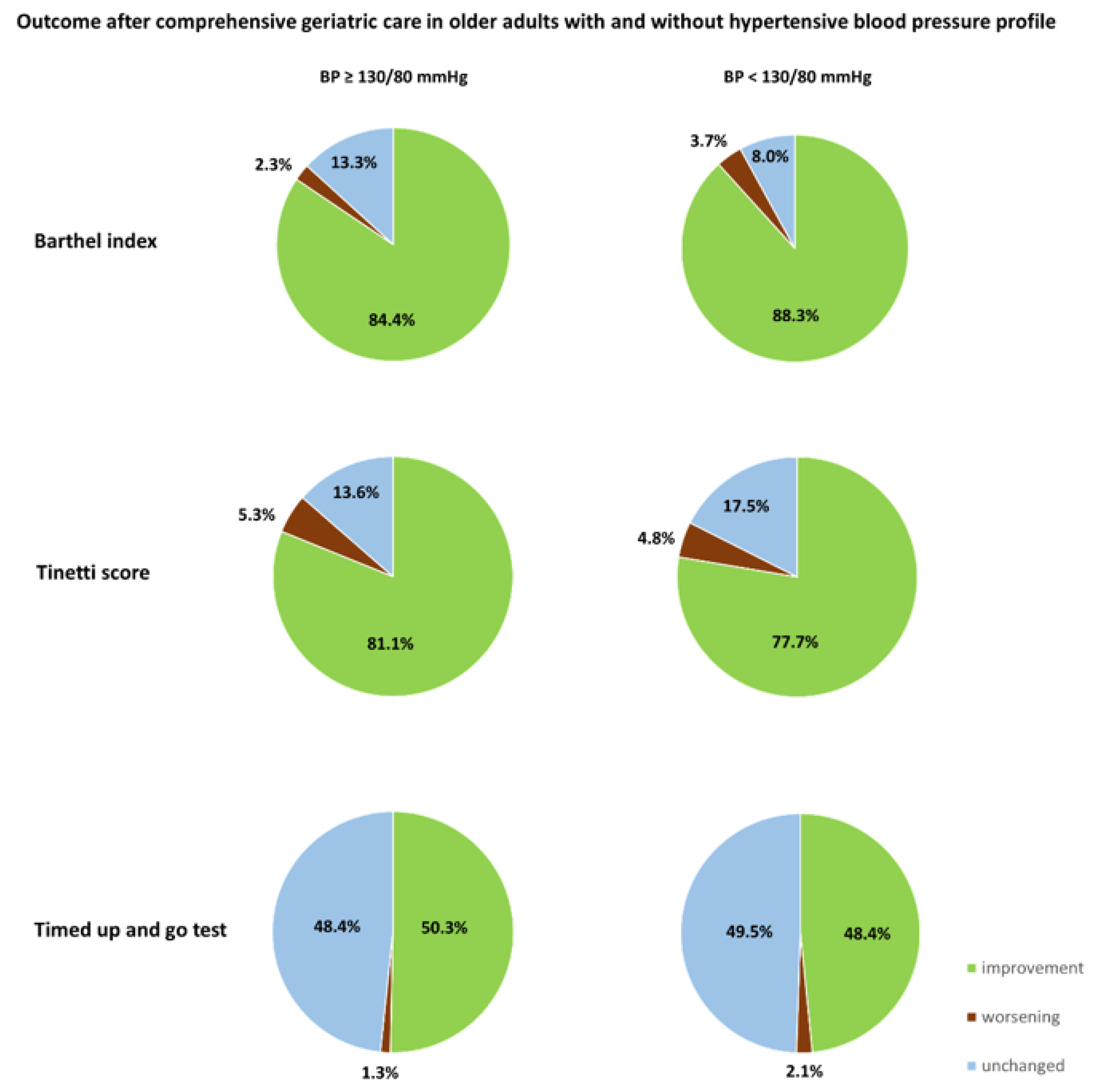
| Patients with mean BP≥130/80 mmHg | |||
| Barthel index (median, IQR) | 50 (35–60) | 65 (50–80) | <0.001 |
| Tinetti score (median, IQR) | 13 (5.75–18) | 17 (12–21) | <0.001 |
| Timed up and go test (median, IQR) | 4 (3–5) | 3 (2–4) | <0.001 |
| Patients with mean BP < 130/80 mmHg | |||
| Barthel index (median, IQR) | 45 (31.25–60) | 65 (45–80) | <0.001 |
| Tinetti score (median, IQR) | 12 (3–18) | 17 (11–21) | <0.001 |
| Timed up and go test (median, IQR) | 4 (3–5) | 3 (3–4) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meyer, M.; Niemöller, U.; Arnold, A.; Stein, T.; Erkapic, D.; Schramm, P.; Tanislav, C. Hypertensive Blood Pressure and Its Impact on Functional Outcomes among Older Adults Receiving Comprehensive Geriatric Care. Geriatrics 2023, 8, 32. https://doi.org/10.3390/geriatrics8020032
Meyer M, Niemöller U, Arnold A, Stein T, Erkapic D, Schramm P, Tanislav C. Hypertensive Blood Pressure and Its Impact on Functional Outcomes among Older Adults Receiving Comprehensive Geriatric Care. Geriatrics. 2023; 8(2):32. https://doi.org/10.3390/geriatrics8020032
Chicago/Turabian StyleMeyer, Marco, Ulrich Niemöller, Andreas Arnold, Thomas Stein, Damir Erkapic, Patrick Schramm, and Christian Tanislav. 2023. "Hypertensive Blood Pressure and Its Impact on Functional Outcomes among Older Adults Receiving Comprehensive Geriatric Care" Geriatrics 8, no. 2: 32. https://doi.org/10.3390/geriatrics8020032