

Severe Periodontitis Increases the Risk of Oral Frailty: A Six-Year Follow-Up Study from Kashiwa Cohort Study
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
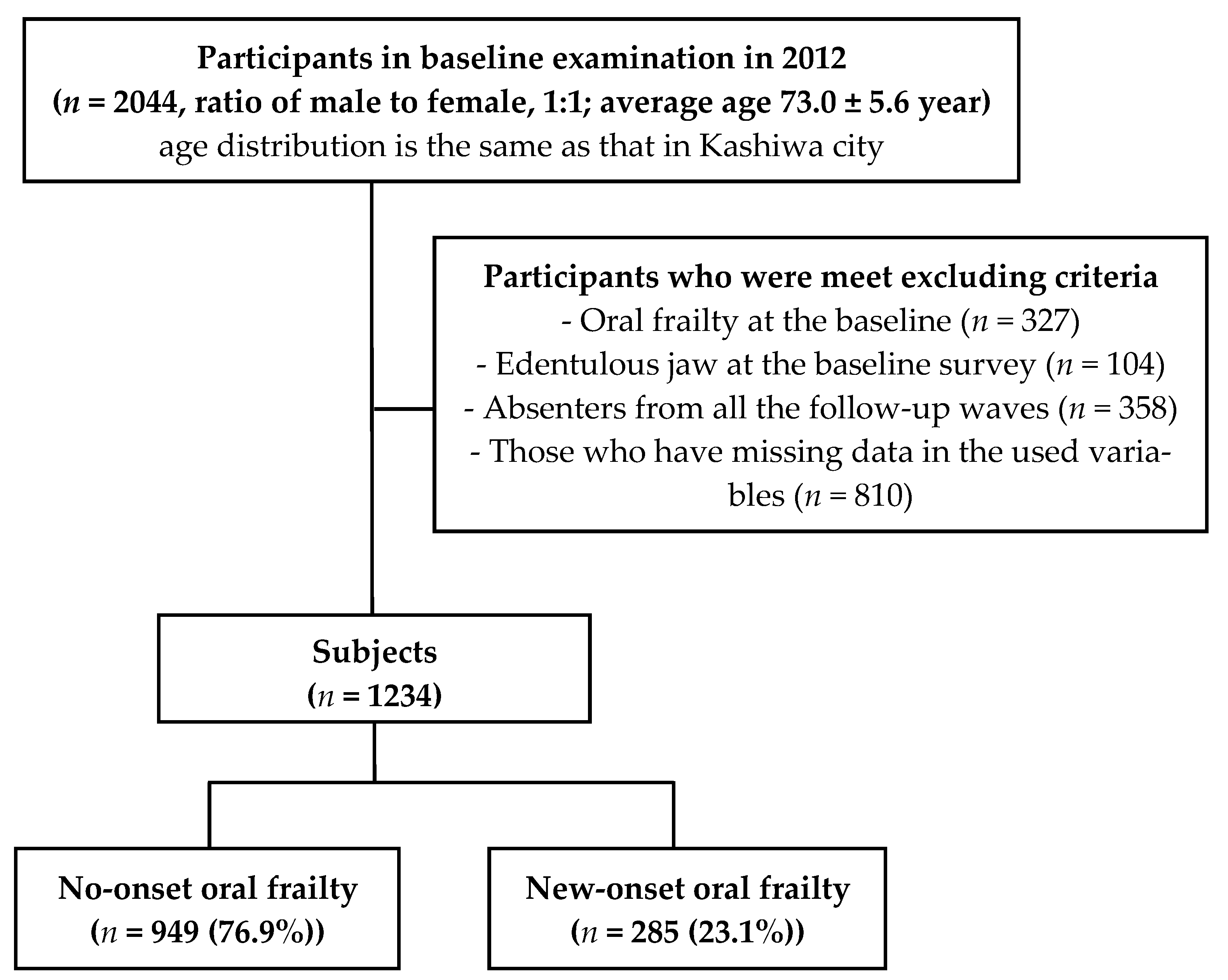
2.1. Setting and Participants
2.2. Measures
2.3. Oral Frailty
2.4. Periodontal Health Status
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Study Participant Characteristics
3.2. Comparison of Basic Characteristics at Baseline with and without New-Onset Oral Frailty
3.3. Comparison of Periodontal Health Status at Baseline with and without New-Onset Oral Frailty
3.4. Relationship between Periodontal Health Status and New-Onset Oral Frailty
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walston, J.; Hadley, E.C.; Ferrucci, L.; Guralnik, J.M.; Newman, A.B.; Studenski, S.A.; Ershler, W.B.; Harris, T.; Fried, L.P. Research agenda for frailty in older adults: Toward a better understanding of physiology and etiology: Summary from the American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults. J. Am. Geriatr. Soc. 2006, 54, 991–1001. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Watanabe, Y.; Hirano, H.; Arai, H.; Morishita, S.; Ohara, Y.; Edahiro, A.; Murakami, M.; Shimada, H.; Kikutani, T.; Suzuki, T. Relationship Between Frailty and Oral Function in Community-Dwelling Elderly Adults. J. Am. Geriatr. Soc. 2017, 65, 66–76. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Takahashi, K.; Hirano, H.; Kikutani, T.; Watanabe, Y.; Ohara, Y.; Furuya, H.; Tetsuo, T.; Akishita, M.; Iijima, K. Oral Frailty as a Risk Factor for Physical Frailty and Mortality in Community-Dwelling Elderly. J. Gerontol. Ser. A 2018, 73, 1661–1667. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, M.; Watanabe, Y.; Motokawa, K.; Shirobe, M.; Inagaki, H.; Motohashi, Y.; Mikami, Y.; Taniguchi, Y.; Osuka, Y.; Seino, S.; et al. Oral frailty and gait performance in community-dwelling older adults: Findings from the Takashimadaira study. J. Prosthodont. Res. 2021, 65, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, M.; Motokawa, K.; Watanabe, Y.; Shirobe, M.; Inagaki, H.; Edahiro, A.; Ohara, Y.; Hirano, H.; Shinkai, S.; Awata, S. Association between Oral Frailty and Nutritional Status among Community-Dwelling Older Adults: The Takashimadaira Study. J. Nutr. Health Aging 2020, 24, 1003–1010. [Google Scholar] [CrossRef]
- Hoshino, D.; Hirano, H.; Edahiro, A.; Motokawa, K.; Shirobe, M.; Watanabe, Y.; Motohashi, Y.; Ohara, Y.; Iwasaki, M.; Maruoka, Y.; et al. Association between Oral Frailty and Dietary Variety among Community-Dwelling Older Persons: A Cross-Sectional Study. J. Nutr. Health Aging 2021, 25, 361–368. [Google Scholar] [CrossRef]
- Ohara, Y.; Motokawa, K.; Watanabe, Y.; Shirobe, M.; Inagaki, H.; Motohashi, Y.; Edahiro, A.; Hirano, H.; Kitamura, A.; Awata, S.; et al. Association of eating alone with oral frailty among community-dwelling older adults in Japan. Arch. Gerontol. Geriatr. 2020, 87, 104014. [Google Scholar] [CrossRef]
- Nishimoto, M.; Tanaka, T.; Takahashi, K.; Unyaporn, S.; Fujisaki-Sueda-Sakai, M.; Yoshizawa, Y.; Iijima, K. Oral frailty is associated with food satisfaction in community-dwelling older adults. Nippon. Ronen Igakkai Zasshi 2020, 57, 273–281. [Google Scholar] [CrossRef]
- Ohara, Y.; Yoshida, N.; Kono, Y.; Hirano, H.; Yoshida, H.; Mataki, S.; Sugimoto, K. Effectiveness of an oral health educational program on community-dwelling older people with xerostomia. Geriatr. Gerontol. Int. 2015, 15, 481–489. [Google Scholar] [CrossRef]
- Wang, T.F.; Huang, C.M.; Chou, C.; Yu, S. Effect of oral health education programs for caregivers on oral hygiene of the elderly: A systemic review and meta-analysis. Int. J. Nurs. Stud. 2015, 52, 1090–1096. [Google Scholar] [CrossRef]
- Ferguson, J.W. The Palmer notation system and its use with personal computer applications. Br. Dent. J. 2005, 198, 551–553. [Google Scholar] [CrossRef]
- Hama, Y.; Kanazawa, M.; Minakuchi, S.; Uchida, T.; Sasaki, Y. Properties of a color-changeable chewing gum used to evaluate masticatory performance. J. Prosthodont. Res. 2014, 58, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Utanohara, Y.; Hayashi, R.; Yoshikawa, M.; Yoshida, M.; Tsuga, K.; Akagawa, Y. Standard values of maximum tongue pressure taken using newly developed disposable tongue pressure measurement device. Dysphagia 2008, 23, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Sakayori, T.; Maki, Y.; Hirata, S.; Okada, M.; Ishii, T. Evaluation of a Japanese “Prevention of long-term care” project for the improvement in oral function in the high-risk elderly. Geriatr. Gerontol. Int. 2013, 13, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. The Manuals of the Evaluation for Ability to Perform Daily Activities on Preventive Care. 2009. Available online: http://www.mhlw.go.jp/topics/2009/05/dl/tp0501-1c_0001.pdf (accessed on 24 October 2022). (In Japanese).
- Ainamo, J.; Barmes, D.; Beagrie, G.; Cutress, T.; Martin, J.; Sardo-Infirri, J. Development of the World Health Organization (WHO) community periodontal index of treatment needs (CPITN). Int. Dent. J. 1982, 32, 281–291. [Google Scholar] [PubMed]
- Kakudate, N.; Muramatsu, T.; Endoh, M.; Satomura, K.; Koseki, T.; Sato, Y.; Ito, K.; Ogasawara, T.; Nakamura, S.; Kishimoto, E.; et al. Factors associated with dry mouth in dependent Japanese elderly. Gerodontology 2014, 31, 11–18. [Google Scholar] [CrossRef]
- Okada, T.; Ikebe, K.; Inomata, C.; Takeshita, H.; Uota, M.; Mihara, Y.; Matsuda, K.; Kitamura, M.; Murakami, S.; Gondo, Y. Association of periodontal status with occlusal force and food acceptability in 70-year-old adults: From SONIC Study. J. Oral Rehabil. 2014, 41, 912–919. [Google Scholar] [CrossRef]
- Kosaka, T.; Ono, T.; Kida, M.; Fushida, S.; Nokubi, T.; Kokubo, Y.; Watanabe, M.; Miyamoto, Y.; Ikebe, K. Deterioration of periodontal status affects declines in masticatory performance: The Suita study. J. Clin. Periodontol. 2021, 48, 1208–1215. [Google Scholar] [CrossRef]
- Scully, C.; Greenman, J. Halitology (breath odour: Aetiopathogenesis and management). Oral Dis. 2012, 18, 333–345. [Google Scholar] [CrossRef] [Green Version]
- Durham, J.; Fraser, H.M.; McCracken, G.I.; Stone, K.M.; John, M.T.; Preshaw, P.M. Impact of periodontitis on oral health-related quality of life. J. Dent. 2013, 41, 370–376. [Google Scholar] [CrossRef]
- Dumitrescu, A.L. Depression and Inflammatory Periodontal Disease Considerations—An Interdisciplinary Approach. Front. Psychol. 2016, 7, 347. [Google Scholar] [CrossRef]
- Gaur, S.; Agnihotri, R. Alzheimer’s disease and chronic periodontitis: Is there an association? Geriatr. Gerontol. Int. 2015, 15, 391–404. [Google Scholar] [CrossRef] [PubMed]
- Kuzuya, M.; Hirakawa, Y.; Suzuki, Y.; Iwata, M.; Enoki, H.; Hasegawa, J.; Iguchi, A. Association between unmet needs for medication support and all-cause hospitalization in community-dwelling disabled elderly people. J. Am. Geriatr. Soc. 2008, 56, 881–886. [Google Scholar] [CrossRef]
- Gellad, W.F.; Grenard, J.L.; Marcum, Z.A. A systematic review of barriers to medication adherence in the elderly: Looking beyond cost and regimen complexity. Am. J. Geriatr. Pharmacother. 2011, 9, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.; Van der Weijden, F.; Doerfer, C.; Herrera, D.; Shapira, L.; Polak, D.; Madianos, P.; Louropoulou, A.; Machtei, E.; Donos, N.; et al. Primary prevention of periodontitis: Managing gingivitis. J. Clin. Periodontol. 2015, 42 (Suppl. S16), S71–S76. [Google Scholar] [CrossRef] [PubMed]
- Westfelt, E. Rationale of mechanical plaque control. J. Clin. Periodontol. 1996, 23, 263–267. [Google Scholar] [CrossRef]
- Shinsho, F. New strategy for better geriatric oral health in Japan: 80/20 movement and Healthy Japan. Int. Dent. J. 2001, 51 (Suppl. S3), 200–206. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. Report on the Survey of Dental Diseases in Japan. 2016. Available online: http://www.mhlw.go.jp/toukei/list/62-17b.html (accessed on 17 January 2023).
- Hakuta, C.; Mori, C.; Ueno, M.; Shinada, K.; Kawaguchi, Y. Evaluation of an oral function promotion programme for the independent elderly in Japan. Gerodontology 2009, 26, 250–258. [Google Scholar] [CrossRef]
- Shirobe, M.; Watanabe, Y.; Tanaka, T.; Hirano, H.; Kikutani, T.; Nakajo, K.; Sato, T.; Furuya, J.; Minakuchi, S.; Iijima, K. Effect of an Oral Frailty Measures Program on Community-Dwelling Elderly People: A Cluster-Randomized Controlled Trial. Gerontology 2021, 68, 377–386. [Google Scholar] [CrossRef]


{kind=link}
| Total (n = 1234) | No-Onset (n = 949) | New-Onset (n = 285) | P | |
|---|---|---|---|---|
| Basic attributes, Physical conditions | ||||
| Age, year | 72.2 (±5.1) | 71.7 (±4.8) | 73.8 (±5.6) | <0.001 |
| Sex, men | 50.8% | 51.2% | 49.5% | 0.607 |
| BMI, kg/m2 | 23.0 (±3.0) | 23.0 (±2.9) | 22.9 (±3.3) | 0.462 |
| Education, year | 12.9 (±2.8) | 12.9 (±2.7) | 12.7 (±2.8) | 0.147 |
| IADL | 4.9 (±0.4) | 4.9 (±0.4) | 4.8 (±0.6) | 0.086 |
| Cognitive function, MMSE score | 28.4 (±1.8) | 28.4 (±1.7) | 28.1 (±1.9) | 0.021 |
| GDS-15 score | 2.4 (±2.7) | 2.2 (±2.7) | 2.7 (±2.7) | 0.009 |
| Yearly income (≤1.4 million yen) | 55.6% | 54.8% | 58.2% | 0.304 |
| Polypharmacy (≥6 medications) | 14.6% | 12.9% | 20.4% | 0.002 |
| Present chronic conditions | ||||
| Hypertension | 41.4% | 40.5% | 44.6% | 0.218 |
| Diabetes mellitus | 11.6% | 10.5% | 15.1% | 0.035 |
| Osteoporosis | 9.3% | 8.4% | 12.6% | 0.029 |
| Dyslipidemia | 39.9% | 38.6% | 44.2% | 0.088 |
| Malignant neoplasm | 14.7% | 14.2% | 16.5% | 0.344 |
| Heart disease | 15.5% | 14.9% | 17.5% | 0.272 |
| Apoplexy | 5.7% | 4.7% | 8.8% | 0.010 |
| Oral frailty component | ||||
| Number of remaining teeth | 23.0 (±6.5) | 24.4 (±5.2) | 18.2 (±7.7) | <0.001 |
| Chewing ability | 18.4 (±5.9) | 19.0 (±5.9) | 16.5 (±5.6) | <0.001 |
| Tongue pressure | 31.4 (±7.3) | 31.8 (±7.2) | 29.9 (±7.4) | <0.001 |
| Articulatory oral motor skill (“ta” times/s) | 6.2 (±0.8) | 6.3 (±0.8) | 6.0 (±0.9) | 0.001 |
| Difficulties eating tough foods (yes) | 8.7% | 6.7% | 15.1% | <0.001 |
| Difficulties in swallowing on tea or soup (yes) | 14.3% | 11.8% | 22.5% | <0.001 |
| Other Oral status | ||||
| Number of functioning teeth | 27.3 (±2.3) | 27.4 (±2.2) | 26.8 (±2.5) | <0.001 |
| Oral wettability (<3 mm classified as dry mouth) | 34.2% | 34.3% | 33.9% | 0.899 |
| Total (n = 1234) | No-Onset (n = 949) | New-Onset (n = 285) | P | |
|---|---|---|---|---|
| Community Periodontal Index (CPI) | ||||
| Score 0 | 17 (1.4%) | 12 (1.3%) | 5 (1.8%) | 0.187 |
| Score 1 | 17 (1.4%) | 12 (1.3%) | 5 (1.8%) | |
| Score 2 | 281 (22.8%) | 217 (22.9%) | 64 (22.5%) | |
| Score 3 (moderate periodontitis) | 439 (35.5%) | 353 (37.2%) | 86 (30.2%) | |
| Score 4 (severe periodontitis) | 480 (38.9%) | 355 (37.4%) | 125 (43.9%) |
| n (%) a | Unadjusted Hazard Ratio (95% CI) | p | Adjusted Hazard Ratio (95% CI) b | P | |||
|---|---|---|---|---|---|---|---|
| The number of participants | 285/1234 (23.1%) | ||||||
| Community Periodontal Index (CPI) | |||||||
| ≤2 | 74/315 (23.5%) | 1.00 | 1.00 | ||||
| ≥3 (moderate periodontitis) | 211/919 (23.0%) | 1.02 | (0.78–1.33) | 0.892 | 1.09 | (0.83–1.44) | 0.530 |
| ≤3 | 160/754 (21.2%) | 1.00 | 1.00 | ||||
| 4 (severe periodontitis) | 125/480 (26.0%) | 1.38 | (1.09–1.74) | 0.007 | 1.42 | (1.12–1.81) | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishimoto, M.; Tanaka, T.; Hirano, H.; Watanabe, Y.; Ohara, Y.; Shirobe, M.; Iijima, K. Severe Periodontitis Increases the Risk of Oral Frailty: A Six-Year Follow-Up Study from Kashiwa Cohort Study. Geriatrics 2023, 8, 25. https://doi.org/10.3390/geriatrics8010025
Nishimoto M, Tanaka T, Hirano H, Watanabe Y, Ohara Y, Shirobe M, Iijima K. Severe Periodontitis Increases the Risk of Oral Frailty: A Six-Year Follow-Up Study from Kashiwa Cohort Study. Geriatrics. 2023; 8(1):25. https://doi.org/10.3390/geriatrics8010025
Chicago/Turabian StyleNishimoto, Misa, Tomoki Tanaka, Hirohiko Hirano, Yutaka Watanabe, Yuki Ohara, Maki Shirobe, and Katsuya Iijima. 2023. "Severe Periodontitis Increases the Risk of Oral Frailty: A Six-Year Follow-Up Study from Kashiwa Cohort Study" Geriatrics 8, no. 1: 25. https://doi.org/10.3390/geriatrics8010025