
Hand Dexterity Is Associated with the Ability to Resolve Perceptual and Cognitive Interference in Older Adults: Pilot Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Procedures
2.2.1. Demographics, Cognitive and Neurological Assessments
2.2.2. Hand Dexterity Assessment
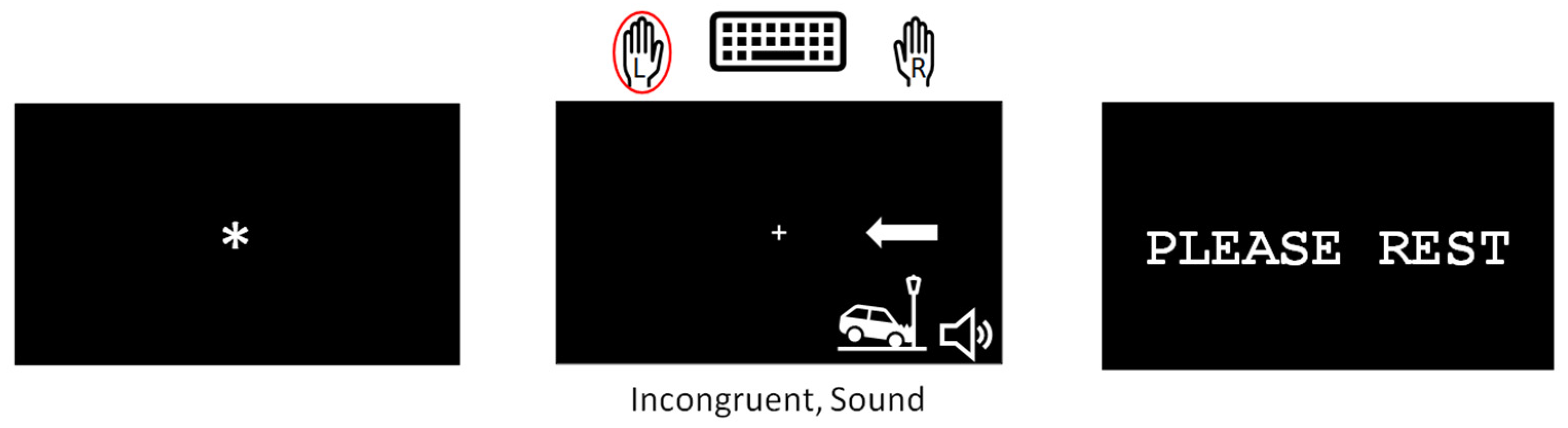
2.3. Modified Simon Task
2.4. Data Analyses
2.4.1. Demographic and Hand Dexterity Data Analyses
2.4.2. Modified Simon Task Data Analyses
3. Results
3.1. Demographic and Clinical
3.2. Behavioral
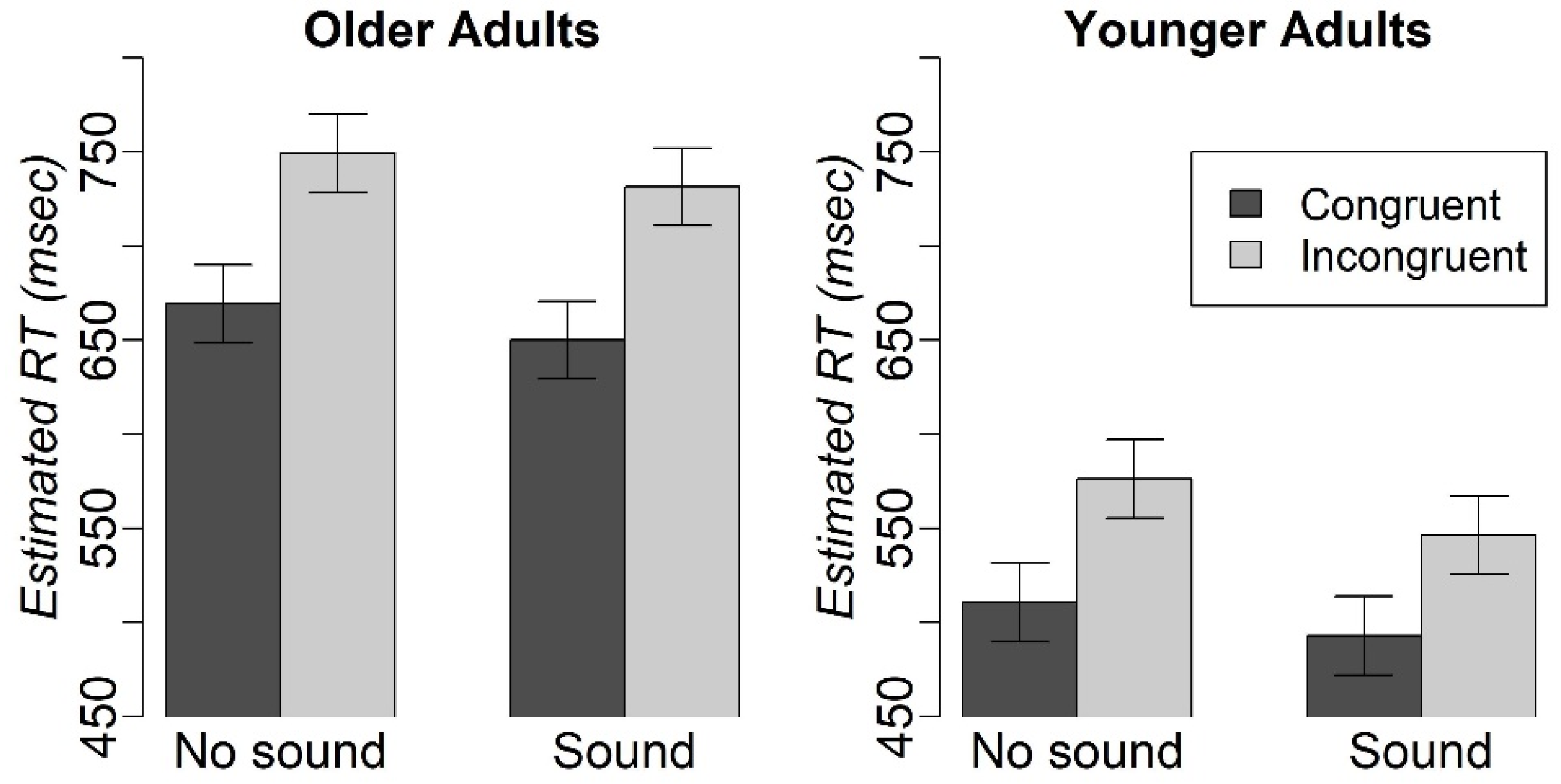
3.2.1. The Effect of Task Condition and Age Group on RT and Accuracy in the Modified Simon Task
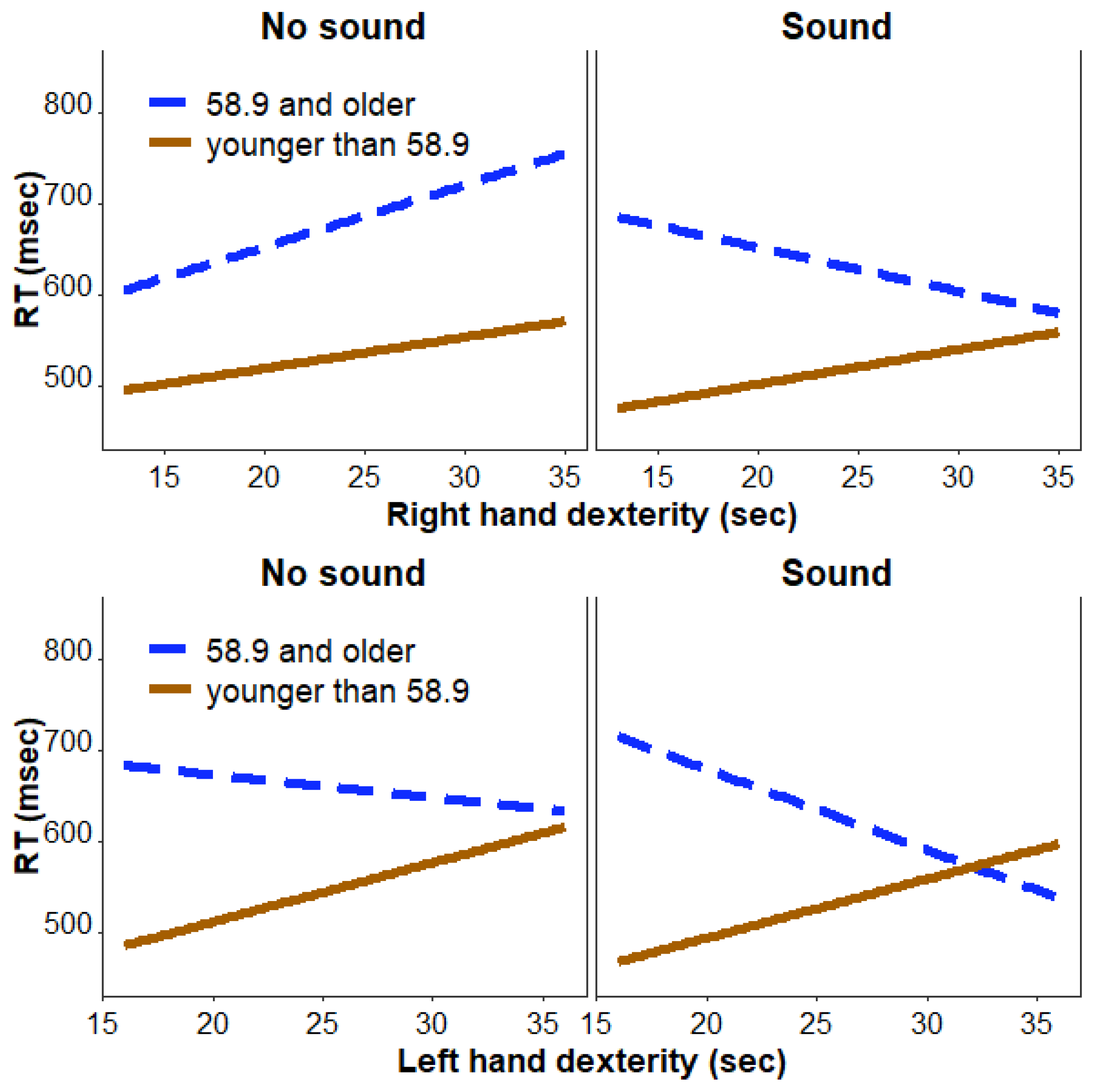
3.2.2. The Effect of Task Condition, Hand Dexterity, and Age Group on RT in the Modified Simon Task
3.2.3. The Effect of Task Condition, Hand Dexterity, and Age Group on Accuracy in the Modified Simon Task
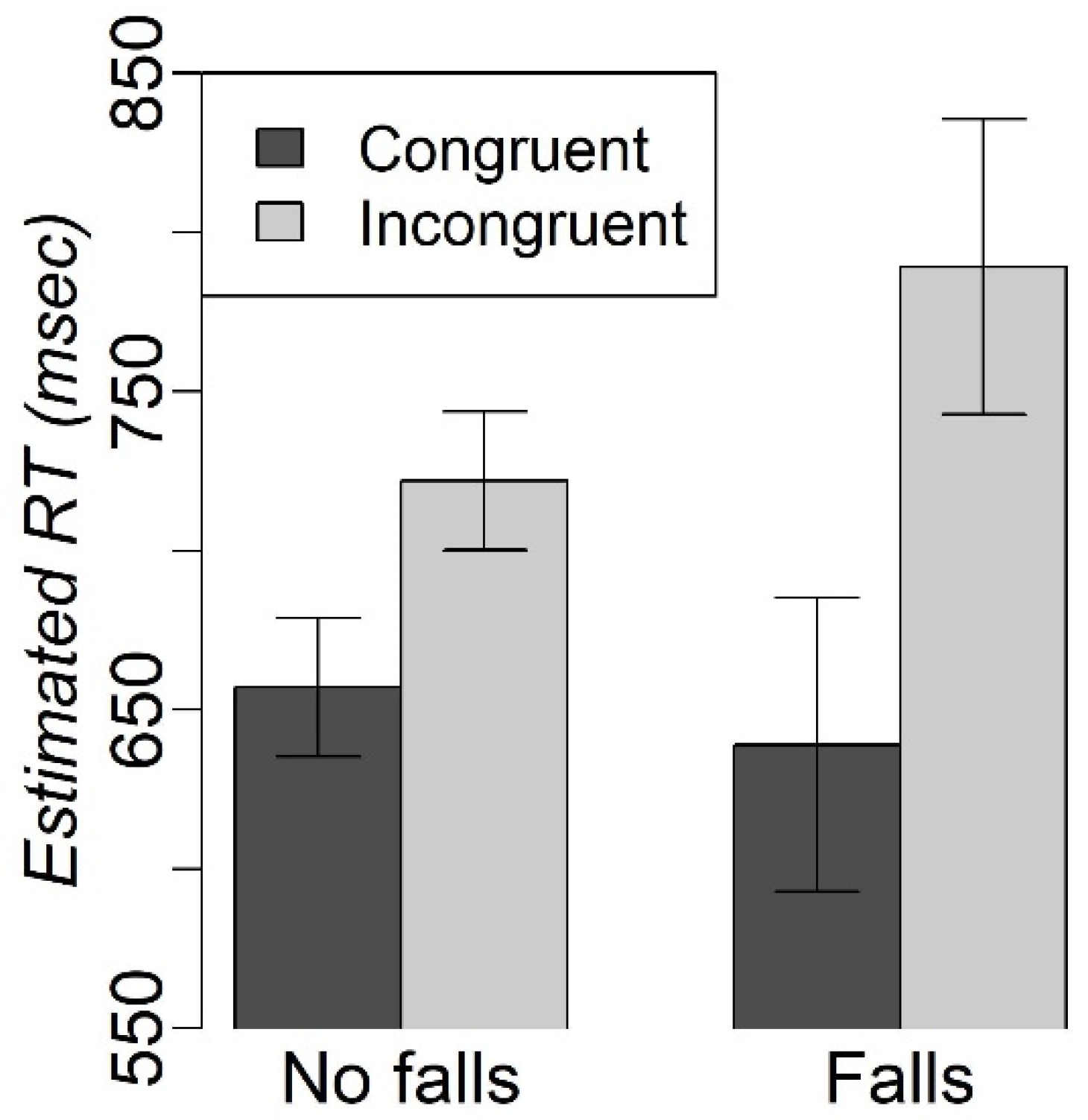
3.2.4. Exploratory Analyses in the Group of Older Individuals
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wais, P.E.; Gazzaley, A. The Impact of Auditory Distraction on Retrieval of Visual Memories. Psychon. Bull. Rev. 2011, 18, 1090–1097. [Google Scholar] [CrossRef] [Green Version]
- MacLeod, C.M. Half a Century of Reseach on the Stroop Effect: An Integrative Review. Psychol. Bull. 1991, 109, 163–203. [Google Scholar] [CrossRef] [PubMed]
- Bessette, K.L.; Karstens, A.J.; Crane, N.A.; Peters, A.T.; Stange, J.P.; Elverman, K.H.; Morimoto, S.S.; Weisenbach, S.L.; Langenecker, S.A. A Lifespan Model of Interference Resolution and Inhibitory Control: Risk for Depression and Changes with Illness Progression. Neuropsychol. Rev. 2020, 30, 477–498. [Google Scholar] [CrossRef]
- Collette, F.; Schmidt, C.; Scherrer, C.; Adam, S.; Salmon, E. Specificity of Inhibitory Deficits in Normal Aging and Alzheimer’s Disease. Neurobiol. Aging 2009, 30, 875–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rinne, P.; Hassan, M.; Fernandes, C.; Han, E.; Hennessy, E.; Waldman, A.; Sharma, P.; Soto, D.; Leech, R.; Malhotra, P.A.; et al. Motor Dexterity and Strength Depend upon Integrity of the Attention-Control System. Proc. Natl. Acad. Sci. USA 2018, 115, E536–E545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alonso, R.N.; Eizaguirre, M.B.; Cohen, L.; Quarracino, C.; Silva, B.; Pita, M.C.; Yastremiz, C.; Vanotti, S.; Garcea, O. Upper Limb Dexterity in Patients with Multiple Sclerosis. Int. J. MS Care 2021, 23, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Nowak, D.A.; Grefkes, C.; Dafotakis, M.; Küst, J.; Karbe, H.; Fink, G.R. Dexterity Is Impaired at Both Hands Following Unilateral Subcortical Middle Cerebral Artery Stroke. Eur. J. Neurosci. 2007, 25, 3173–3184. [Google Scholar] [CrossRef]
- Sunderland, A.; Bowers, M.P.; Sluman, S.M.; Wilcock, D.J.; Ardron, M.E. Impaired Dexterity of the Ipsilateral Hand after Stroke and the Relationship to Cognitive Deficit. Stroke 1999, 30, 949–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Almeida Lima, K.C.; Borges, L. da S.; Hatanaka, E.; Rolim, L.C.; de Freitas, P.B. Grip Force Control and Hand Dexterity Are Impaired in Individuals with Diabetic Peripheral Neuropathy. Neurosci. Lett. 2017, 659, 54–59. [Google Scholar] [CrossRef]
- Proud, E.L.; Morris, M.E. Skilled Hand Dexterity in Parkinson’s Disease: Effects of Adding a Concurrent Task. Arch. Phys. Med. Rehabil. 2010, 91, 794–799. [Google Scholar] [CrossRef]
- de Paula, J.J.; Albuquerque, M.R.; Lage, G.M.; Bicalho, M.A.; Romano-Silva, M.A.; Malloy-Diniz, L.F. Impairment of Fine Motor Dexterity in Mild Cognitive Impairment and Alzheimer’s Disease Dementia: Association with Activities of Daily Living. Rev. Bras. Psiquiatr. 2016, 38, 235–238. [Google Scholar] [CrossRef] [Green Version]
- Abe, T.; Soma, Y.; Kitano, N.; Jindo, T.; Sato, A.; Tsunoda, K.; Tsuji, T.; Okura, T. Change in Hand Dexterity and Habitual Gait Speed Reflects Cognitive Decline over Time in Healthy Older Adults: A Longitudinal Study. J. Phys. Ther. Sci. 2017, 29, 1737–1741. [Google Scholar] [CrossRef] [Green Version]
- Walters, B.H.; Huddleston, W.E.; O’Connor, K.; Wang, J.; Bement, M.H.; Keenan, K.G. The Role of Eye Movements, Attention, and Hand Movements on Age-Related Differences in Pegboard Tests. J. Neurophysiol. 2021, 126, 1710–1722. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi-Cuya, K.E.; Sakurai, R.; Suzuki, H.; Ogawa, S.; Takebayashi, T.; Fujiwara, Y. Observational Evidence of the Association between Handgrip Strength, Hand Dexterity, and Cognitive Performance in Community-Dwelling Older Adults: A Systematic Review. J. Epidemiol. 2018, 28, 373–381. [Google Scholar] [CrossRef] [Green Version]
- Elías, M.N.; Munro, C.L.; Liang, Z. Executive Function, Dexterity, and Discharge Disposition in Older Intensive Care Unit Survivors. Am. J. Crit. Care 2020, 29, 484–488. [Google Scholar] [CrossRef]
- Simon, J.R.; Rudell, A.P. Auditory S-R Compatibility: The Effect of an Irrelevant Cue on Information Processing. J. Appl. Psychol. 1967, 51, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Kawai, N.; Kubo-Kawai, N.; Kubo, K.; Terazawa, T.; Masataka, N. Distinct Aging Effects for Two Types of Inhibition in Older Adults: A near-Infrared Spectroscopy Study on the Simon Task and the Flanker Task. Neuroreport 2012, 23, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Proctor, R.W.; Pick, D.F.; Vu, K.P.L.; Anderson, R.E. The Enhanced Simon Effect for Older Adults Is Reduced When the Irrelevant Location Information Is Conveyed by an Accessory Stimulus. Acta Psychol. 2005, 119, 21–40. [Google Scholar] [CrossRef] [PubMed]
- Van der Burg, E.; Olivers, C.N.L.; Bronkhorst, A.W.; Theeuwes, J. Pip and Pop: Nonspatial Auditory Signals Improve Spatial Visual Search. J. Exp. Psychol. Hum. Percept. Perform. 2008, 34, 1053–1065. [Google Scholar] [CrossRef]
- Chamberland, C.; Hodgetts, H.M.; Vallières, B.R.; Vachon, F.; Tremblay, S. Pip and Pop: When Auditory Alarms Facilitate Visual Change Detection in Dynamic Settings. In Proceedings of the Human Factors and Ergonomics Society, Los Angeles, CA, USA, 15 September 2016; SAGE Publications: Los Angeles, CA, USA; pp. 284–288. [Google Scholar]
- Nelson, H.E. National Adult Reading Test (NART): Test Manual. Wind. UK NFER-Nelson 1982, 124, 1–25. [Google Scholar]
- Andersen, K.W.; Siebner, H.R. Mapping Dexterity and Handedness: Recent Insights and Future Challenges. Curr. Opin. Behav. Sci. 2018, 20, 123–129. [Google Scholar] [CrossRef]
- Amunts, K.; Schlaug, G.; Schleicher, A.; Steinmetz, H.; Dabringhaus, A.; Roland, P.E.; Zilles, K. Asymmetry in the Human Motor Cortex and Handedness. Neuroimage 1996, 4, 216–222. [Google Scholar] [CrossRef]
- Dassonville, P.; Zhu, X.H.; Uǧurbil, K.; Kim, S.G.; Ashe, J. Functional Activation in Motor Cortex Reflects the Direction and the Degree of Handedness. Proc. Natl. Acad. Sci. USA 1997, 94, 14015–14018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Kellor, M.; Frost, J.; Silberberg, N.; Iversen, I.; Cummings, R. Hand Strength and Dexterity. Am. J. Occup. Ther. 1971, 25, 77–83. [Google Scholar] [PubMed]
- Mathiowetz, V.; Weber, K.; Kashman, N.; Volland, G. Adult Norms for the Nine Hole Peg Test of Finger Dexterity. Occup. Ther. J. Res. 1985, 5, 24–38. [Google Scholar] [CrossRef]
- Wang, Y.C.; Magasi, S.R.; Bohannon, R.W.; Reuben, D.B.; McCreath, H.E.; Bubela, D.J.; Gershon, R.C.; Rymer, W.Z. Assessing Dexterity Function: A Comparison of Two Alternatives for the NIH Toolbox. J. Hand Ther. 2011, 24, 313–321. [Google Scholar] [CrossRef] [Green Version]
- Mendoza-Sánchez, S.; Molina-Rueda, F.; Florencio, L.L.; Carratalá-Tejada, M.; Cuesta-Gómez, A. Reliability and Agreement of the Nine Hole Peg Test in Patients with Unilateral Spastic Cerebral Palsy. Eur. J. Pediatr. 2022, 181, 2283–2290. [Google Scholar] [CrossRef]
- Johansson, G.M.; Häger, C.K. A Modified Standardized Nine Hole Peg Test for Valid and Reliable Kinematic Assessment of Dexterity Post-Stroke. J. Neuroeng. Rehabil. 2019, 16, 8. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.M.; Walker, S.C. Fitting Linear Mixed-Effects Models Using Lme4. J. Stat. Softw. 2015, 67, 48. [Google Scholar] [CrossRef]
- Makowski, D.; Ben-Shachar, M.S.; Patil, I.; Lüdecke, D. Estimation of Model-Based Predictions, Contrasts and Means. Available online: https://easystats.github.io/modelbased/ (accessed on 24 January 2023).
- Kuznetsova, A.; Brockhoff, P.B.; Christensen, R.H.B. LmerTest Package: Tests in Linear Mixed Effects Models. J. Stat. Softw. 2017, 82, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Mosso, M.; Freudenberg, A.; McCracken, K.; McGivern, R.F. Sex Differences in Implicit Processing of Allocentric Relationships between Objects and Location in a Simon Task. PLoS ONE 2020, 15, e0235964. [Google Scholar] [CrossRef]
- Proctor, R.W.; Vu, K.P.L. Mixing Location-Irrelevant and Location-Relevant Trials: Influence of Stimulus Mode on Spatial Compatibility Effects. Mem. Cogn. 2002, 30, 281–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aisenberg, D.; Henik, A. Stop Being Neutral: Simon Takes Control! Q. J. Exp. Psychol. 2012, 65, 295–304. [Google Scholar] [CrossRef]
- Herweg, N.A.; Bunzeck, N. Differential Effects of White Noise in Cognitive and Perceptual Tasks. Front. Psychol. 2015, 6, 1639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, A. A Review of the Effects of Noise on Human Performance. Scand. J. Psychol. 1989, 30, 185–206. [Google Scholar] [CrossRef]
- Awada, M.; Becerik-Gerber, B.; Lucas, G.; Roll, S. Cognitive Performance, Creativity and Stress Levels of Neurotypical Young Adults under Different White Noise Levels. Sci. Rep. 2022, 12, 14566. [Google Scholar] [CrossRef]
- Vasylenko, O.; Gorecka, M.M.; Rodríguez-Aranda, C. Manual Dexterity in Young and Healthy Older Adults. 1. Age- and Gender-Related Differences in Unimanual and Bimanual Performance. Dev. Psychobiol. 2018, 60, 407–427. [Google Scholar] [CrossRef] [Green Version]
- Özcan, A.; Tulum, Z.; Pinar, L.; Başkurt, F. Comparison of Pressure Pain Threshold, Grip Strength, Dexterity and Touch Pressure of Dominant and Non-Dominant Hands within and between Right- and Left-Handed Subjects. J. Korean Med. Sci. 2004, 19, 874–878. [Google Scholar] [CrossRef] [Green Version]
- Martin, J.A.; Ramsay, J.; Hughes, C.; Peters, D.M.; Edwards, M.G. Age and Grip Strength Predict Hand Dexterity in Adults. PLoS ONE 2015, 10, e0117598. [Google Scholar] [CrossRef] [Green Version]
- Kornatz, K.W.; Christou, E.A.; Enoka, R.M. Practice Reduces Motor Unit Discharge Variability in a Hand Muscle and Improves Manual Dexterity in Old Adults. J. Appl. Physiol. 2005, 98, 2072–2080. [Google Scholar] [CrossRef]
- Carmeli, E.; Patish, H.; Coleman, R. The Aging Hand. J. Gerontol.-Ser. Biol. Sci. Med. Sci. 2003, 58, 146–152. [Google Scholar] [CrossRef] [Green Version]
- Clark, B.C.; Taylor, J.L. Age-Related Changes in Motor Cortical Properties and Voluntary Activation of Skeletal Muscle. Curr. Aging Sci. 2012, 4, 192–199. [Google Scholar] [CrossRef]
- Tegelbeckers, J.; Schares, L.; Lederer, A.; Bonath, B.; Flechtner, H.H.; Krauel, K. Task-Irrelevant Novel Sounds Improve Attentional Performance in Children with and without ADHD. Front. Psychol. 2016, 6, 1970. [Google Scholar] [CrossRef] [Green Version]
- McDonald, J.J.; Teder-Saälejärvi, W.A.; Hillyard, S.A. Involuntary Orienting to Sound Improves Visual Perception. Nature 2000, 407, 906–908. [Google Scholar] [CrossRef] [PubMed]
- Störmer, V.S. Orienting Spatial Attention to Sounds Enhances Visual Processing. Curr. Opin. Psychol. 2019, 29, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Facts about Falls|Fall Prevention|Injury Center|CDC. Available online: https://www.cdc.gov/falls/facts.html (accessed on 3 January 2023).
- Woolcott, J.C.; Richardson, K.J.; Wiens, M.O.; Patel, B.; Marin, J.; Khan, K.M.; Marra, C.A. Meta-Analysis of the Impact of 9 Medication Classes on Falls in Elderly Persons. Arch. Intern. Med. 2009, 169, 1952–1960. [Google Scholar] [CrossRef] [Green Version]
- Martínez-López, E.J.; Hita-Contreras, F.; Jiménez-Lara, P.M.; Latorre-Román, P.; Martínez-Amat, A. The Association of Flexibility, Balance, and Lumbar Strength with Balance Ability: Risk of Falls in Older Adults. J. Sport. Sci. Med. 2014, 13, 349–357. [Google Scholar]
- Ambrose, A.F.; Paul, G.; Hausdorff, J.M. Risk Factors for Falls among Older Adults: A Review of the Literature. Maturitas 2013, 75, 51–61. [Google Scholar] [CrossRef]
- Center for Disease Control and Prevention (CDC). Prevalence Estimates|Vision and Eye Health Surveillance System|Vision Health Initiative (VHI). Available online: https://www.cdc.gov/visionhealth/vehss/estimates/amd-prevalence.html (accessed on 3 January 2023).
- Feys, P.; Lamers, I.; Francis, G.; Benedict, R.; Phillips, G.; Larocca, N.; Hudson, L.D.; Rudick, R. The Nine-Hole Peg Test as a Manual Dexterity Performance Measure for Multiple Sclerosis. Mult. Scler. 2017, 23, 711–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conklyn, D.; Stough, D.; Novak, E.; Paczak, S.; Chemali, K.; Bethoux, F. A Home-Based Walking Program Using Rhythmic Auditory Stimulation Improves Gait Performance in Patients with Multiple Sclerosis: A Pilot Study. Neurorehabil. Neural Repair 2010, 24, 835–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahraki, M.; Sohrabi, M.; Taheri Torbati, H.R.; Nikkhah, K.; NaeimiKia, M. Effect of Rhythmic Auditory Stimulation on Gait Kinematic Parameters of Patients with Multiple Sclerosis. J. Med. Life 2017, 10, 33–37. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 17.2 | Older Adults (58.9–85 yo) | Younger Adults (18–58.9 yo) | Statistics for Comparison of Older vs. Younger Adults | Cohen’s d for Comparison of Older vs. Younger Adults | |
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | |||
| n | 73 | 37 | 36 | ||
| Sex (number of females) | 42 | 21 | 21 | chi2 = 0, p = 1 | na |
| Age (years) | 53.33(20.76) | 71.61(6.32) | 34.54(11.36) | t(71) = 17.29 p < 0.001 | 4.1 |
| IQ (NART) | 112.23(6.82) | 114.2(5.58) | 110.21(7.43) | t(71) = 2.6 p = 0.01 | 0.62 |
| Cognitive Function (MoCA) | 27.52(1.82) | 27.3(2.09) | 27.75(1.48) | t(71) = −1.06 p = 0.3 | −0.25 |
| Right (Dominant) Hand Dexterity (sec) | 20.27(3.45) | 21.54(3.52) | 18.97(2.88) | t(71) = 3.41 p = 0.001 | 0.81 |
| Left (non-Dominant) Hand Dexterity (sec) | 22.33(3.76) | 23.95(4.12) | 20.67(2.46) | t(71) = 4.12 p = 0.0001 | 0.98 |
| AMD Status | 16 | 16 | 0 | na | na |
| (Number AMD) | |||||
| Fall Status (Number with fall) | 7 | 7 | 0 | na | na |
| Congruency | Sound Condition | Age Group | RT, Msec Mean(SD) | Accuracy Mean(SD) |
|---|---|---|---|---|
| Congruent | No sound | older | 657.36(192.94) | 0.98(0.14) |
| Congruent | No sound | younger | 513.78(163.27) | 0.99(0.11) |
| Congruent | Sound | older | 640.21(200.77) | 0.98(0.14) |
| Congruent | Sound | younger | 498.04(160.64) | 1(0.06) |
| Incongruent | No sound | older | 737.33(200.07) | 0.96(0.19) |
| Incongruent | No sound | younger | 581.16(180.43) | 0.96(0.19) |
| Incongruent | sound | older | 721.13(192.17) | 0.95(0.22) |
| Incongruent | sound | younger | 550.73(166.11) | 0.96(0.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwalbe, M.; Satz, S.; Miceli, R.; Hu, H.; Manelis, A. Hand Dexterity Is Associated with the Ability to Resolve Perceptual and Cognitive Interference in Older Adults: Pilot Study. Geriatrics 2023, 8, 31. https://doi.org/10.3390/geriatrics8020031
Schwalbe M, Satz S, Miceli R, Hu H, Manelis A. Hand Dexterity Is Associated with the Ability to Resolve Perceptual and Cognitive Interference in Older Adults: Pilot Study. Geriatrics. 2023; 8(2):31. https://doi.org/10.3390/geriatrics8020031
Chicago/Turabian StyleSchwalbe, Marie, Skye Satz, Rachel Miceli, Hang Hu, and Anna Manelis. 2023. "Hand Dexterity Is Associated with the Ability to Resolve Perceptual and Cognitive Interference in Older Adults: Pilot Study" Geriatrics 8, no. 2: 31. https://doi.org/10.3390/geriatrics8020031